
흉추 4-8번(T4-8)은 항상 kypotic change가 과도해지면서 문제가 발생
이러한 관절의 dysfunction이 생체역학적 과부하를 일으키는 문제에 대한 검사와 평가, 치료에 대한 논문
정말 멋진 논문
![]() mid thoracic dysfucntion 진단.pdf
mid thoracic dysfucntion 진단.pdf
Introduction
- 현대사회에서 앉기(sitting)는 상체자세(upright posture)에 명백한 영향을 초래. 특히 mid-thoracic부위는 좀더 후만(kyphotic)되는 방향으로 진행되는 경향
- 흉추와 rib cage의 선천적인 안정성때문에 직접적으로 통증을 유발하지 않는 반면, 이 기능적인 biomechanical deficit는 운동계 시스템을 통해 이차적으로 문제를 초래
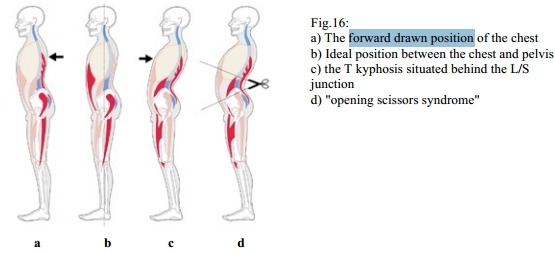
- head forward posture(경추 7번 body를 평행선으로 긋고, 추체중앙과 귀중앙을 선으로 그어 만들어지는 각도가 ( 38.5~42.5 (retroversion<38.5~42.5<forward posture))도까지 정상), chin protrusion, round shoulder(둥근어깨 증후군), 증가된 lumbo-sacral lordosis, sternum과 symphysis의 approximation은 전형적인 비정상 정렬의 변화. => mid thoracic kyphosis
- 이 결과 필연적으로 국소적 조직이 불안정해지고, 다양한 통증이 만들어짐.
- 이 논문은 3part로 이루어져 있음
- 첫째, muscle imbalance를 포함한 dysfunction, 그 문제가 만들어지는 비정상 정렬에 대한 내용
- 둘째, treatment issue
- 셋째, 그와 관련된 임상적 issue를 서머리함
Mid-thoracic(T4-T8) dysfunction
- Mid-thoracic(T4-T8) dysfunction은 아래 그림과 같이 오랫동안 앉기 자세의 결과로 초래
- Mid-thoracic(T4-T8) dysfunction은 아래 그림과 같이 thoracic, lumba-pelvic, cervico-cranial posture가 사슬관계로 서로 연관되어 있음. 이 문제는 기능부전의 측면뿐 아니라 재활치료의 측면까지 서로 영향을 미침.
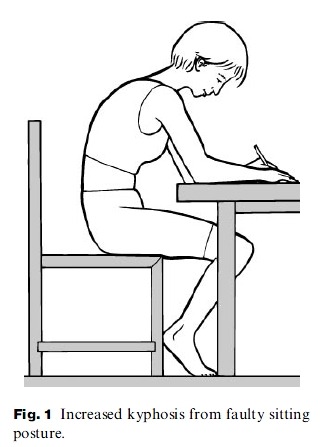
- thoracic kyphosis 증가의 결과 생체역학적 과부하와 기능적 적응은 locomotor system의 여러부위에 영향을 미침
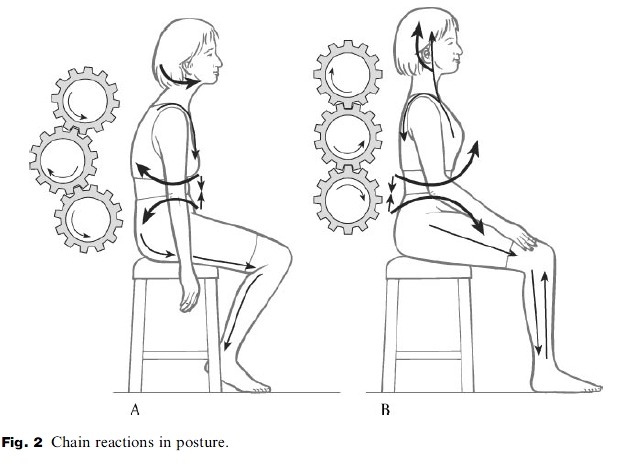
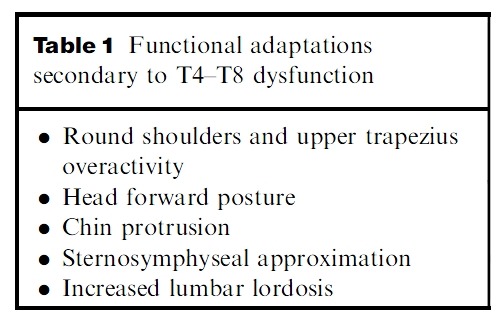
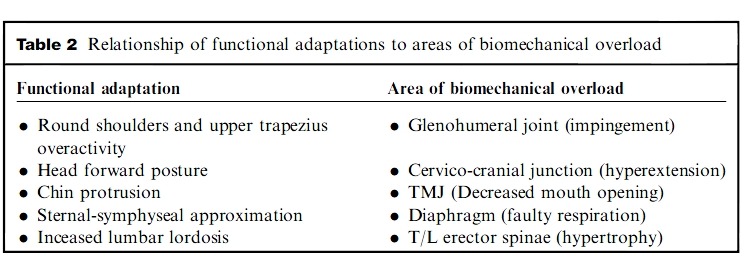
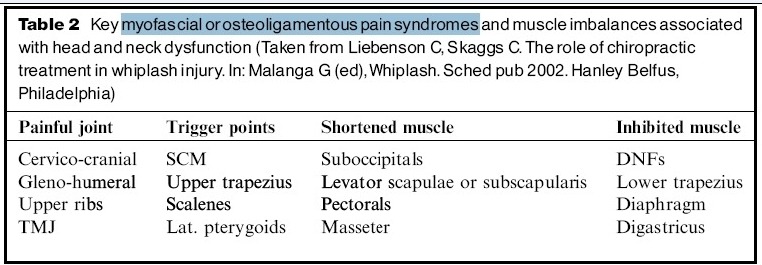
Brugger's sternosymphyseal syndrome is an apt description of the collection of pain syndromes, functional
limitations, and performance deficits which can all result from this endemic postural disorder (Lewit 1996, 1999; Liebenson et al. 1998; Liebenson 1999). In the kyphotic posture the sternum and symphysis pubis approximate affecting not just the joints already mentioned but key muscles such as the diaphragm in basic functions such as respiration. Tables 1 and 2 summarize some of the more clinically relevant examples of functional adaptation and biomechanical overload secondary to mid-thoracic dysfunction.
- 브뤼거가 제안한 sterno-symphyseal syndrome은 특유의 postural disorder 결과를 야기할 수 있는 통증 기술, 기능제한, 수행능력 제한의 가장 적합한 표현.
- kyphotic posture에서 sternum and symphysis pubis는 approximation되어 관절 뿐만 아니라 호흡에 관련된 근육(diaphragm)에 영항을 미침.
mid-thoracic dysfunction으로 야기되는 functional adaptation
- round shoulder와 상부승모근의 과활성화 => 충돌증후군(GH joint pain)
- head forward posture => C0-C1 cervico-cranial junction(hyperextension)문제
- chin protrusion => TMJ(입벌리기 감소)
- sternosymphyseal approximation => 호흡능력 저하
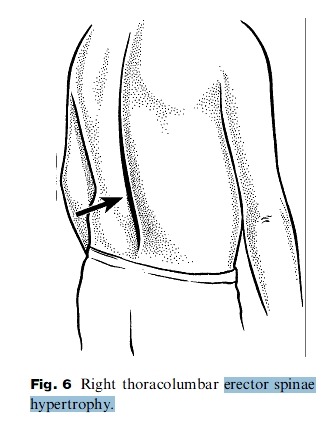
- lumbar lordosis의 증가 => thoracolumbar erector spinae hypertrophy(척추기립근 과활성화)
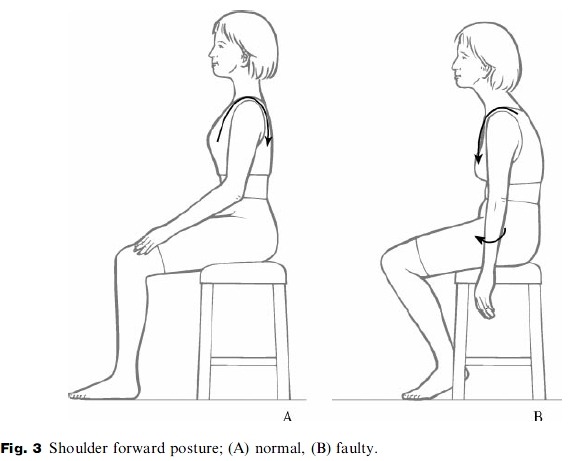
Increased mid-thoracic kyphosis pitches the shoulders forward into a rounded and internally rotated position (Fig. 3) (Janda 1996, 1998;Liebenson et al. 1998). With the shoulders rolled forward the pectorals habituate to a shortened
length as do the internal rotators including subscapularis, pectorals, and latissmus dorsi. This increases stress on the glenohumeral (GH) joint anteriorly and superiorly by altering the scapulohumeral rhythm, reducing mobility in arm elevation and predisposing to mechanical impingement of the subacromial space, anterior labrum instability, and rotator cuff tendinosis (Wilk & Arrigo 1992; Kamkar et al. 1993; Grant et al. 1997; Norris 1998; Liebenson et al. 1998).
- mid-thoracic kyphosis 증가는 아래 그림과 같이shoulder forward를 초래하고, 둥근어깨를 만들면서 상완의 내회전 변형을 야기. 그 결과 대소흉근이 짧아지는 습관때문에 견갑하근, 대소흉근, 광배근을 포함한 내회전 근육으로 함께 작용.
- 이러한 변화는 SHR을 변화시켜 GH joint에 ant, sup방향으로 부하를 증가시키고, arm elevation mobility를 감소시켜 subacromial space, ant labrum instability, 회전근개 tendinosis의 mechanical impingement의 소인을 만들어냄.
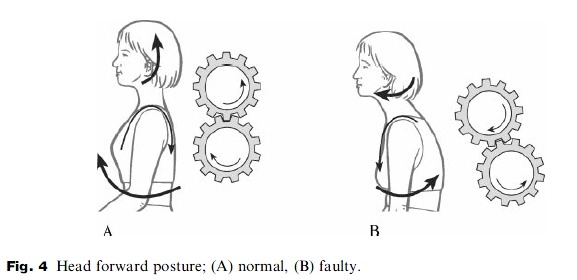
With the shoulders forward the upper trapezius functionally adapts by tensing in order to check-rein(견제수단) both the forward shoulders and head. Often this upper trapezius tension is mistakenly treated as a primary problem when it is usually secondary to the other biomechanical factors which are `upstream' of it. The head forward posture goes hand in hand with increased thoracic kyphosis (Fig. 4) (Janda 1986, 1996, 1998; Murphy 1999; Lewit 1996, 1999; Liebenson 1996; Liebenson et al. 1998; Skaggs & Liebenson 2000).
- shoulder forward와 함께 상부승모근은 forward shoulder and head를 견제하기 위해 긴장하면서 기능적으로 적응함. 이러한 상부승모근 긴장은 때때로 primary problem으로 치료하는데 실제 이 문제는 대개 secondary(2차적인) 문제임(upstream).
- head forward posture는 thoracic kyphosis증가와 관련됨.
Usually the lower cervical spine loses its normal lordosis and the cervico-cranial junction (C0-C1) secondarily
compensates by hyperextending in an attempt to keep the visual gaze in the horizontal plane (Watson, Trott 1993; Murphy 1999; Janda 1986; Liebenson et al. 1998). Often treatment is mistakenly focused on the compensatory C0-C1 hyperextension rather than the source of this functional adaptation.
- 일반적으로 horizontal plane에서 visual gaze를 유지하기 위해 하부경추 normal lordosis 소실과 c0-c1은 과신전되면서 2차적으로 보상함. 때때로 치료는 source of this functional adaptation보다 보상적 변화가 일어난 c0-c1의 과신전에 초점이 맞추어지는 실수를 범함.
Chin protrusion normally follows from head forward posture and will alter function of the temperomandibular joint
(TMJ) (Janda 1986; Skaggs & Liebenson 2000). Specifically when a protruded chin is present the patient has decreased
extensibility in mouth opening which alters the biomechanics of the TMJ increasing stress on the disc (Skaggs & Liebenson 2000).
- chin protrusion은 head forward posture를 따라 발생하고 TM joint의 기능을 변화킬 수 있음. 명확하게 chin protrusion이 발생하면 환자는 mouth opening에서 신장성이 감소되고, 이는 TMJ의 생체역학적 스트레스를 악화시킴.
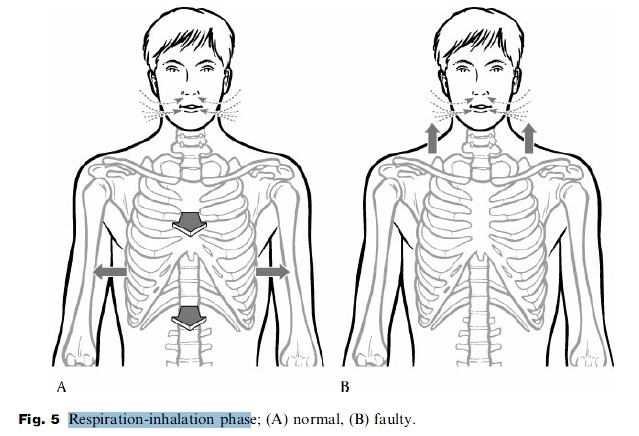
Faulty respiration secondary to the sternosymphyseal syndrome occurs due to lower rib compression on the diaphragm (Lewit 1999; Liebenson 1999a, 1999b). The accessory muscles of respiration such as the scalenes and shoulder girdle elevators substitute for the inhibited diaphragm and result in upper chest breathing predominating over belly breathing (Fig. 5) (Simons et al. 1999; Lewit 1980, 1999; Liebenson et al. 1998; Liebenson 1999b). In the seated position the patient breathes by vertically raising their chest rather than widening the rib cage in the horizontal plane (Lewit 1980, 1999; Liebenson et al. 1998; Liebenson 1999b).
- sternosymphyseal syndrome에 의해 2차적으로 발생하는 Faulty respiration은 하부 늑골압박에 의해 초래됨
- 부호흡근인 사각근, shoulder girdle elevator(upper trapezius and levator scapulae)는 기능저하된 흉곽근육(inhibited diaphragm)을 대신하고, 그 결과 upper chest 호흡을 일으킴. 그래서 아래 그림과 같이 앉기 자세에서 환자는 수평면에서 rib cage를 넓혀 호흡하지 못하고, 그들의 chest를 수직방향으로 들어올려 호흡함.
When thoracic kyphosis is increased compensations above and below occur in an attempt to stabilize the bodies center of mass and restore equilibrium. Most of the changes above have already been described. Commonly, increased anterior pelvic tilt and shortened psoas or increased lumbar lordosis is present as a secondary compensation or functional
adaptation to decreased thoracic mobility in extension (Norris 1998). Overactivity of the thoraco- lumbar (T/L) erector spinae muscles is seen as an attempt to check-rein the forward drawn posture (Fig. 6). The muscles may even become hypertrophied in chronic cases in individuals who have sedentary histories (Janda 1996; Lewit 1999; Liebenson & Chapman 1998b).
- thoracic kyphosis가 증가할때 발생한 위, 아래 보상성 움직임은 평형을 회복하고, 신체 중심을 안정화하기 위해서 발생
- 흔히 보상성 움직임으로 증가된 ant pelvic tilt, 짧아진 요근 또는 증가된 요추전만이 관찰되는데, 이는 2차적 보상움직임이나 또는 감소된 thoracic mobility in extension에 기능적 적응으로 발생함.
- thoraco- lumbar (T/L) erector spinae muscles의 과활성화는 아래 그림과 같이 forward drawn posture를 견제하기 위해 나타남. 이러한 근육의 과활성화에 의한 hypertrophy는 sedentary work를 오래하는 사람에게서 만성적으로 나타남.
Assessment of myofascial pain and muscle imbalance associated with mid-thoracic dysfunction
Myofascial pain, muscular overload, and joint strain are clinically related. With postural change such as increased thoracic kyphosis certain muscle imbalances in other regions predictably occur and are easily indentifiable. In many cases when thoracic kyphosis increases other joints such as the GH or upper cervical find themselves in new
positions. The GH may be drawn forward and internally rotated while the upper cervical spine is hyperextended.
With a change in joint position agonist and antagonist muscles surrounding these joints will undergo length and tension changes.
mid thoracic dysfunction과 관련된 근육 불균형, mps의 평가
- 근막통, 근육과부하, 관절 strain은 임상적으로 서로 연관됨. 증가된 thoracic kyphosis와 같은 자세 변화는 예측가능한 부위, 쉽게 확인할 수 있는 부위에 muscle imbalance를 야기
- 아주 많은 case에서 thoracic kyphosis가 증가할때, GH joint 또는 상부경추(upper cervical spine)는 새로운 자세를 잡음. 예를들어 상부경추가 과신전되는 동안 GH는 drawn forward가 될 수 있고, 내회전 될 수 있음.
- change in joint position과 함께 관절의 주동근과 길항근은 길어지거나 긴장되는 변화를 겪을 수 있음.
Muscles which are held in a shortened position for a long period of time may adapt to this by losing their flexibility or `resting length'(Norris 1998, 2000). As a result, even passive positioning of the related joints back to more `neutral'
or `centrated' positions may be hindered by resultant passive insufficiency of the shortened tissues. When passive mobilization or positioning of a joint such as a forward drawn GH joint into a `neutral' posture is restricted passive
insufficiency is said to be present. A forward drawn shoulder will typically overload the anterior glenoid labrum and lengthening of the shortened pectorals and posterior joint capsule will be necessary in order to `centrate' the GH joint.
- 오랫동안 근육이 짧아지는 자세가 되면 근육의 특성인 flexibility 또는 resting length를 잃어버리는 적응을 할 수 있음.
- 그 결과 중립자세, 중심자세와 관련된 수동적 positioning에서조차도 짧아진 조직의 resultant passive insufficiency에 의해 방해될 수 있음.
- forward drawn GH joint가 중립자세로 되는 것과 같은 passive mobilization 또는 positioning of a joint가 제한될때, passive insufficiency는 존재하는 것으로 말해짐???
- forward drawn shoulder는 anterior glenoid labrum에 전형적으로 과부하가 걸릴 수 있고, 짧아진 흉근, post joint capsule가 늘어나는 것이 GH 관절이 가운데 자리잡기 위해서 필요할 수 있음.
참고) Muscle Resting Length and Passive Tension
A muscle’s resting length is the length of the muscle at full rest. A healthy muscle will have some tension even at full rest, but not enough to cause a chronic involuntary flexion of the muscle (passive tension). A muscle with healthy tonicity should not have a shortened resting length, involuntary contraction or passive tension build-up.
- 근육의 resting length는 완전 휴식상태에서 근육의 길이를 말함. 건강한 근육은 완전 휴식상태에서도 약간의 tension을 가지고 있음.
- 건강한 tonicity를 가진 근육은 "짧아진 rest length"를 가지면 안되고, 불수의 근수축, 수동적 긴장을 가지면 안됨.
Then, the muscles which have been in lengthened positions or inhibited will need to be facilitated and re-educated to function in their `inner-range' (Norris 2000; Richardson et al. 1999). This `inner-range' is the range of muscle length
where the joint is in a `neutral' position and agonist and anagonist muscles are in balance with respect to their length. Naturally, if muscle shortening (or overactivity) and lengthening (or inhibition) are present and these changes occurred
secondary to thoracic kyphosis then symptoms from the related joint such as the GH joint (i.e. rotator cuff tendinitits, anterior instability, impingement) will eventually recur unless the source of the biomechanical overload is addressed.
- 그래서 늘어나거나 움직임이 제한된 근육은 촉진되거나 관절의 Inner range내에서 기능을 위해 재교육되는 것이 필요할 수 있음.
- inner-range는 근육길이의 범위로 관절이 중립자세에 있을때, 주동근과 길항근은 근육의 길이에 대하여 균형을 잡는 것을 말함.
- 일반적으로 만약 근육이 과활성화로 shortening되고, 억제되어 lengthening된다면, 이 변화는 2차적으로 thoracic kyphosis을 일으키고, 그것과 관련된 GH joint의 증상(회전근개 건염, 어깨 ant instability, impingement)은 다시 나타날 수 있음. 생체역학적 과부하 source가 부여되지 않아도...
Functional adaptations to the thoracic kyphosis often lead to other tissues becoming overloaded. While it is the overloaded tissues which usually generate pain it is important to realize that the source of such biomechanical overload is in other
tissues functional related, but at a distance in the kinetic chain (Kibler 1998; Kibler et al. 1998; Lewit 1999, 1999b).
- thoracic kyphosis에 기능적 적응은 때때로 다른 조직에 과부하를 초래함. 조직이 과부하가 걸리때 일반적으로 통증이 발생하고, 이러한 생체역학적 과부하 source는 기능적으로 연관된 다른 조직에 통증을 발생시킴. 하지만 이는 사슬관계내의 distance에서 발생.
Key myofascial or osteoligamentous pain syndromes and muscle imbalances associated with T4±T8 dysfunction include the following (see Table 3):
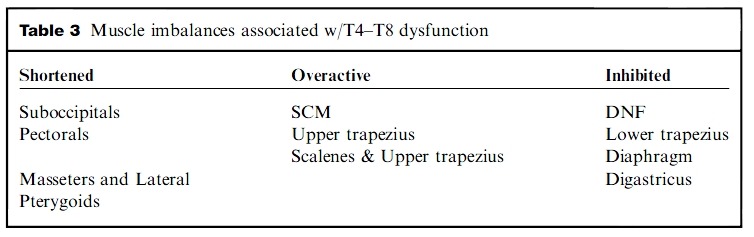
T4-T8 dysfunction과 관련된 muscle imbalance
- 후두하근 짧아짐, SCM 과활성화, DNF 근육 억제
- 대흉근 짧아짐, 상부승모근 과활성화, 하부승모근 억제
- 대흉근 짧아짐, 사각근과 상부승모근 과활성화, diaphragm 억제
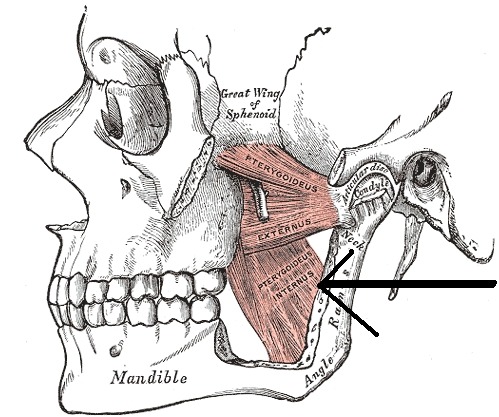
- masseter and lateral pterygoid 짧아짐, ......diagastricus 억제
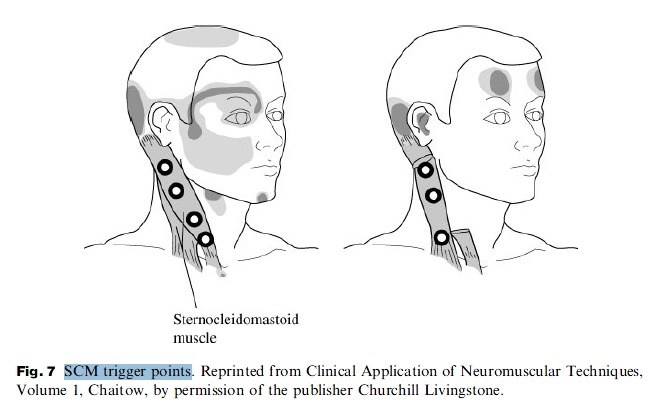
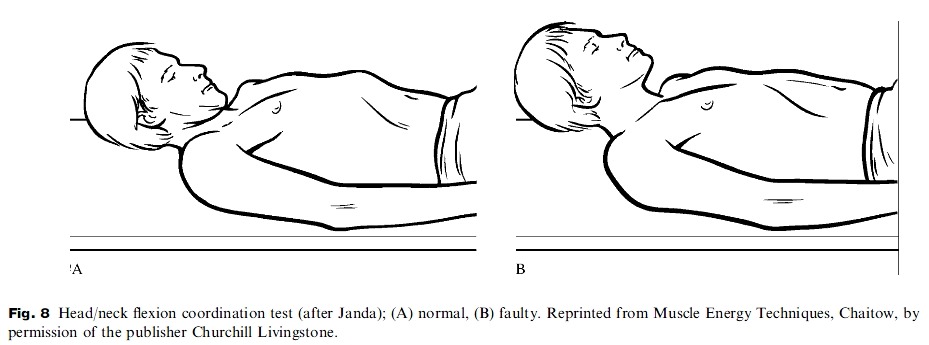
Pain referred from the sternocleidomastoid (SCM) muscle(s) or upper cervical joints is related to muscle imbalance
involving shortened suboccipitalis combined with overactive SCM and inhibited deep neck flexors (DNF) (Fig. 7). A simple screen is to perform the head/neck flexion test (Fig. 8). .
- SCM 또는 upper cervical joint로부터의 referred pain은 과활성화된 SCM과 억제된 DNF와 연관되어 짧아진 후두하근(suboccipitalis)의 muscle imbalance와 연관되어짐.
- screening test는 그림 8번의 head/neck flexion coordination test로 시행.
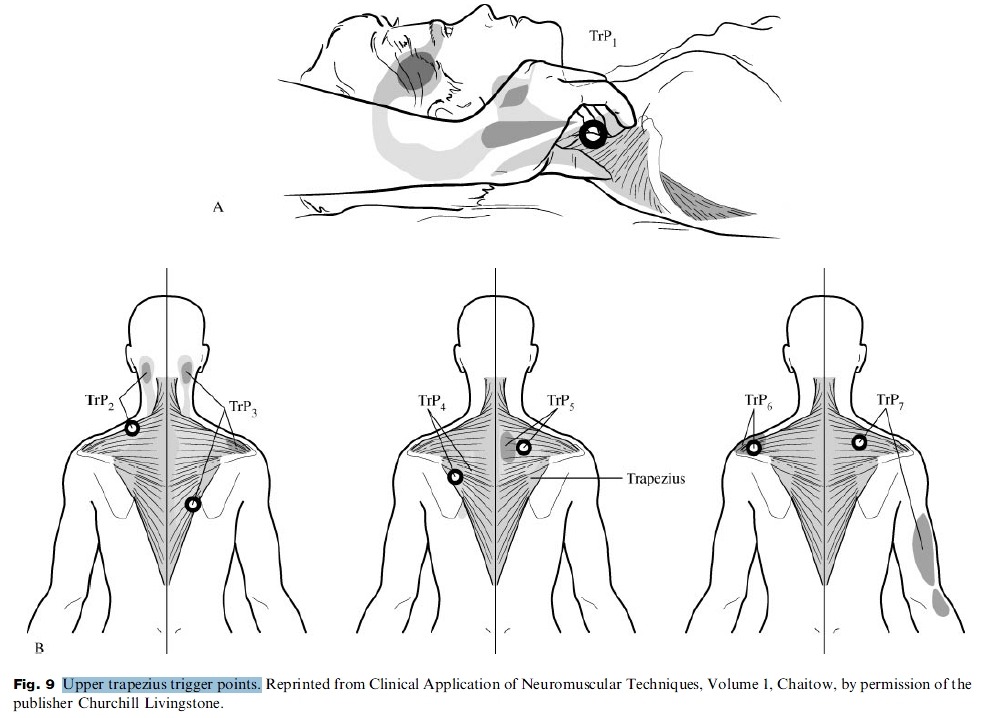
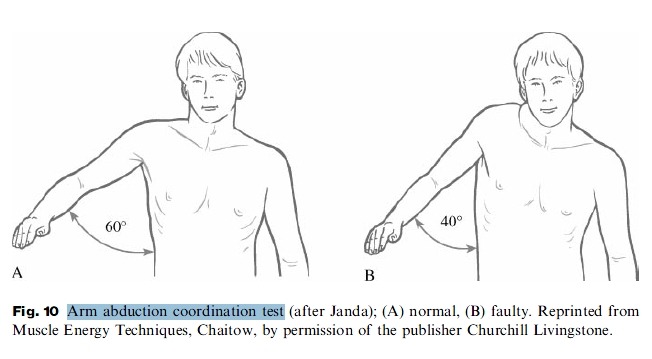
Pain referred from upper trapezius or pectoral muscles or GH joint is related to muscle imbalance involving shortened
pectorals combined with overactive upper trapezius and inhibited lower trapezius and dorsal erector spinae (Fig. 9A
& B). A simple screen is to perform the arm abduction test (Fig. 10).
- 상부승모근 또는 대흉근 또는 GH joint로부터의 referred pain은 overactive된 상부승모근과 억제된 하부승모근, 척추기립근과 연관된 짧아진대흉근과 관련된 muscle imbalance와 관련이 있음.
- simple screening test는 그림 10의 arm abduction test를 시행함.
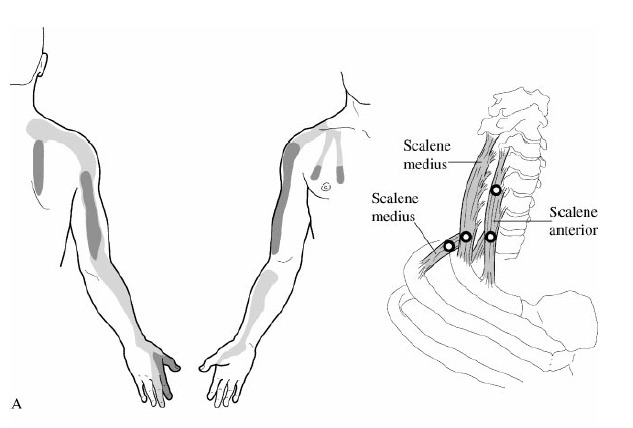
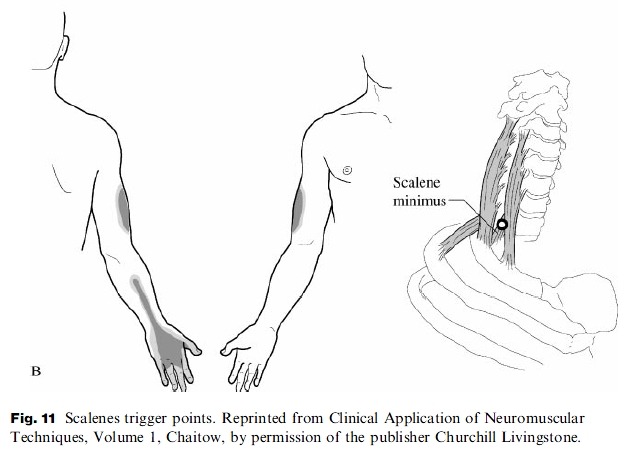
Pain referred from scalenes or upper trapezius muscles or upper ribs is related to muscle imbalance involving overactive
scalenes and upper trapezius combined with inhibition of the diaphragm (Fig. 11). A simple screen is to perform an evaluation of respiration during inhalation (Fig. 5).
- 사각근 또는 상부승모근, upper rib의 referred pain은 사각근과 상부승모근의 overactive와 관련됨. 흉곽의 억제와 함께
- simple screen 테스트는 그림 5와 같이 흡입동안 호흡을 평가하는 검사로 시행.
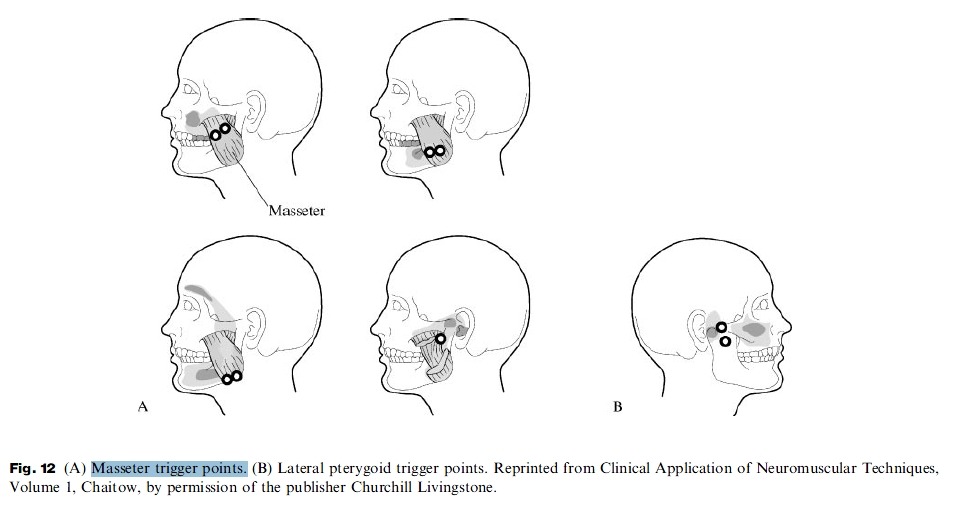
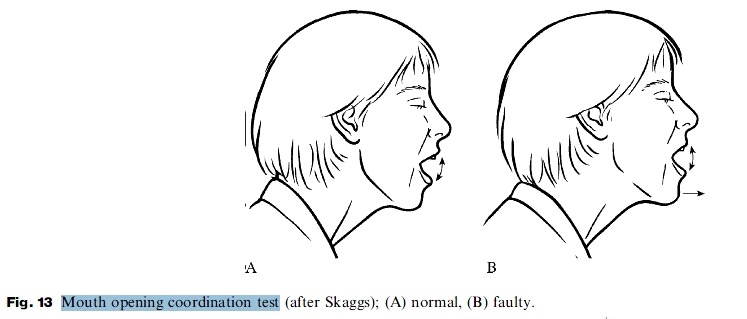
Pain referred from the masseter or lateral pterygoid muscles or the TMJ is related to shortened masseters and lateral pterygoids combined with inhibition of the digastricus (Fig. 12A & B). A simple screen is to perform the mouth opening test (Fig. 13).
- 교근과 외측 익돌근, TMJ의 referred pain은 짧아진 교근과 익돌근과 연관됨. 악이복근(digastricus) 억제와 combined된..
- simple screening test는 그림 13과 같이 mouth opening test를 시행.
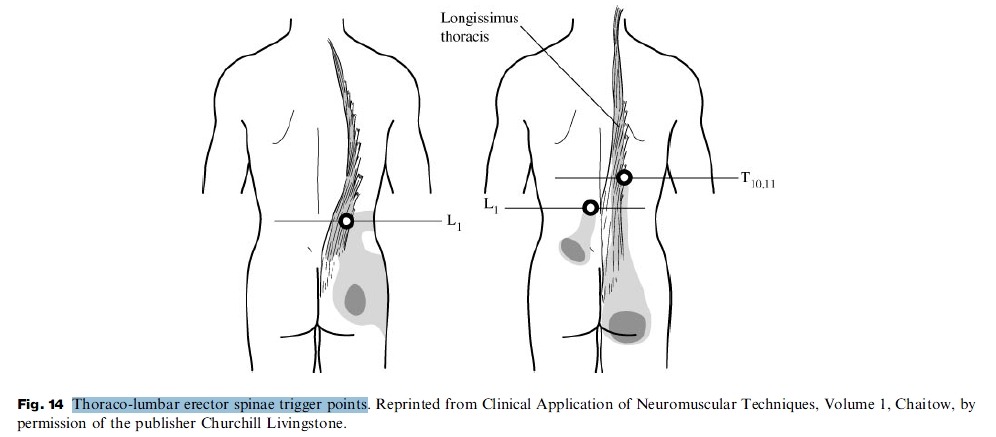
Pain referred from the T/L erector spinae muscle(s) or T10-L5 joints is related to overactivity of the T/L erector spinae combined with inhibition of the dorsal erector spinae (Fig. 14). A simple screen is to perform the standing arm elevation test (Fig. 15).
- T/L erector spinae muscle 또는 T10-L5 joint의 referred pain은 T/L erector spinae muscle의 overactivity와 연관됨. dorsal erector spinae의 억제와 combined되어.
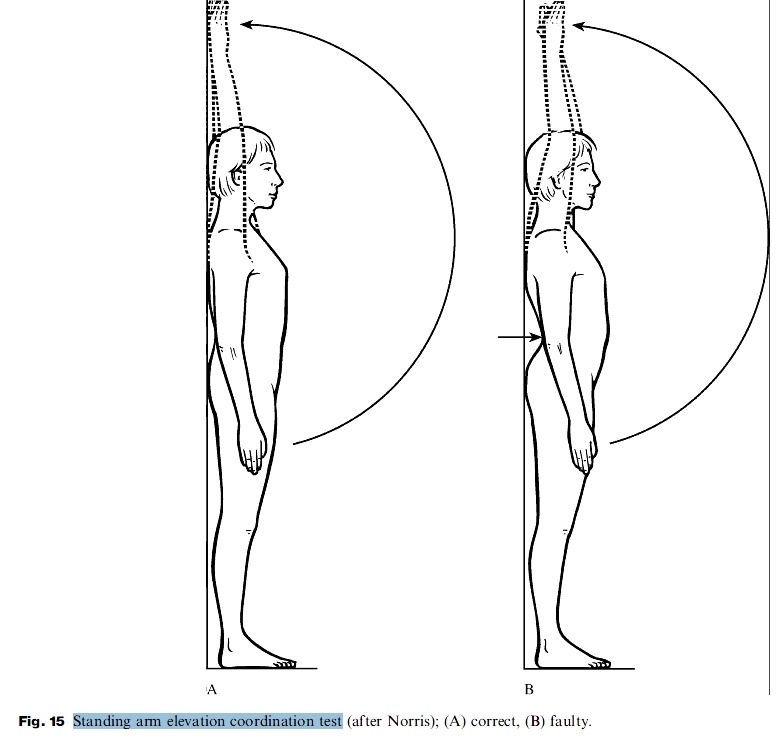
A simple functional test for evaluating mid-thoracic extension mobility is the standing arm elevation test (Fig. 15). To perform this test follow these steps:
. Patient stands with their buttocks and spine against a wall
. Feet are slightly forward (about 2 inches) - 1인치는 2.54cm임.
. Patient is instructed to raise arms directly in front and then all the way overhead
The test is + if:
. Lumbar lordosis :증가
. Arms don't reach the wall.
Summary
An examination of mid-dorsal kyphosis and related dysfunctions should be considered a routine part of the work-up for many pain syndromes. Such an evaluation can be customized based on the patient's presenting complaint and history. Mid-dorsal kyhphosis can be either a key perpetuating factor or underlying cause of pain generators such as the TMJ, shoulder, cervical spine or even low back. Part two of this series will discuss treatment of mid-thoracic dysfunction including patient advice, manipulation and exercise.
댓글
댓글 리스트-
답댓글 작성자문형철 작성자 본인 여부 작성자 작성시간 12.03.23 땡큐 ㅎㅎㅎ
-
작성자육동일 작성시간 13.02.18 T-L Spine이 kyphosis 되면서 L-spine의 exessive lordosis, Head forward posture 의 원인말고 L-spine의 Straigthening의 요인일 수 도 있나요 교수님..? 연세가 많으신 노인분들은 Stenosis를 동반한 L-spine의 exessive lordosis가 자주 보이는데 젊은 연령층에서는 L-spine의 exessive lordosis 보다는 오히려 Straigthening curvature를 동반한 HNP 소견이 더 자주 보이는 것 같아서 여쭤봅니다.
-
작성자송영석 작성시간 13.11.25 아주 좋은 자료네요.
- round shoulder와 상부승모근의 과활성화 => 충돌증후군(GH joint pain) : 상부승모근/견갑거근/하부승모근
- head forward posture => C0-C1 cervico-cranial junction(hyperextension)문제 : SCM/후두하근/ DNF
- chin protrusion => TMJ(입벌리기 감소) : 외익상근 / 교근/ 이복근
- sternosymphyseal approximation => 호흡능력 저하 : 사각근 / 대흉근 / 횡격막
- lumbar lordosis의 증가 => thoracolumbar erector spinae hypertrophy(척추기립근 과활성화) -
작성자09정문권 작성시간 14.02.19 head forward posture
chin protrusion
round shoulder
lumbosacral lordosis
mid thoracic kyphosis
>> 결국 머리-경추-턱-어깨-흉추-흉곽-(나아가서는 허리) 까지 하나의 complex로 이해가능(당연한 사실이기도..우리몸은 하나의 유기체니까)
>> 즉 어떤사람의 특정자세만 보고도 그 사람의 구조가 어떻게 변해갈지 예후판단가능
동시에 치료역시 어떤식으로 해나갈지에 대한 해답을 제시
해결책은 브뤼거호흡운동 + chin-in 등이 효과적 -
작성자장은석 작성시간 14.02.24 ★ mid-thoracic dysfunction
앉기 자세 → mid thoracic(T4-8)의 후만 → 직접적통증X But! 이차적 문제 초래
head forward posture, chin protrusion, round shoulder, 증가된 lumbo-sacral lordosis, sternum과 symphysis의 approximation. => mid thoracic kyphosis
- round shoulder와 상부승모근의 과활성화 => 충돌증후군
- head forward posture => C0-C1 cervico-cranial junction(hyperextension)문제
- chin protrusion => TMJ(입벌리기 감소)
- sternosymphyseal approximation => 호흡능력 저하
- lumbar lordosis의 증가 => 척추기립근 과활성화