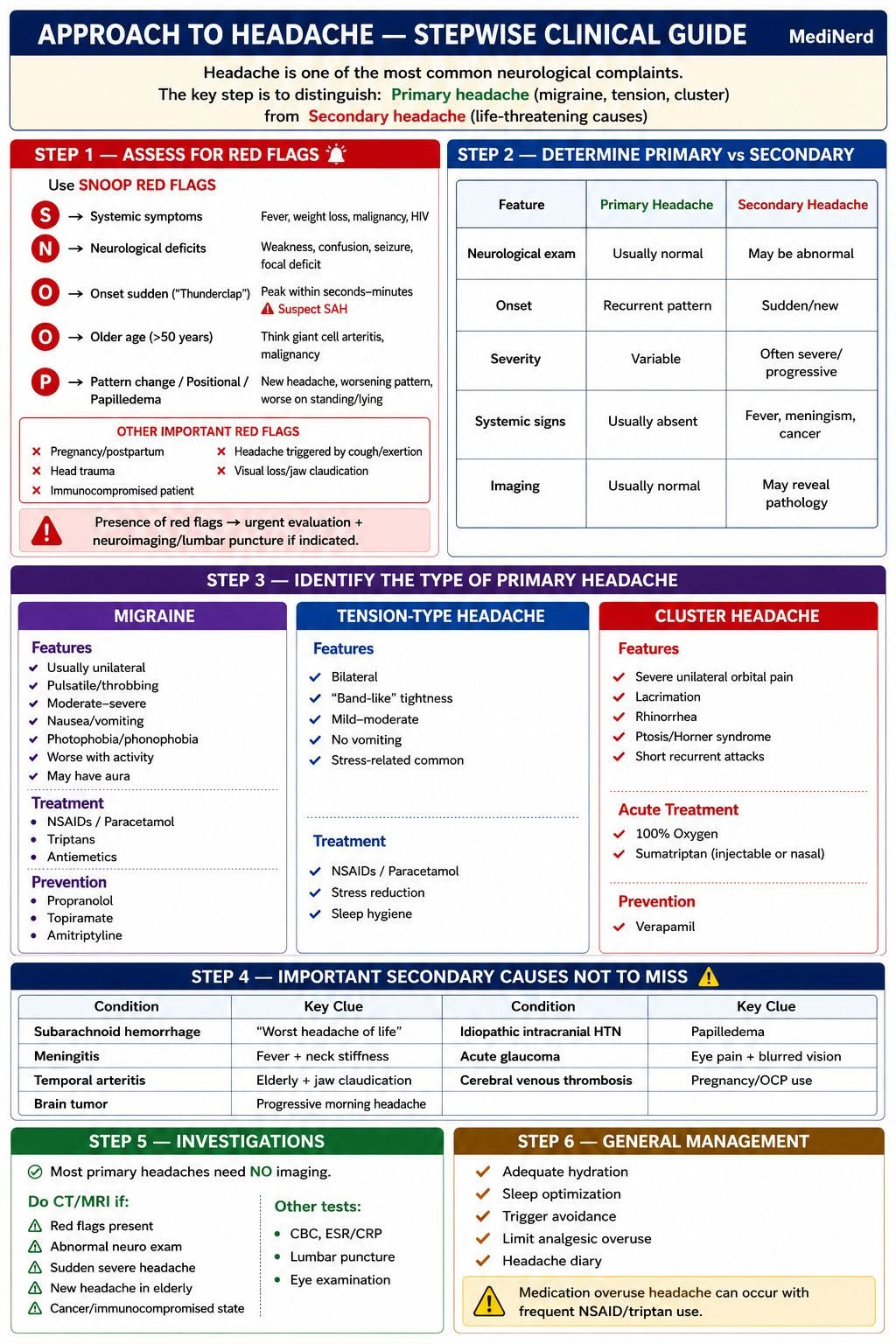
🧠 APPROACH TO HEADACHE — STEPWISE CLINICAL GUIDE
📌 Headache is one of the most common neurological complaints.
The key step is to distinguish:
✅ Primary headache (migraine, tension, cluster)
from
⚠️ Secondary headache (life-threatening causes)
━━━━━━━━━━━━━━━━━━━━
✅ STEP 1 — ASSESS FOR RED FLAGS 🚨
Use SNOOP RED FLAGS
🔴 S → Systemic symptoms
➡️ Fever, weight loss, malignancy, HIV
🔴 N → Neurological deficits
➡️ Weakness, confusion, seizure, focal deficit
🔴 O → Onset sudden (“Thunderclap”)
➡️ Peak within seconds–minutes
⚠️ Suspect SAH
🔴 O → Older age (>50 years)
➡️ Think giant cell arteritis, malignancy
🔴 P → Pattern change / Positional / Papilledema
➡️ New headache, worsening pattern, worse on standing/lying
⚠️ Other important red flags: ❌ Pregnancy/postpartum
❌ Head trauma
❌ Immunocompromised patient
❌ Headache triggered by cough/exertion
❌ Visual loss/jaw claudication
📌 Presence of red flags → urgent evaluation + neuroimaging/lumbar puncture if indicated.
━━━━━━━━━━━━━━━━━━━━
✅ STEP 2 — DETERMINE PRIMARY vs SECONDARY
Feature :Primary Headache➡️ Secondary Headache
Neurological exam: Usually normal ➡️ May be abnormal
Onset :Recurrent pattern ➡️ Sudden/new
Severity: Variable ➡️ Often severe/progressive
Systemic signs: Usually absent ➡️ Fever, meningism, cancer
Imaging: Usually normal ➡️ May reveal pathology
━━━━━━━━━━━━━━━━━━━━
✅ STEP 3 — IDENTIFY THE TYPE OF PRIMARY HEADACHE
🟣 MIGRAINE
📌 Usually: ✅ Unilateral
✅ Pulsatile/throbbing
✅ Moderate–severe
✅ Nausea/vomiting
✅ Photophobia/phonophobia
✅ Worse with activity
⚡ May have aura
Treatment
💊 NSAIDs / Paracetamol
💊 Triptans
💊 Antiemetics
Prevention
💊 Propranolol
💊 Topiramate
💊 Amitriptyline
━━━━━━━━━━━━━━━━━━━━
🔵 TENSION-TYPE HEADACHE
📌 Features: ✅ Bilateral
✅ “Band-like” tightness
✅ Mild–moderate
✅ No vomiting
✅ Stress-related common
Treatment
💊 NSAIDs / Paracetamol
💊 Stress reduction
💊 Sleep hygiene
━━━━━━━━━━━━━━━━━━━━
🔴 CLUSTER HEADACHE
📌 Features: ✅ Severe unilateral orbital pain
✅ Lacrimation
✅ Rhinorrhea
✅ Ptosis/Horner syndrome
✅ Short recurrent attacks
Acute Treatment
💨 100% Oxygen
💉 Sumatriptan
Prevention
💊 Verapamil
━━━━━━━━━━━━━━━━━━━━
✅ STEP 4 — IMPORTANT SECONDARY CAUSES NOT TO MISS ⚠️
Condition: Key Clue
Subarachnoid hemorrhage: “Worst headache of life”
Meningitis: Fever + neck stiffness
Temporal arteritis : Elderly + jaw claudication
Brain tumor: Progressive morning headache
Idiopathic intracranial HTN: Papilledema
Acute glaucoma : Eye pain + blurred vision
Cerebral venous thrombosis: Pregnancy/OCP use
━━━━━━━━━━━━━━━━━━━━
✅ STEP 5 — INVESTIGATIONS
📌 Most primary headaches need NO imaging.
Do CT/MRI if:
⚠️ Red flags present
⚠️ Abnormal neuro exam
⚠️ Sudden severe headache
⚠️ New headache in elderly
⚠️ Cancer/immunocompromised state
Other tests:
🧪 CBC, ESR/CRP
🧪 Lumbar puncture
🧪 Eye examination
━━━━━━━━━━━━━━━━━━━━
✅ STEP 6 — GENERAL MANAGEMENT
✅ Adequate hydration
✅ Sleep optimization
✅ Trigger avoidance
✅ Limit analgesic overuse
✅ Headache diary
⚠️ Medication overuse headache can occur with frequent NSAID/triptan use.
━━━━━━━━━━━━━━━━━━━━
🎯 QUICK EXAM PEARLS
🧠 Migraine → unilateral + throbbing + nausea
🧠 Tension → bilateral “tight band”
🧠 Cluster → unilateral eye pain + autonomic symptoms
🧠 Thunderclap headache → rule out SAH first