🦴 APPROACH TO RHEUMATOID ARTHRITIS (RA) — STEPWISE CLINICAL GUIDE
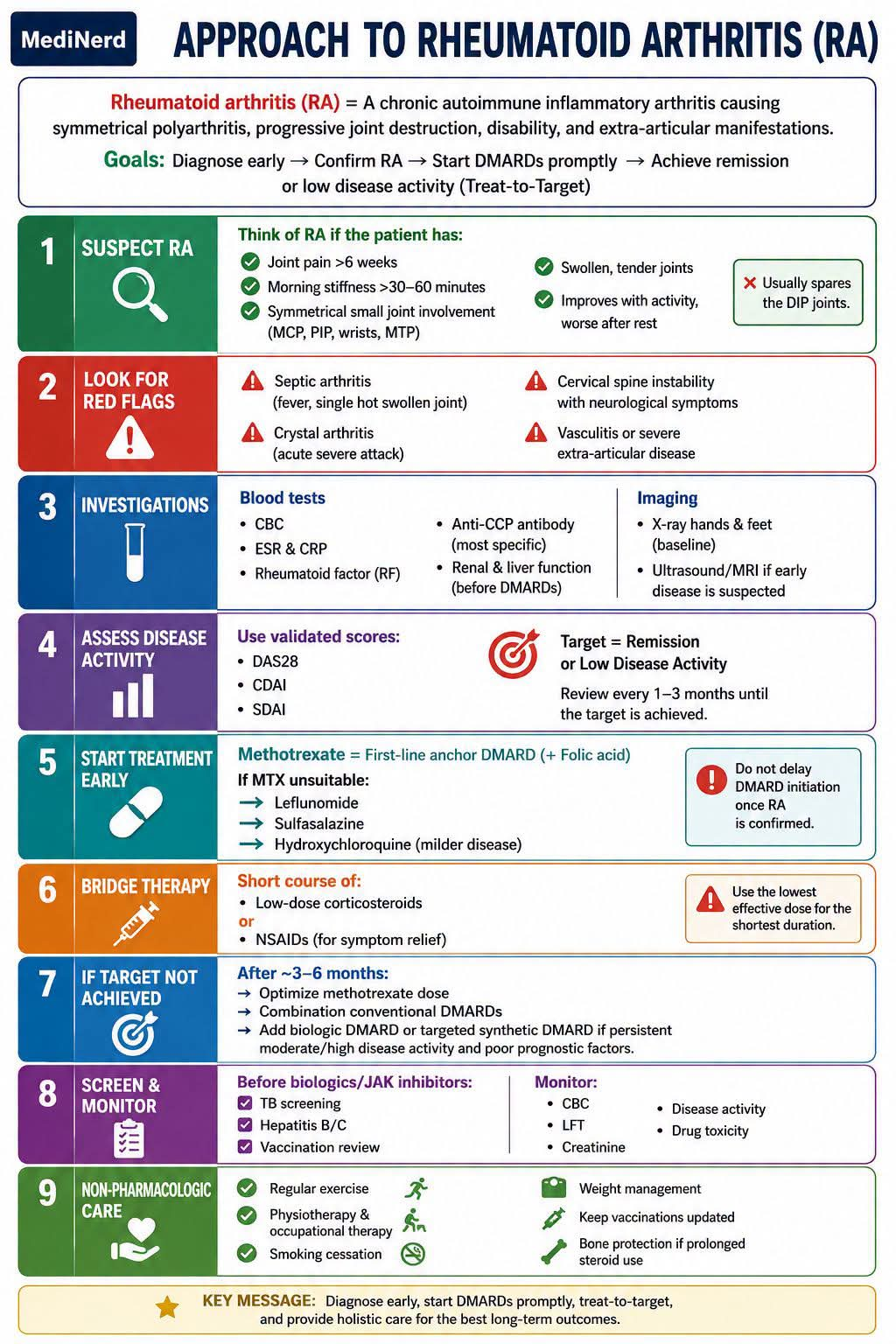
📌 Rheumatoid arthritis (RA) = A chronic autoimmune inflammatory arthritis causing symmetrical polyarthritis, progressive joint destruction, disability, and extra-articular manifestations.
🎯 Goals: Diagnose early → Confirm RA → Start DMARDs promptly → Achieve remission or low disease activity (Treat-to-Target)
━━━━━━━━━━━━━━━━━━
✅ STEP 1 — SUSPECT RA
Think of RA if the patient has:
✅ Joint pain >6 weeks
✅ Morning stiffness >30–60 minutes
✅ Symmetrical small joint involvement (MCP, PIP, wrists, MTP)
✅ Swollen, tender joints
✅ Improves with activity, worse after rest
🚫 Usually spares the DIP joints.
━━━━━━━━━━━━━━━━━━
✅ STEP 2 — LOOK FOR RED FLAGS
🚨 Septic arthritis (fever, single hot swollen joint)
🚨 Crystal arthritis (acute severe attack)
🚨 Cervical spine instability with neurological symptoms
🚨 Vasculitis or severe extra-articular disease
━━━━━━━━━━━━━━━━━━
✅ STEP 3 — INVESTIGATIONS
🩸 Blood tests • CBC • ESR & CRP • Rheumatoid factor (RF) • Anti-CCP antibody (most specific) • Renal & liver function (before DMARDs)
🩻 Imaging • X-ray hands & feet (baseline) • Ultrasound/MRI if early disease is suspected
━━━━━━━━━━━━━━━━━━
✅ STEP 4 — ASSESS DISEASE ACTIVITY
Use validated scores:
📊 DAS28
📊 CDAI
📊 SDAI
🎯 Target = Remission or Low Disease Activity
Review every 1–3 months until the target is achieved.
━━━━━━━━━━━━━━━━━━
✅ STEP 5 — START TREATMENT EARLY
💊 Methotrexate = First-line anchor DMARD (+ Folic acid)
If MTX unsuitable:
➡️ Leflunomide
➡️ Sulfasalazine
➡️ Hydroxychloroquine (milder disease)
⚠️ Do not delay DMARD initiation once RA is confirmed.
━━━━━━━━━━━━━━━━━━
✅ STEP 6 — BRIDGE THERAPY
Short course of:
💉 Low-dose corticosteroids
or
💊 NSAIDs (for symptom relief)
⚠️ Use the lowest effective dose for the shortest duration.
━━━━━━━━━━━━━━━━━━
✅ STEP 7 — IF TARGET NOT ACHIEVED
After ~3–6 months:
➡️ Optimize methotrexate dose
➡️ Combination conventional DMARDs
➡️ Add biologic DMARD or targeted synthetic DMARD if persistent moderate/high disease activity and poor prognostic factors.
━━━━━━━━━━━━━━━━━━
✅ STEP 8 — SCREEN & MONITOR
Before biologics/JAK inhibitors:
✔ TB screening
✔ Hepatitis B/C
✔ Vaccination review
Monitor:
• CBC
• LFT
• Creatinine
• Disease activity
• Drug toxicity
━━━━━━━━━━━━━━━━━━
✅ STEP 9 — NON-PHARMACOLOGIC CARE
🏃 Regular exercise
🦴 Physiotherapy & occupational therapy
🚭 Smoking cessation
⚖ Weight management
💉 Keep vaccinations updated
🦷 Bone protection if prolonged steroid use
━━━━━━━━━━━━━━━━━━
📝 MediNerd Pearls
🔹 Early diagnosis + early DMARD = Better long-term outcomes.
🔹 Anti-CCP positivity predicts more aggressive disease.
🔹 Treat to remission, not just pain relief.
🔹 Steroids are bridging therapy, not long-term treatment.
🔹 Monitor drug toxicity regularly and adjust therapy based on disease activity.
#MediNerd #RheumatoidArthritis #Rheumatology #medicine