
무엇이 치료인가?
어디를 치료할 것인가?
어떻게 치료할 것인가?
이것을 알기 위해서 우리는 "인체의 어디에서 문제가 되어 어떤 길을 거쳐 뇌가 어떻게 통증을 느끼는가"를 알아야 한다.
오늘의 주제는 통증의 pathway이다.
간단하게 정리하면
물리적 자극(overuse, overcompression, overtraction 등), 화학적 자극(화상 등), 병리적자극(자가면역, 통풍 등)에 의하여 인체의 조직은 염증(inflamation)이 발생하여 통각 수용기(free nerve ending)를 자극하면 nerve에서 전기적 에너지로 척수에 전달, synaps를 통해 화학적자극으로 바뀌고, 다시 spinothalamic tract를 전기적 에너지로 바뀌어 hypothalmus시상하부로 전달되고 대뇌의 sensory area(감각영역)으로 전달된다. 대뇌에서는 전기에너지를 마음(아프다는 감정)으로 변환된다.
더 간단하게 정리하면
어떤 자극에 의해 인체의 조직은 염증이 발생하고, 신경의 길을 따라 척수에 전달되고 spinothalamic tract, 시상하부를 거쳐 대뇌에서 통증을 느끼게 된다.
책으로 소개하면 "의학신경 해부학"
인터넷 사이트를 소개하면 http://anatomy.yonsei.ac.kr/neuro-web/
panic bird....
자세하게 그림으로 정리하면
1. free nerve ending

| Touch | ||||||||||||||
| ||||||||||||||





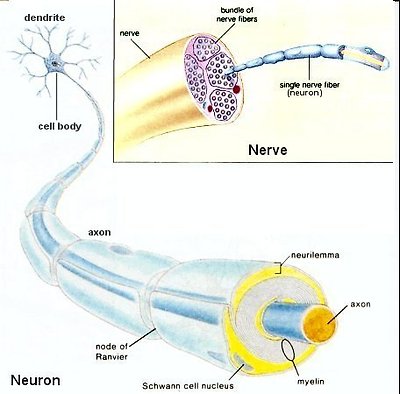
2. nerve
- 염증이라는 화학적 자극이 전기적에너지로 바뀌어 nerve를 따라 척수(spinal cord)로 전달된다.
transport - neuron의 cell body에서 만들어진 신경전달물질, 에너지 등이 전달되는 과정 또는 nerve의 말단에서 사용하고 남은 찌꺼기 등을 cell body로 전달시키는 과정

|
1. 투불린(tubulin) |
|
2. 카이네신(kinesin) |
|
3. 용해소체이전소포 |
|
4. 시냅스이전소포 |
|
5. 다이네인(dynein) |
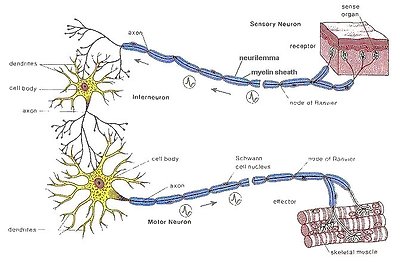
3. spinal cord
- 신경을 따라 전달된 전기에너지는 synapse에서 신경전달물질의 화학적과정을 거치며 다시 전기에너지로 변형되어 교차하여 spinothalamic tract을 따라 시상하부로 전달

|
1. 일반체원심성분(GSE) |
6. 후근(posterior root) |
|
2. 일반내장원심성분(GVE) |
7. 전근(anterior root) |
|
3. 일반내장구심성분(GVA) |
8. 교감신경절(sympathetic ganglion) |
|
4. 일반체구심성분(GSA) |
9. 백색교통가지(white rami communicantes) |
|
5. 척수신경절(spinal ganlion) |
10. 회색교통가지(gray rami communicantes) |
synapse

|
1. 시냅스이전부분(presynaptic portion) |
|
2. 시냅스틈새(synaptic cleft) |
|
3. 시냅스이후부분(postsynaptic portion) |
|
4. 시냅스소포(synaptic vesicle) |
|
5. 미토콘드리아(mitochondria) |
|
6. 시냅스이전치밀질(presynaptic density) |
|
7. 시냅스이후치밀질(postsynaptic density) |

|
A. 후각(posterior horn) |
|
B. 그물형성체(reticular formation, 망상체) |
|
C. 시상(thalamus, VPLc) |
|
1. 신척수시상로(neospinothalamic tract) |
|
2. 구척수시상로(paleospinothalamic tract) |
|
3. 방사관(corona radiata)
|
그림 5-23. 척수시상로(spinothalamic tract)의 경로.

|
A. 후각(posterior horn) |
|
B. 그물형성체(reticular formation, 망상체) |
|
C. 시상(thalamus, VPLc) |
|
1. 신척수시상로(neospinothalamic tract) |
|
2. 구척수시상로(paleospinothalamic tract) |
|
3. 방사관(corona radiata) |
그림 5-25. 입체적으로 나타낸 척수시상로(spinothalamic tract).
hypothalamus(시상하부)
- 통증, 촉각, 냉각, 열각, 진동각, 두점분별감각 등을 각각의 영역을 거쳐 뇌로의 전달

|
1. 일차체감각영역(S I)과 이차체감각영역(S II) |
2. 일차운동영역(M I)과 전운동영역(premotor area) |
|
3. 보완운동영역(supplementary motor area, SMA) |
4. 전전두엽피질(prefrontal cortex)과 |
|
5. 흑색질(substantia nigra)의 |
6. 창백핵(globus pallidus)의 |
|
7. 소뇌시상로(cerebellothalamic tract)와 |
8. 배쪽 및 등쪽삼차시상로(ventral and |
|
9. 내측섬유띠(medial lemniscus)와 |
그림 8-5. 시상 배쪽핵군(ventral nuclear group)의 주요 연결
대뇌에서의 감각인지

그림 11-8. 감각호문쿨루스(sensory homunculus).
Figure 2: Pain pathways I

Pain fibres terminate mainly in the superficial dorsal horn (laminae I- II). Ad fibres enter lamina I (and V) and synapse on a second set of neurons. These neurons will carry the signal to the thalamus and are part of the spinothalamic tract (STT). The C fibres enter the spinal cord and synapse on lamina I cells and lamina II interneurons - neurons that make synaptic connections with other cells within the local environment. The interneurons convey the signal to the STT cells that reside mainly in laminae I, IV and V. The axons of the STT cells project across the spinal cord to the STT, which is located in the ventrolateral quadrant of the contralateral spinal cord white matter.
Figure 3: Temperature and pain pathways II

The STT transmits information about temperature and pain, as well as “simple” touch (i.e. related to localisation of stimulus) and visceral sensations. It mediates the discriminative and arousal-emotional components of these sensations by separating out the “fast” (discriminative aspect) and “slow” (affective aspect) components of pain into different regions of the tract that are transmitted in parallel to the thalamus. Discriminative pain reaches the thalamus directly without making connections elsewhere in the nervous system, whereas arousal-emotional pain reaches the thalamus indirectly via connections with brainstem regions. Slow pain is also transmitted by other pathways such as the spinoreticular tract.
The STT may be divided into the lateral STT and the anterior STT. Pain and temperature is transmitted mainly in the lateral STT. The lateral-STT transmits the sensations of both fast and slow pain. The anterior STT conveys sensations of simple touch (stimulus localisation). The STT ascends the entire length of the cord and the brainstem, staying in about the same location all the way up. It is here in the brainstem that the different modalities separate out to terminate in different thalamic and brainstem nuclei. The fast pain STT axons terminate in the ventroposterior nucleus, which comprises the ventral posterolateral (VPL) and ventral posteromedial (VPM) and the posterior (PO) nuclei. These axons seem to mediate mainly the sense of “simple touch” and pain. These sensations are separated within the thalamus: neurons in the VPL and VPM do not respond specifically to noxious stimulation, whereas cells in the PO receive inputs from both low- and high-threshold afferents. These cells are associated with the conscious perception of pain.
The slow pain-STT axons innervate the non-specific intralaminar nuclei of the thalamus, and the reticular formation in the brainstem. These axons form at least part of the forebrain pain pathway associated with the affective quality (unpleasantness and fear of further injury) of pain and can be dissociated from the discriminative quality (the type and nature of the injury itself). The projections to the reticular formation may underlie the arousal effects of painful stimuli. The arousal itself may activate noradrenergic neurons in the locus coeruleus, and thus decrease the upward pain transmission. This may be an example of a negative feedback loop in the nervous system.
Table 2: Comparison of central pathways for pain transmission
|
Direct (fast) |
Indirect (slow) | |
|
Tract |
Lateral-STT |
Lateral-STT Spinoreticular tract (SRT) |
|
Origin |
Lamina I & IV, V |
Lamina I, IV,V, (and VII, VIII) |
|
Somatotopic organisation |
Yes |
No |
|
Body representation |
Contralateral |
Bilateral |
|
Synapse in reticular formation |
No |
Yes |
|
Sub-cortical targets |
None |
Hypothalamus Limbic system Autonomic centres |
|
Thalamic nucleus |
Ventral posterolateral (VPL) |
Intra-laminar nuclei Other midline nuclei |
|
Cortical location |
Parietal lobe (SI cortex) |
Cingulate gyrus |
|
Role |
Discriminative pain (quality intensity, location) |
Affective-arousal components of pain |
|
Other functions |
Temperature Simple touch |
It has long been known that the STT is an important pain pathway because when it is damaged, pain and temperature sense is abolished on the contralateral side of the body below the lesion. It has been used, as a last resort, by surgeons to relieve intractable cancer pain. However, pain is not permanently abolished because of preservation of one side of the bilateral indirect pathways. Also, the transmission of simple tactile modalities (detection, location) via the anterior STT explains why touch sensation is preserved in people with dorsal column lesions (although they are unable to discriminate the nature of the stimulus).