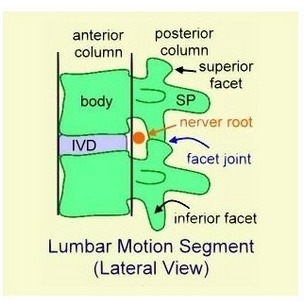
facet joint는 synovial joint이고 lumbar의 posterior portion에 위치하고 요추의 수동안정화 구조물로 중요한 역할을 한다.
어떤 원인(허리디스크, 척추골반의 부정렬 등)에 의해 요추의 ant portion에 걸려야할 부하가 post portion에 주어지기 시작하면
Lumbar Facet Joint syndrome이 발생하고 진행하면 Osteoarthritis가 된다.
찾아야할 생체역학 - facet joint에 걸리는 부하는 척추 신전시 최대 30%!
이러한 기본 역학의 이해를 바탕으로 아래 논문을 읽어야 한다.
궁극적인 치료는 비정상적인 부하가 post portion에 걸리는 것을 정상적으로 ant portion으로 옮겨지게 하는 것이다.
간단한 정리
1. Lumbar FJ contain hyaline cartilage, synovial membrane, fibrous capsule, and a joint space with a potential capacity of 1 to 2 mL
2. The FJ play an important role in load transmission; they provide a posterior load-bearing helper, stabilizing the motion segment in flexion and extension and also restricting axial rotation.
![]() Lumbar Facet Joint Osteoarthritis.pdf
Lumbar Facet Joint Osteoarthritis.pdf
Objectives: The facet joints (FJ) can be a potentially important source of symptoms because of the high level of mobility and load forces, especially in the lumbar area. We reviewed the anatomy, biomechanics, and possible sources of pain of the FJ, natural history, and risk factors of lumbar FJ osteoarthritis and briefly reviewed the relevant imaging methods.
Methods: PubMed and MEDLINE databases (1950-2006) were searched for the key words “facet joints,” “zygapophyseal joints,” “osteoarthritis,” “low back pain,” and “spondyloarthritis.” All relevant articles in English were reviewed. Pertinent secondary references were also retrieved.
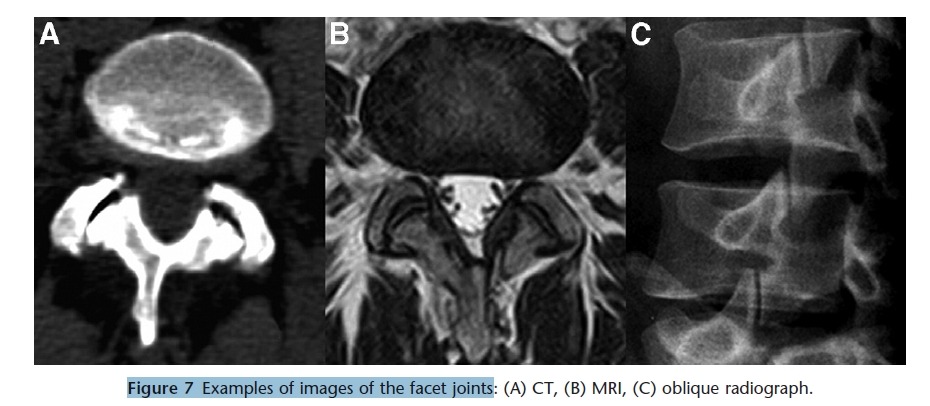
Results: The FJ play an important role in load transmission; they provide a posterior load-bearing helper, stabilizing the motion segment in flexion and extension and also restricting axial rotation. The capsule of the FJ, subchondral bone, and synovium are richly innervated and can be a potential source of the low back pain. Degenerative changes in the FJ comprise cartilage degradation that leads to the formation of focal and then diffuse erosions with joint space narrowing, and sclerosis of the subchondral bone. Because the most prominent changes occur in bone, the best method of evaluation of the FJ is computed tomography. Risk factors for lumbar FJ osteoarthritis include advanced age, relatively more sagittal orientation of the FJ, and a background of intervertebral disk degeneration.
Conclusions: An up-to-date knowledge of this subject can be helpful in the development of diagnostic techniques and in the prevention of lumbar FJ osteoarthritis and low back pain and can assist in the determination of future research goals.
Anatomy and Biomechanics
A fuller understanding of the FJ can only be appreciated by considering their anatomy and unique biomechanics.
This knowledge assists in our understanding of their imaging findings and more importantly the predilection for
OA in FJ given the loads imparted through them.
The lumbar facet (zygapophyseal) joints are paired, true synovial joints that comprise the posterolateral articulation
between vertebral levels (Fig. 1).
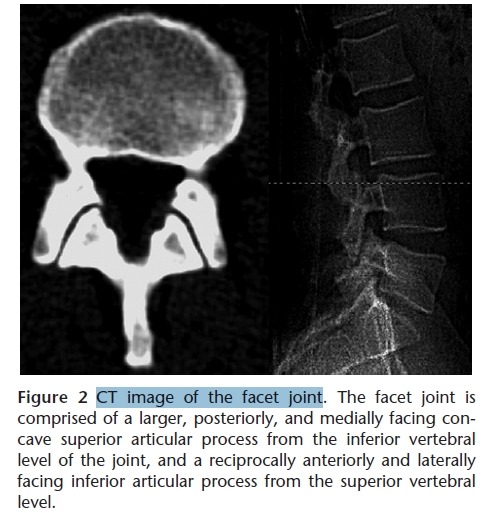
Each joint comprises a larger, posteriorly, and medially facing concave superior articular process from the inferior vertebral level of the joint and a reciprocally anteriorly and laterally facing inferior articular process from the superior vertebral level (Fig. 2).
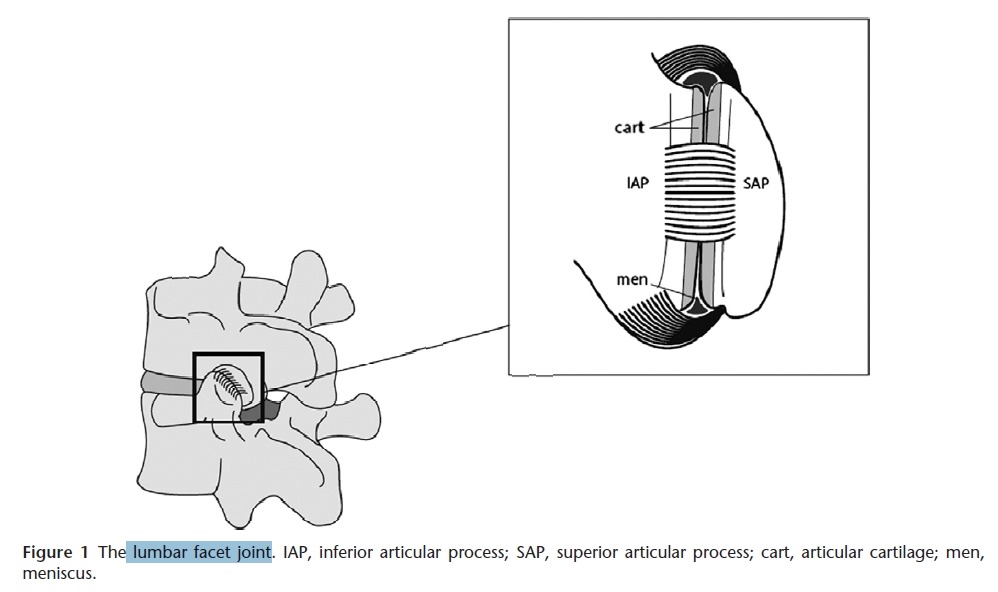
Each joint’s morphology approximates somewhere between a “C” and “J” shape (13). Lumbar FJ contain hyaline cartilage, synovial membrane, fibrous capsule, and a joint space with a potential capacity of 1 to 2 mL (14). The existence of menisci (meniscoids) in the lumbar FJ has been emphasized in numerous publications (15-17). Two types of joint inclusions have been demonstrated:
(1) fat-filled synovial reflections at the superior and inferior poles of the joint;
(2) rudimentary fibrous invaginations arising from the dorsal and ventral portions of the capsule (16,18).
Those menisci serve to compensate for the incongruence of articular surfaces and to fill in empty spaces (19). Kos and coworkers (19,20) proposed that mobile, peduncular meniscoids can, at sudden or nonphysiological movements, be caught between articular surfaces and cause spinal blockade and painful conditions.
However, Bogduk and Engel (18) have indicated that the small size of menisci make entrapment unlikely. Panjabi and coworkers (21) reported a clear tendency toward an increase in the cartilaginous area of the facets in the lower lumbar segment. Similarly, the inner capsular
area also displayed a pattern of an increase from L1-2 to
L5-S1; thus, larger facets were more likely to carry wider
capsules (22). The fibrous capsule of the FJ is 1 mm thick
and attaches 2 mm from the articular margins (23,24).
The capsule serves to limit rotation (22,25,26) and resists
a backward sliding motion during extension (23).
Adaptation of the human spine to the upright position
throughout evolution included the development of vertebral
curvatures (mainly thoracic kyphosis and lumbar lordosis)
requiring alteration of articular facet orientation
(27). Articular facet orientation can be important in providing
stability to the spine and controlling its motion
under complex loading in the upright bipedal human
mechanism. The orientation of the FJ in a transverse
plane varies from the upper level of the lumbar spine to
the lower 1 (13). The lumbar facets are generally sagittally
oriented (Fig. 2). The facets of T12-L2 are oriented closer
to the midsagittal plane of the vertebral body (mean
range, 26-34°), while the facets of L3-L5 are oriented
away from that plane (mean range, 40-56°) (28). The
oblique orientation of the facets contributes to many spinal
functions, such as resistance to intervertebral shear
forces, compressive forces, and intervertebral torsion
(29,30). Sagittal orientation of the FJ allows greater range
of flexion and limits axial rotation in the lumbar region
(31). In the sagittal plane all lumbar FJ are oriented at
approximately 170° to vertical (21,28). The orientation ethnic group (28).
The influence of age on orientation of the FJ remains
controversial. Love and coworkers (32) found that older
adults both with and without degenerative spondylolisthesis
(that usually is secondary to FJ degeneration (33))
had a significantly greater mean sagittal angle of the FJ
than those in the younger group. They consider this angle
increasingly to be the result of arthritic remodeling because
the capacity for wear to change the characteristics of
a joint is commonly seen elsewhere in the body, and it
seems unlikely that the FJ would react differently. Other
investigators (28,34), however, did not find any association
between age and FJ orientation.
From a biomechanical point of view, the FJ play an
important role in load transmission; they provide a posterior
load-bearing helper, stabilizing the motion segment
in flexion and extension, and they are also involved in the
mechanism of rotational kinematics by restricting the axial
rotation (30). They are designed to block axial rotation
and forward sliding of the lumbar vertebrae. By blocking
forward slide, they prevent the vertebral bodies from dislocating
under the weight of the trunk when the spine is
flexed forward (35). In a normal healthy spinal unit, the
lumbar spine transmits loads between each intervertebral
level through the vertebral bodies and intervertebral disc
(anterior column) and 2 FJ (30,36,37). Under normal
conditions, between 3 and 25% of segmental load are
transmitted over the FJ; this percentage increases up to
47% in degenerative facets (38,39). The percentage of
load transferred through the posterior elements is also
highly dependent on spinal posture (39) and increases
during spine extension (39-42).
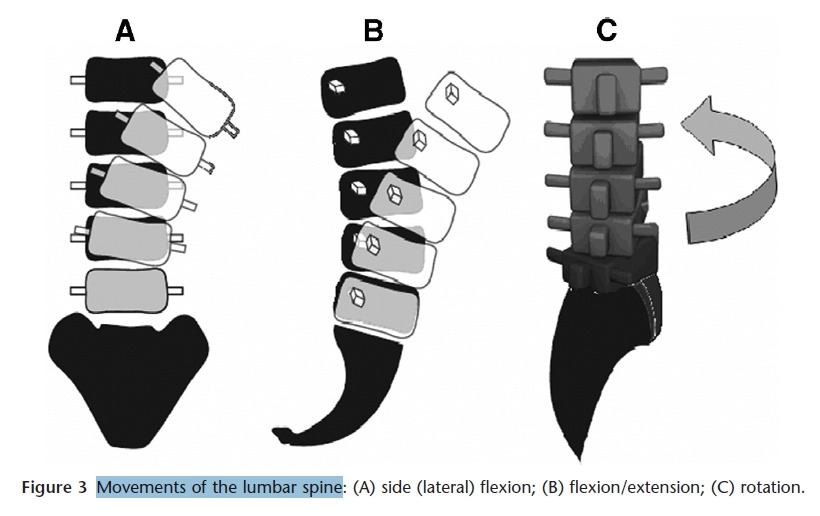
Mobility of the lumbar spine (Fig. 3) is greatest during flexion/extension movements (cumulative mobility in segments L1-5: 57°) and more limited during lateral bending (L1-5: 26°) and axial rotation (L1-5: 8°) (31).
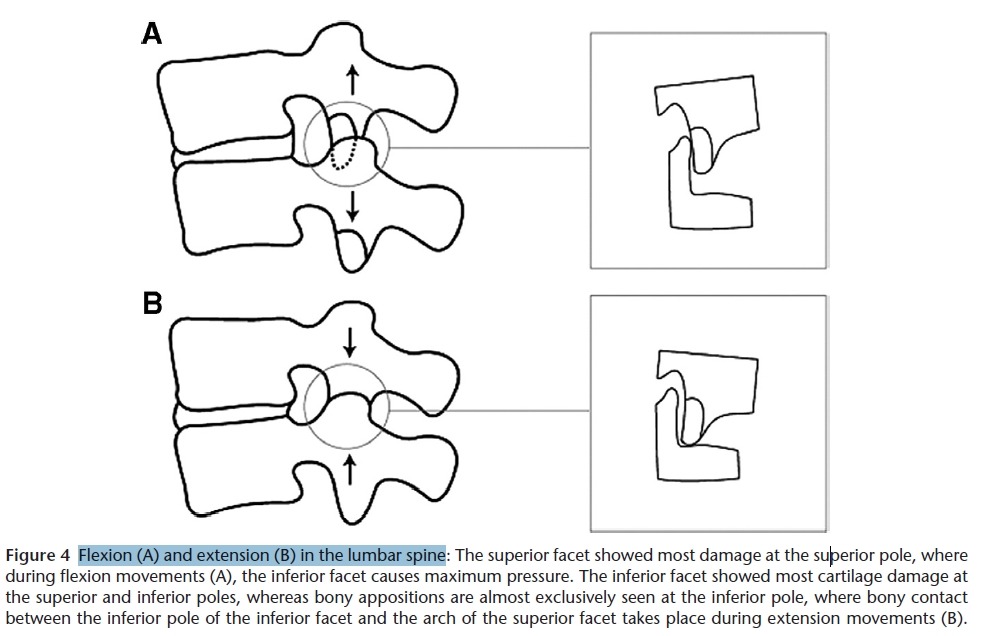
The wide range of flexion/extension movement in the lumbar spine causes physiological gaping of the FJ in the
final phases of movements, and this can lead to maximum pressure on the lower edge of the inferior facet during
extension and on the upper edge of the superior facet during flexion (30,39,43) (Fig. 4).
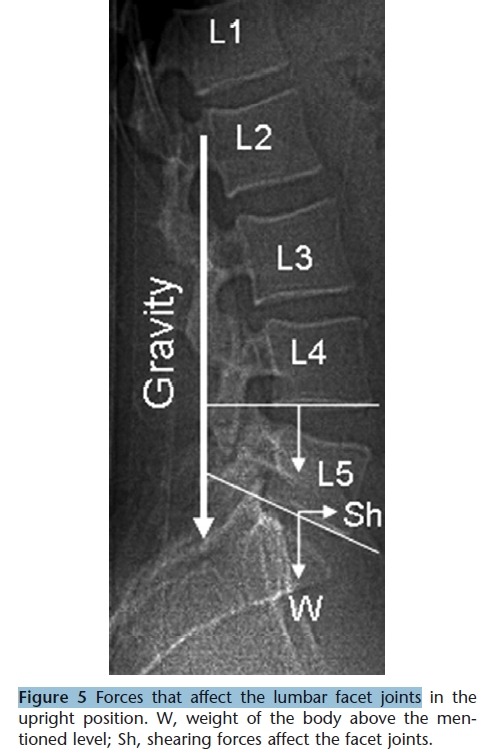
In an upright position there are continuous forward shear forces applied to the FJ between the 5th lumbar vertebra and sacrum (Fig. 5) because of lumbar lordosis. During flexion, these forces increase and also appear in higher levels of the spine above L5-S1. In lower segments of the spine, these shearing forces are higher because of the higher weight of the body above this level and because of the longer leverage of the center of body mass. Therefore, the aforementioned tendency toward the increasing cartilaginous area of the facets in the lower lumbar segment (21) seems to be a normal
consequence of Wolf’s law (44). The more coronal orientation of the FJ in lower spinal segments (28) may also be an adaptation to the shearing forces influencing the lower back.
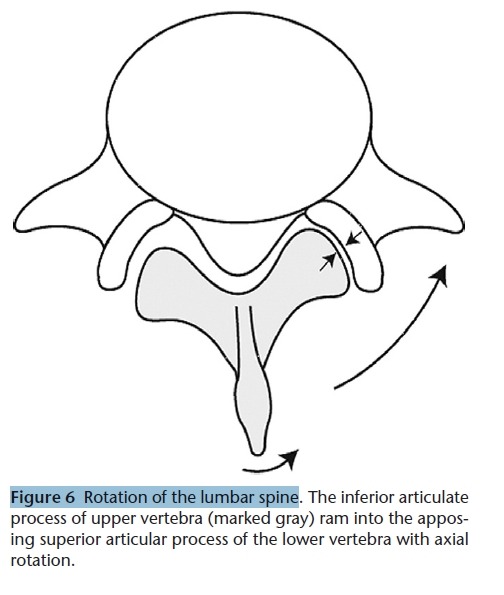
Axial rotation of the lumbar vertebrae occurs around a longitudinal axis that passes through the posterior third of
the vertebral bodies and intervertebral discs. During this rotation, the posterior elements of the moving upper vertebra
swing laterally, in a direction opposite to that of the rotation. With this movement the inferior articulate process of this vertebra will ram into the apposing superior articular process of the lower vertebra (Fig. 6). This mechanism of axial rotation blocking protects the intervertebral discs from excessive torsion (35).
Pain Originates from the Facet Joints
Each lumbar FJ is innervated by the medial branches of the primary dorsal rami from that level and the level above
(45,46). For example, the FJ L4-L5 are innervated by both the L4 and the L3 medial branches. The L1-L4 medial branches of the dorsal rami run across the superior portion of the subjacent transverse process, under the mamillo-accessory ligament at the junction of the superior articular process and the root of the transverse process, and then onto the lamina. On the lamina, the nerve divides, giving off branches to the FJ below, the joint at that level, the interspinous ligament and muscle, and the multifidus muscle. The L5 dorsal ramus runs in the groove between the superior articular process of S1 and the sacral ala (13,47,48). The medial branch of L5 divides from the dorsal ramus of L5 at the inferior aspect of the FJ L5-S1. A communicating branch from the S1 posterior ramus may travel from the superior edge of the posterior S1 foramen up to the inferior margin of the FJ L5-S1 (48). The capsule of the FJ is richly innervated with nociceptive and autonomic nerve fibers (49-51). Mechanoreceptors have been demonstrated in rabbit FJ capsules (52,53) and substance P innervation has been isolated in degenerative FJ subchondral bone (54). The synovium may contain nociceptors (49,50), although these synovial nerves may serve only to regulate blood flow (55,56).
FJ have been mentioned in the medical literature as a source of low back and lower extremity pain since 1911(57). The fact that pain can originate from the FJ is widely accepted in the radiologic and orthopedic literature (58-66). This is supported by investigations employing successful intra-articular or peri-articular joint blocks (58,64). Estimates of the prevalence of lumbar FJ pain have ranged from 7 to 75% among patients reporting back pain. On the basis of controlled, comparative, local anesthetic diagnostic blocks, the prevalence in the United States of lumbar FJ pain in patients with chronic LBP has been established as 15% in a sample of injured workers (64) and 40 to 45% in a pain management practice(65,66). In an Australian study with patients in a rheumatology practice, the prevalence was 40% (67). However,
the association between pain originating from the FJ and the degenerative changes in those joints continues to be an enigma and controversial. The majority of reports indicate no correlation between the clinical symptoms of LBP and imaging, including radiographs, magnetic resonance resonance imaging (MRI), computed axial tomography (CT)
scanning, single photon emission (SPECT) scanning, and radionuclide bone scanning (64-75). Even the role of
FJ abnormalities in patients with LBP is still debated (62-64).
On the one hand, Lewinnek and Warfield (58) found that 96% of patients with CT-documented OA of the FJ responded to the injection technique. On the other hand, Schwarzer and coworkers (72) were not able to demonstrate a significant correlation between the degree of OA seen on CT and the pain score achieved during the intra-articular facet block. Additional studies are needed to understand the connection between degenerative changes in FJ and the pain originating from them.
The neural foramen is bordered by the superior articular process, pars interarticularis, and posterior portion of the vertebral body. FJ hypertrophy or a synovial cyst can contribute to lateral and central lumbar stenosis, which can lead to impingement on the exiting nerve root. Thus, FJ pain may occasionally produce a pain referral pattern indistinguishable from disc herniation. Clinically, pain that originates from lumbar FJ is defined as “lumbar facet joint syndrome.” The diagnosis is made clinically and by excluding other origins of LBP (76). The typical symptoms and signs are localized “pseudoradicular” lumbar pain that may radiate unilaterally or bilaterally to the buttock, the hip, the groins, and the
thighs, typically ending above the knee without neurological deficits (59,77). Patients usually report increased complaints in the morning and during periods of inactivity (78). Pain increases with stress, exercise, lumbar spine extension, rotary motions, and when standing or sitting. Lying and flexion of the lumbar spine lead to pain relief (78). However, Jackson (79) in his review concluded that the facet syndrome is not a reliable clinical diagnosis, and indeed in the recent scientific literature, we found infrequent mention of it.
Degenerative Process of the Facet Joints
OA of the FJ is similar to that of all diarthrodial joints
(80). Cartilage degradation leads to the formation of focal
and then diffuse erosions, with sclerosis of the subchondral
bone (78). Facet hypertrophy, apophyseal malalignment,
and osteophyte formation may narrow the spinal
canal or intervertebral foramen and create central and/or
lateral stenosis. Destabilization of the 3-joint complex
(intervertebral disc and 2 allied FJ) may lead to degenerative
instabilities including degenerative spondylolisthesis
and scoliosis (81). As we mentioned before, the richly
innervated FJ may be a source of a back pain.
Some studies reported that degenerative changes are
more common on the superior facet than on the inferior
facet (82,83). However, in Tischer and coworkers’ (26)
cadaveric study, where the changes were observed directly
on the FJ, they found no difference in the incidence of
degenerative changes in the superior and inferior facets,
but the location of damage was different between superior
and inferior facets. Cartilage defects were located mostly
at the margins of the articular surface, the central zone
being relatively well preserved. The superior facet showed
most damage at the superior pole, where, during flexion
movements, the inferior facet causes maximum pressure
(Fig. 4A). The inferior facet showed most cartilage damage
at the superior and inferior poles, whereas bony appositions
are almost exclusively seen at the inferior pole,
where bony contact between the inferior pole of the inferior
facet and the arch of the superior facet can take place
during extension movements (Fig. 4B). Adams and Hutton
(30) have already suggested such points of overload,
but their work could not prove the concept to be valid.
Jinkins (43) also argued that these locations are under
excessive stress, especially on a background of intervertebral
disk degeneration.
Tischer and coworkers (26) found that osteophyte formation
is less frequent in FJ than cartilage defects and that
they formed mainly on the superior facet on the lateral
margin where the dorsal capsule is attached. Axial lumbar
rotation can cause stretching of the posterior part of the
contralateral joint capsule. This mechanical environment
promotes changes in the dorsal capsular attachment and
subsequent to fibrocartilage metaplasia in association
with bone spur formation (25,84,85). The phenomenon
is most prominent in degenerated motion segments,
where higher axial rotation places more stress on the dorsal
capsule (25). A recent study (26) found osteophytes on
the lateral margin more frequently in severely degenerated
facets; the second most common location was at the inferior
pole of the inferior facet, where the inferior facet
contacts the isthmus of the neural arch of the corresponding
superior facet during extension. The overall relative
low prevalence of osteophyte formation is confirmed by
Eisenstein and Parry, who found severe cartilage lesions
with subchondral bone erosion in 12 patients, while osteophyte
formation was markedly absent in all cases (78).
The capsule seemed to become small (narrow) and thin
with advancement of degenerative changes in the joint
cartilage. Therefore, in patients with degenerative
changes of the lumbar facets, joint motion is likely to be
limited or altered because of the suggested capsular factor
as well as because of the structural changes (22).
Synovial cysts, the outpouching of synovial membrane
of the FJ, were originally described by Baker in 1877 (86),
who defined it as being a para-articular cyst secondary to
processes occurring within an adjacent degenerative joint.
The first description of a spinal synovial cyst was made by
Von Gruker in 1880 (87), in a postmortem examination
description. They are most frequently found in FJ L4-L5
(65%), but are also seen at the L5-S1 (31%) and L3-L4
(4%) levels. They may produce a well-defined cystic structure
with calcification in the cyst wall (88,89). In a recent
retrospective study of 303 MRI scans, Doyle and Merrilees
(90) have demonstrated, in a symptomatic population,
that the presence of synovial cyst was independently
associated with an increased grade and frequency of FJ
OA. They also found no correlation between synovial cyst
occurrence and disc degeneration grade. Another team
(89) found no or minimal disc degeneration in 65% of
their synovial cysts population, whereas in 100% of the
patients relatively severe FJ OA was observed.
Hypertrophy of articulate processes has been mentioned
in several studies as a sign of FJ OA: “facet joint
hypertrophy” (60,91,92). However, Barry and Livesley
(93) in their CT study of 100 patients found that the 13
patients with degenerative FJ and radiologically normal
discs did not have significantly larger FJ than the 35 patients
with disc disease and radiologically normal FJ. They
concluded that the term “facet joint hypertrophy” should
not be used when osteoarthritic changes are noted on CT
scan because these joints are not significantly larger than
normal FJ.
facet joint image