하부운동사슬을 전체적으로 이해할때 필요한 자료
천장관절은 비전형적인 활액관절이어서 약간이지만 매우 중요한 움직임을 허용함.
- 천골(sacrum)기준으로 천장관절에서 몸통앞쪽으로 살짝 이동하는 forward motion
- 장골의 inward motion과 좌골의 outward motion등이 있어 birth canal(산도) 직경을 증가하게 할 수 있음.
panic bird...
![]() Functional Anatomy of the Lower Limb.pdf
Functional Anatomy of the Lower Limb.pdf
Following on from my lecture on the upper limb I would now like to treat the lower limb in a similar fashion: moving distally from the pelvic girdle to the foot.
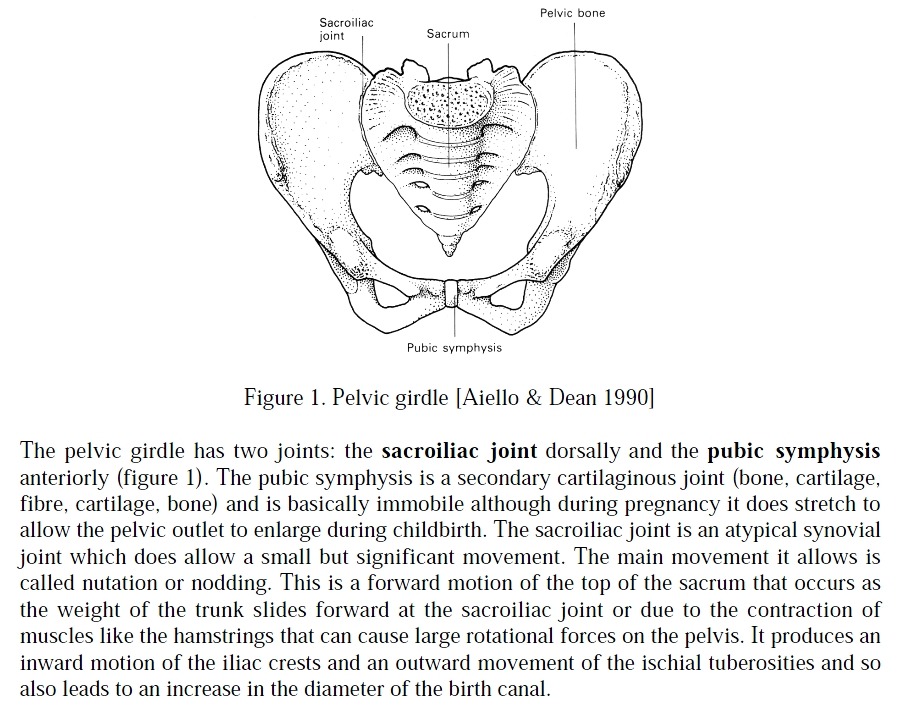
- 골반대는 천장관절(SI joint)과 치골결합(pubic symphysis)으로 구성
- 치골결합은 연골결합이고 출산시 약간 움직이지만 기본적으로는 움직이지 않는 관절
- 천장관절은 비전형적인 활액관절이어서 약간이지만 매우 중요한 움직임을 허용함.
- 천골(sacrum)기준으로 천장관절에서 몸통앞쪽으로 살짝 이동하는 forward motion
- 장골의 inward motion과 좌골의 outward motion등이 있어 birth canal(산도) 직경을 증가하게 할 수 있음.
The hip joint is a classic ball-and-socket joint allowing flexion, extension, adduction, abduction, and medial and lateral rotation. The hip joint is a much more stable joint than the shoulder since it has a much more substantial bony cup (acetabulum) for the head of the femur and has a more restricted range of movement.
- 고관절은 전형적인 구상관절로 굴곡, 신전, 내전, 외전, 내회전, 외회전을 허용함.
- 대퇴골의 골두를 위한 acetabulum이 움직임을 좀더 제한하기 때문에 고관절은 어깨관절보다 더 안정성이 있음.
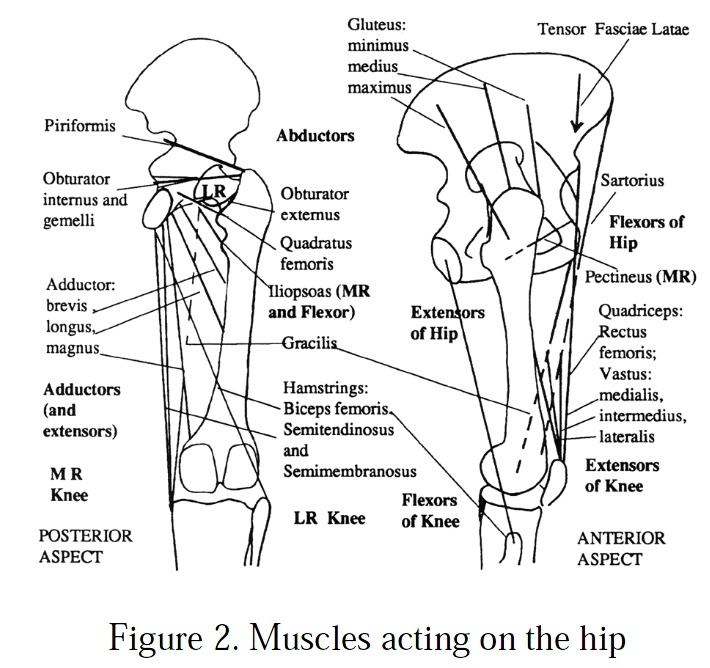
Even so the short lateral rotators (obturator internus, the superior and inferior gemelli, piriformis, quadratus femoris) do have an important stabilisation role. The prime movers can be grouped into four compartments: anterior, posterior, medial (adductor) and buttock, and their actions assigned accordingly as flexors, extensors, adductors and abductors. There is of course some overlap with several muscles having multiple actions: for example gluteus maximus acts as a hip extensor when the hip is flexed; and adductor magnus is also a hip extensor as well as an adductor.
- 좀더 짧은 고관절 외회전 근육이 중요한 안정성 역할을 담당함.
- 고관절 주동근은 4 부분으로 그룹화됨. 굴곡근, 신전근, 내전근, 외전근
- 기능을 중첩하는 multiple action을 하는 근육도 있음.
In addition muscles in the hamstring group (biceps femoris, semitendinosus and semimembranosus) are also knee flexors and the quadriceps muscles (rectus femoris, vastus medialis, intermedius, lateralis) are knee extensors. Such muscles cross more than one joint and this seems to be important in the lower limb for energy transfer between segments and to keep the muscles operating and their optimal length.
- 게다가 햄스트링은 무릎굴곡근이고 대퇴사두근은 무릎 신전근.
- 어떤 근육은 한관절음 넘어 하지에 중요한 역할을 수행함.
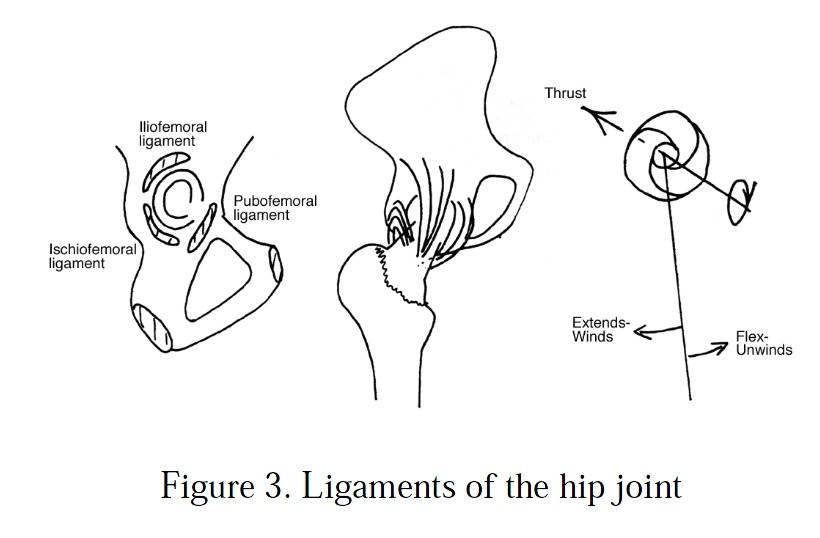
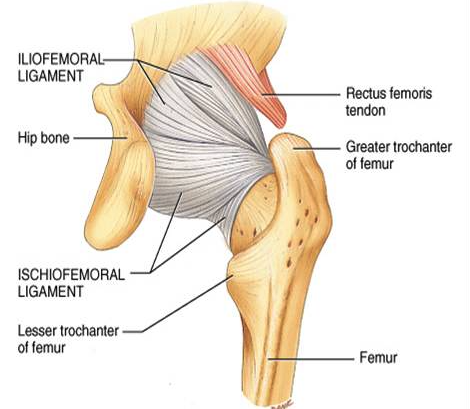
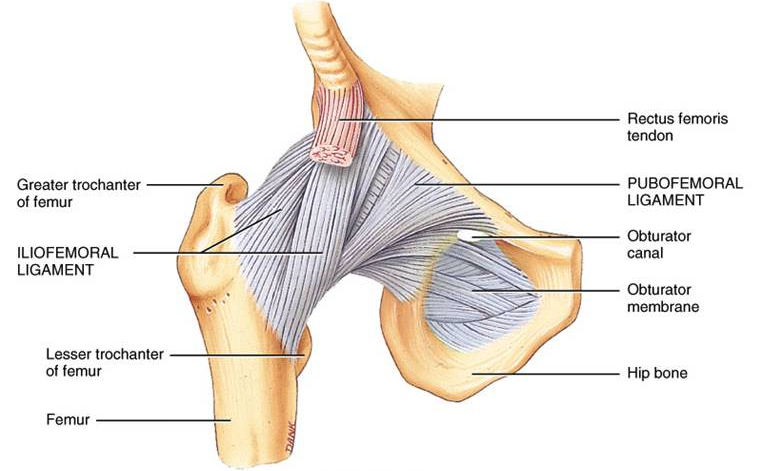
The hip joint itself is also stabilised by the actions of the iliofemoral, ischiofemoral and pubofemoral ligaments (figure 3). These wind around the neck of the femur in such a way that they tighten in extension. This drives the head of the femur firmly into the acetabulum preventing dislocation and also limits hip extension. The pubofemoral ligament, because of its position, also limits abduction. Other movements of the hip (flexion and adduction) are limited by muscle stretch. Flexion is limited by the hamstrings and since these are lax when the knee is flexed considerably more hip flexion is possible if combined with knee flexion.
- 고관절 자체는 3가지 인대에 의해서 안정성을 가짐. iliofemoral, ischiofemoral, pubofemoral ligament
- pubofemoral ligament는 그들의 위치때문에 내전을 제한함.
- 고관절의 다른 움직임(굴곡과 내전)은 근육 스트레치에 의해 제한됨.
- 굴곡은 햄스트링에 의해서 제한되고 무릎을 굴곡하면 햄스트링이 이완되므로 ...
The hip joint is very stable and is almost never dislocated in a healthy adult. The one occasion where it can occur is in car accidents where the victim is sitting in the from seat and the force of the impact forces the femur posteriorly. The flexion of the hip means that the
ligaments are lax, and the direction of the force pushes the head of the femur towards the weakest and shallowest part of the acetabulum.
- 건강한 성인에서 고관절은 매우 안정적이이서 서의 탈구되지 않음.
- 고관절을 굴곡하면 인대은 이완됨... 이 자세에서 전방쪽으로는 탈구될 수 있는 약한 구조 방향이 있음.
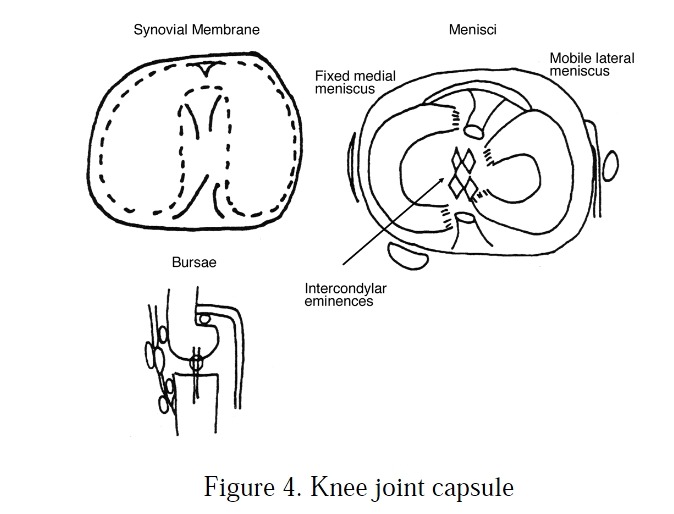
The knee joint is considerably more complex than the hip joint. It is generally described as a hinge joint but this does not do it justice! As can be seen from figure 4 the synovial membrane is a horseshoe shape with the gap posteriorly. Within the synovial cavity are two articular disks: both are attached to the surrounding joint capsule but the lateral meniscus is much more mobile. You can also see from figure 4 that there are a large number (approximately 15) of bursae associated with the knee joint. They act to reduce the friction between the various structures (tendons, muscles, bone) associated with the joint.
- 무릎관절은 고관절보다 복잡한 구조임. 경첩관절이지만 경첩관절의 온전한 정의에 부합하지 않음.
- 그림 4에서 보는 바와같이 활액막은 편자형태로 뒤쪽으로 gap이 있음.
- 관절강내에 두개의 관절연골이 있음. 반달연골은 관절낭 주위에 부착하고 있지만 바깥쪽 반달연골은 좀더 움직이는 구조임.
- 무릎관절에 관련된 점액낭이 많이 있음. 점액낭은 다른 구조(힘줄, 근육, 뼈)사이에 마찰을 줄이는 역할.
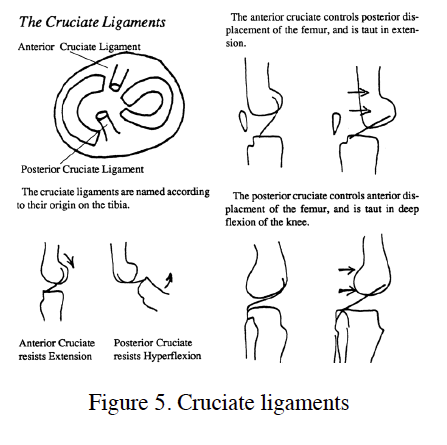
Within the joint capsule are two important intracapsular ligaments: the cruciate ligaments (figure 5). These are names by their relative origins on the tibia and cross before inserting in the opposite order between the femoral condyles. The anterior cruciate (which is the one that is most commonly injured) becomes taught during extension and posterior displacement of the femur thus is restricts these movements and can be injured in forced hyperextension. The posterior cruciate prevents the opposite movements: hyperflexion and anterior displacement of the femur.
- 관절낭 내에 두가지 중요한 인대가 있음. 십자인대
- 가장 흔하게 손상되는 전십자인대는 무릎을 신전하고 .......
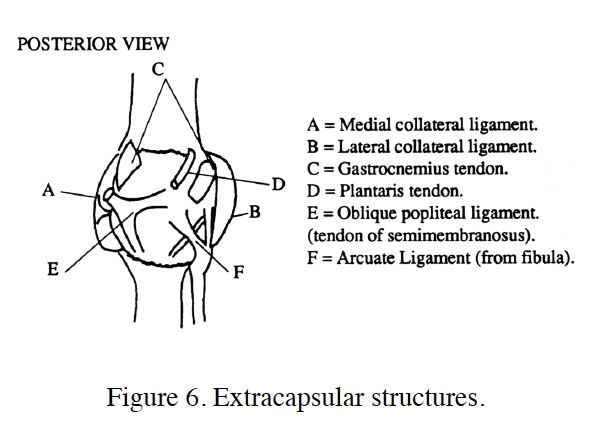
Figure 6 shows the extracapsular structures. This includes two other important ligaments, the
medial and lateral collateral ligaments, that stabilise the joint against lateral movements.
Once again the tendons of the various muscles that cross the joint are also important in
stabilisation.
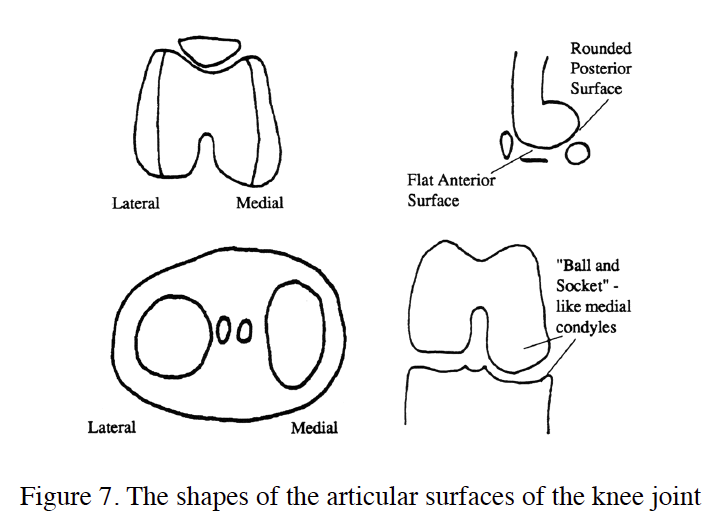
When we look in detail at the shapes of the articular surfaces we can begin to see why the
knee cannot be described as a simple hinge joint (figure 7). The lateral femoral condyle is
smaller than the medial condyle and its articulation with the corresponding tibial condyle is
more circular. The cross-section of the femoral condyles is not uniformly circular with a
rounded posterior surface but a flattened anterior surface. The medial tibial condyle is
described as more “ball and socket-like”.
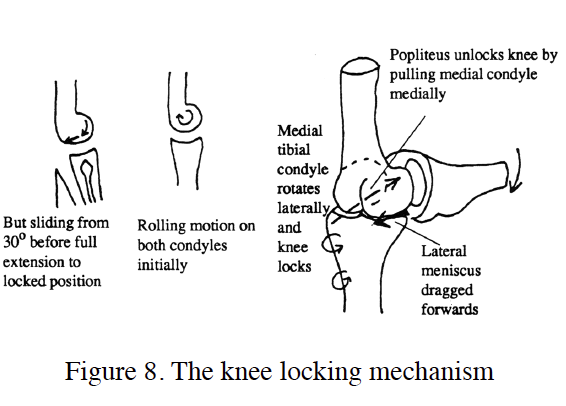
These features interact to produce the locking mechanism of the knee. This mechanism
means that the knee can remain in full extension with no muscular activity which makes
standing much more comfortable and energy efficient. In figure 8 we can see how it works.
As we start to extend a flexed knee initially both the medial and lateral femoral condyles are
able to roll on the tibia plateau. However because the lateral condyle is smaller the flattened
anterior part of the articular surface comes into contact sooner on this side. The movement
there becomes a sliding movement and 30° before full extension the joint becomes close
packed on the lateral side. The only way the knee can continue to extend is for the tibia to
laterally rotate allowing the medial condyle of the femur to continue to rotate and then slide
itself when its own flattened surface comes into contact with the tibia. The end result of this
rotation is that the anterior crucitate is tightened and the knee joint is locked into extension
with the flat part of the femoral condyles tightly pulled onto the tibia. The knee is stable in
this extended position and in fact the tibia needs to be medially rotated by a small muscle
called popliteus before flexion can occur. Note in this description popliteus unlocks the knee
joint by medially rotating the tibia. This could equally well be described as laterally rotating
the femur if the tibia was fixed which would be the case in normal walking for example.
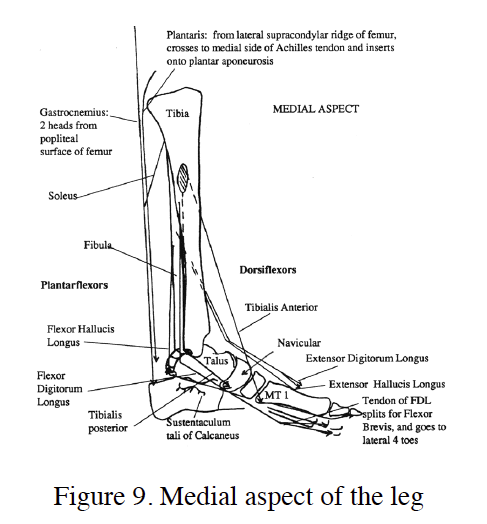
Moving distally we can start to see similarities between the leg and the arm musculature.
Figure 9 shows the medial aspect of the leg and we can see the flexor and extensor
compartments. During development the leg is rotated 180° in the thigh region such that in the
anatomical position the distal flexors are now on the dorsal aspect (flexors of the knee and
ankle joints). Arm flexors are always ventral. In an attempt to avoid confusion flexion and
extension of the ankle have alternative names: plantarflexion and dorsiflexion.
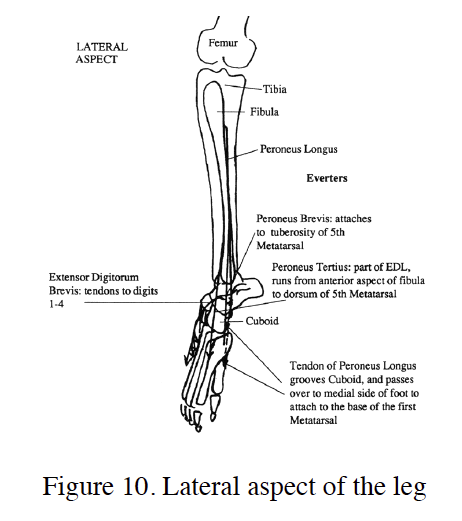
There is also an additional compartment on the lateral side (figure 10) containing the
peroneal muscles (peronius longus, brevis and tertius).
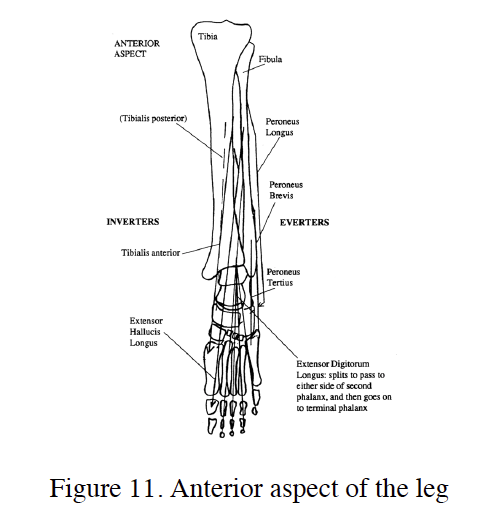
As can be seen in figure 11 the peroneal muscles laterally and the tibialis muscles medially
produce two new movements known as eversion and inversion. These are not really
equivalent to supination and pronantion even though they do all involve rotation around the
longitudinal axis of the limb. Supination and pronantion would have to occur by movement
of the tibia and fibula which does not occur. Evertion and invertion take place between the
bones of the foot and are more equivalent to the small amount of rotation that can take place
at the midcarpal joint.
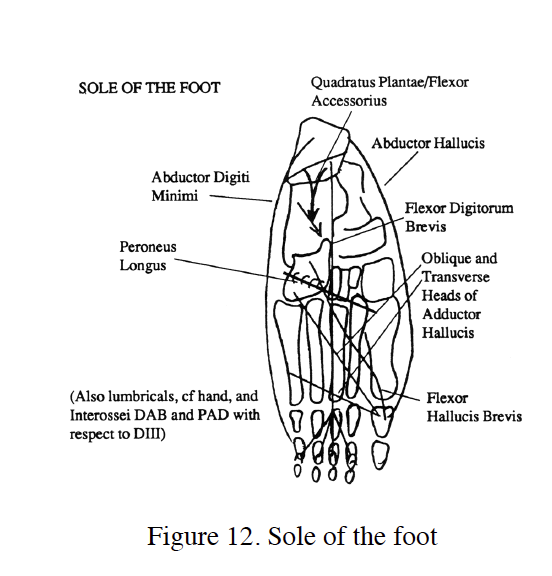
The muscles of the lower leg are equivalent to the extrinsic muscles of the hand and within
the foot itself are the equivalents of the intrinsic muscles. In fact, as shown in figure 12, there
are as many intrinsic muscles in the foot as in the hand and the movements they produce are
equivalent (flexion, extension, abduction and adduction of the toes). However the degree of
movement available and the independent control is much less although with training the
dexterity of the feet can be greatly enhanced.
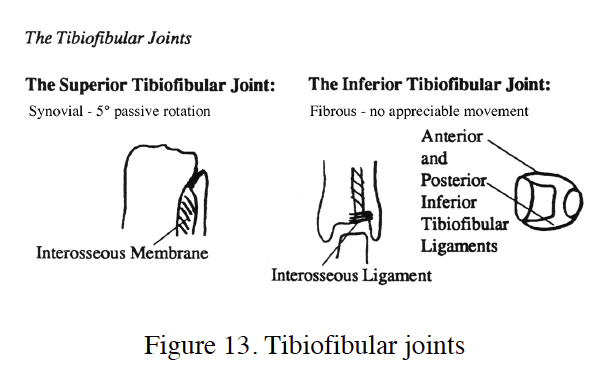
Figure 13 shows the tibiofibular joints – equivalent but much less mobile than the radioulnar
joints. The proximal joint is actually synovial and allows a small degree of rotation although
there are no muscles directly producing this action. It occurs to accommodate movements in
the talus at the tibiocrural (tibiotalal) joint. The inferior tibiofibular joint is a largely
immobile fibrous joint.
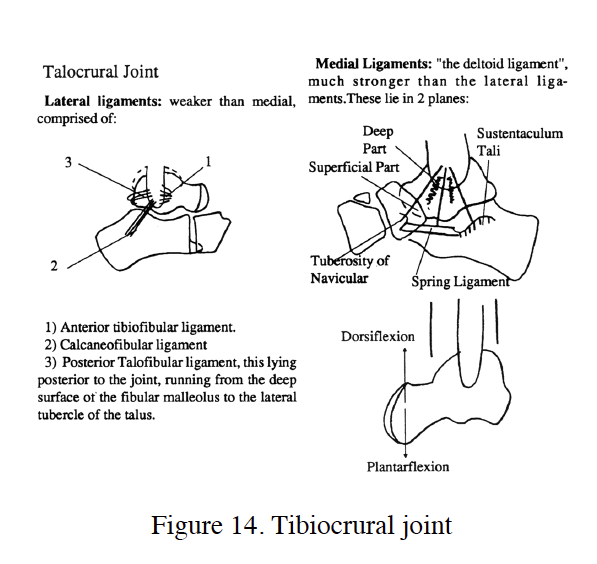
The ankle joint, much like the wrist joint is a complex of several synovial joints. The
movements can however be more easily assigned to specific bones. The tibiocrural joint
(figure 14) between the distal end of the tibia and the talus (with a small contribution from
the fibula on the lateral side) is where most of the flexion and extension takes place. It is
stabilised by medial and lateral ligaments. The lateral ligaments are weaker and therefore
more commonly damaged in sprains. The anterior part of the talar trochlear (the articular
surface of the talus is wider than the posterior part. This means that in dorsiflexion the tibia
and fibula are pushed apart tightening the tibiofibular ligaments and stabilising the joint. In
plantar flexion these ligaments are lax and the joint is less stable. Ankle injuries often occur
when the ankle is fully flexed.
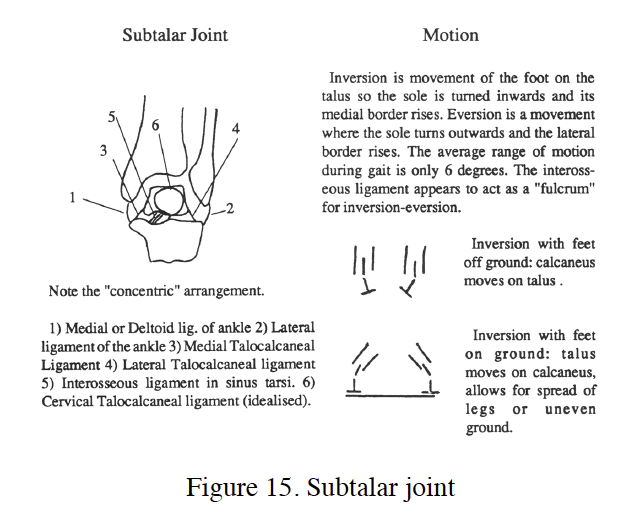
The subtalar (talocalcaneal) joint is between the talus and calcaneus and is where the actions
of inversion and eversion take place as shown in figure 15. The range of movement is quite
small but important for walking and standing on uneven ground.
There are a number of other named joints between tarsal bones (midtarsal joint, transverse
tarsal joint, intertarsal joints) and the tarsametatarsal joints but these show relatively little
movement. They are a collection of synovial sliding joints with tight ligaments that allow
small movements of the tarsal and metatarsal bones to accommodate uneven grounds. The
Metatarsophalageal joints and the various interphalangeal joints are largely equivalent to their
homologous counterparts in the hand. The MTP joints allow rather more extension than
flexion (the opposite to the hand) but the IP joints allow more flexion than extension exactly
as in the hand.
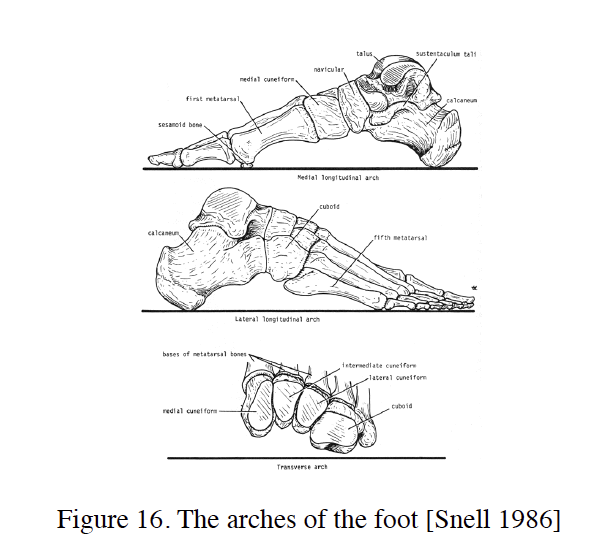
One important feature of the foot are the arches. The bones of the foot do not lie flat on the
substrate but are maintained as arches with only the ends of the arch in contact with the
ground. Anatomically three arches have been described and these are illustrated in figure 16
but only the medial arch (and perhaps to some extent the lateral arch) has any real function.
The arches of the foot convert the foot from a rigid lever to a sprung platform and this has
noticeable effects on running efficiency and performance since it allows the foot to store
elastic energy from one stride to the next.
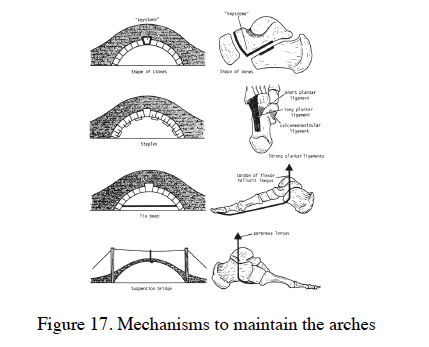
There are several anatomical mechanisms that act to maintain the arches of the foot
illustrated in figure 17. The first is the shape of the bones and the orientation of the joints
which forces them into an arch shape. This interlocking has to be maintained by external
ligaments both close to the joint (such as the so-called spring ligament between the calcaneus
and the navicular) and as a truss acting at the base of the arch. This truss is also helped by the
plantar aponeurosis. The centre of the arch is also actively supported by the direct action of
certain muscles. If these mechanisms fail then the person is described as having fallen arches
or flat feet.