오랜만에 논문을 찾아본다
근수축억제 현상은 인체기능 회복과정에서 심각한 장애요소다
panic bird...
![]() Quadriceps Arthrogenic Muscle Inhibition.pdf
Quadriceps Arthrogenic Muscle Inhibition.pdf
Quadriceps Arthrogenic Muscle Inhibition:
Neural Mechanisms and Treatment Perspectives
Quadriceps Arthrogenic Muscle Inhibition: Neural Mechanisms and Treatment Perspectives David Andrew Rice, BHSc,* and Peter John McNair, PhD†
Objectives: Arthritis, surgery, and traumatic injury of the knee joint are associated with longlasting inability to fully activate the quadriceps muscle, a process known as arthrogenic muscle inhibition (AMI). The goal of this review is to provide a contemporary view of the neural mechanisms responsible for AMI as well as to highlight therapeutic interventions that may help clinicians overcome AMI.
Methods: An extensive literature search of electronic databases was conducted including AMED, CINAHL, MEDLINE, OVID, SPORTDiscus, and Scopus.
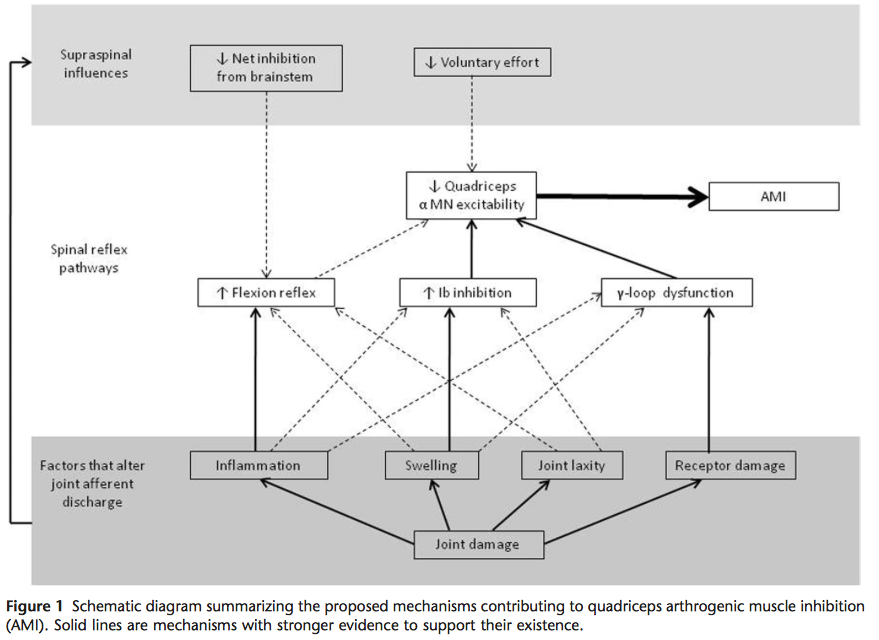
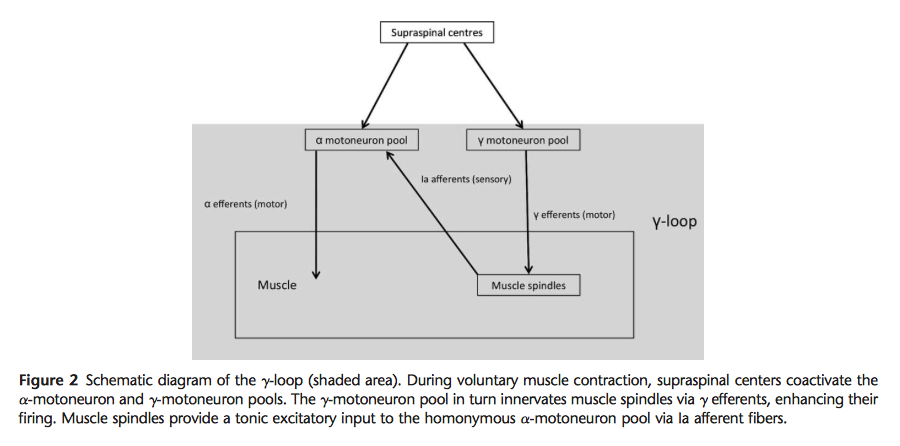
Results: While AMI is ubiquitous across knee joint pathologies, its severity may vary according to the degree of joint damage, time since injury, and knee joint angle. AMI is caused by a change in the discharge of articular sensory receptors due to factors such as swelling, inflammation, joint laxity, and damage to joint afferents. Spinal reflex pathways that likely contribute to AMI include the group I nonreciprocal (Ib) inhibitory pathway, the flexion reflex, and the gamma-loop. Preliminary evidence suggests that supraspinal pathways may also play an important role. Some of the most promising interventions to counter the effects of AMI include cryotherapy, transcutaneous electrical nerve stimulation, and neuromuscular electrical stimulation. Nonsteroidal anti-inflammatory drugs and intra-articular corticosteroids may also be effective when a strong inflammatory component is present with articular pathology.
Conclusions: AMI remains a significant barrier to effective rehabilitation in patients with arthritis and following knee injury and surgery. Gaining a better understanding of AMI’s underlying mechanisms will allow the development of improved therapeutic strategies, enhancing the rehabilitation of patients with knee joint pathology.
ⓒ 2010 Elsevier Inc. All rights reserved. Semin Arthritis Rheum 40:250-266
Keywords: quadriceps, muscle inhibition, voluntary activation, arthrogenic, knee trauma
Marked weakness of the quadriceps muscles is typically observed following knee injury, after knee surgery and in patients with arthritis. This is partly due to muscle atrophy and partly to ongoing neural inhibition that prevents the quadriceps from being fully activated, a process known as arthrogenic muscle inhibition (AMI). AMI has been linked to articular swell- ing, inflammation, pain, joint laxity, and structural dam- age (1-4). The relative importance of these factors is not clearly understood but it is generally accepted that AMI is caused by a change in the discharge of sensory receptors from the damaged knee joint (1,2,4-8). Anomalous joint afferent discharge may have powerful effects on the cen- tral nervous system, influencing the excitability of multi- ple spinal and supraspinal pathways that combine to limit activation of the quadriceps muscles.
Quadriceps AMI has long been of concern to clinicians as it contributes to muscle atrophy and can delay or even prevent effective strengthening, hindering rehabilitation considerably. While mild AMI does not preclude strength gains (9-11), it is likely to restrict their magnitude as a portion of the muscle cannot be activated. During the first few months after injury or surgery, or when joint damage is extensive, AMI may be severe and quadriceps strength- ening protocols can be largely ineffective. Despite resis- tance training, quadriceps strength may remain un- changed or even decline significantly (12-17), an effect attributed to AMI (12,17). As a result, quadriceps strength deficits often remain long after the initial joint trauma (18,19). Persistent quadriceps weakness is clini- cally important as it may impair dynamic knee stability (14,20), physical function (14,21-23), and quality of life (22), increase the risk of re-injury to the knee joint (24), and contribute to the development and progression of osteoarthritis (OA) (25-27).
The objective of this review is to provide the reader with a deeper understanding of AMI, with a focus on its potential neural mechanisms and therapeutic interven- tions that may help reduce its impact on rehabilitation. The first section of this article describes the presentation of AMI, including factors that may influence its severity and time course. We then review the sensory innervation of the knee joint and provide an outline of factors that may alter afferent discharge in the presence of knee dam- age. Thereafter, we examine the spinal reflex pathways that have been implicated in AMI and discuss the poten- tial influence of supraspinal centers on this process. Fi- nally, we present the most promising therapeutic inter- ventions that may help clinicians overcome AMI.