Communicating about fascia: history, pitfalls, and recommendations.
작성자문형철작성시간11.12.09조회수783 목록 댓글 1근막에 대한 모든 것
• Dense connective tissue
• Areolar connective tissue
• Superficial fascia
• Deep fascia
• Intermuscular septa
• Interosseal membrane
• Periost
• Neurovascular tract
• Epimysium
• Intra- and extramuscular aponeurosis
• Perimysium
• Endomysium
맞나. ㅎㅎ
![]() Communicating about fascia. history, pitfalls, and recommendations.pdf
Communicating about fascia. history, pitfalls, and recommendations.pdf
INTRODUCTION
In classical Latin, the term “fascia” meant nothing more than band (a long and narrow piece) of material.(1)In that sense of the word, head or hair bands have been called fasciae in the past, and it may be that an anatomic ligament deserves such a name if the original meaning is taken literally. Another example is musculus sartorius, which, in the 17th century was reported(1) to sometimes have been called m. fascialis because of its shape (for example, van de Speigel and Casseri(2)).
Despite such an original literal meaning of this word, the inherent implication of an author using the word “fascia” in 19th-century gross anatomy texts is often that of an undifferentiated tissue that wraps around more “specialized” tissues or that forms a packing material between them.(3) Take, for example, the description in Quain’s Elements of Anatomy(4,5): “to signify those membranous sheets of reticulated or felted fibrous tissue, which invest or intervene between the soft parts, especially muscles.” Wilson(6)similarly provided a most simple description: “Fascia a Bandage.” It should be noted that this view can also already be found in the 18th century(7):
The Use of the Membranes is, to wrap up and cover the Parts, to strengthen them, to defend several of them from being hurt by the subjacent Bones, to sustain the Vessels that are ramified upon them, to keep the Parts united; and ‘tis wroth our Observation, that the admirable Sympathy, or Consent of the Parts one with another, depends in a great measure upon their Fibrous Connexions. (p. IXX)
At the present time, “fascia” has been used frequently by anatomists and non-anatomists, but its general meaning can be so vague that it implies little more than some form of connective tissue. It seems a fact that this confusion of terms is not new and unique to our times at all (see also Eycleshymer(8)), despite the fact that Hyrtl,(1) before giving an explanation, states that “nobody needs an explanation of the word fascia,” but nevertheless gives one to be complete.
DISCUSSION
We entertain an opinion contrary to that of Hyrtl. The very name of our (present and previous) Fascia Research Congress is an example, because the explicit decision of the initiators and organizers was to invite presentations of all types of relevant connective tissues. We intend to propose a change to neither the name of this congress nor its aim; rather, we want to make people aware of the difficulties of communication when using the word “fascia.” Particularly in a context such as a conference, where people from many scientific and clinical disciplines will be participating, a natural language barrier will be present (and here we are referring not only to the various national languages of the participants) related to jargon and connotations in use in various disciplines. We hope to be able to bridge such barriers with mutual respect and an effort of open communication. But to be able to do so, we need to be aware of the limitations and difficulties of our definitions and use of terms.
Anatomists are a little more precise when talking of superficial and deep fascia. These terms indicate the topographic relationships of the tissue with respect to the skin. Recently, there has been a resurgence of interest in the biomechanics of fascia, in part motivated by interest in the pathophysiology of musculoskeletal pain (note that the connective tissues are only implied in such a name) and its treatment with both conventional and “alternative” manual therapies such as massage, chiropractic, osteopathy, and Rolfing.(9,10) The term “fascia” in this context refers mostly to a form of connective tissue that equates histologically to dense irregularly arranged connective tissue. To the anatomist however, “fascia” may also be the so-called “loose” (areolar) connective tissue, dense connective tissue, or a combination of the two—with or without fat! As an example, consider the intermuscular connective tissues (epimysium) that delimit the border between two adjacent muscles.
It should be pointed out that words with a mechanical connotation (such as “loose”) are often used without actual mechanical testing under well-defined conditions and are therefore more morphologic than mechanical in nature. In the dissection room, areolar connective tissues of the epimysia are easily broken by blunt dissection—for example, with simple use of fingers. (Note that this is a very unphysiologic loading on the tissue, because very short thin strands of collagenous tissues are stretched enormously, beyond their breaking strength.) Despite the name used for them, these tissues have been shown experimentally to play a part in so-called epimuscular myofascial force transmission—that is, force transmission between muscle and surrounding tissues by paths other than the myotendinous ones (for reviews, see Huijing(11–13)). From this fact, it can be derived that, under more physiologic loading (shearing), such tissues are sufficiently stiff to allow transmission of a significant percentage of the total muscle force and sufficiently strong to fail to break under the associated loads. Note the extreme contrast between those words and the term “loose.”
The modern reader and author therefore need to be aware of possible ambiguities and misunderstandings stemming from different meanings of the word “fascia.” As with many classification systems, the various classes of fascia become less clear when examined in detail. Thus, even standard anatomy texts, continuing the tradition of distinguishing between superficial and deep fascia, recognize that one or both may be locally absent and that the superficial fascia can occasionally contain sheets of dense connective tissue.(14)Moreover, ultrasound and magnetic resonance imaging in live human subjects also suggest that the histologic distinction between superficial and deep fascia is not always clear.
Recent anatomic studies of fresh human cadavers have pointed out that, although the overall structure of the superficial fascia is that of a honeycomb consisting of non-densely laid-down collagen, it also frequently contains, parallel to the plane of the skin, prominent sheets of dense connective tissue that are comparable in thickness and appearance to the dense connective tissue of the nearby deep fascia.(15,16)However, some publications indicate that areolar connective tissue layers within the superficial fascia can be quite compliant.(17) Similarly, the deep fascia enveloping the muscles can, in some cases, be composed of multiple layers of dense and fat-containing areolar connective tissue rather a single, dense, continuous membrane. Recent studies of human subjects suggest that chronic low back pain is associated with the presence of an increased thickness or number (or both) of dense connective tissue layers, separated by fat, that can span the whole thickness between the dermis and the muscle in the back, making it difficult (if not impossible) to distinguish between the superficial and the deep fascia.a
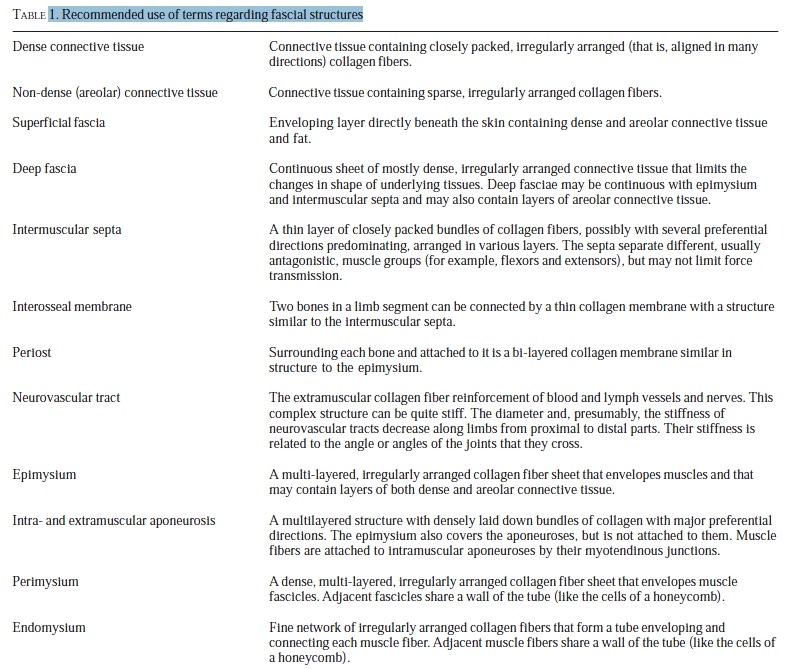
To ease communication and minimize ambiguity, we suggest that the term “fascia” should not be used by itself—that is, without further definition or refinement—because it is not clear whether this term refers to an anatomic entity or a type of tissue (Table 1). The commentary that follows therefore addresses the implications of using the terms set out in the remainder of this subsection at the Second International Fascia Research Congress and in the future literature to define further the character of “fascia.”

Dense Connective Tissue
“Dense connective tissue” is connective tissue containing closely packed fibers. The fibers are predominantly collagen, although in some sites, elastic fibers may be present in abundance (for example, ligamentum nuchae and flavum). The high collagen content imparts high tensile strength and high stiffness once the network is stretched sufficiently to align more fibers, if this is not already the case. If the functional requirement is to resist stretch from many different directions, the fibers will be arranged in a mesh (as in many parts of joint capsules, except the ligaments). This tissue is not woven—that is, it does not have fibers crossing each other systematically in an alternating way as in most old-fashioned textiles—but resembles more the felt-like structure of modern non-woven textiles and other materials that depend on chemical cross-linking rather than on intertwining. Such tissue is best described as a dense irregular(multidirectionally stranded) connective tissue. However, if functional demands dictate that the tensile loading is predominantly in one or only a few directions, it follows that the collagen strands will be in a parallel arrangement along the direction of the loads imposed.
Such a connective tissue typifies most tendons, ligaments, aponeuroses, and intermuscular septa, and is referred to as dense regular connective tissue. In both regular and irregular dense connective tissues, the cells embedded within their collagen-reinforced matrix are predominantly fibroblasts.
Non-Dense (Areolar) Connective Tissue
Non-dense (areolar) connective tissue contains more sparsely arranged fibers and strands (both collagen and elastic) that are not arranged in any predominant directions. Commonly, such connective tissue is called “loose connective tissue,” but we advise against the use of the word “loose” because of its unjustified mechanical connotations (discussed earlier).
The most common form of non-dense connective tissue by far is areolar connective tissue, and unless an author is at pains to be referring to another form of loose connective tissue (for example, reticular connective tissue that forms a stroma for lymphoid organs), loose connective tissue is likely to be equated with areolar tissue. Fibers are far less numerous in this tissue than in dense connective tissue, and although fibroblasts are also present, other cells of a wider range of types are typically present as well. In particular, areolar connective tissue can contain a variable population of white blood cells (or their differentiation products) that have entered from the small blood vessels passing through. The numbers of such cells are greater when an infection is present.
Areolar connective tissue also contains neurovascular bundles and small branches of sensory nerves that may terminate in the dense or areolar connective tissue layers.(18) An important function of areolar connective tissue is that it can allow some amount of shear deformation to occur between two adjacent dense connective tissue layers such that they can “glide” past one another. This function has been demonstrated in dynamic ultrasound imaging of layers within the thoracolumbar fascia.b
Superficial Fascia
The superficial fascia (synonymous with fascia superficialis, tela subcutanea, hypoderm, hypodermis, stratum subcutaneous, subcutis, panniculus adiposus) is an enveloping layer directly beneath the skin and thus continuous with the dermis, this location being the only certain implication of referring to a tissue as “superficial fascia.” Thus, although loose connective tissue or fat is common in the superficial fascia, a delicate three-dimensional meshwork of dense irregular connective tissue (with loose connective tissue and fat within its meshes) or more obvious sheets of tissue (for example, in association with the great saphenous vein as it courses through the superficial fascia of the lower limb) may also be present.(19)Superficial fascia can even contain skeletal muscle, well exemplified by the “muscles of fascial expression” that enable humans to smile, laugh, cry, and frown.
Deep Fascia
Deep fascia (synonymous with fascia profunda) is typically a continuous sheet of mostly dense irregular connective tissue keeping an underlying structure (particularly muscle) in position. It is thus classically a tight-fitting “ensheathing fascia” that needs a degree of tensile strength so that it can maintain the form of the body part and preserve the associated surface contour(20); hence, its dense connective tissue character. So close is the association between deep fascia and muscle in some regions of the body that the fascia can be firmly adherent to the underlying muscles and thus form an aponeurosis for them. It should also be noted that, in some parts of the body (for example, the neck), the association between fascia and underlying muscle is formally recognized by referring to the deep fascia of the region as “investing fascia.” This part of the language is particular to surgeons, because of the importance of such fascia in relation to the spread of infections.
Elsewhere, certain regions of deep fascia may be given unique names that generally define their topographic location (thoracolumbar fascia, crural fascia, plantar fascia), but sometimes their character (fascia lata). Readers need to be aware that deep fascia is not always synonymous with dense connective tissue, for it can contain varying amounts of less-dense connective tissue (both areolar connective tissue and fat).
Aponeurosis
The term “aponeurosis” is a difficult one because, among other reasons, it makes reference to the Greek “neuron,” which to modern users means “nerve.” Hyrtl(1) points out (p. 69) that until Aristotle (384–322 bc) named neura as nerves, the term “neuron” referred to any fibrous anatomic structure (for example, ligament, tendon). Confusion in the distinction between nerves and tendinous tissues (present even before Aristotelian times and sometimes lasting into post-Renaissance times) seems to have contributed. Galen, who was very aware of the morphologic and functional distinction between nerves and tendons,(21) used the term “aponeurosis” in two ways: for the tissues making the conversion of “muscle flesh” to tendon, and for the tendon itself.
For some time in the 18th and 19th centuries, the fasciae were included by anatomists (particularly, but not exclusively, French-language authors) as a category under the aponeuroses. For example, Winslow, in an English translation(22) of his book written in French(23) states about the fascia lata: “This Aponeurosis grows firmer and thicker in it’s progress toward the Os Pubis” (p. 165). Other examples can be found.(24–30) Later, these structures were again distinguished as separate entities—see, for example, Heiderich.(31)
In modern anatomy, an aponeurosis is often considered a flat tendon. This sheet-like part is likely, because of differences in morphology, to have mechanical properties different from those of tendon. So this difference should be expected even if tendon and aponeurosis were to be put together using identical materials with identical material properties.
The aponeurosis may have extra- as well intramuscular parts (for example, the human m. gastrocnemius). Muscle fibers attach to the intramuscular parts and are thus connected via the aponeurosis to tendon and to bone. Notably, however, many muscles have muscle fiber origins or insertions on intermuscular septa, interosseal membranes, or even the deep fascia. For example, most of the fibers of the human gluteus maximus muscle (on average 82% of its mass—in some individuals, 100%) insert on the fascia lata. In such muscles, the fascial structure operates as the intramuscular aponeurosis for the muscle. It is likely that such intramuscular aponeuroses are less independent than their counterparts mentioned earlier, because they are connected to bone in many directions. Muscular aponeuroses that are only a section of a fascial sheet may give the impression that they will not be reshaped into a tendon closer to the bone. However, such fascial sheets may be continuous and thus supported by or even hanging from ligaments, or crossing a joint. In such a case, some similarity in structure to the classical aponeurosis–tendon combination may be seen. This is clearly the case in the rat: Dr. Jaap van der Wal, who made groundbreaking progress on this subject in his thesis work,(32) will speak on this subject at the 2009 Fascia Congress. The same principle may apply just as well in humans, even though such connections are not as readily apparent as in the rat.
SUMMARY
We do not recommend that the term “fascia” be given such a wide meaning that it also includes all tendons and ligaments, for that is simply acknowledging that tendons and ligaments are forms of connective tissue and equates “fascia” with connective tissue in general. It “muddies” the simple definitions of tendons and ligaments that are still helpful to the beginner new to the field. But such caution does not stop us acknowledging that tendons and ligaments can commonly blend with fascia—and in particular, that they can become “fascial” near their attachment sites.
aLangevin HM, Stevens-Tuttle D, Fox JR, Badger GJ, Bouffard NA, Krag MH. Ultrasound evidence of altered lumbar connective tissue structure in human subjects with chronic low back pain. Paper to be presented at the Second International Fascia Research Congress; October 27–30, 2009; Amsterdam, Netherlands.
bFox JR, Stevens-Tuttle D, Langevin HM. Quantification of thoracolumbar fascia shear plane motion during passive flexion in human subjects with chronic low back pain. Paper to be presented at the Second International Fascia Research Congress; October 27–30, 2009; Amsterdam, Netherlands.
CONFLICT OF INTEREST NOTIFICATION
The author declares that there are no conflicts of interest.