joint capsule안에는 synovium이 있고, synovial fluid가 정상체액으로 존재하여 lubricant 역할을 함.
synovitis가 발생하면? synovitis는 어떤 기전으로 발생하는가?
활막 침착질환에는 어떤 것이 있으며, 어떻게 치료해야 하는가?
활액증식 질환인 색소성융모결절성 활막염(pigmented villonodular synovitis), 건초거세포종(giant cell tumor of tendon sheath), 헤모시데린 활막염(hemosiderotic synovitis), 활액막지방침착(fatty infiltration of the synovial membrane)에 대해서 논의
panic bird....
A b s t r a c t
Synovium is specialized mesenchymal tissue that is essential for the appropriate function of the locomotor apparatus. It is the site for a series of pathologic processes that are characteristic, and in some cases specific, to this distinctive tissue. In this article, the normal microscopic anatomy of synovium is briefly reviewed. Synovial proliferative disorders, including pigmented villonodular synovitis, giant cell tumor of tendon sheath, hemosiderotic synovitis, and fatty infiltration of the synovial membrane are discussed.
- 활액막은 특수화된 간엽조직으로 이동장치에 적합한 기능을 가진 필수적인 구조임.
- 활액막은 독특한 조직으로 특이한 병리적 반응의 연속성을 가지는 부위임.
- 이 논문에서는 정상 활액막의 미세현미경적 구조를 탐구함.
- 활액증식 질환인 색소성융모결절성 활막염(pigmented villonodular synovitis), 건초거세포종(giant cell tumor of tendon sheath), 헤모시데린 활막염(hemosiderotic synovitis), 활액막지방침착(fatty infiltration of the synovial membrane)에 대해서 논의함.
Additionally, the subjects of intrasynovial cartilaginous lesions (primary and secondary synovial chondromatosis) and crystal deposition diseases are reviewed. Finally, the response of synovial tissues to implanted foreign materials that are used in large and small joint arthroplasty are described.
- 추가로 내부활막 연골질 병변(1차성 2차성 활막 연골종), 수정체침착질환 등에 대해 논의함.
- 결국 활막조직이 foreign물질이 침착할때 발생하는 질환에 대해 토의함.
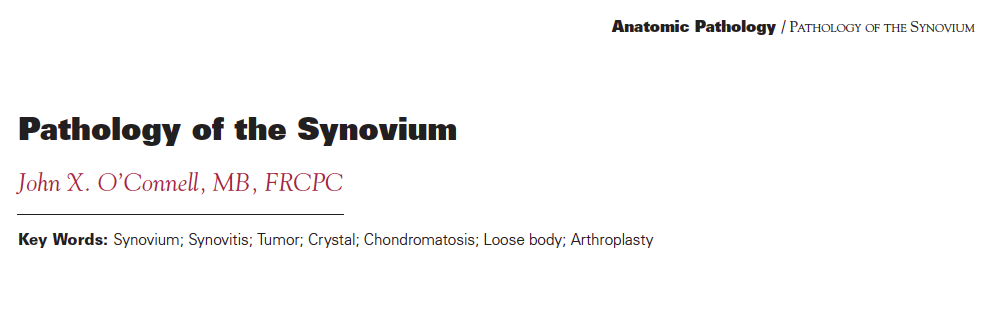
Phylogenetically, synovium is one of the newer attributes of the vertebrate locomotor apparatus. The first synovial joints developed in the piscine jaw of ancestors of modern lungfish by an evolutionary process that modified preexisting fibrous and cartilaginous joints, which were the predominant articulation of the early sea- and land-dwelling vertebrates.1 Embryologically, synovium is derived from specialized mesoderm termed the interzonal mesenchyme ❚Image 1❚.1
- 계통발생적으로, 활막은 척추동물 이동장치의 새로운 공헌자의 한가지임.
- 활액관절의 발생학, 진화론에 관한 이야기...
This differentiates from the primitive mesenchyme that lies between developing mobile cartilaginous skeletal elements. Fully developed mature connective tissue retains the capacity to differentiate into synovium as exemplified by the development of adventitial bursae and pseudarthroses and the synovial reaction to fixed foreign implanted material such as breast implants.
As Gray’s Anatomy eloquently proposes, “...once a region of pliant connective tissue is established between rigid skeletal elements [or foreign material], their ultimate separation by a synovial cavity appears to be an evolutional probability.”1
- 그레이 아나토미 설명 "유연한 결합조직의 부위가 간단한 골격요소사이에 발생하면, 그들의 활막 공간에 의한 궁극적 분리는진화적으로 일어날 가능성을 보임.
참고) synoviocyte 활액세포
Fibroblast-like synoviocytes (FLS) represent a specialised cell type located inside joints in the synovium. These cells play a crucial role in the pathogenesis of chronic inflammatory diseases, such as rheumatoid arthritis.
- 섬유아세포같은 활액세포는 관절내측 활막에 위치한 특별한 세포. 이 세포는 류마티스 관절염과 같은 만성 염증성질환에서 중요한 역할을 함.
Fibroblast-like synoviocytes in normal tissues[edit]
The inner lining of the joint consists of the synovium (also called the synovial membrane), a thin layer located between the joint capsule and the joint cavity. The word "synovium" is derived from the word "synovia" (or synovial fluid), which is a clear, viscous fluid produced by the synovium, and its main purpose is to reduce friction between the joint cartilages during movement. Synovium is also important to maintain proper joint function by providing the structural support and supply of the necessary nutrients to the surrounding cartilage.
- 활막은 관절강과 관절 캡슐사이에 존재하는 얇은 층.
- 활액은 맑고, 점액성의 액체로 활막에서 분비함. 활액의 주요 목적은 움직일때 관절연골사이에 마찰을 줄이기 위함. 활막은 관절연골에 영양을 공급과 구조지지를 제공함으로써 적절한 기능을 유지함.
Synovial membrane is divided into two compartments – the outer layer (subintima) and the inner layer (intima). The inner layer is mainly composed of two cell types, specialized macrophages (macrophage-like synovial cells) and fibroblast-like synoviocytes, which are important in maintaining the internal joint homeostasis. These cells represent the main source of hyaluronic acid and also other glycoproteins, major components of the synovial fluid.[1][2]
- 활막은 바깥층(subintima)와 안쪽층(intima) 두 구조로 나뉨.
- 내측 층은 주로 대식세포와 관절내 항상성유지에 중요한 역할을 수행하는 활막세포와같은 섬유아세포로 구성됨.
Fibroblast-like synoviocytes are cells of mesenchymal origin that display many characteristics common with fibroblasts, such as expression of several types of collagens and protein vimentin, a part of cytoskeletal filaments. Unlike fibroblasts, fibroblast-like synoviocytes also secrete unique proteins, that are normally absent in other fibroblast lineages. These include especially lubricin, a protein crucial for the joint lubrication. Furthermore these cells express a number of molecules important for the mediation of the cell adhesion, such as cadherin-11, VCAM-1, various integrins and their receptors. Specific for fibroblast-like synoviocytes is also the expression of CD55; this protein is often used to identify this cell type in the synovium by immunohistochemistry.[3]
- 섬유아세포같은 활액세포는 간엽세포 기원이고 섬유아세포 특성을 보임. 예를들어 콜라겐을 합성하는 등.
- 섬유아세포와는 다르게, 활액세포는 독특한 단백질을 분비함. 이는 관절윤활을 위한 루브리신같은 단백질을 포함함.
- 게다가 활액세포는 ....
The role of fibroblast-like synoviocytes in the pathogenesis of rheumatoid arthritis[edit]
Synovial hyperplasia (an increase in cell number) is a typical feature of the autoimmune disease called rheumatoid arthritis (RA). During the progression of this disease the synovial membrane becomes a place where constant inflammatory processes take place, which can eventually lead to cartilage damage and joint destruction and deformation. Due to the changes in proliferative and apoptotic processes the total number of cells increases in the synovium, and significantly increases also the number of fibroblast-like synoviocytes. These cells, together with other immune cells such as macrophages, lymphocytes, neutrophils, mast cells, dendritic cells and platelets, create an inflammatory environment in the synovium, attract more immune cells to the damaged place and thus contribute to the joint destruction.[1][2][3]
- 활액증식은 류마티스같은 전형적인 자가면역질환의 특성임.
- 활액막 질환의 진행과정동안 지속적인 염증과정이 진행되고 이는 결국 연골파괴와 관절파괴, 변형을 초래함.
- 증식과 세포사멸과정에서 변화때문에 활막에서 세포숫자가 증가하고, 섬유아세포같은 활액세포의 숫자가 증가함.
- 이러한 세포는 다른 면역세포인 대식세포, 임파구, 중성구, 비만세포, 수지상세포, 혈소판과 함께 염증환경을 만들어냄.
Fibroblast-like synoviocytes that are present in the synovium during rheumatoid artritis display altered phenotype compared to the cells present in normal tissues. They lose the property called contact inhibition (cells arrest their growth in the case when more cells come into contact with each other), and they also lose the growth dependency on adhesive surfaces; both these phenomena contribute to the increase in the number of fibroblast-like synoviocytes in the inflammatory tissue and are also typical for example for the growth of cancerous cells. In addition, these cells can produce a number of pro-inflammatory signalling molecules, especially Il-6 and IL-8, prostanoids and matrix metalloproteinases (MMPs), which may directly affect other cells and also participate in the inflammation enhancement.[3] These processes are influenced by microvesicles derived from platelets, which can contribute to the activation of fibroblast-like synoviocytes through secretion of IL-1.[4]
- 섬유아세포같은 활막세포는 활막에 존재하여 류마티스 관절염동안 정상조직 세포에 변형을 초래함. ...
Normal Anatomy
Synovium is composed of 2 to 3 layers of specialized cells termed synoviocytes. The synoviocytes overlie loose connective tissue consisting of fat, collagen, and blood vessels.2,3 Synoviocytes, like their mesodermal first cousins, mesothelial cells, grow as layers that surround fluid-filled spaces. By light microscopy, synoviocytes are relatively indistinct, appearing only as flattened, oval, dark-staining nuclei that usually seem removed from the immediate luminal surface by a fine layer of eosinophilic tissue.2,3
- 활막은 synoviocyte로 불리는 특수세포의 2-3층으로 구성됨.
- 활액세포는 지방, 콜라겐, 혈관의 loose 한 결합조직에 걸쳐있음. 활액세포는 활액으로 가득찬 공간주위에서 성장함.
- 현미경으로 활액세포는 상대적으로 뚜렷하지 않고, flattened, oval, dark-staining 핵 형태를 보이고, 호산구조직층에 의해서 중간 luminal surface으로부터 일반적으로 제거됨.
Most of the time, cytoplasmic borders are not visible, although when the cells are stimulated to divide or react to injury, they achieve rounded epithelioid morphologic features. Ultrastructurally,
the cells lining the luminal aspect of the synovial cavity have ovoid nuclei, inconspicuous nucleoli, and long cytoplasmic processes that extend in a tendril-like arrangement circumferentially from the nucleus. The cytoplasmic processes contain flattened endoplasmic reticulum, ribosomes, a well-developed Golgi complex, and numerous subplasmalemmal pinocytotic vesicles.2-4
- 대부분의 시간동안,
The processes interdigitate extensively, but cell junctions are not present. The surface synovial cells traditionally have been termed B
cells.3,4 Deep beneath the tangled web of surface cell processes are oval to rounded cells that have nuclear features similar to those of B cells. These so-called A cells lack cytoplasmic processes, but they have short filopodia.3,4 The A cells have cytoplasmic organelles similar to those of the B cells, as well as occasional lysosomes.
Transitional forms between the A and B cells also are found. A and B cells are embedded in an extracellular matrix rich in collagen and
pools of amorphous ground substance.3,4 The supporting connective tissue beneath the surface synoviocytes varies in its composition depending on anatomic site. In large joints that contain folds of synovium, there typically is a well-developed vascular network and
relatively abundant mature adipose tissue.4 Deep beneath this loose connective tissue is the dense, supporting, fibrous joint capsule. In tendon sheaths, the supporting connective tissue network is scant, and the synovial cells lie in close apposition to the fibrous layer of the tendon sheath or the tendon.2,3
Immunohistochemically, synoviocytes stain positively for vimentin and focally for CD68 (KP1). They are not labeled by antibodies to cytokeratin, S-100 protein, actins, desmin, CD34, or leukocyte common antigen.5
Synovial Proliferative Disorders
Pigmented Villonodular Synovitis and Giant Cell Tumor of Tendon Sheath
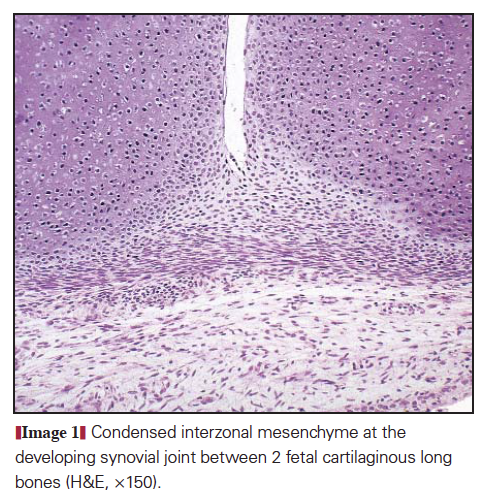
Pigmented villonodular synovitis (PVNS) is a proliferative disorder of the synovial lining of joints that produces localized or diffuse nodular thickening of the synovial membrane.6-10 Any synovial joint may be affected, but the knee is affected the most frequently.6-10 PVNS affects males and females with equal frequency and occurs in a wide age range, with greatest incidence in the second to fourth
decades.6-10 Patients typically complain of pain, swelling, or both of the affected joint.6-10 PVNS appears as a villous and nodular thickening of the synovial membrane ❚Image 2❚.
Diffuse involvement of the synovium results in thin, finger-like excrescences admixed with 0.5- to 2.0-cm rounded nodules that cover the normally smooth synovial membrane. Localized nodular synovitis produces a single bulging mass within the synovium.6,7,10
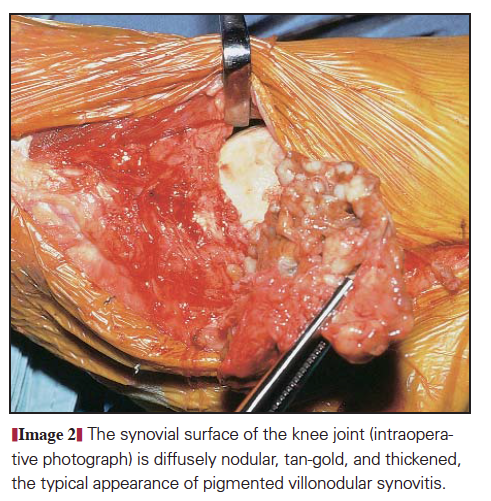
Microscopically, PVNS results in a papillary, villous, and nodular expansion of the synovial membrane. The surface synovial cells overlie a lobular and sheet-like arrangement of mononuclear rounded and epithelioid cells, multinucleated osteoclast-like giant cells, and lipid-rich cells.6-10 The mononuclear cells frequently contain large hemosiderin granules and have central round nuclei, often with prominent nucleoli. Mild nuclear pleomorphism often is seen. Mitotic counts rarely exceed 5 per 10 high-power fields. Necrosis is rare. The sheets and nodules of mononuclear cells, which likely represent proliferated surface synovial cells, are embedded in a collagenous stroma.5 In some cases, the nodular growth pattern is accentuated by broad bands of collagen. Most of the hemosiderin in PVNS lies beneath the surface synovial layer, and it often is found in aggregates in the rounded nodules ❚Image 3❚.6,7,10
A minority of cases of diffuse PVNS can result in bone erosion, sometimes involving adjacent bones of a joint.6 PVNS is treated by surgical excision. Localized disease responds well to this approach; however, lesions that diffusely affect the synovium have a high rate of local recurrence (>50%).8,9 PVNS that is refractory to repeated surgical excisions may be managed by low-dose radiation therapy.11
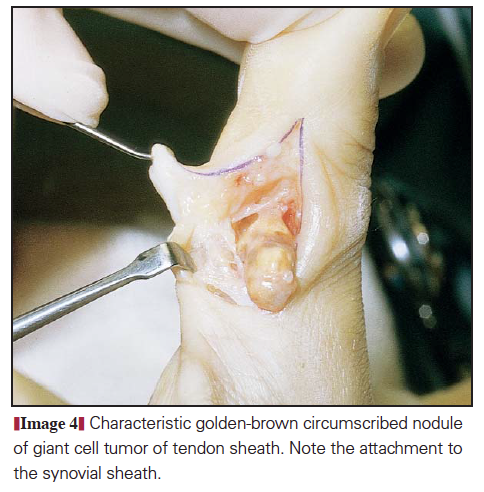
Localized giant cell tumor of tendon sheath (GCTTS) is histologically virtually identical to PVNS and represents its extra-articular analogue.6 GCTTS may arise in any synovial sheath; however, the tendon sheaths of the hands are affected preferentially ❚Image 4❚.5-7,10,12
Because of restricted space, localized GCTTS usually is small and only rarely exceeds 2.0 cm. However, diffuse GCTTS, which arises in extraarticular bursae, may exceed 10.0 cm.6,13 Unlike PVNS, GCTTS is grossly exclusively nodular, although microscopically
it is identical to an individual lobule of PVNS.5,6 In general, GCTTS contains less hemosiderin than does PVNS. Diffuse GCTTS frequently demonstrates microcystic cleft like spaces.
When GCTTS is treated by local excision, local recurrence is approximately 10% to 20%. As with PVNS, some GCTTS may exhibit local aggressive growth, including invasion of bone.6,8,10 Immunohistochemically, PVNS and GCTTS have a similar staining reaction to normal and reactive synovium, i.e., the mononuclear cells and multinucleated osteoclast-like giant cells react positively with antibodies to CD68 and vimentin.5 Ultrastructurally, PVNS and GCTTS are composed of cells that predominantly exhibit intermediate features of type A and B cells.12,14
Whether PVNS/GCTTS represents a neoplasm or an exuberant reactive proliferation is controversial. The detailed microscopic observations of Jaffe et al6 have provided most of our understanding and classification of these synovial proliferations, and they believed that the proliferations were nonneoplastic reactive lesions. This has been the predominant viewpoint for many years. More recently, however,
cytogenetic abnormalities, including trisomy 7, have been identified in short-term cell cultures of PVNS and GCTTS.15,16 This has been suggested as evidence that they are true neoplasms.15,16 An alternative method of evaluating clonality in cell populations from females involves assaying for patterns of X chromosome inactivation. By using this method, some investigators have demonstrated that GCTTS is composed of a nonclonal population of cells,17 supporting the original assertions of Jaffe et al.6
Hemosiderotic Synovitis
Hemosiderotic synovitis develops as a result of chronic
intra-articular hemorrhage. It occurs in hemophiliac males
who are predisposed to hemarthrosis, especially of the
knees.18-20 Patients with hemosiderotic synovitis typically complain of pain and stiffness of the involved joint, because
almost invariably, secondary osteoarthritis develops in association
with chronic intra-articular hemorrhage.18,20,21
Hemosiderotic synovitis appears as a brown or rust
color of the normal glistening translucent synovial
membrane. In early hemosiderotic synovitis, fine villous
projections extend into the joint cavity, but the larger nodules
and thickened fronds of PVNS do not occur. In the later
stages, after chronic repeated hemorrhage, the synovium
becomes thickened and opaque owing to intrasynovial and
subsynovial fibrous scarring.19,20
In hemosiderotic synovitis, cuboidal, plump, surface synovial cells contain granules of hemosiderin, and they line the flat synovial surfaces and the villous processes.19,22 In addition, hemosiderin-laden macrophages lie within the subsynovial connective tissue, often in association with small blood vessels ❚Image 5❚.19,22
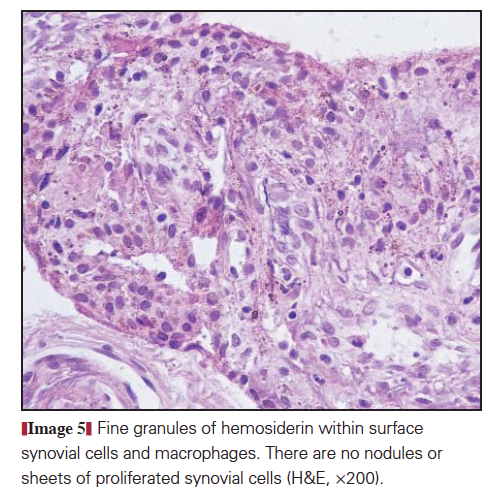
Sheets of mononuclear synovial
cells, lipid-laden cells, or multinucleated osteoclast-like giant
cells are not a feature of hemosiderotic synovitis.
Hemosiderotic synovitis often is associated with severe
degenerative articular cartilage disease. Hence, the treatment
revolves around surgical and conservative management of
the arthritis.18,20
A subset of hemosiderotic synovitis is caused by
intrasynovial hemangiomas.22-24 These are rare tumors;
fewer than 200 have been reported.22 Any joint may be
affected, although the knee is the most frequent site.22
Intrasynovial hemangiomas are localized tumors that occur
exclusively within the supporting synovial connective tissue.
Most patients complain of pain, a mass, or both. The hemangiomas
traditionally are classified as capillary, cavernous,
and arteriovenous types. They average about 4.0 cm.22 Occasionally,
thrombosed large vascular spaces with papillary
endothelial hyperplasia may be found. Intra-articular hemorrhage
may cause acute pain and swelling of the joint and, if
repeated, may produce histologic features of hemosiderotic
synovitis.22 The hemorrhage is rarely as progressive as that
in the bleeding diatheses, and accelerated osteoarthritis is not
usually a feature. Synovial hemangiomas are managed by
local excision, and recurrence is uncommon.
Villous Lipomatous Proliferation of the Synovial
Membrane (Lipoma Arborescens)
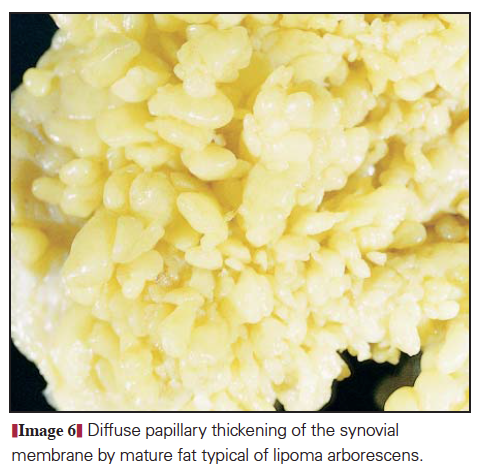
Lipoma arborescens, which is characterized by fatty infiltration of the subsynovial connective tissue, is one of the rarest of the synovial proliferative lesions.25 The disorder preferentially affects adult men and manifests as a slowly developing swelling.25-29 Any synovial-lined joint may be involved, but the knee is the favored site.25 Grossly, the entire synovium assumes a bright yellow, nodular, papillary appearance. It does not have the golden-brown color of PVNS or hemosiderotic synovitis ❚Image 6❚.25-29
Microscopically, the subsynovial connective tissue is thickened massively by an
infiltrate of mature adipose tissue.25-29 The surface synovial
cells typically appear reactive and epithelioid. Mitoses are
not found. Minor degrees of fatty infiltration of the subsynovial
space are normal in certain parts of the synovial
membrane, particularly in the knee joint, and slight nodular
thickening is a nonspecific finding in the synovium of osteoarthritic
joints. In a single microscopic field, this may simulate
lipoma arborescens, but this diagnosis should be made only when there is diffuse villous and nodular involvement. Most investigators think that lipoma arborescens is nonneoplastic and merely represents an excessive accumulation of fat in the subsynovial space.25 The cause is unknown. Treatment is synovectomy, and recurrence is rare.
Cartilage and Crystals
Cartilaginous Lesions of the Synovium
Primary Synovial Chondromatosis
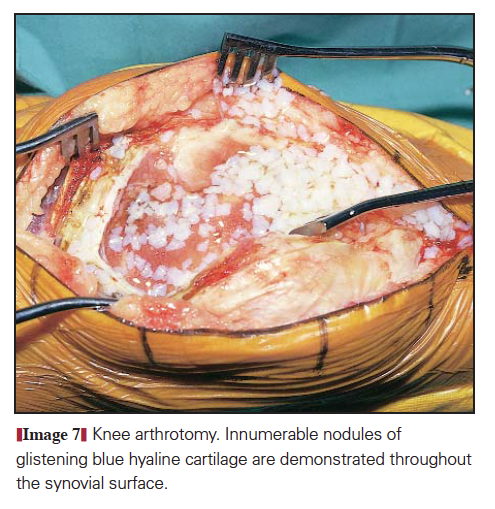
In primary synovial chondromatosis, multiple nodules of metaplastic hyaline cartilage expand the subsynovial connective tissue.30-32 This disorder affects patients in a wide age range from childhood to late adult life; the disease shows no sex preference.30-32 Patients complain of pain and swelling related to the involved joint.30-32 Any joint may be affected, including the extra-articular synovial tendon sheaths.33,34 There is no association between synovial chondromatosis and antecedent trauma, although an injury may draw attention to an involved joint. Synovial chondromatosis appears as numerous glistening blue-gray nodules in the synovial membrane ❚Image7❚.30-34
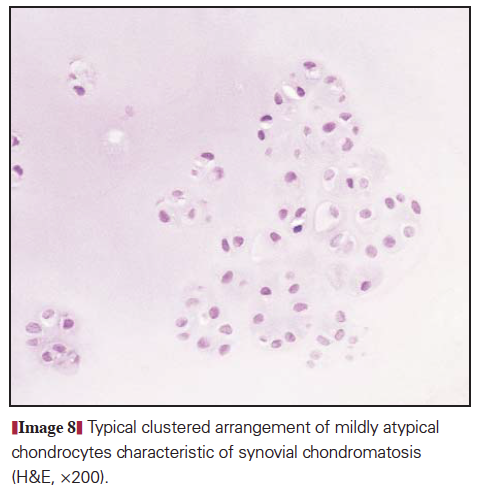
Nodules range from 2.0 mm to more than 1.0 cm and are firm on cut section. They often demonstrate chalky yellow regions that represent calcification, foci of enchondral ossification, or both. Microscopically, nodules of hypercellular hyaline cartilage are embedded in the synovial connective tissue.30-34 Individual nodules are circumscribed and round and demonstrate greater cellularity than articular cartilage. Chondrocytes typically are clustered rather than evenly distributed throughout the matrix.30-34 The individual cells exhibit a considerable size range and nuclear chromaticity. Most have pyknotic dark-staining nuclei, but many cells have atypical features, including large nuclei, dispersed chromatin, and nucleoli. Occasional mitoses may be found. The degree of cellularity and nuclear atypia found in synovial chondromatosis in most cases equals or exceeds that seen in low- and intermediate-grade intraosseous chondrosarcoma ❚Image8❚.30-34
Hence, care must be taken to avoid an erroneous
diagnosis of malignant neoplasm in this setting. Knowledge
of the radiographic and clinical features is, therefore, essential.
Enchondral ossification, when present, proceeds from
the periphery toward the center of the lobules. Synovial
chondromatosis is managed by synovectomy of the involved
joint. Recurrence develops in up to 15% of cases.35
Bona fide chondrosarcomas of synovium are extremely
rare neoplasms.35,36 These tumors may arise de novo or
secondary to preexisting primary synovial chondromatosis.36
The exact incidence of the latter event is unknown but generally
is considered rare. A recent review of cases of synovial
chondromatosis managed at a single hospital in Northern
Ireland demonstrated the surprisingly high rate of malignant
transformation of 5%.35 Clinical and radiographic information
is extremely important for establishing a diagnosis of
synovial chondrosarcoma. The chondrosarcomas are
frequently larger than synovial chondromatosis and more
consistently present as soft tissue masses.36 Bone destruction
adjacent to the joint also should arouse suspicion,36 although
this also may be seen in a minority of cases of synovial
chondromatosis.35 Histologically, chondrosarcomas of the synovium exhibit diffuse hypercellularity that lacks the
chondrocyte clustering typical of synovial chondromatosis.
35,36 In addition, spindling of tumor cells at the
periphery of lobules suggests chondrosarcoma. The degree
of nuclear atypia is not helpful for establishing a diagnosis of
malignant neoplasm unless extreme anaplasia is present,
since primary synovial chondromatosis characteristically has
mild to moderate atypia of the chondrocyte nuclei.36 Mitotic
figures and myxoid change of the stroma favor a diagnosis of
malignant neoplasm.36 The most useful and definitive
finding for a diagnosis of malignant neoplasm is permeative
destructive invasion of the bones around the joint.35,36 When
benign synovial chondromatosis “invades” bone, it does so
in a pushing manner, which is in contrast with the permeative
growth that characterizes chondrosarcoma. When chondrosarcoma
develops in the synovium, it typically is highgrade,
and pulmonary metastases frequently occur.35,36
Secondary Synovial Chondromatosis and Loose Bodies
“Loose” bodies develop when intra-articular fragments
of bone or hyaline articular cartilage come to lie free in the
joint cavity.30 Causes of loose bodies include idiopathic
epiphyseal osteonecrosis, osteochondral fracture, and osteochondritis
dissecans.37,38 Some of these “loose” fragments
are incorporated rapidly in papillary folds of synovium and,
thus, are attached to the lining of the joint by a long pedicle,
permitting mobility within the joint cavity. This interposition
of the fragment between the articulating ends of the bones
causes joint locking, which is the cardinal symptom of intraarticular
loose bodies.37 Other symptoms include pain and
swelling.30
Loose bodies may be single or multiple and often are
larger than individual nodules of synovial chondromatosis,
measuring more than 1.5 cm each. The external aspect of an
individual loose body is hard, white, and usually nodular and
bosselated. Sectioning the nodule sometimes demonstrates
the central osteoarticular fragment that initiated the
process.37,38
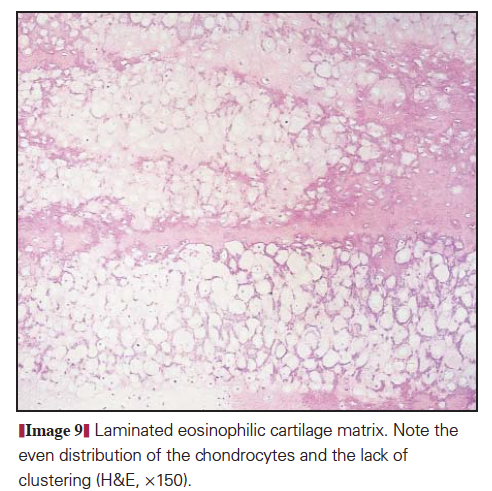
Loose bodies are composed predominantly of reactive or metaplastic cartilage; however, in contrast with synovial chondromatosis, this is usually not lobular and exhibits features intermediate between hyaline cartilage and fibrocartilage. 30,37,38 The matrix typically stains eosinophilic in H&E-stained sections and exhibits a more uniform cellularity than primary synovial chondromatosis, in addition to a
distinctly laminar arrangement of cells and matrix ❚Image 9❚.
Loose bodies rarely have the chondrocyte pleomorphism,
atypia, and mitotic activity that are features of synovial chondromatosis.
The inciting fragment is frequently at the center of the
loose body.37,38 It is usually hyaline articular cartilage or an
osteochondral fragment consisting of articular cartilage and
subchondral bone plate. The latter may seem viable or
necrotic depending on the underlying disease that produced
the loose body. At the edge of the inciting fragment, osteoclastic
resorption is frequently prominent, and islands of
metaplastic cartilage “invade” and replace its substance.38
Careful examination of the external surface of the loose body
may reveal an attenuated layer of synovium, at least focally.
This layer of cells is, however, extremely fragile and not
uncommonly is removed by handling the specimen,
explaining its frequent apparent absence.
Loose bodies are managed by local removal only; total
synovectomy is unnecessary. Recurrences are less common
than for primary synovial chondromatosis and depend on the
underlying disease process.
Crystal-Induced Synovial and Joint Diseases
Deposition of crystals within synovium, articular cartilage,
and periarticular soft tissue is associated with a spectrum
of clinical conditions ranging from asymptomatic soft
tissue aggregates through severe chronic destructive
arthropathies.39,40 The 3 endogenously formed crystals that
produce disease are monosodium urate, calcium pyrophosphate
dihydrate, and calcium hydroxyapatite.
Crystal formation occurs slowly and requires months or
years to develop. In general, crystal deposition needs locally
elevated levels of the precrystalline constituents in the
affected tissues. In addition, alterations in composition and
structure of the extracellular matrix contribute to crystal
formation.
The pathogenesis of joint destruction and synovial
inflammation is related to the ingestion of the crystals by phagocytic cells. They release chemotactic agents that
magnify the inflammatory reaction.39 Ultimately, the bone,
cartilage, and soft tissue injury that characterizes all of the
crystal deposition diseases is produced by enzymatic degradation
of the osseous and cartilaginous extracellular matrix.39
The stimulus that initiates the inflammatory reaction in each
crystal deposition disorder varies and often is incompletely
known.
Monosodium Urate Crystal Deposition Disease (Gout)
Gout is a systemic disease characterized by elevated
serum uric acid levels to more than 7 mg/dL (0.42 mmol/L),
tissue deposits of monosodium urate (tophi), recurrent acute
arthritis precipitated by urate deposits, and renal disease,
including uric acid lithiasis.39 Gout is relatively common,
with an overall prevalence of 2 per 1,000 of the population;
however, the prevalence increases dramatically with age to a
rate of 15 per 1,000 in men during the fourth and fifth
decades of life.39 About 30% of patients have primary hyperuricemia.
The remaining 70% exhibit hyperuricemia
secondary to another disease, usually renal failure, or as an
adverse effect of drug therapy.39 Tophi may occur at any connective tissue site, but the
first metatarsophalangeal joint and the soft tissues around the
pinna of the ear are affected preferentially.40 Acute attacks of
gout may be precipitated by sudden changes in serum uric
acid levels, trauma, and a variety of other causes. Clinically,
acute gouty arthritis closely mimics acute septic arthritis and
manifests as a painful, swollen, red joint.39 After resolution
of the first attack, patients may remain asymptomatic or
chronic gouty arthritis may develop.39
Pathology.—Monosodium urate crystal deposits within
synovium result in a papillary thickening and opacification
of the membrane.40,41 The tophi are cream-white and usually
soft. Larger tophi may be tan because of abundant admixed
fibrous tissue, and these may manifest clinically as hard
nodules. Since monosodium urate is dissolved by aqueous
solutions, formalin fixation and conventional tissue
processing usually result in the loss of the crystal from tissue
sections.40,41 If white deposits are recognized on fresh or
even partially fixed gross specimens, smearing the material
on a slide with a blade is an effective way to identify the
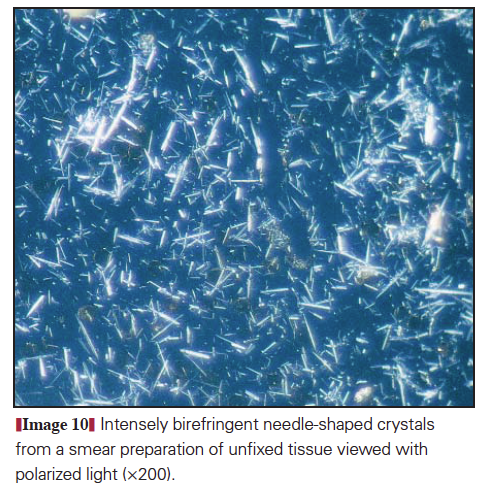
crystals. Microscopically, these smear preparations demonstrate
elongated needle-shaped crystals that are refractile and
exhibit intense negative birefringence when viewed with redcompensated
polarized light ❚Image 10❚.
The crystals usually
can be recognized readily based on their shape and intense
birefringence alone. Since they are dissolved by water, the
most efficient way to recognize them in tissue sections is to
perform a frozen section of the affected region or process
tissue that has been fixed in absolute alcohol using a
processing cycle that eliminates extended exposure to
formalin or dilute alcohol.40,41 Minor losses of crystal occur
during staining; however, enough crystals usually survive to
be visible in H&E-stained sections. The monosodium urate
appears as amorphous granular aggregates of yellow-brown
material embedded in thickened fibrotic synovium.40,41
Usually, the deposits are associated with a brisk histiocytic
and foreign body giant cell reaction. If the synovium or any
connective tissue deposit of monosodium urate has been
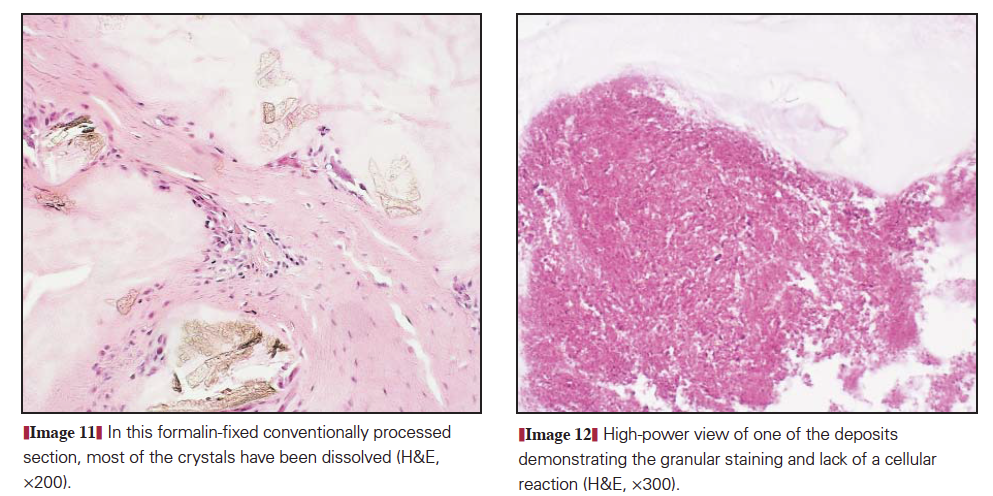
processed routinely, all of the crystals usually are dissolved.41 By light microscopy, pools of pale blue to eosinophilic amorphous material remain at the site of previous crystal deposition, representing the proteinaceous matrix that surrounds the crystals. It survives the tissue processing and staining procedures. Frequently, this matrix bears the imprint of the crystals, which are arranged as linear clusters, and, hence, a fibrillary or feathery pattern of lines may be seen within this substance ❚Image 11❚.41
Larger tophi
may exhibit ossification at their periphery, and, similarly,
intraosseous deposits commonly show ossification. In acute
attacks of gouty arthritis, the synovial membrane contains a
dense neutrophilic infiltrate in addition to the crystal
deposits. Joint aspiration is an equally effective way of identifying
the needle-like crystals of monosodium urate during
an acute attack.
Calcium Pyrophosphate Dihydrate Crystal Deposition
Disease (Pseudogout)
Pseudogout is so named because it is a clinical
syndrome characterized by recurrent paroxysmal attacks of
severe arthritis that may proceed to a chronic destructive
arthropathy.39,40,42 Like gout, the acute and chronic joint injury is a manifestation of intra-articular crystal deposition,
in this case, calcium pyrophosphate dihydrate
(Ca2P2O7
.2H2O). In addition to deposits in the synovial
membrane and periarticular tissues, crystals also are found in
hyaline articular cartilage, fibrocartilaginous menisci, and
intervertebral disks (chondrocalcinosis).43-46 Chondrocalcinosis
affects up to 15% of adults older than 65 years, and
radiographically detectable deposits are present in the
hyaline and fibrocartilage of the knees, symphysis pubis, and
wrist.39,42 Chondrocalcinosis and pseudogout occur as
primary idiopathic abnormalities in about 90% of affected
persons. Pseudogout also is associated with other metabolic
disorders, including hyperparathyroidism, gout, hemochromatosis,
and hypophosphatasia.39
Acute pseudogout arthritis most commonly develops in
the knee. Patients typically seek care because of an acutely
inflamed joint. Synovial fluid aspiration reveals an elevated
polymorphonuclear leukocyte count and free and intracellular
calcium pyrophosphate dihydrate crystals (within
neutrophils). These crystals are considerably shorter than
monosodium urate crystals and are rhomboidal rather than
needle-shaped.43-46 In addition, they demonstrate positive
birefringence when examined with compensated polarized
light. Chronic pyrophosphate arthropathy refers to an accelerated
form of destructive arthritis that radiographically and
clinically closely resembles severe osteoarthritis.42
Pathology.—Grossly, the synovial deposits of calcium
pyrophosphate dihydrate appear as flecks of chalky white
material on the surface of the membrane. These rarely
achieve the large size of gouty deposits. In addition to the
synovial crystals, similar deposits are present in the articular
cartilage and fibrocartilaginous menisci. Microscopically,
pyrophosphate deposits appear dark blue to purple in nondecalcified
H&E-stained slides.45,46 These deposits have a
distinctly granular appearance that may be enhanced by
lowering the microscope condenser or reducing the intensity
of the light source ❚Image 12❚.
Examination with polarizing
light usually identifies only a few short rhomboidal crystals;
however, a larger number of crystals may be seen on
unstained slides.43,44 Within the articular cartilage and fibrocartilage,
the crystal deposits characteristically are not associated
with a histiocytic or foreign body giant cell reaction.
However, the chondrocytes in the vicinity of the deposits
may exhibit “degenerative” features, including swelling and a
basophilic alteration of the adjacent cartilage matrix.45 These
cells are thought to represent the source of the pyrophosphate
that forms the crystalline deposits.45 The synovial deposits
are associated with small foci of metaplastic cartilage, and
these more commonly elicit a histiocytic reaction.45 Decalcification
of tissue often results in complete removal of the
crystals and leaves oval to rounded pools of basophilic material.
They often lack a cellular reaction and may be overlooked
easily. Like the gouty deposits that have been
dissolved in aqueous solution, the regions of decalcified
pyrophosphate demonstrate a fibrillar or feathery appearance;
however, the striations are shorter than those in gouty tophi.
Basic Calcium Phosphate (Hydroxyapatite) Crystal
Deposition Disease
Hydroxyapatite crystal deposition disease is the least
well known but possibly the most common of these disorders.
39 The basic calcium phosphates are the calcium crystals that are found in periarticular soft tissues, most frequently
around the shoulder joint, and are responsible for the clinical
syndrome known as calcific tendinitis.47-49 These crystals
also may be found in tendons and synovial sheaths at
multiple other locations and in intervertebral disks.50 Clinically,
calcific tendinitis produces recurrent acute episodes of
shoulder pain that frequently evolves into chronic shoulder
disability.39,50 Intra-articular deposition of the basic calcium
salts may produce a rapidly destructive arthritis. This accelerated
arthritis is most common in elderly women and may
occur in any joint.51 Unlike gout and pseudogout, which are
associated with acute synovitis, in hydroxyapatite crystal
deposition disease, the destructive arthritis and synovitis lack
an acute inflammatory component. Pathology.—Synovial deposition of basic calcium phosphate
is associated with a papillary and fibrous thickening of
the membrane.50 Macroscopically, recognizable crystal
deposits appear cream-white and occasionally aggregate to
produce small cysts that discharge viscous, paste-like material
when incised.50 Individual calcium hydroxyapatite crystals
are extremely small, measuring only 75 to 250 nm, and
they cannot be resolved by the light microscope. Specific
identification of these crystals, therefore, can be accomplished
only by transmission electron microscopy or x-ray
diffraction studies.49-51 By light microscopy, the crystals may
be recognized when they aggregate into large clumps. The
crystals stain blue-purple by H&E before decalcification and
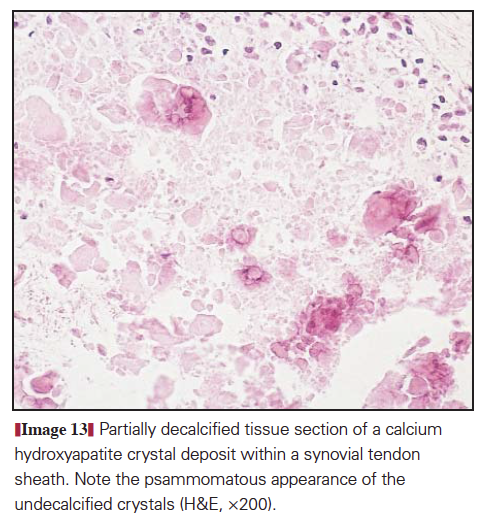
palely eosinophilic or basophilic after decalcification.47,50
The undecalcified crystal aggregates are poorly refractile and
do not exhibit birefringence. A laminated psammomatous
appearance usually can be appreciated in at least some of
them ❚Image 13❚.47
In joint fluids, the aggregated crystals
form irregularly sized and shaped microspheroids. In soft
tissue, the hydroxyapatite is associated variably with a histiocytic
or foreign body giant cell reaction; however, a
neutrophilic inflammatory reaction is not seen.50 Intra-articular
deposition of the crystals frequently is associated with
severe destructive degenerative joint disease.52 It is postulated
that histiocytic and synovial ingestion of the crystals
stimulates proteolytic enzyme release that contributes to the
breakdown of cartilage and tendon.50 Crystal deposition in
tendons near their osseous origin or insertion may result in
cortical erosion and simulate a malignant bone neoplasm.53
Synovial Reaction to Loosened Joint
Arthroplasties
Large Joint Detritic Synovitis
Large joint arthroplasty is one of the most common
elective orthopedic surgical procedures performed. More
than 120,000 such operations are performed each year in the
United States, and the results of these are generally
excellent.54 Complications are few; however, as arthroplasties
have been performed on younger and more physically
active patients, an increased incidence of aseptic loosening
of the prostheses has occurred.55 This loosening occurs
because the materials used in large joint reconstruction, ie,
polyethylene, metal alloys, and methyl methacrylate (bone
cement), although highly durable and relatively inert, have a
tendency to undergo mechanical failure over time, particularly
with excessive use. In vivo, this mechanical failure
usually is manifested by progressive fragmentation of the
components.54,56,57 This fragmentation occurs at the interface
between moving parts of the artificial joint or between host
tissue and foreign material. The net result is that microscopic
fragments of the arthroplasty components are extruded into
the joint cavity where they elicit an inflammatory reaction.
54,56,57 This reaction usually is accompanied by osteolysis
of the involved bones, producing clinically detectable
loosening of the arthroplasty. The cardinal symptom of loosened
prostheses is progressive pain.55
Pathology
Detritic synovitis is the descriptive term applied to the
constellation of changes seen in the synovium and soft tissue
that surrounds loose large joint arthroplasties. The most
commonly involved joints are the hips and knees. Detritic
synovitis manifests as red-tan nodular thickening of the
synovium.54 In a few cases, the synovium may be black
owing to the extensive deposition of metal debris.
In detritic synovitis, particles of synthetic material in the
synovium are associated with an intense histiocytic and
foreign body giant cell reaction.54,56,57 The histiocytes are
oval and rounded and have abundant eosinophilic foamy to
granular cytoplasm. Nuclei are central and round and lack
nucleoli. Mitoses are not seen. Three types of foreign material
are recognizable.54 Methyl methacrylate is dissolved
during tissue processing. It elicits a foreign body giant cell
reaction that surrounds large oval and rounded defects. The
defects appear empty but often contain fine granules of
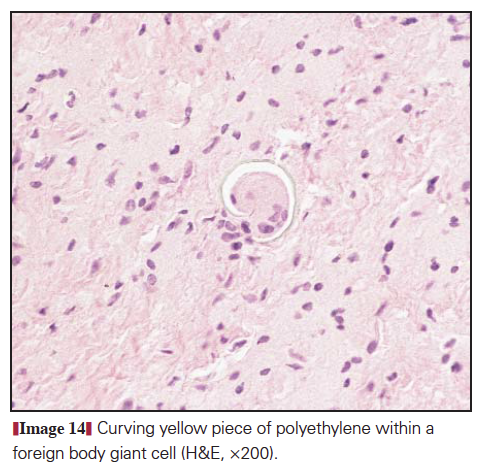
refractile nonpolarizable barium.54 Needle-shaped fragments
of polyethylene also are found in foreign body giant
cells.54,56,57 These fragments are typically small and may be
overlooked unless the slides are examined under polarized
light. Larger pieces of polyethylene appear green-yellow
with conventional H&E stains ❚Image 14❚.54
The metal debris
is the most inconspicuous and, therefore, most easily overlooked
of the foreign material. Although the metal particles
rarely exceed 50 μm, most pieces measure less than 1 μm
and are dispersed evenly as single fragments in the cytoplasm
of histiocytes.54,56,57 Additional histologic findings
include papillary fibrocartilaginous metaplasia of the
synovial surface, sheets of coagulative necrosis without
inflammation, aggregates of hemosiderin-laden macrophages,
and, in a few cases, reactive myofibroblastic proliferations
that resemble nodular-proliferative fasciitis.54 Stromal
infiltrates of neutrophils are correlated strongly with bacterial
infection surrounding the prosthesis.54,56,57
Particles of metal and polyethylene and the typical histiocytic
reaction that accompanies them can be found in
regional lymph nodes. The lymph nodes often are enlarged
and may be suggestive of malignant tumor.58 This can result
in confusion at the time of staging procedures performed
during treatment of pelvic malignant neoplasms, usually
prostatectomy in men and hysterectomy and oophorectomy
in women.
Detritic synovitis occurs in a background of loose large
joint prostheses, and, hence, its management revolves around
reconstruction of the affected joint. This frequently is troublesome
because of the severe localized osteoporosis that
usually accompanies loosening of the prosthesis.
Small Joint Detritic Synovitis
The prostheses used to replace damaged small synovial
joints, such as those in the hands and feet, are different from
those used for large joint arthroplasty. Small joint prostheses
are composed of silicone polymers. Silicone (dimethylsiloxane)
is composed of carbon, oxygen, hydrogen, and
silica. Depending on the length of polymer chain and the
degree of cross-linking between individual chains, silicone
may have the properties of a liquid, a gel, or a solid. The
solid silicone prostheses, which often are referred to by their
proprietary name, Silastic, have been used extensively for
small joint reconstruction. Like their large joint counterparts,
they have, for the most part, been extremely successful for
alleviating pain and dysfunction. Unfortunately, as with large
joint arthroplasties, a minority of patients encounter problems
due to mechanical failure, particularly in joints
subjected to great degrees of stress and activity, such as the
thumb and hallux.59-61 The abraded silicone particles are
capable of eliciting an inflammatory reaction that differs
somewhat from large joint detritic synovitis.
Pathology
Small joint detritic synovitis produces a nodular thickening
of synovial membrane similar to its large joint counterpart.
59-61 Blackening of the membrane does not occur since
metal alloys are not a part of these prostheses. Microscopically,
the subsynovial space is expanded by a histiocytic and
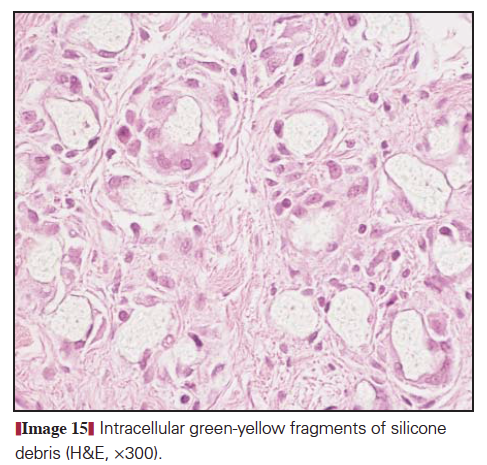
multinucleated giant cell infiltrate that surrounds small fragments
of yellow-green lobulated foreign material (the fragmented solid phase silicone).59-61 This material predominantly occurs in the cytoplasm of mononuclear histiocytes, synovial cells, and multinucleated giant cells; however, small pieces may be found in an entirely extracellular location ❚Image 15❚.
Solid silicone is refractile but not birefringent
and, hence, is not visible when viewed with polarized
light.59-61 Neutrophils typically are not found unless there is
a coexistent bacterial infection. Other changes in the
synovial membrane include scattered lymphocytes and
plasma cells, strands of fibrous tissue, and embedded shards
of bone. The latter probably arise from the adjacent bones, which also may contain large amounts of silicone particles.
60,61 In a few cases, the intraosseous silicone elicits
intense osteoclastic resorptive activity that may produce radiographically
and surgically detectable cystic defects.62 Silicone
synovitis is managed by thorough curettage and reconstruction
of the affected joint, if possible.