
내장기 도수치료(Visceral Manipulation)란?
내장기 도수치료(영어로 Visceral Manipulation, VM)는
오스테오패시(osteopathy) 매뉴얼 테라피의 한 분야로,
손을 이용해 내장 기관(위, 간, 장, 자궁 등)과 주변 근막·인대의 긴장과 유착을 풀어주는 치료법입니다.
프랑스 오스테오패스 Jean-Pierre Barral이 개발했으며,
내장 기관의 자연스러운 이동성(mobility: 외력에 대한 움직임)과
운동성(motility: 내장 자체의 미세 리듬)를 회복하는 데 초점을 맞춥니다.
이는 근골격계 문제뿐 아니라
소화불량, 변비, 만성 통증, 골반 통증 등 내장 관련 증상에 적용됩니다.
사용자가 공유한 논은
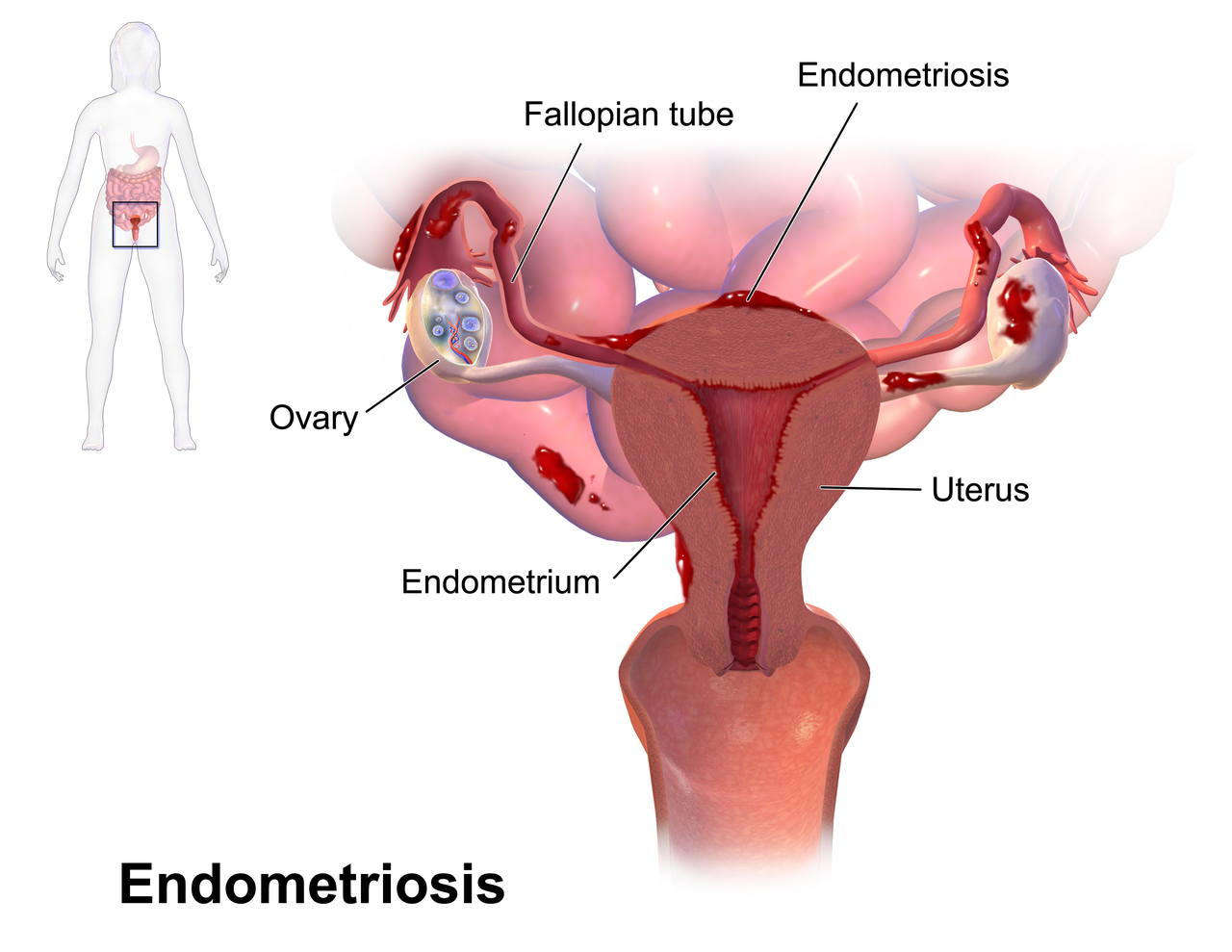
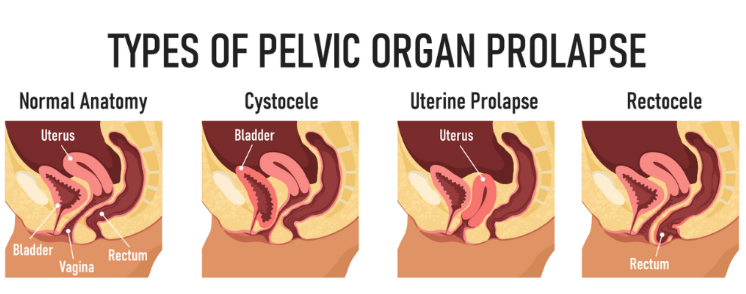
자궁내막증(endometriosis)과 골반장기탈출(pelvic organ prolapse) 여성 60명을 대상으로 한 연구입니다.
주 1회 5주간 내장기 조작을 적용한 결과,
삶의 질(WHOQOL-BREF 점수)이 유의하게 개선되었으나(자궁내막증 그룹 p=0.0001, 탈출 그룹 p=0.0093),
자세 안정성은 큰 변화가 없었습니다.
이는 내장기 조작이 비침습적·비약물적으로 삶의 질을 높일 수 있음을 시사합니다.
아래는 치료 시술의 일반적인 모습입니다.

기전(Mechanism)
내장기 도수치료의 작용 기전은 해부학·생리학·신경학에 기반합니다.
주요 포인트는 다음과 같습니다:
- 근막 연결과 이동성 회복: 내장 기관은 복막·인대·근막으로 서로 연결되어 있습니다. 염증, 수술, 외상 등으로 유착(adhesions)이 생기면 이동성이 제한되고, 이는 통증이나 기능 장애를 유발합니다. 치료로 근막 긴장을 풀면 내장 기관이 자유롭게 움직이며 혈액·림프 순환이 개선됩니다.
- 자율신경계 영향: 내장-체성 반사(viscerosomatic reflex)를 통해 내장 문제는 근골격계 통증(예: 요통)을 일으킬 수 있습니다. 반대로 치료는 교감신경 과흥분을 완화하고 부교감신경을 활성화해 소화·순환을 촉진합니다. 엔터릭 신경계(enteric nervous system, 장 내 독립 신경망)도 영향을 받아 장 운동이 정상화됩니다.
- 통증 완화: 만성 염증이나 유착은 통각수용체를 자극해 중추 감작(central sensitization)을 일으킵니다. 부드러운 조작은 C-tactile 섬유를 자극해 통증 신호를 억제하고, 인터오셉션(interoception: 내부 감각)을 개선합니다.
- 체액 순환과 항상성: 오스테오패시 창시자 Andrew Taylor Still의 원리에 따라, 체액(혈액·림프) 순환 장애가 질병 원인이라고 봅니다. 치료로 순환을 촉진해 조직 영양과 해독을 돕습니다.
논문에서도 이러한 기전을 언급하며, 수술 후 흉터·유착이 내장 이동성을 저하시키고 통증을 유발한다고 설명합니다.
치료 방법(Treatment Methods)
치료는 숙련된 치료사가 손으로 직접 시행하며, 강한 압력이 아닌 부드럽고 정밀한 터치가 핵심입니다.
일반적인 접근은 다음과 같습니다:
- 평가 단계: 환자가 누운 상태에서 복부에 손을 얹고 내장 기관의 리듬·이동성·긴장 부위를 촉진(palpation)으로 평가합니다.
- 기본 기법:
- 직접 기법(Direct Technique): 제한된 방향으로 부드럽게 압박·스트레칭해 유착을 풀음 (예: 10초 압력 후 반복).
- 간접 기법(Indirect Technique): 기관이 자연스럽게 움직이는 방향으로 따라가며 긴장을 유도해 풀음.
- 구체적 기술 예시 (논문에서 사용된 방법 포함):
- 횡격막(diaphragm) 이완: 호흡과 내장 움직임의 기반.
- 골반 횡격막·요도생식기 횡격막 이완.
- 자궁·난소·나팔관 일반 이완 및 이동(mobilization).
- 광인대(broad ligament)·치골능절인대 스트레칭.
- 간·위·장 등 특정 기관 대상 조작 (예: 간은 후상방으로 완만히 이동).
세션은 보통 20~40분, 주 1~2회 진행되며, 4~10회 코스가 일반적입니다.
J Clin Med
. 2025 Jan 24;14(3):767. doi: 10.3390/jcm14030767
The Effect of Osteopathic Visceral Manipulation on Quality of Life and Postural Stability in Women with Endometriosis and Women with Pelvic Organ Prolapse: A Non-Controlled Before–After Clinical Study
Małgorzata Wójcik 1,*, Małgorzata Kampioni 2, Zuzana Hudáková 3,4, Idzi Siatkowski 5, Witold Kędzia 6, Grażyna Jarząbek-Bielecka 6
Editors: Camran R Nezhat, Christian Lunghi, Federica Tamburella
- Author information
- Article notes
- Copyright and License information
PMCID: PMC11818518 PMID: 39941438
Abstract
Background: Visceral manipulation is a soft tissue manual work technique that originates from and is classified within the Osteopathic Manipulative Technique (OMT), focusing on the fascial tissue mobilisation of the visceral system. Manual therapy on internal organs is based on anatomy, physiology and physics.
Methods: Sixty women with endometriosis and pelvic organ prolapse, aged 41.5 ± 12.02, participated in the study. The women had manipulation therapy once a week for 5 weeks. The World Health Organisation Quality of Life BREF questionnaire and a postural stability assessment were administered before and after performing visceral manipulation.
Results: The p-value = 0.0093 obtained in the group with prolapses and the p-value = 0.0001 in the group with endometriosis indicated that the applied visceral manipulation improved the women’s quality of life. No effect of therapy was observed on postural stability.
Conclusions: Visceral manipulation improved the quality of life of both study groups of women. A significant difference was also observed when comparing the two groups for area.
배경:
내장기 조작(visceral manipulation)은 연조직 수기 기술로,
오스테오패시 조작 기법(Osteopathic Manipulative Technique, OMT)에 속하며
내장 시스템의 근막 조직 이동화에 초점을 맞춘다.
내장 기관에 대한 수기 요법은 해부학, 생리학, 물리학에 기반한다.
방법:
자궁내막증과 골반장기탈출 진단을 받은 60명의 여성(평균 연령 41.5 ± 12.02세)이 연구에 참여하였다.
여성들은 5주 동안 주 1회 내장기 조작 요법을 받았다.
내장기 조작 시행 전후에 세계보건기구 삶의 질 간략 설문지(WHOQOL-BREF)와 자세 안정성 평가를 실시하였다.
endometriosis and pelvic organ prolapse
결과:
탈출군에서 p-value = 0.0093, 자궁내막증군에서 p-value = 0.0001로,
적용된 내장기 조작이 여성들의 삶의 질을 개선한 것으로 나타났다.
자세 안정성에는 요법의 효과가 관찰되지 않았다.
결론:
내장기 조작은 두 연구 그룹 여성들의 삶의 질을 개선하였다.
두 그룹을 비교했을 때 면적(area)에서 유의한 차이가 관찰되었다.
1. Introduction
Visceral manipulation is a soft tissue manual work technique that originated from and is classified within the Osteopathic Manipulative Technique, focusing on the mobilisation of the fascial tissues of the visceral system [1,2]. Gynaecological conditions should be considered as related to somatic dysfunction (SD) [3], which is defined as an altered function that is associated with inflammation and palpable symptoms in body structures in different regions of the body [4,5].
Manual therapy on internal organs is based on anatomy, physiology and physics, the study of which has provided the following information. (1) Visceral structures have a significant mass and are subject to the laws of physics just like the musculoskeletal system [6,7]. (2) Internal organs are connected to each other through a two-layered system of serous membranes, i.e., the pleurae, pericardium and peritoneum [8,9]. (3) Visceral structures are connected to each other through an extensive network of fascial connections [10,11,12,13]. (4) Nociceptive stimuli direct pain to the somatic system via the visceral reflex. The homeostatic afferent pathway is a sensory adjunct of the autonomic nervous system that carries signals from the primary small-diameter Adelta and C afferent fibres, representing the physiological state of each tissue of the body [14,15]. Visceral nociceptors are activated by ischaemia and inflammation [16,17,18]. (5) Intestinal wall contraction is regulated by a rich neuronal network that functions independently of the central nervous system [19]. (6) Visceral dysfunction, e.g., inflammation, contributes to central sensitisation and chronic pain states [20,21]. (7) Abdominal and thoracic wall scarring resulting from surgical procedures affects the soft tissues. Loss of mobility runs from the epidermis through subcutaneous tissue to muscular and visceral structures, which can contribute to local tissue dysfunction and pain conditions [13,22]. (8) Adhesions occur following trauma, surgery, tumours and inflammatory processes [23,24]. Adhesions are innervated and are capable of generating pain. They may contribute to constipation, small bowel obstruction, pelvic pain and infertility [25,26].
Visceral manipulation aims to improve or regain the mobility of internal organs [27]. Visceral manual therapy takes into account the three-dimensional dynamics of human body biomechanics, including musculoskeletal and musculo-fascial structures, the connective tissues of organs and reflex activities in the central and peripheral nervous system, including circulation and fluid drainage in the human body [28].
The internal organs, the muscular system and all other systems and structures in the human body must be understood in terms of the connective tissue that surrounds them and the body fluids that flow through them, i.e., blood and lymph [29]. In order to improve the health and how the human body functions, it is necessary to consider the effects on the aforementioned structures and especially the surrounding connective tissue and body fluids (blood and lymph) [29]. Andrew Taylor Still, who is the founder of osteopathy, believed that the cause of dysfunction/disease in the human body is an impaired circulation of body fluids [30]. In the case of internal organs, visceral dysfunction is said to be defined as the impaired mobility of the visceral structure and all associated muscular, neurological, vascular, lymphatic and bony components [31].
Endometriosis, i.e., the presence of endometrial tissue called the endometrium outside the uterine cavity, and pelvic organ prolapse are conditions that negatively affect women’s quality of life. This is particularly true in terms of their sexual life, social relationships and work [32,33]. The most common treatments for endometriosis are hormone therapy, physical medicine treatments and diet [34,35,36]. Pelvic floor muscle strengthening exercises are also used to treat pelvic organ prolapse [37]. Organ prolapse is often accompanied by urinary incontinence [36]. Depending on medical indications, both conditions are treated surgically [38,39].
Abnormalities in muscle and fascial tone in the pelvic region can affect postural stability [13]. Postural stability refers to the ability to hold the body in a position to perform a task successfully. Postural stability requires adequate postural muscle strength and neuromotor control. Pelvic floor dysfunction leads to abnormalities in the pelvic–lumbar complex, affecting stability and posture [13,40]. Correct posture and abdominal muscle tone affect normal pelvic floor muscle tone, which in turn affects urinary continence [41]. Patients with endometriosis often adopt a flexed position of their body (they have a deepened thoracic kyphosis of the spine) due to pain, which in turn influences the adoption of an abnormal body posture [42].
1. 서론
내장기 조작은 연조직 수기 기술로,
오스테오패시 조작 기법에서 유래하였으며
내장 시스템의 근막 조직 이동화에 초점을 맞춘다[1,2].
부인과 질환은
체성 기능장애(somatic dysfunction, SD)와 관련이 있는 것으로 고려되어야 한다[3].
체성 기능장애는
신체 여러 부위의 구조에서 염증 및 촉진 가능한 증상과 관련된 기능 변화로 정의된다[4,5].
내장 기관에 대한 수기 요법은
해부학, 생리학, 물리학에 기반하며,
이들 학문의 연구를 통해 다음과 같은 정보를 얻었다.
(1) 내장 구조는 상당한 질량을 가지며 근골격계와 마찬가지로 물리법칙의 적용을 받는다[6,7].
(2) 내장 구조는 장막(pleurae, pericardium, peritoneum)의 이중층 시스템을 통해 서로 연결되어 있다[8,9].
(3) 내장 구조는 광범위한 근막 연결 네트워크를 통해 서로 연결되어 있다[10,11,12,13].
(4) 통각 자극은 내장-체성 반사(visceral reflex)를 통해 체성 시스템으로 통증을 전달한다.
항상성 구심 경로는 자율신경계의 감각 보조 경로로,
신체 각 조직의 생리 상태를 나타내는 소직경 Adelta 및 C 구심 섬유에서 신호를 전달한다[14,15].
내장 통각수용체는 허혈과 염증에 의해 활성화된다[16,17,18].
(5) 장벽 수축은 중추신경계와 독립적으로 작동하는 풍부한 신경 네트워크에 의해 조절된다[19].
(6) 내장 기능장애(예: 염증)는 중추 감작(central sensitisation)과 만성 통증 상태에 기여한다[20,21].
(7) 수술로 인한 복부 및 흉부 벽 흉터는 연조직에 영향을 미친다.
이동성 상실은 표피에서 피하조직, 근육 및 내장 구조로 이어져 국소 조직 기능장애와 통증 상태에 기여할 수 있다[13,22].
(8) 유착은 외상, 수술, 종양, 염증 과정 후에 발생한다[23,24].
유착은 신경분포를 가지며 통증을 유발할 수 있다.
이는 변비, 소장 폐색, 골반 통증, 불임에 기여할 수 있다[25,26].
내장기 조작은
내장 기관의 이동성을 개선하거나 회복하는 것을 목표로 한다[27].
내장 수기 요법은 인체 생체역학의 3차원 동역학을 고려하며,
근골격계 및 근근막 구조, 장기 결합조직, 중추 및 말초 신경계의 반사 활동, 순환 및 체액 배출을 포함한다[28].
내장 기관, 근육 시스템 및 인체의 모든 다른 시스템과 구조는
이를 둘러싼 결합조직과 혈액 및 림프와 같은 체액의 관점에서 이해해야 한다[29].
인체의 건강과 기능을 개선하기 위해서는 앞서 언급한 구조,
특히 주변 결합조직과 체액(혈액 및 림프)에 미치는 영향을 고려해야 한다[29].
오스테오패시의 창시자인 Andrew Taylor Still은
인체의 기능장애/질병 원인이
체액 순환 장애라고 믿었다[30].
내장 기관의 경우,
내장 기능장애는
내장 구조 및 관련 근육, 신경, 혈관, 림프, 골격 구성요소의 이동성 장애로 정의된다[31].
자궁내막증(자궁내막 조직이 자궁강 외부에 존재하는 상태)과 골반장기탈출은
여성의 삶의 질에 부정적인 영향을 미치는 질환이다.
특히 성생활, 사회적 관계, 직업 면에서 그렇다[32,33].
자궁내막증의 가장 흔한 치료는
호르몬 요법, 물리치료, 식이요법이다[34,35,36].
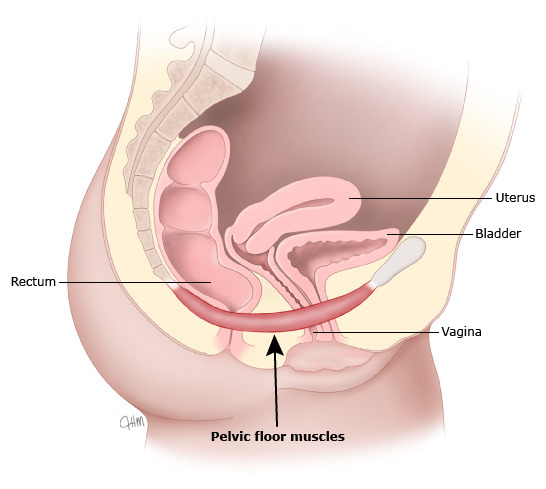
골반장기탈출 치료에는
골반저 근육 강화 운동이 사용된다[37].
장기 탈출은 종종 요실금과 동반된다[36].
의학적 적응증에 따라 두 질환 모두 수술로 치료된다[38,39].
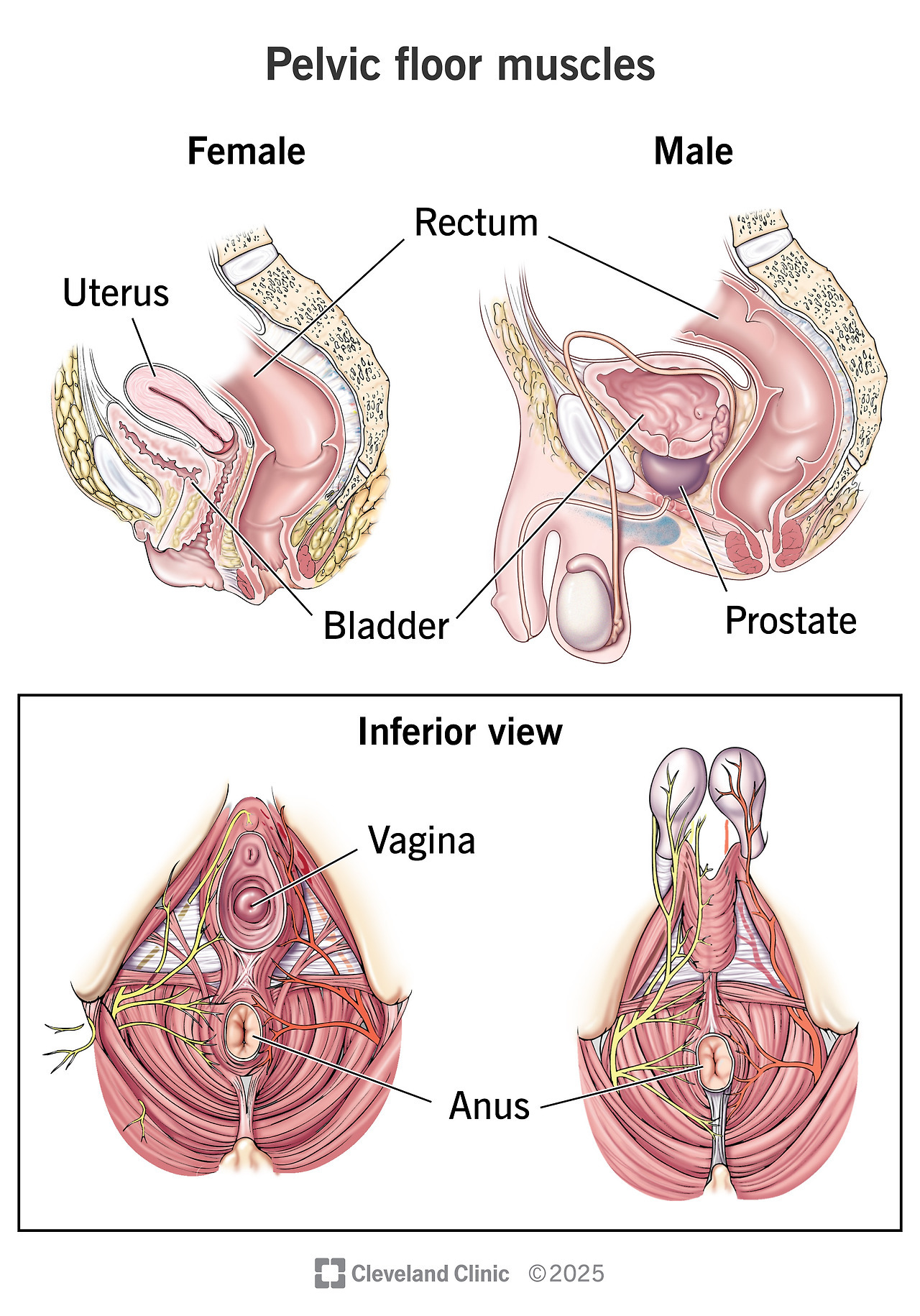
골반 부위의 근육 및 근막 긴장 이상은
자세 안정성에 영향을 미칠 수 있다[13].
자세 안정성은
과제를 성공적으로 수행하기 위해
신체를 특정 위치에 유지하는 능력을 의미한다.
자세 안정성은
충분한 자세 근력과 신경운동 조절을 필요로 한다.
골반저 기능장애는
골반-요추 복합체의 이상을 유발하여 안정성과 자세에 영향을 미친다[13,40].
올바른 자세와 복근 긴장은
정상적인 골반저 근육 긴장에 영향을 미치며,
이는 다시 요실금에 영향을 준다[41].
자궁내막증 환자는
통증으로 인해 신체를 굽힌 자세(흉추 후만증 증가)를 취하는 경우가 많아
비정상적인 자세를 유발한다[42].
With a view to demonstrating the practical use of visceral manipulation, it was decided to test whether this therapy could have an impact on the health of women diagnosed with endometriosis and pelvic floor static disorders. A review by Ruffini et al. provides information on the use of OMT for somatic dysfunction in patients with endometriosis [3]. Although the authors did not include details about the specific treatment techniques used in the included studies, analysing these studies allows for some insights into the osteopathic approaches applied in research within this clinical context. For example, in the case report from Goyal et al. [43], it is noted that the osteopathic treatment consists of all the major diaphragms’ release (pelvic diaphragm, abdominal diaphragm, thoracic outlet and hyoid diaphragm release) during the first session and, in the second session, gastro-oesophageal junction release, sigmoid colon release, cranial therapy to the occiput, sacral release and dural tube rocking. In the pilot study from Sillem et al. [44], it is reported that a standardised approach was used for osteopathic treatment starting with release of musculoskeletal blocks, particularly of the sacroiliac joints. Depending on clinical findings, this was followed by the mobilisation of the diaphragm and abdominal organs using standard techniques. The pelvic floor was released using the so-called grand manoeuvre: the movement of the abdominal organ compartment in a cranial direction. The treatment was concluded in many cases with the mobilisation of the temporomandibular joints and cervical spine. Each patient was prescribed six treatment sessions, of which a median of six were carried out, usually at weekly intervals. Ott presented a case study of a 24-year-old woman who was diagnosed with endometriosis and started hormone therapy. As there were complaints of LBP (lower back pain), pelvic and lower abdominal pain, osteopathic treatment was applied, based on a model based on the patient’s needs. The osteopath applied four sessions of OMT, which had a significant effect on reducing the pain symptoms, so that the hormone therapy started was discontinued after an agreement with the doctor [45]. Daraï and colleagues [46] studied the effect of standardised osteopathic treatment on women with colorectal endometriosis. This study demonstrated the effect of osteopathic treatment in improving women’s quality of life. Another study by Daraï et al. found in women with endometriosis that a single OMT session had a positive effect on pain reduction and led to an improvement in their general health, social functioning and mental health [47].
Prior to the study, the research hypothesis was defined: visceral manipulation applied for 5 weeks (one time per week) has an effect on postural stability parameters and the quality of life of women with pelvic organ prolapse and endometriosis.
내장기 조작의 실용성을 입증하기 위해,
이 요법이 자궁내막증과 골반저 정적 장애 진단 여성의 건강에 영향을 미칠 수 있는지 검증하기로 하였다.
Ruffini 등의 리뷰는
자궁내막증 환자의 체성 기능장애에 대한 OMT 사용 정보를 제공한다[3].
저자들은 포함된 연구에서 사용된 구체적인 치료 기법에 대한 세부사항을 포함하지 않았으나,
이들 연구를 분석하면 해당 임상 맥락에서 연구된 오스테오패시 접근법에 대한 통찰을 얻을 수 있다.
예를 들어, Goyal 등의 증례 보고[43]에서는
오스테오패시 치료가 첫 세션에서 모든 주요 횡격막(골반 횡격막, 복부 횡격막, 흉곽 출구, 설골 횡격막) 이완으로 구성되었고,
두 번째 세션에서는 위식도 접합부 이완, S상결장 이완, 후두부 두개 요법, 천골 이완, 경막관 흔들기 요법으로 구성되었다고 보고되었다.
Sillem 등의 파일럿 연구[44]에서는
오스테오패시 치료에 표준화된 접근법을 사용하였으며,
천골장골 관절을 포함한 근골격계 블록 이완부터 시작하였다.
임상 소견에 따라
횡격막과 복부 장기 이동화를 표준 기법으로 시행하였다.
골반저는
소위 'grand manoeuvre'(복부 장기 구획을 두개 방향으로 이동)로 이완하였다.
많은 경우 치료는
측두하악 관절과 경추 이동화로 마무리되었다.
각 환자는 6회 치료를 처방받았으며,
중간값 6회를 주 1회 간격으로 시행하였다.
Ott은 24세 여성의 자궁내막증 증례를 제시하였으며,
호르몬 요법을 시작하였으나
요통, 골반 및 하복부 통증으로 인해 환자 필요에 기반한 모델로
오스테오패시 치료를 4회 적용하여 통증 증상을 유의하게 감소시켰고,
의사와 합의 후 호르몬 요법을 중단하였다[45].
Daraï 등은 대장 자궁내막증 여성에 대한 표준화된 오스테오패시 치료 효과를 연구하였으며, 이 연구는 오스테오패시 치료가 여성의 삶의 질을 개선하는 효과를 입증하였다[46]. Daraï 등의 또 다른 연구에서는 자궁내막증 여성에서 단일 OMT 세션이 통증 감소에 긍정적 효과를 보였으며 일반 건강, 사회적 기능, 정신 건강을 개선하였다[47].
연구 전에 연구 가설을 정의하였다: 5주 동안(주 1회) 적용된 내장기 조작은 골반장기탈출과 자궁내막증 여성의 자세 안정성 매개변수와 삶의 질에 영향을 미친다.
2. Materials and Methods
2.1. Type of Study and Participants
Sixty women (n = 30) with endometriosis and n = 30 with pelvic organ prolapse, aged 41.5 ± 12.02, participated in the study. Recruitment of the women participating in the study was conducted over a one-year period. At the time of recruitment, women were interviewed with regard to the study’s inclusion and exclusion criteria. Participants in the study were women who self-referred for osteopathic treatment. Inclusion criteria were as follows: use of surgical treatment only, use of visceral manipulation at the latest one month after surgical treatment, no history of physiotherapy or osteopathy, no concomitant medical conditions (e.g., diabetes, hypertension), no medication, no stimulants or depressants used (e.g., drinking alcohol or smoking) and written consent provided to participate in the study in accordance with the Declaration of Helsinki. Exclusion criteria were as follows: failure to meet the inclusion criterion, inability to attend a visceral therapy session, e.g., due to infection, and lack of written consent to participate in the study. Prior to the visceral manipulation being performed, study participants were informed how it was to be performed and that they could opt out at any stage of the study. Participation in the study was entirely voluntary and the visceral manipulation was performed free of charge.
2.2. Visceral Manipulation
Visceral manipulation was performed between 3.00 p.m. and 8.00 p.m. in a warm and quiet room on women with endometriosis and pelvic organ prolapse after surgical treatment. During the visceral manipulation, the study participant lay on her back in her underwear on an adjustable therapy table. Visceral manipulation was performed on all study participants by the same therapist and was performed one time per week for 5 weeks. The following procedures were performed: diaphragm muscle relaxation, a general technique to relax the pelvic diaphragm and urogenital diaphragm, stretching of the pubococcygeal ligament, relaxation of the curtain membrane, a general technique to relax the uterus, a general technique to relax the ovaries and fallopian tubes, and mobilisation of the uterine broad ligament [48]. Stretching pressure lasting 10 s was applied during visceral manipulation and repeated until the patient felt no soft tissue stretching. The duration of the session for each patient was 20 min, timed using a stopwatch. Visceral manipulation was performed by only one person, an experienced physiotherapist with twenty-eight years of experience, and a certified osteopath with six years of experience. In the event of a study woman being unable to attend a session, e.g., due to an infection, visceral therapy was not rescheduled and the woman in question was excluded from further participation in the study. As the proposed number of sessions was five, one per week, we structured the sessions with a fixed schedule on designated days of the week to ensure a weekly interval was maintained, thus ensuring a fixed protocol for all participants in the study.
내장기 조작은 오후 3시부터 8시 사이에 따뜻하고 조용한 방에서,
수술 치료를 받은 자궁내막증과 골반장기탈출 여성들을 대상으로 시행되었다.
내장기 조작 동안 연구 참여자는
속옷 차림으로 조절 가능한 치료 테이블에 바로 누운 자세를 취하였다.
모든 연구 참여자에 대한 내장기 조작은
동일한 치료사 한 명이 시행하였으며,
5주 동안 주 1회 실시되었다.
다음과 같은 시술이 수행되었다:
횡격막 근육 이완,
골반 횡격막과 비뇨생식기 횡격막을 이완시키는 일반 기법,
치골미골인대(pubococcygeal ligament) 스트레칭,
막막(curtain membrane) 이완,
자궁을 이완시키는 일반 기법,
난소와 나팔관을 이완시키는 일반 기법,
그리고 자궁 광인대(uterine broad ligament)의 이동화(mobilisation)[48].
내장기 조작 동안 10초 동안 지속되는 스트레칭 압력을 가하였으며,
환자가 연조직 스트레칭을 더 이상 느끼지 않을 때까지 반복하였다.
각 환자의 세션 시간은 20분으로, 스톱워치로 측정하였다.
내장기 조작은 28년 경력의 숙련된 물리치료사이자 6년 경력의 인증된 오스테오패스 한 명만이 시행하였다.
연구 참여 여성 중 감염 등으로 인해 세션에 참석하지 못하는 경우, 내장 요법은 재조정되지 않았으며 해당 여성은 연구의 추가 참여에서 제외되었다. 제안된 세션 수는 주 1회 총 5회였으므로, 우리는 지정된 요일에 고정된 일정을 구성하여 주간 간격을 유지하도록 하였고, 이에 따라 연구의 모든 참여자에게 고정된 프로토콜을 보장하였다.
2.3. Outcome Measures: Quality of Life and Postural Stability
The study used the standardised World Health Organisation Quality of Life BREF (WHOQOL-BREF) questionnaire. On the day of visceral manipulation, the women completed a questionnaire anonymously before it was performed. On the last day, post-session, the participants also completed a questionnaire anonymously. For the purpose of this publication, the individual domains of the questionnaire were not analysed. The maximum number of points that the respondent could receive was 130 and the minimum was 26 points.
Postural stability was also evaluated before the visceral therapy session and after the last session. Postural stability (anterior–posterior, lateral–medial pivoting and postural field) was assessed using the Computerised Stability Platform CQStab2P-vUSB-1506. The test was conducted with the participants’ eyes open for 30 s. The subject stood on the platform barefoot, with the upper limbs along the torso and looking ahead. After the test was completed, a report of postural stability parameters was produced in the device’s computer programme. The values of anterior–posterior and lateral–posterior swings and the ellipse area of the centre of gravity were taken into account for statistical analysis. The smaller the values for excursion and ellipse area, the better the postural stability. Individual manufacturers of stabilometric platforms do not provide standards for healthy or sick people. The outcome assessor was not aware of the aim of the study.
2.4. Statistical Analysis
The data collected were statistically analysed. As a normal distribution of numbers was not observed, the Wilcoxon test was applied to test whether visceral manipulation has a significant effect on improving quality of life and postural stability values of the groups of women studied. A comparison was also made between the group of women with endometriosis and the group of patients with pelvic organ prolapse as to whether visceral manipulation affected quality of life and postural stability values in the study groups, also using the Wilcoxon test. The results are also presented as boxplots. The R statistical package [49] was used for this analysis. The statistical analysis was carried out by an experienced mathematician and statistician. The study was carried out after the approval of the Bioethics Committee of Poznan University of Medical Sciences No. 305/23 and after written consent of the study participants was obtained. In addition, the study was registered in the Clinical Trials Registry (Registry ID: NCT05978414).
3. Results
A total of 96 women with surgical treatment were enrolled in the study (42 with endometriosis and 54 with pelvic organ prolapse), of whom 30 were excluded because they did not meet the criteria for participation. A total of 66 women started the study. During its course, three women (with endometriosis) were excluded because they could not attend the scheduled visceral manipulation session and three women (with pelvic organ prolapse) dropped out on their own accord after the first visceral therapy session. After the visceral manipulation sessions, the women reported no side effects.
Before proceeding to the statistical analysis, a check was made to see if there was a normal distribution of numbers. Since it was not observed, the Wilcoxon test was used to determine whether the visceral manipulation improved the quality of life of the women with endometriosis and pelvic organ prolapse. The p-value = 0.0093 (Table 1, Figure 1) obtained in the group of women with pelvic organ prolapse and the p-value = 0.0001 (Table 1, Figure 1) in the group of women with endometriosis indicate that the applied visceral manipulation improved the quality of life of the women.
Table 1.
Quality of life of women with endometriosis and pelvic organ prolapse before and after visceral manipulation.
Groupp-Value
| endometriosis WHOQOL BREF | 0.0001 |
| pelvic organ prolapse WHOQOL BREF | 0.0093 |
Figure 1.
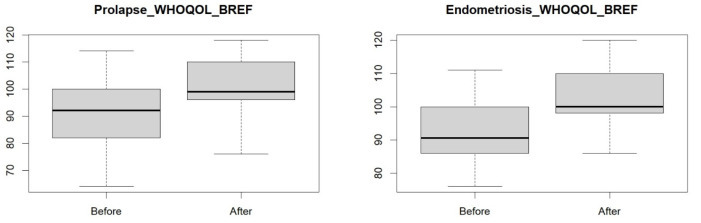
Quality of life in a group of women with endometriosis and pelvic organ prolapse before and after visceral manipulation.
Next, a comparison was made between the study groups of women with endometriosis and pelvic organ prolapse before the visceral manipulation to determine whether the study groups differed. The resulting p-value = 0.9882 (Figure 2) indicates that the study groups did not differ, i.e., both study groups had a similar quality of life. Also, after the visceral manipulation, the two groups did not differ in terms of p-value = 0.2254 (Figure 2), meaning that after the therapy, both groups of women had a similar quality of life.
Figure 2.
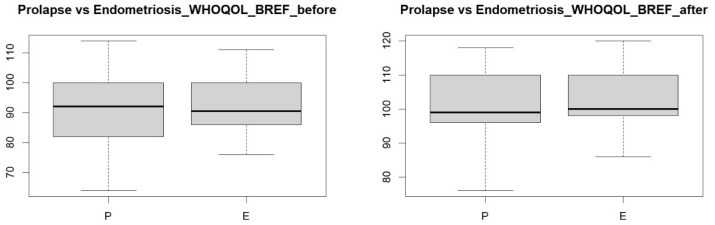
Comparison of quality of life between groups of women with endometriosis and pelvic organ prolapse before and after visceral therapy.
The next step in the statistical analysis was to see if the visceral manipulation influenced postural stability values. For this group of data, a normal distribution was not observed either; thus, the Wilcoxon test was applied to determine whether the visceral manipulation affected the values of postural stability in the group of women with pelvic organ prolapse and endometriosis. The Wilcoxon test was also used to make comparisons between the study groups of women. The results are presented as boxplots.
The values obtained for postural stability showed no effect of the visceral manipulation in both study groups of women with their eyes open for anterior–posterior and lateral–medial tilt and area (Table 2, Figure 3 and Figure 4).
Table 2.
Postural stability values of a group of women with endometriosis and pelvic organ prolapse with their eyes open for anterior–posterior pivot (EOAP: eyes-open anterior–posterior), lateral–medial pivot (EOML: eyes-open medial–lateral) and surface area (EOSA: eyes-open surface area).
Groupp-Value
| endomertiosis EOAP | 0.4158 |
| endometriosis EOML | 0.9234 |
| endometriosis EOSA | 0.3827 |
| pelvic organ prolapse EOAP | 0.6152 |
| pelvic organ prolapse EOML | 0.9117 |
| pelvic organ prolapse EOSA | 0.6843 |
Figure 3.
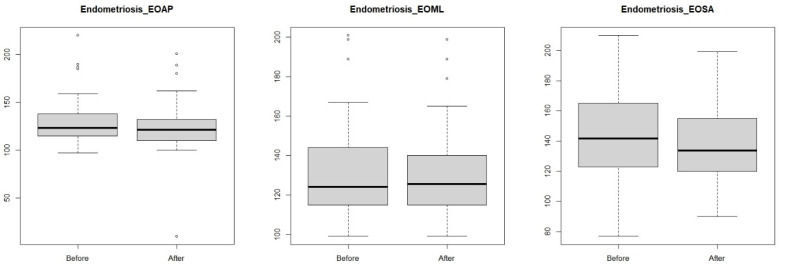
Anterior–posterior (eyes-open anterior–posterior) and lateral–medial (eyes-open medial–lateral) outcrops and surface area (eyes-open surface area) in a group of women with endometriosis before and after visceral manipulation.
Figure 4.
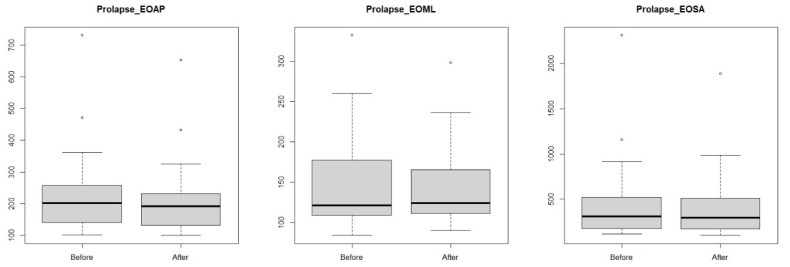
Anterior–posterior (EOAP: eyes-open anterior–posterior) and lateral–medial (eyes-open medial–lateral) outcrops and surface area (eyes-open surface area) in a group of women pelvic organ prolapse before and after visceral manipulation.
A comparison was then made between the study groups of women with endometriosis and pelvic organ prolapse. No significant statistical value was observed between the study groups for anterior–posterior and lateral–medial pivoting (Table 3, Figure 5), meaning that these values were similar in the two study groups after the visceral manipulation. A significant statistical value was observed for the area after the visceral manipulation, which means that the study groups differed (Figure 5).
Table 3.
Comparison between study groups of women with endometriosis and pelvic organ prolapse in terms of their postural stability values with their eyes open for anterior–posterior pivoting (EOAP: eyes-open anterior–posterior), lateral–medial pivoting (EOML: eyes open medial–lateral) and surface area (EOSA: eyes-open surface area).
Groupp-Value
| endometriosis vs. pelvic organ prolapse EOAP | 0.558 |
| endometriosis vs. pelvic organ prolapse EOML | 0.5385 |
| endometriosis vs. pelvic organ prolapse EOSA | 0.0221 |
Figure 5.
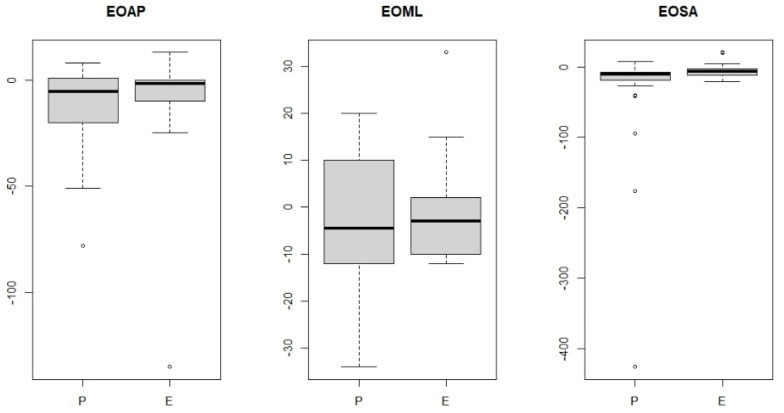
Comparisons of endometriosis (E) vs. pelvic organ prolapse (P) groups for anterior–posterior pivoting (EOAP: eyes-open anterior–posterior), lateral–medial pivoting (EOML: eyes-open medial–lateral) and surface area (EOSA: eyes-open surface area).
4. Discussion
The World Health Organisation (WHO) defines quality of life as a person’s perception of their position in life in the context of the culture and value system in which they live, in relation to their goals, expectations, standards and concerns [43]. A cross-culturally applicable quality of life assessment was developed by the WHOQOL group with the support of fifteen international field centres [50].
Gynaecological conditions are common in women worldwide, carrying high treatment costs [3]. Worldwide, it is estimated that 10% of women of reproductive age have endometriosis [51], and pelvic organ prolapse is experienced by 40% of women and is predicted to become increasingly frequent [52].
The use of OMT in gynaecological conditions can support neurophysiological and cerebral activity in healing processes [3,53,54,55,56]. In visceral manipulation, the osteopath’s hands are the main tool for working with the patient, meaning interoception through the sense of touch can play a key role in this therapy [55]. Touch has been identified as an exteroceptive and interoceptive modality [55]. Interoception is supported by small-diameter low-conductance unmyelinated C-tactile (CT) fibres, which may be significant in the mechanism of action of touch-based manual therapy [55]. Manual therapies, which include visceral manipulation, still do not have a well-founded clinical value [55]. Performing visceral gynaecological techniques also involves working within the abdominal cavity, so it would also be reasonable to consider mechanisms occurring in the gastrointestinal (GI) tract, which has excellent neural control at two levels [57]. One is the enteric nervous system (ENS), comprising Auerbach’s and Meissner’s plexuses, described as a local nervous mechanism that controls bowel function independently, and the second level is the innervation coming from the central nervous system (CNS) [57]. Perhaps the positive effect of visceral manipulation should also be sought in the neural pathways transmitting intestinal information to the CSN [58]. Consideration should also be given to the occurrence of viscero-somatic reflexes, which appear when the diseased visceral organ transmits information via afferent nerves [59]. The spinal cord supervises somatic efferent and afferent stimulation and visceral afferent stimulation at the same segmental level via the autonomic nervous system. A high degree of somatic and visceral convergence is present in the area of lamina I of grey matter. At the interneurons of lamina I, somatic fibres and visceral C-fibres form synapses. The stimulation of these interneurons produces a sympathetic signal to internal organs with dysfunction [60]. Abnormal activity of the nervous system at given spinal levels creates a maladaptive reflex arc that also contributes to internal organ dysfunction [60]. Osteopaths use OMT to attenuate sympathetic nervous system activity and, at the same time, visceral dysfunction, through the somato-peritoneal reflex network. Regardless of the technique used, the aim of osteopathic manipulative treatment is to eliminate or reduce somatic dysfunction in order to decrease the somatic component in the spinal cord and improve the overall functioning of the nervous system [60].
Our study results indicate that visceral manipulation can be an effective tool to improve the quality of life of women with endometriosis or pelvic organ prolapse. It is worth emphasising that this is a non-pharmacological and non-invasive way to improve quality of life. In our study, we used the standardised World Health Organisation Quality of Life BREF questionnaire (WHOQOL-BREF).
De Marco et al. used visceral manipulation in their randomised control trial (RCT) in women with urinary incontinence. In addition to visceral manipulation, patients received pelvic floor muscle training, and thoracic spine mobilisation was introduced [61]. When performing visceral manipulation, tensile pressure lasting 5 s was applied. The authors showed no positive effect of the combination of therapies in women on the reduction in incontinence symptoms. The International Consultation on Incontinence Questionnaire-Urinary Incontinence Short Form (ICQ-UI-SF) was used in this study. In this study, the patients underwent visceral manipulation one time per week for 5 weeks, and we also used visceral manipulation one time per week for 5 weeks.
Yosri et al., in an RCT, used visceral manipulation in combination with a low-calorie diet in women with polycystic ovary syndrome accompanied by menstrual problems. This study found a statistically significant improvement in the reduction in menstrual problems in the group in which visceral manipulation was used [62]. In this study, tensile pressure lasting 6 s was applied and repeated until the patient did not feel any stretching of the soft tissues. The Polycystic Ovary Syndrome Quality of Life scale (PCOSQOL) questionnaire was used to determine symptoms associated with menstrual disorders.
In their RCT, Lagrange et al. used visceral manipulation in post-surgical breast cancer patients who were undergoing chemotherapy to alleviate side-effects such as vomiting, nausea and constipation. In this study, no significant differences were found for the reduction in vomiting, nausea and constipation. In contrast, patient-reported quality of life related to digestion improved significantly [63]. The Cancer (EORTC) QLQ-C30 Quality of Life questionnaire was used to assess quality of life in this study.
Visceral manipulation has also been used in patients with musculoskeletal dysfunction. Tamer et al. used visceral manipulation in patients with non-specific lower back pain. In their RCT, they used the 36-Item Short Form Survey (SF-36) Quality of Life questionnaire. The authors showed a positive effect of visceral manipulation on improving the quality of life of non-specific LBP sufferers, demonstrating the effect of therapy on reducing pain sensations among the subjects [64]. Moreover, Panagopoulos et al. conducted an RCT to evaluate the effects of standard physiotherapy and visceral manipulation in patients with sacral pain. Their results showed that the intervention group experienced less pain than the placebo group after 52 weeks [65].
Eguara et al. applied visceral manipulation to patients with gastroesophageal reflux disease (GERD). They used the GerdQ questionnaire and the Cervical Range of Motion (CROM) to assess the effectiveness of the therapy. The results of the study showed alleviation of GERD symptoms and cervical spine mobility after visceral manipulation [66]. In this study, patients received only two therapy sessions with a one-week interval between the first and second session.
Neto et al.’s RCT showed a positive effect of visceral manipulation in post-stroke patients in terms of reducing constipation. Due to the nature of their condition, participants in the study were also subjected to neurological physiotherapy for motor improvement. In this study, the mobilisation of the ascending colon, descending colon, sigmoid colon and sphincters (cardiac, pyloric, Oddi, duodenogastric and ileocaecal) was performed. Stretching pressure for 1 min was applied [67]. The authors also assessed the postural stability of the patients, observing improved parameters in the group that underwent visceral manipulation [67].
Postural stability is most commonly assessed in people with musculoskeletal conditions [68,69] or in neurological diseases [70,71]. Previous studies on the postural stability and quality of life of women have examined assessments related to lower back pain, mineral density, muscle strength, chemotherapy and the impact of physical activity in women with breast cancer [72,73,74,75]. Buscemi et al.’s study was carried out on healthy subjects but showed an effect of OMT, which improved postural stability values [76].
Our results for postural stability showed in the comparison of the female groups studied that they differed statistically significantly for the value of the area of the centre of gravity, which may indicate the effect of the visceral manipulation, which improved their stability. The surface area is the area in which the body’s centre of gravity oscillates. The smaller the surface area, the better the body’s balance. In an adult, the centre of gravity in the pelvis is located at the level of the first sacral vertebra—S1 [77]. In turn, the pelvis acts as a hinge between the spine and hips to maintain balance during bipedalism [77]. Pelvic organ prolapse in women affects the pelvic area, and the ongoing disease process of endometriosis also predominantly affects the pelvis. It may be the case that the ongoing disease process affects the location of the centre of gravity in women.
OMT techniques can have different effects on neurophysiological function and should be promoted in a personalized fashion by focusing on somatic dysfunction (SD) [4,78]. In practice, osteopaths use many different techniques on different parts of the body during the same session [78]. The black box approach should also be kept in mind [78]. The black box leaves the osteopath free to apply the main principles of osteopathy, treating ‘what he finds’ in the patient, while intermediate parameters are assessed to measure outcomes [78].
Visceral manipulation was used in a standardised way to reinforce the methodology and the possibility of generalising the results. In our protocol, we assumed that during each session, the same visceral manipulation would be performed for all patients lasting the same amount of time. The intervention protocol we adopted was also intended to make our study better understood by other professionals who do not refer to somatic dysfunction in their practice, which is a characteristic term for osteopaths and refers to distinctive strategies. Osteopathic treatment must focus on the lowering of somatic dysfunction through shared decision making by the therapeutic team formed by the doctor and the osteopath. In this case, the selection of the appropriate osteopathic treatment will also depend on the professional experience of the doctor and osteopath. In addition, everyday osteopathic praxis, in which osteopathic therapy is patient-centred, should be incorporated and involve outcome-based strategies. Osteopathic treatment aims to improve patients’ adaptability by focusing on somatic dysfunction through shared decision making by the therapeutic team formed by osteopaths and other health professionals. The tool of osteopaths to work with patients is their hands. Touch is a tool for detecting somatic dysfunctions like neurofascial active areas, which can act as an osteopath–patient interface to transmit the biological and physiological effects of touch [79,80]. Inhibition tests, which are manual functional tests used in the diagnosis of SD, are tests in which the osteopath applies manual mechanical stimuli to dysfunctional tissues and assesses the biological responses that occur simultaneously with the application of the stimulus [81]. Osteopathic structural–functional models, which include the biomechanical, respiratory–circulatory, metabolic, neurological and biopsychosocial models, have been developed to promote our understanding of patients’ complex health functioning. The models also contribute to the preparation of a comprehensive management plan to restore and maintain their health potential [82].
The use of standardized osteopathic visceral techniques, selected based on the expertise of the involved professionals (i.e., the physician and the osteopath), differs significantly from real-world daily osteopathic practice. In routine clinical settings, practitioners typically adopt a whole-body personalized osteopathic approach. This approach involves a shared decision-making process that incorporates the patient’s input, tailoring the intervention to the individual’s clinical presentation [83].
Strengths and Limitations
One definite limitation of this study is the small group of women surveyed; thus, the results obtained should be treated as preliminary observations. Certainly, one limitation of this study is also the lack of groups of women who could be treated with a placebo or women who received conservative treatment. On the other hand, the strengths of this study are the inclusion criterion for women less than one month after surgical treatment and the rigid protocol of conducting five therapy sessions with a weekly interval between sessions and with a fixed time for each session. Further research taking into account both the weaknesses and strengths of this study will provide hard evidence for a greater demonstration of the positive effects of visceral manipulation in women with endometriosis and pelvic organ prolapse.
5. Conclusions
The use of five treatments at weekly intervals improved the quality of life of women with endometriosis and pelvic organ prolapse. Visceral manipulation also improved the area of the centre of gravity in both study groups.
Acknowledgments
We would like to thank the women who participated in our research.
Author Contributions
Conceptualization, M.W.; methodology, M.W.; software, M.W. and I.S.; validation, M.W. and I.S.; formal analysis, M.W. and I.S.; investigation, M.W. and I.S.; resources, M.W. and I.S.; data curation, M.W. and I.S.; writing—original draft preparation, M.W. and I.S.; writing—review and editing, M.W., M.K., Z.H., I.S., W.K. and G.J.-B.; visualization, M.W.; supervision, M.W.; project administration, M.W. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsink, approved by the Ethics Committee Medical University in Poznan (permit No. KB/305/2023, 11 May 2023) and registered in the Clinical Trials Registry (Registry ID: NCT05978414).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
Funding Statement
This research received no external funding.
Footnotes
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
References
- 1.Parsons J., Marcer N. Osteopathy: Models for Diagnosis, Treatment and Practice. Churchill Livingstone; Edinburgh, UK: 2005. pp. 135–167. [Google Scholar]
- 2.Orrock P. Profile of members of the Australian Osteopathic Association: Part 1—The practitioners. Int. J. Osteopath. Med. 2009;12:14–24. doi: 10.1016/j.ijosm.2008.04.002. [DOI] [Google Scholar]
- 3.Ruffini N., D’Alessandro G., Pimpinella A., Galli M., Galeotti T., Cerritelli F., Tramontano M. The Role of Osteopathic Care in Gynaecology and Obstetrics: An Updated Systematic Review. Healthcare. 2022;10:1566. doi: 10.3390/healthcare10081566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Tramontano O., Tamburella F., Dal Farra F., Bergna A., Lunghi C., Innocenti M., Cavera F., Savini F., Manzo V., D’Alessandro G. International Overview of Somatic Dysfunction Assessment and Treatment in Osteopathic Research: A Scoping Review. Healthcare. 2022;10:28. doi: 10.3390/healthcare10010028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. [(accessed on 7 January 2025)]. Available online: https://www.aacom.org/docs/default-source/publications/glossary2017.pdf.
- 6.Novack J.C., Whitton E.L., Smith R.N., Sciarretta J.D., Nguyen J. Abdominal Wall Evisceration Coupled with Iliac Vascular Injury after Blunt Trauma. Cureus. 2023;15:e34917. doi: 10.7759/cureus.34917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Jeong H., Jung S., Heo T.G., Choi P.W., Kim J.I., Jung S.M., Jun H., Shin Y.C., Um E. Could the Injury Severity Score be a new indicator for surgical treatment in patients with traumatic splenic injury? J. Trauma Inj. 2022;35:189–194. doi: 10.20408/jti.2021.0065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Brandner E.D., Wu A., Chen H., He
주의점과 효과
효과: 소화장애, 만성 골반통, 변비, 불임 관련 증상, 수술 후 회복 등에 도움이 된다는 연구가 있습니다. 논문처럼 삶의 질 개선 사례가 많습니다.