
비특이적 요통에 대한 코어 안정화 운동과 러시안 전기 자극의 효과: 단일 맹검 무작위 대조 시험
초록 요약
비특이적 요통(NSLBP)은
전 세계 장애의 주요 원인으로,
코어 안정화 운동(CSE)이 일반적인 치료법이지만,
신경근 전기 자극 같은 보조 치료를 추가하면 효과가 증대될 수 있다.
이 무작위 대조 시험(RCT)은
CSE(코어안정화운동)에 러시안 전류(RC)를 추가한 경우가
CSE 단독보다 NSLBP 환자의 통증, 기능 능력, 근육 두께, 척추 안정성 개선에 더 효과적인지 평가했다.
20~25세 환자 50명을 대상으로 6주 동안 시행되었으며,
연구 그룹(그룹 1, n=25)은 CSE + RC를, 대조 그룹(그룹 2, n=25)은 CSE만 받았다.
주요 결과:
VAS(시각 아날로그 척도)로 측정한 통증 강도와 ODI(오스웨스트리 장애 지수)로 측정한 기능 장애.
부차 결과: 초음파로 측정한 횡격막근(TrA)과 요추 다열근(LM) 두께,
Spinal Mouse 장치로 측정한 척추 안정성.
결과 분석에서 그룹 1이 VAS 점수와 ODI 감소,
안정성 점수 및 근육 두께 증가에서 더 큰 개선을 보였다.
결론적으로,
CSE + RC가 통증과 장애 감소,
기능 능력,
TrA/LM 두께,
척추 안정성 증가에 더 효과적이다.
주요 방법
이 단일 맹검 RCT는 Deraya University의 외래 클리닉에서 진행되었다. 대상자: 만성 NSLBP(3개월 이상, VAS >4, ODI ≥19%) 환자 50명(20~25세, BMI 18.5~24.9). 제외 기준: 신경/근골격 질환, 임신, 수술 이력, 방사통, 악성 종양 등. 무작위 배정: 밀봉 봉투 방법으로 그룹 1(CSE + RC)과 그룹 2(CSE 단독)으로 나눔. 샘플 크기: 그룹당 25명(G*Power 계산, 효과 크기 0.88). 중재: 주 3회, 6주. RC: ITO ES-5200 장치(2500Hz 주파수, 50Hz 버스트, 50% 듀티 사이클, 31~58mA 강도) 사용. LM은 엎드린 자세(L4-L5 척추돌기), TrA은 누운 자세(전상장골극 위)에서 적용. 10/50/10 방법(10초 수축, 50초 휴식, 10회 반복, 총 20분). CSE: 압력 바이오피드백 장치로 TrA/LM 활성화 훈련, 정적 대각 운동에서 동적 운동으로 진행(통증 없음). 결과 측정: VAS(통증), ODI(장애), 초음파(근육 두께), Spinal Mouse(안정성). 기준선과 중재 후 평가. 분석: 혼합 모델 MANOVA, Bonferroni 사후 검정, 독립/대응 t-검정(p<0.05). 맹검: 참가자와 평가자 맹검, 치료사는 맹검 불가. 시험 등록: NCT06495099.
주요 결과
통계적으로 유의한 상호작용 효과(F=66.16, p=0.001), 치료 효과(F=4.34, p=0.001), 시간 효과(F=268.69, p=0.001). 그룹 내: 두 그룹 모두 VAS/ODI 감소와 안정성/근육 두께 증가(p<0.001). 그룹 1: VAS 63.22% 감소(4.4점), ODI 72.11% 감소(23.68%), 안정성 23.91% 증가; TrA 두께 37.50%/27.27%(우/좌), LM 22.77%/24.75% 증가. 그룹 2: VAS 48.86% 감소, ODI 43.69% 감소, 안정성 12.83% 증가; TrA 9.09%/9.37%, LM 6.90%/3.85% 증가. 최소 임상 중요 차이(MCID) 초과(VAS ≥2, ODI ≥10). 그룹 간: 그룹 1이 우수(VAS MD -1.04, p=0.008; ODI MD -9.76%, p<0.001; 안정성 MD 7.53%, p=0.02; 우측 TrA MD 0.08cm, p=0.004 등). 순응도 >90%, 그룹 1에서 가벼운 홍반 2건 발생.
논의 포인트
CSE + RC가 CSE 단독보다 통증/장애 감소와 안정성/근육 두께 개선에서 더 효과적이며, MCID 초과. 기전: RC가 A-베타 섬유 활성화(문제 제어 이론), 내인성 오피오이드/사이토카인 감소로 통증 억제; 깊은 근육 모집 강화, 신경근 억제 감소. 기존 연구(Batistella 등 LBP 연구, Lee 등 근육 두께 연구)와 일치. 장점: 빠른 강도 증가, 구조 변화; 단점: 피로, 피부 자극, 장비 필요. 제한점: 장기 추적 미실시, 젊은 표본(일반화 제한), 위약 대조/다른 전기 치료 비교 미실시, 단일 맹검 편향 가능, 효과 크기 변동(좌 LM ηp²=0.09).
결론
만성 NSLBP 젊은 성인에서 6주 동안 CSE + RC가 CSE 단독보다 통증/장애 감소와 TrA/LM 두께/척추 안정성 증가에 더 효과적
- nature
- scientific reports
- articles
- article
Effect of core stability exercises and Russian electrical stimulation on nonspecific low back pain: a single-blinded randomized controlled trial
- Article
- Open access
- Published: 17 December 2025
Effect of core stability exercises and Russian electrical stimulation on nonspecific low back pain: a single-blinded randomized controlled trial
Scientific Reports volume 15, Article number: 44053 (2025) Cite this article
Abstract
Nonspecific low back pain (NSLBP) is a predominant contributor to disability worldwide. Core stability exercises (CSEs) serve as a common intervention; however, their therapeutic effects may be augmented through the incorporation of adjunct modalities such as neuromuscular electrical stimulation. This randomized controlled trial aimed to evaluate whether the addition of Russian current (RC) stimulation to a CSE regimen enhances improvements in pain, functional capacity, muscle thickness, and spinal stability among patients diagnosed with NSLBP compared with a regimen comprising CSE alone. This single-blinded, randomized controlled trial was conducted at the outpatient clinic of Deraya University over a six-week intervention period. A total of fifty patients aged between 20 and 25 years with chronic NSLBP were recruited. The participants were randomly allocated into two groups via a closed-envelope. Group 1 (the study group, n = 25) received CSE and RC three times a week for six weeks, whereas Group 2 (the control group, n = 25) received CSE only. The primary outcomes assessed included pain intensity, measured via the visual analog scale (VAS), and functional disability, evaluated via the Oswestry Disability Index (ODI). The secondary outcomes included the muscle thicknesses of the transversus abdominis (TrA) and lumbar multifidus (LM), which were measured via ultrasonography, and lumbar spine stability, which was assessed via a Spinal Mouse device. The data were analyzed via mixed-model MANOVA for group and time effects, accompanied by post hoc Bonferroni correction. Between-group comparisons were performed via independent t tests, whereas within-group analyses were performed via paired t tests. There was a significant decrease in the VAS score and ODI and a significant increase in the stability score, TrA, and LM thickness, especially in group 1. The demographic characteristics of the groups were comparable at baseline (p > 0.05). Compared with Group 2 (CSE alone), Group 1 (CSE + RC) exhibited significantly greater improvements in the VAS score (MD: -1.04, 95% CI: -1.79–0.29, p = 0.008), ODI (MD: -9.76%, 95% CI: -12.13–7.39, p < 0.001), stability score (MD: 7.53%, 95% CI: 0.95–14.12, p = 0.02), and muscle thickness (e.g., right TrA: MD: 0.08 cm, 95% CI: 0.02–0.12, p = 0.004). There was a significant decrease in the VAS score and ODI and an increase in the stability score, TrA, and LM thickness, especially in group 1. Compared with core stability exercises alone, the Russian current accompanied by core stability exercises results in greater decreases in pain and disability and greater increases in functional ability, TrA and LM thickness, and lumbar spine stability.
비특이적 요통(NSLBP)은
전 세계적으로 장애의 주요 원인이다.
코어 안정성 운동(CSEs)은 흔히 시행되는 중재법이지만,
신경근 전기 자극과 같은 보조적 치료법을 병행함으로써
그 치료 효과를 증진시킬 수 있다.
본 무작위 대조 시험은
CSE 프로그램에 러시아 전류(RC) 자극을 추가했을 때,
CSE 단독 프로그램 대비 NSLBP 환자의 통증, 기능적 능력, 근육 두께 및 척추 안정성 개선 효과가
향상되는지 평가하는 것을 목표로 하였다.
이 단일 맹검 무작위 대조 시험은 데라야 대학 외래 진료실에서 6주간의 중재 기간 동안 수행되었다.
만성 NSLBP를 가진 20~25세 환자 총 50명이 모집되었다.
참가자들은 밀봉된 봉투를 통해 무작위로 두 그룹으로 배정되었다.
그룹 1(연구군, n=25)은 6주간 주 3회 CSE와 RC를 받았으며,
그룹 2(대조군, n=25)는 CSE만 받았다.
주요 평가 결과에는
시각적 아날로그 척도(VAS)로 측정된 통증 강도와 오스웨스트리 장애 지수(ODI)로 평가된 기능적 장애가 포함되었다.
부차적 결과에는
초음파로 측정된 횡복근(TrA) 및 요추 다열근(LM)의 근육 두께와 척추 마우스 장치를 통해 평가된
요추 척추 안정성이 포함되었다.
데이터는 집단 및 시간 효과를 위한 혼합 모델 MANOVA로 분석되었으며,
사후 보네로니 보정을 동반하였다.
집단 간 비교는 독립 표본 t-검정을 통해 수행된 반면,
집단 내 분석은 쌍을 이룬 표본 t-검정을 통해 수행되었다.
특히 그룹 1에서
VAS 점수와 ODI의 유의한 감소,
안정성 점수,
TrA 및 LM 두께의 유의한 증가가 관찰되었다.
그룹 간 인구통계학적 특성은
기저선에서 유사했다(p>0.05).
그룹 2(CSE 단독) 대비 그룹 1(CSE+RC)은
VAS 점수(평균차: -1.04, 95% 신뢰구간: -1.79–0.29, p=0.008),
ODI(평균차이: -9.76%, 95% 신뢰구간: -12.13–7.39, p<0.001),
안정성 점수(평균차이: 7.53%, 95% 신뢰구간: 0.95–14.12, p=0.02),
근육 두께(예: 우측 TrA: 평균차이: 0.08 cm, 95% 신뢰구간: 0.02–0.12, p=0.004).
특히 그룹 1에서
VAS 점수와 ODI는 유의미하게 감소한 반면,
안정성 점수, 복직근(TrA) 및 늑간근(LM) 두께는 증가했다.
코어 안정성 운동 단독 대비, 코어 안정성 운동과 병행한 러시아 전류 치료는
통증 및 장애 감소 효과가 더 크고,
기능적 능력, TrA 및 LM 두께, 요추 척추 안정성 증가 효과가 더 컸다.
Trial registration: The study was registered on clinicaltrials.gov (NCT06495099) on 02/07/2024.
Introduction
Low back pain (LBP) is a highly prevalent musculoskeletal disorder that affects approximately 80% of individuals at some point in their lives1. It is the second leading cause of work absences and a primary reason for seeking healthcare services2.
LBP is typically classified as nonspecific (90%) or specific (10%) on the basis of whether a discernible pathoanatomical cause can be established3.
The symptoms may be categorized according to their duration: acute (lasting less than six weeks), subacute (six to twelve weeks), or chronic (exceeding twelve weeks)4. It is estimated that chronic low back pain (CLBP) afflicts approximately 50% of the general population, and nearly 70% of adults experience at least one episode of LBP during their lifetime5.
Recent epidemiological studies indicate a concerning increase in the incidence of nonspecific low back pain (NSLBP) among young and middle-aged individuals6. This trend is particularly alarming for university students, as research elucidates a heightened vulnerability due to prolonged screen exposure and insufficient physical activity within their daily routines7. Furthermore, suboptimal sitting postures may escalate mechanical stress on the lumbar spine, amplifying static loads on the lumbar joint ligaments8. Prolonged sitting can predispose individuals to diminished lumbar lordosis and an increase in posterior pelvic tilt, subsequently leading to discomfort or pain9.
Approximately 85% of all LBP cases are classified as nonspecific, indicative of conditions not involving inflammation, anatomical alterations, or specific underlying pathologies10. Nonspecific LBP is frequently correlated with abnormalities in neuromuscular function, restricted flexibility of the lumbar muscles, and decreased spinal mobility11.
Nonspecific low back pain (NSLBP) is a prevalent condition influenced by several physical and psychological risk factors, including prolonged standing or ambulation, heavy lifting, poor postural habits, and sedentary behavior. Additional risk factors contributing to the onset of NSLBP include obesity and lifestyle choices characterized by nutritional imbalance12.
Research indicates that patients suffering from chronic NSLBP frequently exhibit weakness and delayed activation of deep stabilizing muscles, specifically the lumbar multifidus (LM) and transversus abdominis (TrA), which can culminate in postural instability and spinal dysfunction2.
The contemporary management of NSLBP is multifactorial, integrating pharmacological interventions (e.g., non-steroidal anti-inflammatory drugs [NSAIDs]), non-pharmacological strategies (e.g., patient education and reassurance), and physical therapy modalities. Among these, exercise therapy focused on core stabilization has emerged as a cornerstone intervention endorsed by international guidelines owing to its efficacy in enhancing both pain relief and functional capacity. Notably, the role of neuromuscular electrical stimulation (NMES), particularly in conjunction with exercise for muscle strengthening, has received increasing attention in recent studies13.
Core stabilization exercise (CSE), also referred to as specific stabilization or motor control exercise, is frequently employed as a therapeutic intervention aimed at addressing lower back pain14. The primary objective of CSE is to enhance neuromuscular control and strengthen the local trunk muscles, specifically the LM and TrA, to facilitate the restoration of their roles in maintaining segmental spinal stability. However, a prominent clinical challenge persists; many patients encounter difficulties in voluntarily isolating and activating these inhibited stabilizers, thereby limiting the overall effectiveness of exercise therapy alone15.
Electrotherapy is widely recognized for its analgesic properties and its ability to mitigate inflammation, enhance the range of motion, and contribute to muscle strengthening16. For example, the Russian current (RC), characterized by its asymmetrical sinusoidal or bipolar current train with a frequency of 2500 Hz, is modulated in bursts at 50 Hz. This type of electrical stimulation has the potential to induce involuntary, targeted muscle contractions. Notably, this modality aids in the activation of deep stabilizing muscles that are typically challenging to engage consciously17.
Despite the individual benefits associated with both CSE and Russian electrical stimulation, high-quality randomized controlled trials (RCTs) that rigorously examine the effects of Russian current on low back pain (LBP) are lacking. Furthermore, the synergistic effects of combining CSE with RES on outcomes related to NSLBP have not been thoroughly investigated. Few studies have employed objective assessment measures, such as ultrasound imaging and spinal mouse stability scores, to evaluate these outcomes effectively.
The present study seeks to bridge this research gap by systematically assessing the impact of augmenting core stability exercises with Russian current on various outcomes, including pain reduction, quality of life, the morphological thickness of the TrA and LM muscles, and the stability of the lumbar spine in individuals diagnosed with nonspecific low back pain.
요통(LBP)은 평생 어느 시점에서 약 80%의 개인에게 영향을 미치는 매우 흔한 근골격계 질환이다1. 이는 업무 결근의 두 번째 주요 원인이며 의료 서비스 이용의 주요 사유이다2.
요통은 일반적으로 식별 가능한 병리해부학적 원인이 확인되는지 여부에 따라 비특이적(90%) 또는 특이적(10%)으로 분류된다3.
증상은 지속 기간에 따라 급성(6주 미만), 아급성(6~12주), 만성(12주 초과)으로 분류된다4. 만성 요통(CLBP)은 일반 인구의 약 50%가 앓고 있으며, 성인의 거의 70%가 일생 동안 적어도 한 번 이상의 요통을 경험하는 것으로 추정된다5.
최근 역학 연구에 따르면 젊은 층과 중년층에서 비특이적 요통(NSLBP)의 발생률이 우려할 만한 수준으로 증가하고 있다6. 특히 대학생들의 경우 일상에서 장시간 화면 노출과 부족한 신체 활동으로 인해 취약성이 높아진다는 연구 결과가 이를 더욱 심각하게 만든다7. 또한 부적절한 앉은 자세는 요추에 가해지는 기계적 스트레스를 증가시켜 요추 관절 인대에 가해지는 정적 부하를 증폭시킬 수 있다8. 장시간 앉아 있는 것은 요추 전만 감소와 후방 골반 경사 증가를 유발하여 불편감이나 통증으로 이어질 수 있다9.
전체 요통 사례의 약 85%는 비특이성으로 분류되며,
이는 염증, 해부학적 변화 또는 특정 기저 병리를 수반하지 않는 상태를 의미한다10.
비특이적 요통은 신경근 기능 이상, 요추 근육 유연성 제한, 척추 가동성 감소와 빈번히 연관됩니다11.
비특이적 요통(NSLBP)은 장시간 서 있거나 걷기, 무거운 물건 들기, 나쁜 자세 습관, 좌식 생활 등 여러 신체적·심리적 위험 요인의 영향을 받는 흔한 질환입니다. NSLBP 발병에 기여하는 추가 위험 요인으로는 비만과 영양 불균형이 특징인 생활 방식 선택이 포함됩니다12.
연구에 따르면 만성 NSLBP를 앓는 환자들은 종종 깊은 안정화 근육, 특히 요부 다열근(LM)과 횡복근(TrA)의 약화와 활성화 지연을 보이며, 이는 자세 불안정성과 척추 기능 장애로 이어질 수 있습니다2.
현대적 NSLBP 관리법은 약물 치료(예: 비스테로이드성 항염증제[NSAIDs]), 비약물적 전략(예: 환자 교육 및 안심시키기), 물리 치료 모달리티를 통합한 다중 요인 접근법이다. 이 중 코어 안정화에 초점을 맞춘 운동 요법은 통증 완화와 기능적 능력 향상 모두에 효과적이라는 점에서 국제적 지침이 권장하는 핵심 중재법으로 부상했다. 특히 근육 강화 운동과 병행하는 신경근 전기 자극(NMES)의 역할은 최근 연구에서 주목받고 있다13.
특정 안정화 운동 또는 운동 제어 운동이라고도 불리는 코어 안정화 운동(CSE)은 요통 치료를 목표로 하는 치료적 개입으로 자주 활용됩니다14. CSE의 주요 목적은 신경근육적 제어력을 향상시키고, 특히 LM과 TrA와 같은 국소적인 몸통 근육을 강화하여 척추 분절 안정성 유지에 있어 이들 근육의 역할을 회복시키는 데 있습니다. 그러나 주요 임상적 어려움이 지속되고 있다. 많은 환자들이 억제된 안정근을 의도적으로 분리하여 활성화하는 데 어려움을 겪어 운동 치료 단독의 전반적 효과를 제한한다15.
전기 치료는 진통 효과와 염증 완화, 가동 범위 향상, 근력 강화에 기여하는 능력으로 널리 인정받고 있다16. 예를 들어, 비대칭 사인파 또는 양극성 전류 열로 특징지어지는 러시아 전류(RC)는 2500Hz의 주파수를 가지며 50Hz의 버스트로 변조됩니다. 이러한 유형의 전기 자극은 비자발적이며 표적화된 근육 수축을 유도할 잠재력을 지닙니다. 특히, 이 방식은 의식적으로 활성화하기 어려운 깊은 안정화 근육의 활성화에 도움을 줍니다17.
CSE와 러시아식 전기 자극 모두 개별적인 이점이 있음에도 불구하고, 요통(LBP)에 대한 러시아 전류의 효과를 엄격히 검토한 고품질 무작위 대조 시험(RCT)은 부족하다. 또한 CSE와 RES를 결합했을 때 비특이적 요통(NSLBP) 관련 결과에 미치는 시너지 효과는 충분히 연구되지 않았다. 초음파 영상 및 척추 마우스 안정성 점수(SMS)와 같은 객관적 평가 도구를 활용해 이러한 결과를 효과적으로 평가한 연구는 거의 없다.
본 연구는 비특이적 요통 진단을 받은 개인을 대상으로, 코어 안정성 운동에 러시아 전류를 병용했을 때 통증 감소, 삶의 질, 복횡근(TrA) 및 요방광근(LM)의 형태학적 두께, 요추 안정성 등 다양한 결과에 미치는 영향을 체계적으로 평가함으로써 이러한 연구 공백을 메우려는 목적을 가진다.
귀무가설
러시아식 전기 자극과 결합된 코어 안정성 운동을 받은 비특이적 요통(NSLBP) 환자와 코어 안정성 운동만 받은 환자 간 통증, 장애, 근육 두께, 요추 안정성에서 유의미한 차이가 없을 것이다.
대립가설 (H₁)
러시아식 전기 자극과 결합된 코어 안정성 운동을 시행한 비특이적 요통(NSLBP) 환자는 코어 안정성 운동만 시행한 환자보다 통증, 장애, 근육 두께 및 요추 안정성에서 유의미하게 더 큰 개선을 보일 것이다.
Null hypothesis
There will be no significant difference in pain, disability, muscle thickness, or lumbar stability between patients with nonspecific low back pain (NSLBP) who receive core stability exercises combined with Russian electrical stimulation and those who receive core stability exercises alone.
Alternate hypothesis (H₁)
Patients with nonspecific low back pain (NSLBP) who receive core stability exercises combined with Russian electrical stimulation show significantly greater improvements in pain, disability, muscle thickness, and lumbar stability than those who receive core stability exercises alone.
Materials and methods
Study design
This single-blinded randomized controlled trial, in which participants were unaware of their assigned treatment group, was conducted at the outpatient clinic of the Faculty of Physical Therapy at Deraya University. The assessor responsible for all outcome measurements, including the visual analog scale (VAS), Oswestry Disability Index (ODI), ultrasound assessments, and Spinal Mouse evaluations, maintained blinding concerning group allocation throughout the study. Randomization of participants was achieved by categorizing patients with odd identification numbers into the treatment group, whereas those with even identification numbers were assigned to the control group. The physical therapist responsible for administering the interventions, which included both CSE and RC, was unable to maintain blinding due to the inherent nature of the electrotherapy application. This process involves tangible aspects such as equipment setup, parameter adjustments, and observable muscle contractions. To mitigate potential bias in the study, a highly standardized treatment protocol was implemented. Furthermore, the statistician conducting the data analysis was blinded to the group assignments, and the independent reviewer was not involved in the application of the interventions, thereby enhancing the integrity of the findings. The present study was meticulously designed, executed, and reported in accordance with the CONSORT 2010 statement, thereby ensuring adherence to principles of transparency and completeness in clinical trial reporting. This prospective randomized controlled trial received prior approval from the ethical committees of the Faculty of Physical Therapy at Deraya University, documented under approval number DCSR-02024-06. Furthermore, it is registered with ClinicalTrials.gov under the identifier NCT06495099 as of 09/07/2024. The trial was first registered on 02/7/2024, and all procedures followed the appropriate guidelines and regulations.
The inclusion criteria were as follows NSLBP patients aged 20–25 years who had experienced symptoms for more than 3 months and whose BMI ranged from 18.5 to 24.9. With pain ratings above four on the visual analog scale (VAS). An age-related disability score of 19% or higher was given by the Oswestry Disability Questionnaire.
The exclusion criteria included neurological or musculoskeletal illnesses impacting the lumbar spine; pregnancy and lactation; a history of lumbar spine surgery; indications of lumbar radiculopathy or myelopathy; and indications of severe pathology, such as malignancy, inflammatory disorders, or infection. Participants who had engaged in any structured exercise or physical therapy program for low back pain within the past three months, those utilizing systemic corticosteroids, and those who routinely consumed analgesics or nonsteroidal anti-inflammatory drugs (NSAIDs) for low back pain more than twice a week or muscle relaxants in the preceding four weeks were also excluded. Finally, individuals exhibiting cognitive impairments that could hinder their ability to follow instructions, as well as those with a recent history of trauma (within the last six months) to the back or pelvis, were disqualified from participation.
Sample size
A sample size calculation was conducted via G. Power (version 3.1.9.7), and the findings indicated that each group needed a sample size of 25 people. The computations were performed with a significance level of α = 0.05 and a statistical power of 80%, and an effect size of 0.88 was calculated based on a previous pilot study and is considered large according to Cohen’s conventions17.
Participants
From a pool of 58 individuals with nonspecific low back pain (NSLBP), fifty patients were selected from the outpatient clinic of Deraya University in Minya. Patients were diagnosed with chronic nonspecific low back pain, classified under the International Classification of Diseases, Eleventh Revision (ICD-11), specifically designated as code MG30.0 for chronic primary low back pain. The initial diagnosis was conducted by a board-certified orthopedic specialist with more than ten years of clinical experience. Following this assessment, the validity of the diagnosis was confirmed by the lead researcher in physical therapy to determine eligibility for inclusion in the study. Patients meeting the specified inclusion criteria were referred by their treating physicians, and participation in the study was formalized through the signing of informed consent documents by those who agreed to participate.
The subjects were randomly assigned to two groups via the closed envelope method (see Fig. 1). Group 1 (study group, n = 25) was given Russian electrical stimulation accompanied by core stability exercises three times a week for six weeks. Group 2 (control group, n = 25) was given core stability exercises three times a week for six consecutive weeks, and reassessment of the patients was performed after the last session of the planned treatment period. Both groups were assessed by the VAS score, the ODI, ultrasonography, and the use of a spinal mouse device before and after treatment.
Assessment tools
The visual analog scale (VAS) was used to assess pain levels. The VAS is a reliable and valid tool for measuring low back pain (LBP) and consists of a 10 cm line where a score of 0 indicates no pain and a score of 10 represents the most severe pain imaginable. The visual analog scale (VAS) is a reliable and valid instrument for evaluating pain18.
Functional disability was evaluated via the Oswestry Disability Index (ODI), a well-established and valid tool for assessing functional impairment in patients with low back pain. The index values range from 0 to 100% and are categorized for analysis: scores between 0 and 19% signify minimal disability, 20–39% denote moderate disability, 40–59% reflect severe disability, 60–79% represent crippling disability, and scores from 80 to 100% indicate bedridden individuals19.
Fig. 1
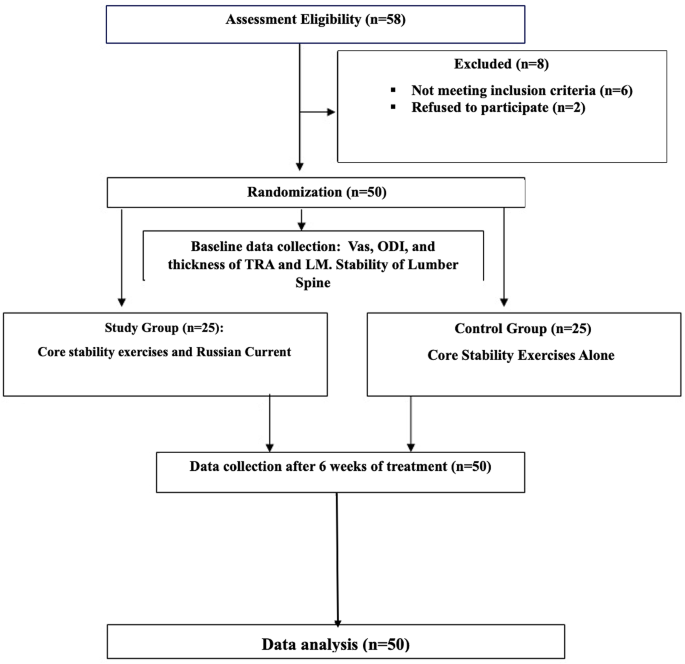
Flow chart of randomization.
Ultrasonography is a dependable and valid technique with strong intrarater reliability for assessing transverse abdominis and lumbar multifidus muscle thickness in patients with chronic low back pain (CLBP). All measurements of muscle thickness in this research were conducted by one operator, guaranteeing strong interrater reliability. Research has consistently demonstrated elevated ICCs for thickness assessments and contraction ratios in the transversus abdominis and lumbar multifidus muscles under both static (ICC = 0.71–0.99) and semidynamic conditions (ICC = 0.73–0.98)20. Ultrasonography was utilized to assess the LM and TrA muscles. Mindray DP10 ultrasonography was used. For the LM muscle, participants were positioned face down with a cushion under the abdomen to reduce lumbar lordosis. The thickness was measured between the fascial plane separating the muscle from the subcutaneous tissue and the posterior aspect of the L4-5 facet joint21 (Fig. 2a).
r the TrA muscle, a linear ultrasonic transducer was placed horizontally on the abdominal wall at the midpoint between the iliac crest and the lower edge of the rib cage, with its inner edge approximately 10 cm from the midline. The individual was positioned comfortably on their back, with a cushion positioned beneath the knees. The probe was placed with its inner edge approximately 10 cm away from the midline. The probe’s ultimate placement was adjusted to guarantee that the medial edge of the transversus abdominis (TrA) was approximately 2 cm away from the medial edge of the ultrasound image while the participant was in a relaxed position21 (Fig. 2b).
Fig. 2
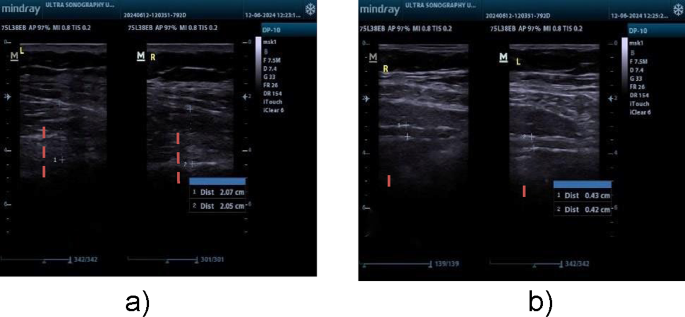
(a) LM thickness measurement, (b) TRA thickness measurement.
The stability and mobility of the lumbar spine were characterized via a surface-based Spinal Mouse system.
The Spinal Mouse system (IDIAG M360©, Fehraltdorf, Switzerland) is a reliable and credible tool for evaluating spinal curvatures, flexibility, and alignment, with high intraclass correlation coefficients (ICCs) ranging from 0.86 to 0.9822. The device was positioned paravertebrally along the spinous processes from C7 to S3 to capture the contour of the skin over the vertebral bodies. All outcome measures were assessed at baseline and after the six-week intervention23. Conversely, motion capture systems provide enhanced features for in-depth biomechanical assessment, focusing on kinematic and kinetic measurements, with ICC values surpassing 0.9024. Moreover, the isokinetic dynamometer is noted for its outstanding reliability in measuring muscle strength, with ICC values ranging from 0.93 to 0.9925.
All outcome measures were assessed at two separate time points: at baseline, before starting the first intervention session, and immediately after completing the 6-week intervention program.
Intervention procedures
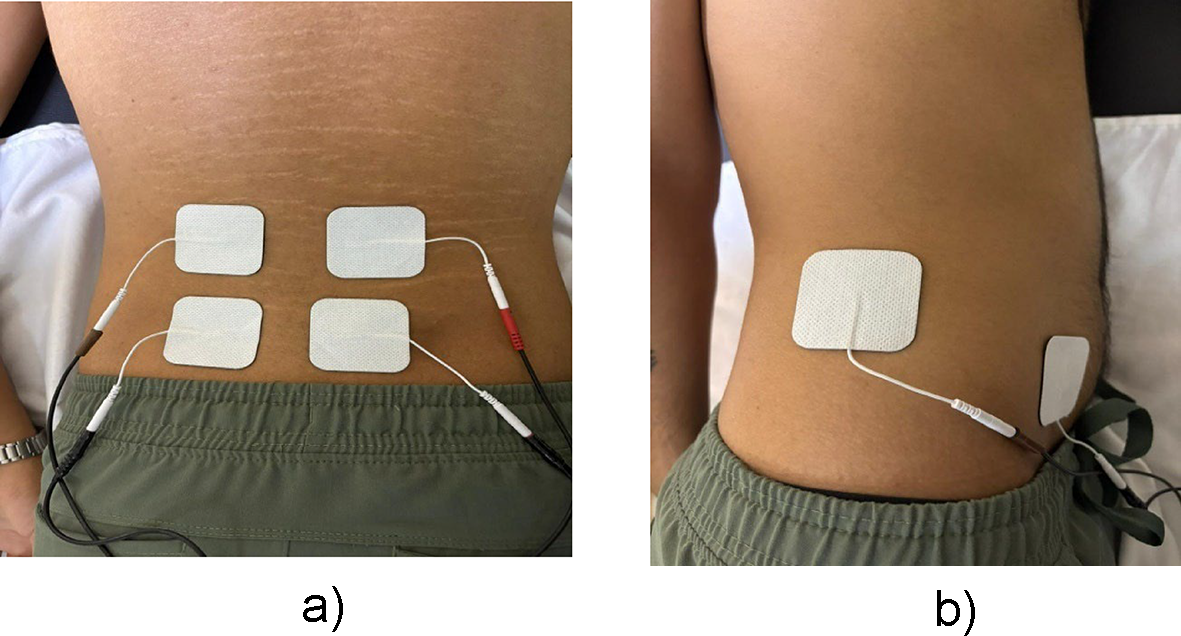
Russian electrical stimulation (RES) was applied three times a week for six weeks. The RES was delivered via an ITO ES-5200 electrotherapy device with a frequency of 2500 Hz, a 50 Hz burst modulation, and a 50% duty cycle. The stimulation strength varied between 31 and 58 mA. First, the amplitude was established at a minimal level adequate for a full and prolonged isometric contraction of the lumbar paraspinal muscles. The amplitude is then gradually elevated to the individual’s maximum tolerance to enhance muscle activation26. Participants were positioned in a prone posture to facilitate targeted activation of the lumbar multifidus (LM) muscle. Electrodes were strategically placed bilaterally on the L4 and L5 spinous processes, ensuring optimal conduction of electrical stimulation during the intervention (Fig. 3a). For the transversus abdominis (TrA) muscle, a reference electrode was placed on the mid-axillary line 1 cm above the iliac crest. The active electrode was positioned 2 cm above and 2 cm medial to the anterior superior iliac spine (Fig. 3b)21. The treatment protocol followed the 10/50/10 method: a 10-second muscle contraction followed by 50 s of rest, repeated 10 times, for a total duration of 20 min17.
Fig. 3
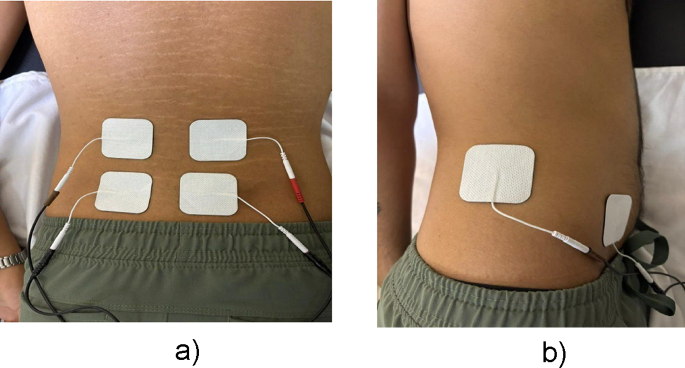
(a) Electrode placement for LM, (b) Electrode placement for TRA.
Core stabilization exercises were included in the intervention for both groups as the standard of care for nonspecific low back pain (NSLBP), thereby allowing the study to isolate the specific additive effect of Russian electrical stimulation. These exercises are a form of motor control training focused on activating and controlling deep spinal muscles, particularly the transversus abdominis (TrA) and lumbar multifidus (LM).
The capacity for TrA activation was assessed via a Stabilizer Pressure Biofeedback Unit (PBU) (Chattanooga Group, Australia). The participants were positioned in a prone posture on a firm surface, with the PBU placed over the TrA muscles, just superior to the anterior superior iliac spines. The PBU was inflated to a pressure of 70 mmHg. The participants were instructed to gently draw their lower abdomen away from the sensor without moving their back or hips, aiming for a pressure decrease of 4–10 mmHg. This contraction was held for 10 s and repeated 10 times2.
Lumbar multifidus activation was facilitated with participants in a crook-lying position. The PBU was maintained at 40 mmHg to monitor spinal control. The participants were instructed to take a relaxed breath, keep their chest still, and attempt to draw their sacrum toward their shoulders, which resulted in a pressure drop of 5–10 mmHg.
The exercise protocol progressed according to the participant’s ability to activate the muscles while maintaining spinal control. Exercises included:
- 1.
- 2.
- 3.
Exercises progressed in complexity from stable positions (e.g., crook-lying) to dynamic movements as participants gained control. It was emphasized that all exercise should be pain free, as discomfort could indicate incorrect forms or excessive intensity27.
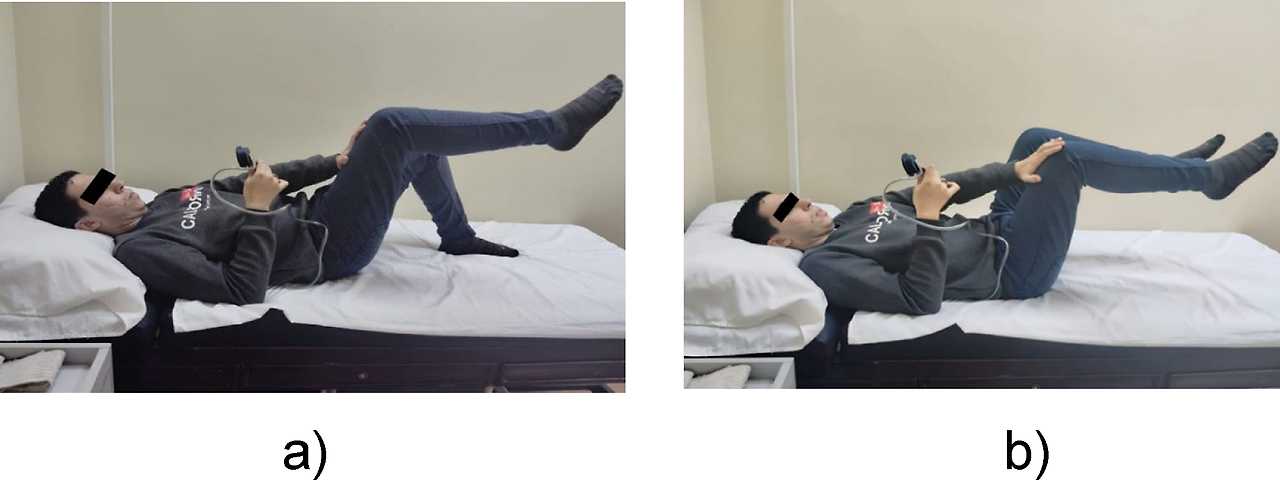
Fig. 4
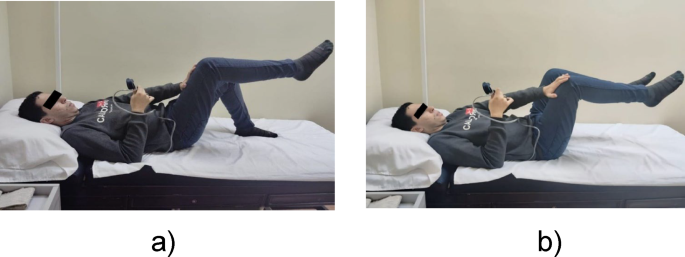
(a) Isometric opposite knee-to-hand push, (b) Isometric knee-to-hand push + 2nd heel lift.
Statistical analysis
All the data were analyzed via the Statistical Package for the Social Sciences (SPSS) version 25 for Windows (IBM, Chicago, IL, USA). The statistical significance threshold for all tests was set at p < 0.05.
An unpaired t test was used to perform a comparative analysis of baseline subject characteristics between the groups. A chi-square analysis was conducted to compare the sex distributions. The Shapiro–Wilk test was used to assess the statistical normality of the data, whereas Levene’s test was used to evaluate the homogeneity of variances between the groups. A mixed MANOVA was employed to examine the effects of the intervention on the primary outcome variables, including the visual analog scale (VAS) score, Oswestry Disability Index (ODI), stability score, and thickness of the transversus abdominis (TrA) and lumbar multifidus (LM) muscles. To account for multiple comparisons, post hoc analyses were performed via the Bonferroni correction. Management of Variables and Uniformity: Possible confounding factors such as age, sex, BMI, and initial outcome scores were managed via the randomized assignment procedure.
Results
Subject characteristics
Table 1 displays the means ± SDs of the participants’ demographic attributes, such as age, height, weight, and BMI. During the study, retention was total, with no participants missing or dropping out from any group. Given the lack of dropouts, an intention-to-treat analysis was conducted, including data from all 50 participants who were randomized in the study. There was no notable difference between the groups regarding age, weight, height, BMI, or sex distribution (p > 0.05). Treatment compliance and adherence: This research revealed a strong adherence rate, as participants in both experimental categories attended more than 90% of the planned sessions (18 sessions) throughout a six-week period. Importantly, no major negative effects were observed during the treatment phase. Nonetheless, two people in the current Russian group noted mild, temporary erythema localized beneath the electrodes. This condition resolved on its own and did not require any pause in the treatment process.
Table 1 shows the subject characteristics of groups 1 and 2.
Table 1 Comparison of subject characteristics between group 1 and group 2.
Effects of treatment on the VAS score, ODI, stability score, TrA, and multifidus thickness
A mixed MANOVA revealed that therapy and time had a significant interaction effect (F = 66.16, p = 0.001, ηp² = 0.92). A statistically significant main effect of treatment was observed (F = 4.34, p = 0.001; ηp²= 0.42). The main effect of time was statistically significant (F = 268.69, p = 0.001; ηp²= 0.0.98).
Within-group comparison
Significant improvements were observed in both groups when posttreatment scores were compared with baseline measurements across all outcome variables. A notable decrease in the visual analog scale (VAS) score and the Oswestry Disability Index (ODI) score was evident, alongside a considerable increase in the stability score for both groups (p > 0.001).
Group 1, which received the combined therapy, demonstrated a mean decrease of 4.4 in the VAS score and a 23.68% decrease in the ODI score. These improvements surpassed the minimum clinically important difference (MCID) standards of 2.0 points for the VAS score and 10 points for the ODI, indicating that the observed enhancements were both statistically significant and clinically relevant. The average percentage changes in the VAS, ODI, and stability scores for this group were 63.22%, 72.11%, and 23.91%, respectively. In Group 2, which received only core stability exercises, the corresponding percentage changes were 48.86% for the VAS score, 43.69% for the ODI, and 12.83% for the stability score, as illustrated in Table 2.
With respect to muscle thickness, considerable posttreatment increases were noted in the right and left transversus abdominis (TrA) and multifidus muscles in both groups compared with their respective pretreatment measurements (p > 0.001). For Group 1, the thicknesses of the right and left TrA and multifidus muscles increased by 37.50%, 27.27%, 22.77%, and 24.75%, respectively. In contrast, Group 2 had smaller percentage increases of 9.09%, 9.37%, 6.90%, and 3.85%, respectively (Table 2).
Between-group comparison
Before the intervention, no statistically significant difference was found between the groups (p > 0.05). However, posttreatment comparisons revealed a significant difference in favor of Group 1, with greater improvements in the VAS score, ODI, stability score, and thickness of the TrA and multifidus muscles (p < 0.05). The partial eta-squared (ηp²) values obtained from the MANOVA are detailed in the tables for further examination of effect sizes (Tables 2 and 3).
Table 2 Mean VAS score, ODI score, and stability score before and after treatment in groups 1 and 2:.
Table 3 Mean TrA and multifidus thicknesses before and after treatment in groups 1 and 2:.
Discussion
This study was designed to investigate the effects of a combined intervention consisting of core stability exercises and Russian electrical stimulation on pain, quality of life, lumbar stability, and the thickness of the transversus abdominis (TrA) and lumbar multifidus (LM) muscles in individuals with nonspecific low back pain.
The results revealed a significant reduction in both the visual analog scale (VAS) score and the Oswestry Disability Index (ODI) score in both treatment groups compared with their respective pretreatment values (p > 0.001). Additionally, notable increases in the stability score and thickness of the TrA and LM muscles were observed.
A posttreatment intersubject-group comparison revealed statistically significant differences, with the combined therapy group showing greater improvements in VAS and ODI scores, along with a more substantial increase in both the stability score and the thickness of the TrA and LM muscles (p < 0.001). The observed decreases in the VAS and ODI scores surpassed the minimum clinically important difference, confirming that the changes were not only statistically significant but also clinically meaningful for patients.
While studies specifically on the effect of Russian current on lower back pain (LBP) are limited, electrotherapy in general has demonstrated efficacy in pain management. This effect is often explained by the gate-control theory proposed by Melzack and Wall. This theory posits that the transmission of noxious stimuli through small-diameter, unmyelinated C fibers and myelinated A-delta fibers can be inhibited by the activation of large-diameter, nonnociceptive A-beta fibers. The activation of these A-beta fibers stimulates inhibitory interneurons in the spinal cord, which in turn “close the gate” to painful stimuli, preventing their transmission to the brain28. When used in appropriate settings, the Russian current selectively activates these A-beta fibers. Consequently, increased A-beta activity reduces the perception of pain. Other proposed mechanisms for the pain-relieving effects of transcutaneous electrical nerve stimulation (TENS) include the activation of descending inhibitory pathways within the central nervous system through the release of endogenous opioids29 or a reduction in proinflammatory cytokines such as IL-1 and IL-6 in the bloodstream30.
Electrotherapeutic methods, which use transdermal electric currents31, are commonly used by physiotherapists because of their beneficial effects on muscle performance and high patient acceptance32,33,34. Neuromuscular electrical stimulation (NMES) activates nerve fibers in a specific sequence. It begins with the activation of Aβ fibers, which produce the sensation of paresthesia that marks the sensory threshold. As the current amplitude increases, the NMES may also activate C fibers, which transmit pain signals. If the current exceeds the motor threshold, muscle contractions may occur35. The findings of this study align with existing research on the benefits of electrotherapy. For example, a randomized trial by Batistella et al. revealed that, compared with a control group, a group receiving current Russian therapy presented significant and sustained reductions in both the VAS score and the Oswestry low back disability index17. Similarly, Lee et al. (2017) reported significant improvements in muscle resistance, thickness, and pain levels following current Russian therapy for quadriceps pain after ACL reconstruction36.
To further support the efficacy of the Russian current, Çankaya et al. demonstrated its added benefits in managing symptoms and improving functional mobility and quality of life for individuals with patellofemoral pain37. Rajan et al. noted a slight advantage of current Russian therapy over other treatments, such as interferential therapy and conventional exercise, for short-term pain reduction and muscle strength improvement in patients with postoperative lower limb fractures38. Among the various NMES modalities designed for muscle strengthening, medium-frequency currents such as Aussie (AC) and Russian (RC) currents are particularly notable for their effectiveness.
Low-frequency currents, such as functional electrical stimulation (FES), are known to increase motor unit recruitment, which contributes to increased muscle strength and pain relief39,40. Specifically, the Russian current can trigger the depolarization of sensory and motor nerve fibers, stimulate fast Type II motor units and thereby promote muscle contractions that lead to an increase in muscle strength41. This finding is supported by studies such as Heggannavar et al., who demonstrated that Russian electrical stimulation effectively improved quadriceps strength and functional capacity in patients with primary osteoarthritis (OA) knee pain42. Similarly, Janarthanan et al. reported that the integration of Russian current and resistance exercises resulted in increased pain relief, strength, and performance in sprinters with calf muscle strain43. Further research by Letícia Cittadin et al. revealed a significant increase in muscle thickness in the nondominant hand of healthy females39, and a review by Pereira et al. suggested that the Russian current was the most effective method for promoting strength and thickness gains33.
However, some studies present conflicting findings. For example, Prabha et al. reported no additional benefits from the Russian current when supervised exercises were already being performed for primary knee osteoarthritis28.
For individuals with chronic nonspecific low back pain (NSLBP), a common issue is the delayed activation of deep stabilizing muscles, which leads to postural instability and exacerbated pain and dysfunction44. This study revealed a 23.91% increase in stability scores in the experimental group compared with a 12.83% increase in the control group, suggesting that Russian electrical stimulation (RES) promotes the recruitment of these weakened stabilizers41. Nevertheless, a known drawback of core stability exercises is the challenge in engaging these deep stabilizing muscles due to neuromuscular inhibition45. Furthermore, a study by Naka et al. on patients with chronic neck and lower back pain revealed that while suprathreshold electrotherapy administered six times per week improved lumbar flexibility, it did not significantly alter pain or disability perceptions46.
The integration of neuromuscular electrical stimulation (NMES), particularly with methodologies such as Russian current, alongside physical exercise, offers several unique benefits. This combined approach can help reduce neuromuscular inhibition, which in turn facilitates earlier and more effective activation of weakened stabilizing muscles, such as the transversus abdominis (TrA) and lumbar multifidus (LM). These muscles are often difficult for patients to activate voluntarily, leading to functional impairments. Consequently, this combined method has the potential to accelerate gains in muscle strength and promote structural changes. However, there are important considerations and potential drawbacks associated with this integrated approach. These include the risk of muscle fatigue, the possibility of skin irritation beneath the electrodes, and the reliance on specialized equipment and clinical expertise for proper implementation. These factors may limit the accessibility and practicality of this treatment for certain patient populations and healthcare settings41.
The findings of this research have significant clinical and academic implications. For clinicians, the evidence supporting the efficacy of combined therapy (CSE + RC) provides a practical framework for achieving faster and more pronounced results in pain relief, functional enhancement, and spinal stabilization. For patients, this protocol offers a more efficient path to recovery, potentially mitigating the long-term effects associated with chronic pain. Furthermore, for the research community, this study contributes to the current understanding of the NMES and establishes a validated framework for future investigations. This could facilitate additional research into the long-term effects and comparative effectiveness of this method against other electrotherapy modalities.
Conclusion
This study revealed that a six-week intervention combining Russian electrical stimulation with core stability exercises is significantly more effective than core stability exercises alone in reducing pain and disability in young adults with chronic nonspecific low back pain. The integrated program also led to a significant increase in the thickness of both the transversus abdominis and lumbar multifidus muscles, along with improvements in lumbar stability. These results support the incorporation of this combined treatment method into clinical practice for this patient population, highlighting its potential to enhance patient outcomes in the management of chronic low back pain.
Limitations and recommendations
This study has several limitations that warrant further discussion for future research. First, the study design did not include long-term follow-up assessments, which limits the understanding of whether the effects of the Russian current (RC) on neuromuscular changes are sustained over time. Future research should incorporate follow-up evaluations at 3 to 6 months to address this limitation. Second, the study was conducted on a sample of young adults, which limits the generalizability of the findings to other populations, such as older adults or those with significant spinal pathologies. It is recommended that future studies evaluate the impact of these rehabilitation interventions across a broader range of demographics, including older adults, athletes, and individuals with different body mass index (BMI) classifications. Third, this study focused on the additive effect of RC on core stability exercises. Future research should compare the effectiveness of RC with that of other electrotherapy methods, such as transcutaneous electrical nerve stimulation (TENS), to determine its relative efficacy. Fourth, while the results generally revealed medium to large effect sizes, certain comparisons, particularly for left multifidus thickness, revealed smaller effect sizes (ηp² = 0.09) and wider confidence intervals. This finding indicates that while the intervention was effective overall, the magnitude of the additional benefit from the Russian current varied significantly among individuals for this specific outcome. Fifth, in addition to the methodological limitations, the use of a single blinded evaluator and therapist, while essential for feasibility, introduces a potential for bias that could influence the results. Additionally, the strict inclusion criteria, although helpful in creating a uniform sample, also limit the direct applicability of the findings to a broader patient population. Sixth, a sham electrotherapy control group was not included. This prevents the definitive exclusion of a placebo effect influencing the results observed in the current Russian group.
Furthermore, a single-blinded design, while necessary for the feasibility of the intervention, presents a potential drawback. Although the participants and the outcome evaluators were blinded, the treating therapist could not be due to the nature of applying the Russian current. Despite implementing standardized procedures for interactions and obscuring the data analyst’s identity, the risk of performance bias cannot be eliminated. Future research should prioritize the development of a robust sham electrotherapy protocol to enable a double-blind design, which would strengthen the validity of the findings by minimizing potential biases.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
CNSLBP:
Chronic nonspecific low back pain
CSE:
Core stabilization exercise
RES:
Russian electrical stimulation
VAS:
Visual analog scale
ODI:
Oswestry Disability Index
TrA:
Transversus abdominis muscle
LM:
Lumbar multifidus muscle
CI:
Confidence interval
References