촉진의 중요성을 어떻게 다 말로 표현할 수 있을까?
Joseph E. Muscolino는 촉진의 대가
panic bird.....
![]() palpation of the anterior neck.pdf
palpation of the anterior neck.pdf

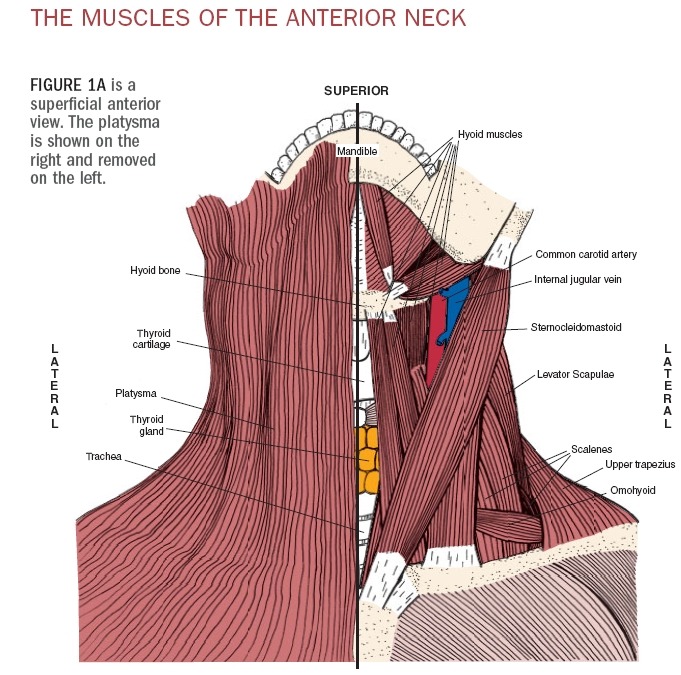
The anterior neck is problematic for many massage therapists. You may avoid working this region for two reasons. First, many endangerment sites are located in the anterior neck, including the trachea, thyroid gland, brachial plexus of nerves, and carotid artery. Second, working in this region can be uncomfortable if you are not skilled and familiar with it. The contours of the transverse processes of the vertebrae are rather sharp and having soft tissue pressed against them can be painful.
Even with these concerns, however, working the anterior neck can be very beneficial for the health of your client, especially one who has suffered a whiplash injury. Therefore, learning how to work the musculature of the anterior neck can be a valuable addition to a massage therapist’s practice. And the first step to learning how to safely and effectively work the anterior neck is learning how to identify, locate and palpate the muscles of this region.
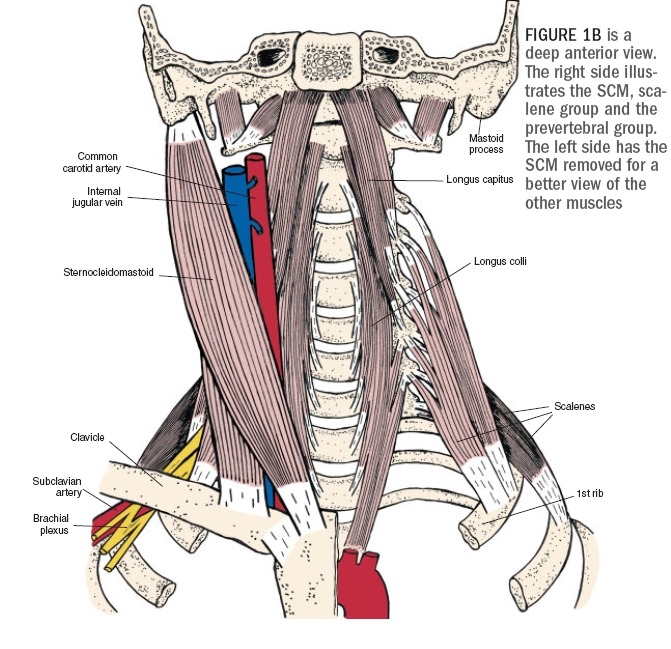
The anterior neck is home to a number
of important muscles, including the
sternocleidomastoid (SCM), scalene
group and the prevertebral group of
muscles (Figures 1A and 1B).* Functionally,
the muscles of the anterior
neck are flexors of the neck at the spinal
joints. Consequently, during a typical
whiplash accident when a person’s head
and neck are forcibly thrown back into
extension, the muscles of the anterior
neck are excessively stretched, triggering
the muscle spindle stretch reflex.
This results in tightness and spasming
of the muscles of the anterior neck.
Beyond local pain from the tightness of
these muscles, tightness of the SCM is
associated with proprioceptive disturbances
of the neck, often resulting in
dizziness. Tightness of the scalenes can
be associated with compression upon
nerves that provide innervation to the
upper extremity. Finally, tightness of
the prevertebral muscles can cause
referral pain that is interpreted as a sore
throat. Given the prevalence of
whiplash injuries, and the variety and
extent of signs and symptoms that can
result, there can be tremendous value
in working the anterior neck musculature
of our clients!
The Scalene and Prevertebral Muscles
While most of you are knowledgeable
and comfortable working the SCM, the
scalenes and prevertebral muscles are
less often addressed. We will begin by
locating and palpating the SCM. The
SCM will then be used as a landmark for
the location and palpation of the scalene
and prevertebral muscle groups.
The SCM has two heads—a sternal and a clavicular head. Inferiorly, the
sternal head attaches onto the
manubrium of the sternum, and the
clavicular head attaches onto the medial
clavicle. Both heads conjoin and attach
superiorly onto the mastoid process of
the temporal bone and superior nuchal
line of the occipital bone. The SCM can
be easily palpated with the client seated
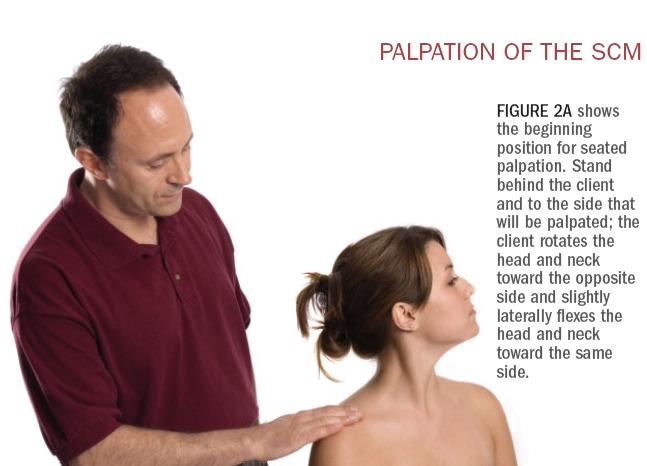
or supine. With the client seated, stand
to the side that will be palpated. Ask the
client to first rotate the head and neck at
the spinal joints to the opposite side
(contralateral rotation) and slightly laterally
flex the head and neck to the
same side (ipsilateral lateral flexion)
(Figure 2A). Now resist the client from
further lateral flexion (Figure 2B) and
the two heads of the SCM will be visible
and palpable. It is important to make
sure that the client maintains the contralateral
rotation; this is especially so
for the sternal head because this head is
more active in creating the rotation
component of the SCM’s actions. If the
clavicular head is not readily palpable,
ask the client to increase the force of
resistance of ipsilateral lateral flexion
because the clavicular head is more
active in creating the lateral flexion
component of the SCM’s actions.
After palpating the entire length of
both heads of the SCM* with the muscle
contracted, palpate the SCM again while
it is relaxed so that its resting baseline
tone can be assessed. When palpating
the SCM, be careful not to place excessive
pressure upon the carotid artery
because this will stimulate a neurologic
reflex that can lower blood pressure;
you can tell if you are pressing upon the
carotid artery by feeling for a pulse
under your fingertips.
Supine palpation of the SCM is also
straightforward. The client is supine
while you are seated at the head of the
table. First ask the client to contralater-ally rotate the head and neck fully to one
side; then ask the client to lift the head
and neck up off the table. The SCM will
be visible and palpable (Figure 2C).
Now that the SCM has been located,
its lateral border can be used as a landmark
for palpation of the scalene group.
The scalene group of muscles is composed
of three muscles—the anterior,
middle and posterior scalenes. (Their
names reflect their positions relative to
each other.) As a group, the scalenes
attach inferiorly to the first and second
ribs; superiorly they attach to the transverse
processes of the second through
seventh cervical vertebrae.
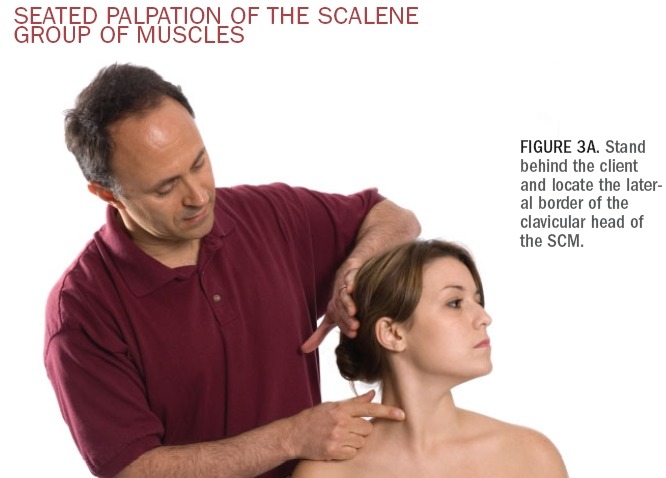
To palpate the scalenes with the
client seated, stand behind the client
and locate the lateral border of the SCM
(be sure that you have the lateral border
of the clavicular head) (Figure 3A).
From there, move your palpating fingers
slightly laterally off the SCM—you will
be over the scalenes. Now ask the client
to take in a short quick breath through
the nose and feel for the contraction of
the scalenes (Figure 3B). Taking in a
breath requires elevation of the ribs,
which is an action of the scalene group.
Once located, palpate the scalenes
while they are contracted, and then
while they are relaxed so that you can
assess their baseline tone. Be sure to
explore the entire breadth of the
scalenes within the anterior aspect of
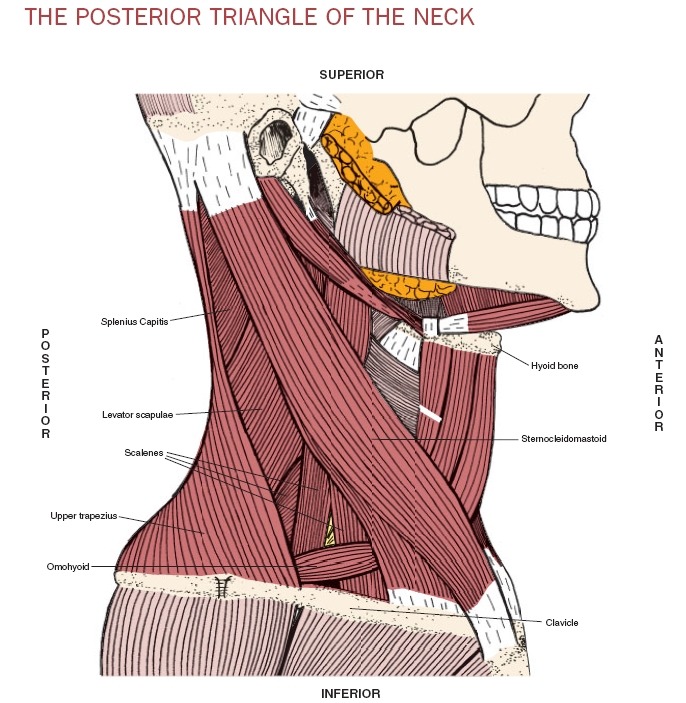
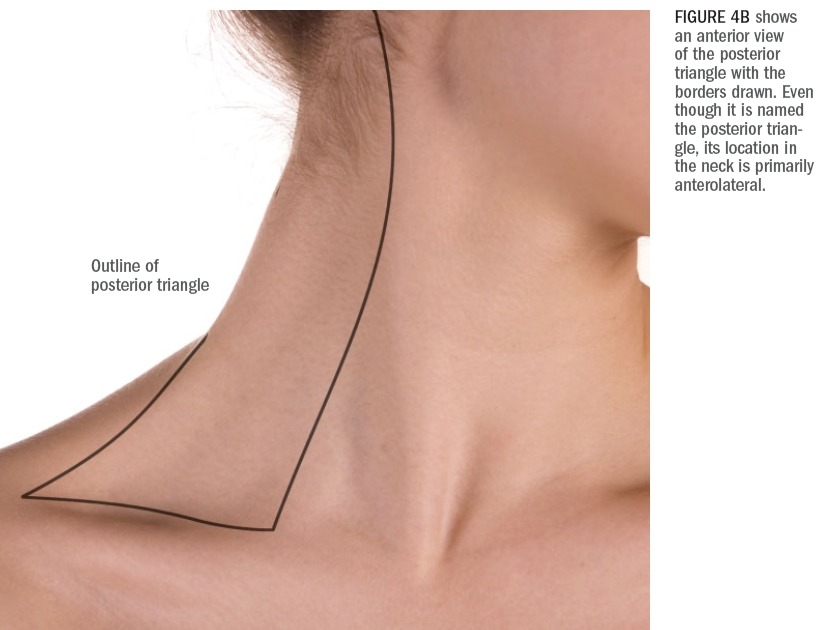
the posterior triangle of the neck (Figures
4A, 4B). The posterior triangle of the
neck is the region of the neck bounded
anteriorly by the SCM, posteriorly by
the upper trapezius and inferiorly by
the clavicle. Superficial within the posterior
triangle are the scalenes, levator
scapulae, splenius capitis and the inferior
belly of the omohyoid. (These muscles
are all deep to the platysma, which
is very thin and does not impede palpa-tion of the muscles that are deep to it.)
When palpating the scalenes, be careful
not to exert excessive pressure upon
the brachial plexus of nerves and/or the
subclavian artery. These structures
travel between the anterior and middle
scalenes.* If you feel a pulse under your
fingertips or the client reports tingling
down the upper extremity, move your
palpating fingers.
The prevertebral group of muscles
consists of the longus colli, longus capitis,
rectus capitis anterior and rectus
capitis lateralis. Of these, the longus
colli and longus capitis can be easily palpated;
these two muscles lie along the
anterolateral vertebral column from the
vertebral level of T3 to the skull. To
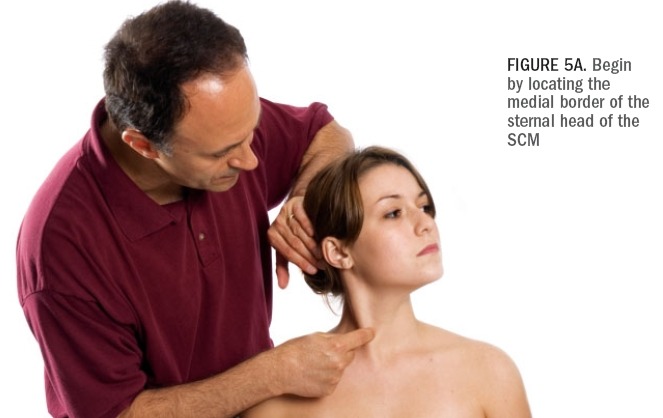
locate the longus muscles, we will again
use the SCM as our landmark. This time, locate the medial border of the
sternal head of the SCM. Next, palpate
just medial to that. Because the longus
muscles are located deep against the
spine, to access them you must gently,
but firmly, sink into the tissue in the
posterior direction aiming toward the
spinal column. It is important that this
be done slowly or it will be very uncomfortable
for the client. To bring out a
contraction of these muscles so that
they are more palpable, resist the client
from flexing the head and neck against
your hand. When palpating the longus
muscles, be careful not to exert too
much pressure against the trachea.
Otherwise, it will be irritated, and the
client may involuntarily cough. (See
right, Figures 5A-5C for this series.)
While many therapists are hesitant to
approach the muscles of the anterior
neck, it usually only takes a little practice
to locate and palpate them, and
only a little more practice to become
smooth and comfortable at it. Of
course, the more proficient you
become, the more comfortable these
palpations are for you and the client.
Once you are proficient at palpating
these muscles, working them in a therapeutic
manner easily follows!