https://academic.oup.com/rheumap/article/7/3/rkad081/7444834

1. 배경 및 목적 (Introduction)
논문은 가장 흔한 mechanical foot pain을 중심으로 다룹니다. 각 조건의 pathophysiology는 tissue stress theory (tensile/compressive overload) 기반.
|
Current and future advances in practice: mechanical foot pain
Open Access
Jill Halstead ,
Shannon E Munteanu
Rheumatology Advances in Practice, Volume 7, Issue 3, 2023, rkad081, https://doi.org/10.1093/rap/rkad081
Published:
31 October 2023
Article history
- Split View
- Share Icon Share
Abstract
Mechanical foot pain affects ∽20% of the UK population >50 years of age, with ∼10% reporting disabling pain that impacts daily activities. For most people, foot pain improves over time, but for some this can become chronic and disabling, affecting physical activity, participation, mental health and work capacity. Mechanical foot pain can present as localized pain, but more often the pain presents in multiple structures. Traditional treatments for mechanical foot pain are largely based on self-management that includes pain control, reassurance of healing trajectory, and activity or footwear modifications. Randomized controlled trials support the short-term use of exercise and foot orthoses for some foot conditions; however, accessibility can be limited by regional variations in procurement compounded by a lack of long-term trials. The roles of weight loss and strengthening of the foot and leg muscles offer new avenues to explore.
기계적 발 통증은
영국 50세 이상 인구의 약 20%에 영향을 미치며,
이 중 약 10%는 일상 활동에 지장을 주는 장애성 통증을 보고합니다.
대부분의 사람에게 발 통증은
시간이 지나면서 호전되지만,
일부에서는 만성적이고 장애를 유발하는 통증으로 진행되어
신체 활동, 사회 참여, 정신 건강 및 업무 능력에 영향을 미칩니다.
기계적 발 통증은
국소적인 통증으로 나타날 수 있지만,
더 흔하게는 여러 구조물에서 동시에 통증이 나타납니다.
기계적 발 통증에 대한 전통적인 치료는
주로 자가 관리에 기반하며,
여기에는 통증 조절, 치유 과정에 대한 안심 제공, 활동 또는 신발 수정이 포함됩니다.
무작위 대조 시험에서는
일부 발 질환에 대해 운동과 발 보조기(orthoses)의 단기 사용이 지지되지만,
지역별 조달 차이와 장기 추적 연구 부족으로 인해 접근성이 제한될 수 있습니다.
체중 감량과 발 및 다리 근육 강화의 역할은
새롭게 탐구할 가치가 있는 방향으로 제시됩니다.
What does this mean for patients?
One in five middle-to older-aged adults report foot pain that occurs during weight-bearing movements, such as walking and standing. Foot pain can present with weakness, symptoms of stiffness and changes in movement, all of which can limit daily activities and occupational duties. Owing to the complexity of the foot anatomy and loads placed on the foot, there are many musculoskeletal foot disorders to consider. In this review, we have presented the common causes of foot pain and separated these into the forefoot, midfoot and hindfoot regions for quick reference. Regarding treatments, changing the demands and loads placed upon the foot is a key strategy. This can be achieved by using appropriate footwear, limiting or changing activities that cause excessive loading, weight loss and wearing insoles inside shoes called orthoses. Maintaining muscle strength is also important, because weakness of the foot and lower leg muscles is found in many cases of foot pain. At present, we do not know how effective other treatments for foot pain are, such as pain medications and injections, hence more research is needed.
Key messages
Mechanical foot pain is common and frequently associated with joint pain and soft tissue pain at the tendon and fascia.
The foot is complex, and the shape of the forefoot and midfoot can change in later life. The wrong size and shape of footwear, especially the toe-box, is a common cause of pain.
Modifying the foot load by pacing, wearing foot orthoses and changing footwear all have the potential to help foot pain and disability.
환자에게 이 텍스트의 의미를 한국어로 설명하고, 전체 내용을 자연스럽게 번역한 버전입니다.
환자에게 이것이 무엇을 의미하나요? (환자 관점에서의 요약)
이 글은 중년에서 노년층 성인(대략 50세 이상) 중 5명 중 1명 정도가 걷거나 서는 등 체중이 발에 실리는 동작에서 발 통증(기계적 발 통증, mechanical foot pain)을 겪고 있다는 연구 리뷰 내용입니다. 이 통증은 단순히 아픈 것에 그치지 않고, 근육 약화, 뻣뻣함, 움직임 변화를 동반해 일상생활(걷기, 서 있기, 계단 오르기)이나 직업 활동을 크게 제한할 수 있습니다.
발은 구조가 매우 복잡하고 매일 엄청난 하중을 받기 때문에 여러 근골격계 질환(관절, 힘줄, 근막 등)이 생길 수 있어요. 이 리뷰에서는 흔한 발 통증 원인을 앞발(forefoot), 중족(midfoot), 뒷발(hindfoot) 영역별로 정리해 의료진이 빠르게 참고할 수 있게 했습니다.
치료의 핵심 메시지는 발에 가해지는 부하(하중)를 줄이고 조절하는 것입니다. 효과가 입증된 주요 방법들:
- 적합한 신발 착용 (특히 발가락 부분 toe-box가 넓고 맞는 신발 – 잘못된 신발 크기/모양이 통증의 흔한 원인)
- 과도한 하중을 주는 활동 제한하거나 변경 (pacing: 활동 조절)
- 체중 감량
- 신발 안에 넣는 깔창(orthoses, 발 보조기/인솔) 착용
- 발과 종아리 근육 강화 운동 (많은 발 통증 환자에게 근육 약화가 동반됨)
현재 진통제나 주사 같은 다른 치료법의 효과는 아직 잘 알려지지 않아 추가 연구가 필요하다고 합니다.
주요 요약 (Key messages):
- 기계적 발 통증은 매우 흔하며, 관절 통증과 힘줄·근막의 연부조직 통증이 자주 함께 나타남.
- 나이가 들수록 발 앞부분과 중간 부분 모양이 변형될 수 있음.
- 특히 발가락 부분이 좁거나 맞지 않는 신발이 통증의 흔한 원인.
- 활동 조절, 발 보조기(orthoses), 신발 교체 등으로 발 부하를 수정하면 통증과 장애를 줄일 가능성이 큼.
결론적으로, 많은 중장년층이 발 통증으로 고생하지만 의료기관을 찾는 사람은 12% 정도에 불과하고, 실제 영향은 크다는 점을 강조합니다. 특히 비만, 여성, 낮은 사회경제적 계층, 무릎·엉덩이 동반 통증 등이 더 심각한 통증이나 장애 위험을 높입니다.
전체 텍스트 한국어 번역 (자연스럽게 정리)
환자에게 미치는 의미?
중년에서 노년층 성인 5명 중 1명이 걷기나 서기 같은 체중 부하 동작 시 발 통증을 호소합니다. 발 통증은 근육 약화, 뻣뻣함, 움직임 변화와 함께 나타나 일상 활동과 직업 활동을 제한할 수 있습니다. 발의 복잡한 해부 구조와 받는 하중 때문에 다양한 근골격계 발 질환을 고려해야 합니다. 이 리뷰에서는 흔한 발 통증 원인을 앞발, 중족, 뒷발 영역으로 나누어 빠른 참고를 위해 제시했습니다.
치료 측면에서 발에 가해지는 요구와 하중을 바꾸는 것이 핵심 전략입니다. 이를 위해 적절한 신발 사용, 과도한 하중 활동 제한 또는 변경, 체중 감량, 신발 안 깔창(orthoses) 착용 등이 있습니다. 또한 발과 하지 근육 약화가 많은 발 통증 사례에서 나타나므로 근력 유지(강화)가 중요합니다. 현재 진통제나 주사 등의 다른 치료 효과는 잘 알려지지 않아 더 많은 연구가 필요합니다.
주요 메시지 기계적 발 통증은 흔하며, 관절 통증과 힘줄·근막의 연부조직 통증이 자주 동반됩니다. 발은 복잡하며, 나이 들수록 앞발과 중족 모양이 변할 수 있습니다. 특히 발가락 부분(toe-box)의 크기와 모양이 잘못된 신발이 통증의 흔한 원인입니다. 활동 조절(pacing), 발 보조기(orthoses) 착용, 신발 변경 등으로 발 하중을 수정하면 발 통증과 장애 개선 가능성이 있습니다.
Introduction
Mechanical foot pain is a term used to describe musculoskeletal foot pain associated with patterns of weight-bearing movement. The prevalence of mechanical foot pain varies from 13 to 39% depending on the case definition and age range of the cohort [1]. The prevalence of disabling foot pain (pain that impacts on daily activities, such as standing, walking and climbing stairs) ranges from 8 to 10% [2, 3]. Increasing age is the greatest determinant for developing mechanical foot pain, with peak incidence between the ages of 55 and 64 years [1]. Obesity is another determinant influencing both the onset and the severity of foot pain [4] and increasing the risk of multiple lower limb pains [5]. Consistently, more women than men report disabling foot pain [6, 7]. The burden of mechanical foot pain is greater in lower socioeconomic groups [6].
Despite the high prevalence of mechanical foot pain, only 12% of people with foot pain consult primary care clinicians, reinforcing the perception that mechanical foot pain has minimal burden and impact [8–10]. The true impact is likely to be high, because 30% of people with mechanical foot pain report persistent and severe symptoms [11]. The risk factors for developing persistent and severe mechanical foot pain include excess body weight, working in manual and intermediate occupations, having poorer physical and mental health, having catastrophizing beliefs, having greater foot-specific functional limitation, and self-assessed hallux valgus [11]. The burden and impact of mechanical foot pain are greatest in lower socioeconomic groups [6], who have an increased likelihood of concomitant knee or hip pains, leading to greater physical and mental burden [12], increased frequency of general practice consultations [5] and increased likelihood of work restrictions and early retirement [13–16].
In general practice and rheumatology clinics, foot pain is often overlooked owing to barriers of performing assessment and removing footwear and hosiery in busy clinics [17]. Foot pain presentations are perceived as challenging in the more complex regions of the midfoot, hindfoot or ankle [18], and this is exacerbated by a lack of diagnostic tests and low confidence and skills shown by the medical and nursing community [19–23]. To aid clinical confidence and recognition, the most common foot conditions in regions for the forefoot, midfoot and hindfoot (for a summary, see Table 1) are presented, followed by clinical management.
서론
기계적 발 통증(mechanical foot pain)은
체중 부하 동작 패턴과 관련된 근골격계 발 통증을 의미합니다.
유병률은
정의와 연령대에 따라 13~39%로 다양하며,
일상 활동(서 있기, 걷기, 계단 오르기)에 지장을 주는 장애성 발 통증은 8~10% 정도입니다.
나이 증가가 가장 큰 위험 요인이며,
55~64세 사이에 최고 발병률을 보입니다.
비만은 발 통증 발생과 중증도에 영향을 주며,
다발성 하지 통증 위험도 높입니다.
여성에서 장애성 발 통증 보고가 남성보다 많습니다.
낮은 사회경제 계층에서 부담이 더 큽니다.
유병률이 높음에도 불구하고 발 통증 환자의 12%만 1차 진료를 찾으며,
이는 발 통증의 부담이 적다는 오해를 강화합니다.
실제로는 30%가 지속적·심한 증상을 호소합니다.
지속적·심한 통증 위험 요인으로는
과체중, 육체노동/중간 직업, 신체·정신 건강 저하, 통증 과장 믿음(catastrophizing),
발 기능 제한, 자가 평가 무지외반증(hallux valgus) 등이 있습니다.
낮은 사회경제 계층에서
무릎·엉덩이 동반 통증이 많아
신체·정신 부담이 크고, 진료 빈도 증가, 업무 제한 및 조기 퇴직 가능성이 높습니다.
일반 진료나 류마티스 클리닉에서 신
발·양말 벗기 어려움 등으로 발 통증이 종종 간과됩니다.
특히 중족·뒷발·발목 부위는 진단이 어렵고,
의료진의 진단 검사 부족과 자신감·기술 저하로 더 힘듭니다.
임상적 자신감과 인식을 돕기 위해
앞발·중족·뒷발 영역별 흔한 발 질환(표 1 요약)을 제시하고,
임상 관리 방안을 이어서 설명합니다.
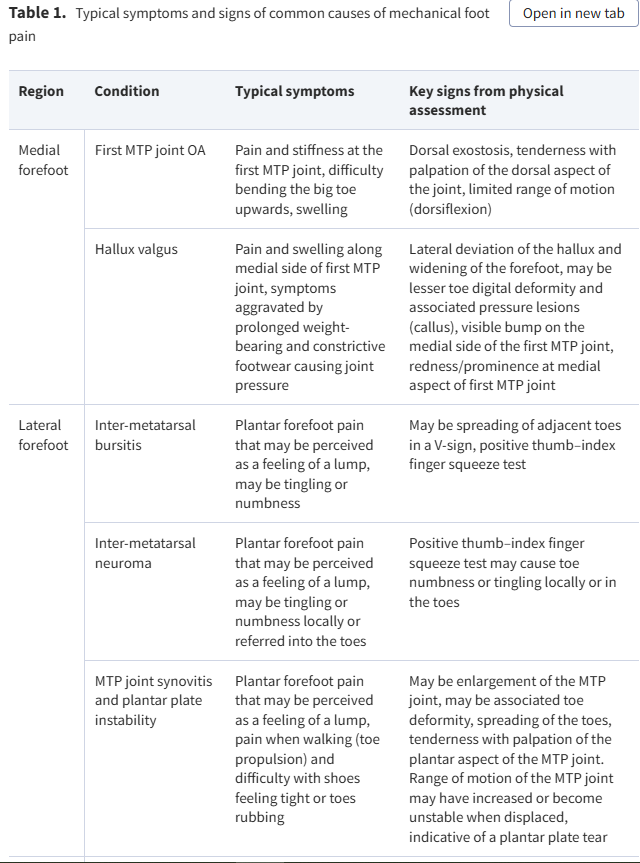
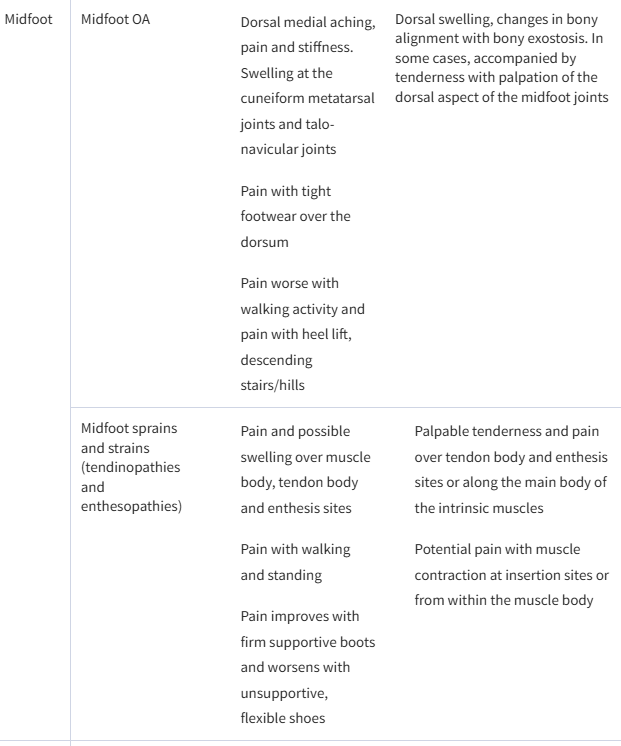
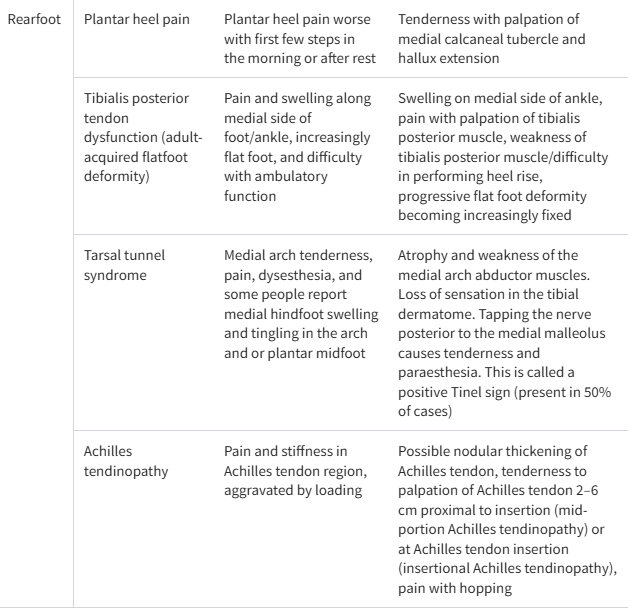
Table 1.
Typical symptoms and signs of common causes of mechanical foot pain
RegionConditionTypical symptomsKey signs from physical assessment
| Medial forefoot | First MTP joint OA | Pain and stiffness at the first MTP joint, difficulty bending the big toe upwards, swelling | Dorsal exostosis, tenderness with palpation of the dorsal aspect of the joint, limited range of motion (dorsiflexion) |
| Hallux valgus | Pain and swelling along medial side of first MTP joint, symptoms aggravated by prolonged weight-bearing and constrictive footwear causing joint pressure | Lateral deviation of the hallux and widening of the forefoot, may be lesser toe digital deformity and associated pressure lesions (callus), visible bump on the medial side of the first MTP joint, redness/prominence at medial aspect of first MTP joint | |
| Lateral forefoot | Inter-metatarsal bursitis | Plantar forefoot pain that may be perceived as a feeling of a lump, may be tingling or numbness | May be spreading of adjacent toes in a V-sign, positive thumb–index finger squeeze test |
| Inter-metatarsal neuroma | Plantar forefoot pain that may be perceived as a feeling of a lump, may be tingling or numbness locally or referred into the toes | Positive thumb–index finger squeeze test may cause toe numbness or tingling locally or in the toes | |
| MTP joint synovitis and plantar plate instability | Plantar forefoot pain that may be perceived as a feeling of a lump, pain when walking (toe propulsion) and difficulty with shoes feeling tight or toes rubbing | May be enlargement of the MTP joint, may be associated toe deformity, spreading of the toes, tenderness with palpation of the plantar aspect of the MTP joint. Range of motion of the MTP joint may have increased or become unstable when displaced, indicative of a plantar plate tear | |
| Midfoot | Midfoot OA |
| Dorsal swelling, changes in bony alignment with bony exostosis. In some cases, accompanied by tenderness with palpation of the dorsal aspect of the midfoot joints |
| Midfoot sprains and strains (tendinopathies and enthesopathies) |
|
| |
| Rearfoot | Plantar heel pain | Plantar heel pain worse with first few steps in the morning or after rest | Tenderness with palpation of medial calcaneal tubercle and hallux extension |
| Tibialis posterior tendon dysfunction (adult-acquired flatfoot deformity) | Pain and swelling along medial side of foot/ankle, increasingly flat foot, and difficulty with ambulatory function | Swelling on medial side of ankle, pain with palpation of tibialis posterior muscle, weakness of tibialis posterior muscle/difficulty in performing heel rise, progressive flat foot deformity becoming increasingly fixed | |
| Tarsal tunnel syndrome | Medial arch tenderness, pain, dysesthesia, and some people report medial hindfoot swelling and tingling in the arch and or plantar midfoot | Atrophy and weakness of the medial arch abductor muscles. Loss of sensation in the tibial dermatome. Tapping the nerve posterior to the medial malleolus causes tenderness and paraesthesia. This is called a positive Tinel sign (present in 50% of cases) | |
| Achilles tendinopathy | Pain and stiffness in Achilles tendon region, aggravated by loading | Possible nodular thickening of Achilles tendon, tenderness to palpation of Achilles tendon 2–6 cm proximal to insertion (mid-portion Achilles tendinopathy) or at Achilles tendon insertion (insertional Achilles tendinopathy), pain with hopping |
Forefoot
The forefoot (defined as the toes to the mid-shaft of the metatarsal bones) is subjected to high vertical and shear stress during gait, particularly during propulsion. Consequently, the forefoot has been reported to be the most prevalent region for foot pain. The term metatarsalgia is commonly used to describe pain occurring at the plantar aspect of the forefoot [24], which can be the result of many different conditions. Common conditions affecting the medial forefoot are first MTP joint OA and hallux valgus. At the lateral forefoot, inter-metatarsal bursitis, inter-metatarsal neuroma and synovitis–effusion of the MTP joints are most common [25]. It is worth noting that the second to fifth toes and MTP joints are common sites for the onset of inflammatory arthritis, and where persistent pain and or swelling is found, further investigations are recommended.
Medial forefoot
OA
First MTP joint OA, also known as hallux rigidus, is characterized by degeneration of joint articular cartilage and bony proliferation at joint margins, but there are also changes in surrounding joint tissues, including synovitis and subchondral bone marrow oedema [26]. The condition affects 8% of people aged ≥50 years and is more prevalent in women and those from lower socioeconomic backgrounds [27]. The main symptoms are localized pain and stiffness at the joint, which adversely impact foot-specific and general health-related quality of life [28].
First MTP joint OA can be diagnosed through history taking and physical assessment. Passive joint movement testing will reproduce pain with maximum dorsiflexion and is accompanied by a limitation of dorsiflexion range of motion [28]. A diagnostic model using pain duration of >25 months, the presence of a dorsal exostosis, hard end-feel, crepitus and <64° of joint dorsiflexion accurately predicted the presence of radiographic first MTP joint OA in a study of 181 people with joint pain [29]. Clinical guidelines for OA recommend radiographic assessment in cases of diagnostic uncertainty or for surgical planning [30].
앞발 (Forefoot)
앞발(발가락부터 중간족골(mid-shaft of the metatarsal bones)까지로 정의)은 보행 중 특히 추진(propulsion) 단계에서 높은 수직 압력과 전단 응력(shear stress)을 받습니다. 따라서 앞발은 발 통증이 가장 흔하게 발생하는 부위로 보고됩니다. 족저부 앞발 통증을 가리키는 용어로 흔히 무지족저통(metatarsalgia)이 사용되며, 이는 여러 다양한 질환의 결과로 나타날 수 있습니다.
앞발 내측(medial forefoot)에서 흔한 질환으로는 제1 중족지절관절(MTP joint) 골관절염(OA)과 무지외반증(hallux valgus)이 있습니다. 외측(lateral forefoot)에서는 중족골간 활액낭염(inter-metatarsal bursitis), 중족골간 신경종(inter-metatarsal neuroma), MTP 관절의 활막염–관절삼출(synovitis–effusion)이 가장 흔합니다. 참고로 제2~5족지와 MTP 관절은 염증성 관절염의 발병 부위로 흔하며, 통증이나 부종이 지속되면 추가 검사가 권장됩니다.
내측 앞발 (Medial forefoot)
골관절염 (OA) 제1 MTP 관절 골관절염(hallux rigidus로도 알려짐)은 관절 연골의 퇴행성 변화와 관절 가장자리의 뼈 증식(bony proliferation)이 특징이며, 주변 관절 조직에도 변화(활막염, 연골하 골수 부종 등)가 동반됩니다. 이 질환은 50세 이상 인구의 약 8%에서 발생하며, 여성과 낮은 사회경제적 배경에서 더 흔합니다. 주요 증상은 관절 부위의 국소 통증과 뻣뻣함으로, 발 특이적·전반적 건강 관련 삶의 질을 저하시킵니다.
진단은 병력 청취와 신체 검사로 가능합니다. 수동 관절 운동 검사 시 최대 배굴(dorsiflexion)에서 통증이 재현되며, 배굴 운동 범위가 제한됩니다. 한 연구(181명 대상)에서 통증 지속 기간 >25개월, 등쪽 돌출(exostosis) 유무, hard end-feel, crepitus(마찰음), 관절 배굴 <64°를 사용한 진단 모델이 방사선상 제1 MTP 관절 OA를 정확히 예측했습니다. OA 임상 지침에서는 진단 불확실 시나 수술 계획 시 방사선 검사를 권장합니다.
Hallux valgus
Hallux valgus is characterized by the progressive subluxation of the first MTP joint owing to lateral deviation of the hallux and medial deviation of the first metatarsal. As the condition progresses, the lateral deviation of the hallux can cause compression against the second toe, leading to lesser toe deformity, callus formation and difficulty in finding comfortable footwear [31]. Hallux valgus can be accompanied by a painful soft tissue (there may be an overlying adventitious bursa from footwear pressure) and bony prominence on the medial aspect of the first metatarsal head, termed a bunion. Hallux valgus is more common in women and those >65 years of age, affecting ∼23% of people aged between 18 and 65 years [32]. This condition causes significant foot pain, disability and reduced health-related quality of life, in addition to impaired balance and increased risk of falls [32–36].
Individuals with symptomatic hallux valgus report pain at the medial aspect of the first MTP joint caused by pressure between the bunion and the shoe or between the first and second toes. These symptoms are aggravated by increased weight-bearing and use of footwear with a constrictive toe-box [31]. Physical assessment reveals varying degrees of deformity, including lateral deviation of the hallux, valgus rotation of the hallux, bony prominence and s.c. bursitis at the medial aspect of the first MTP joint, and lesser toe deformity [31]. The severity of the deformity can be assessed whilst the patient is standing, using the Manchester scale, which involves comparison the patient’s foot with a standardized set of photographs [37] (Fig. 1). Radiological assessment is not necessary, but dorsoplantar weight-bearing radiographs can confirm the presence of the condition (where hallux abductus angle is >15°) [38, 39].
무지외반증 (Hallux valgus)
무지외반증은
무지(hallux)의 외측 편위(lateral deviation)와
제1 중족골의 내측 편위(medial deviation)로 인해
제1 MTP 관절의 점진적 아탈구(subluxation)가 특징입니다.
진행되면서 무지가 제2족지에 압박을 가해
소족지 변형(lesser toe deformity), 굳은살(callus) 형성, 편안한 신발 착용 어려움을 유발할 수 있습니다.
무지외반증은
제1 중족골두 내측에 통증성 연조직(신발 압박으로 인한 부가 활액낭 가능)과 뼈 돌출(bunion)이 동반될 수 있습니다.
이 질환은 여성과 65세 이상에서 더 흔하며,
18~65세 인구의 약 23%에 영향을 줍니다.
상당한 발 통증, 장애, 건강 관련 삶의 질 저하를 유발하며,
균형 장애와 낙상 위험 증가도 동반합니다.
증상이 있는 무지외반증 환자는
제1 MTP 관절 내측 통증을 호소하며,
이는 bunion과 신발 사이 압력이나 제1·2족지 사이 압박으로 발생합니다.
체중 부하 증가와 발가락 부분(toe-box)이
좁은 신발 착용 시 증상이 악화됩니다.
신체 검사에서는
무지의 외측 편위, 무지 회전(valgus rotation), 제1 MTP 관절 내측 뼈 돌출과 피하 활액낭염, 소족지 변형 등
다양한 정도의 변형이 관찰됩니다.
변형 정도는 환자가 서 있는 상태에서 Manchester scale을 사용해 평가하며, 표준화된 사진 세트와 환자 발을 비교합니다 (Fig. 1 참조).
방사선 검사는 필수 아니지만, 체중 부하 dorsoplantar 방사선 사진에서 hallux abductus angle >15°이면 확진할 수 있습니다.
Figure 1.
Manchester scale hallux valgus grading photographs. (A) Grade 1 (no deformity). (B) Grade 2 (mild deformity). (C) Grade 3 (moderate deformity). (D) Grade 4 (severe deformity). From The Grading of Hallux Valgus: The Manchester Scale, by Garrow AP, Papageorgiou A, Silman AJ, et al., JAPMA 91(2): 74–78, 2001; https://doi.org/10.7547/87507315-91-2-74. Used with permission from the American Podiatric Medical Association
Lesser forefootInter-metatarsal and plantar bursitis
Within the forefoot, inter-metatarsal bursae are located between the MTP joints, dorsal to the deep transverse inter-metatarsal ligament [40]. Inter-metatarsal bursitis occurs owing to excessive friction or pressure from the surrounding tissues [41, 42]. Likewise, adventitial plantar bursitis develops in the soft tissues of the forefoot beneath the MTP joints owing to excessive shearing and pressure from the bony structures of the foot with the weight-bearing surface [42, 43].
MTP joint synovitis and instability
Inflammation of the lesser MTP joints, termed synovitis, results from excessive pressure on the plantar forefoot. Over time, the inflammation combined with continuous pressure can weaken stabilizing structures of the joint capsule, including the plantar plate and collateral ligaments. This can lead a progressive subluxation of the proximal phalanx, a condition termed plantar plate syndrome or pre-dislocation syndrome [43, 44]. The second and third MTP joints are commonly affected owing to the significant load they bear [45]. Additionally, the lesser MTP joints can be subjected to increased load owing to first MTP joint pathology or surgery [46, 47].
Inter-metatarsal neuroma
Inter-metatarsal neuromas affect the common plantar digital nerves [48]. They are not true neuromas; instead, they are benign masses composed of perineural fibrosis, local vascular proliferation and nerve degeneration [48, 49]. These lesions typically occur in the second or third web space [48]. In general practice clinics, inter-metatarsal neuroma is reported as the second most common compressive neuropathy presentation behind carpal tunnel syndrome [50], presenting more commonly in women and those aged ≥45 years [50]. Inter-metatarsal neuromas develop because of pressure on the inter-digital nerve from the metatarsal bones or deep transverse inter-metatarsal ligament. Inter-metatarsal neuromas are frequently observed in conjunction with inter-metatarsal bursitis, suggesting a possible link between the two conditions [48, 49].
Diagnosis of lesser forefoot pain
Diagnosing lesser forefoot pain based solely on history taking and a physical assessment is challenging because of the similarity in symptoms and signs for different conditions. Individuals with these conditions report localized dull or sharp pain at the plantar aspect of their forefoot that is aggravated by forefoot loading and constrictive footwear. They may also experience swelling or tingling and perceive feeling a lump beneath the forefoot, described as walking on pebbles or a ridge in the shoe [43, 48]. There may be enlargement of the MTP joint where there is moderate effusion–synovitis, deformity of the toe where pre-dislocation syndrome is present, and spreading of the toes where inter-metatarsal bursitis is present [41]. By palpating the plantar aspect of the MTP joints, immediately distal to the metatarsal head, the presence of pain can confirm MTP joint pathology. Additionally, a thumb–index finger squeeze test of the inter-metatarsal spaces has been reported to have high diagnostic accuracy (sensitivity and specificity >95%) for inter-metatarsal neuroma [51]. However, imaging through musculoskeletal US or MRI is important to confirm a specific diagnosis of lesser forefoot pathology, with high diagnostic accuracy to inform surgical opinion [43, 52].
Midfoot
Midfoot pain affects 20% of people >50 years of age, affecting more women than men, and those in a manual occupations [53]. The midfoot (defined as the area from the mid-shaft of the metatarsals to the talus neck) is a complex region supported by tarsal ligaments, intrinsic muscles and fascia. The midfoot is subjected to mechanical load placed on the arch span during standing and walking. This can be exacerbated by age [54], changes in body weight, pregnancy and muscle fatigue, which are associated with greater midfoot pain and higher plantar pressures [55–58].
Midfoot OA
Symptomatic midfoot OA is the most common presenting condition in this region, affecting 12% of people >50 years of age, 80% of whom report daily pain and disability [53]. Pain in the dorsal central foot region is associated with medial and central midfoot OA with a greater prevalence of disability [59], which requires either weight-bearing radiographs [60] or US imaging assessment to identify joint changes [61]. Midfoot OA presents as an aching pain associated with walking and standing. This can present with osteophytosis and joint narrowing, and MRI studies suggest that bone marrow lesions and tendon signal at the sheath and enthesis can also be associated [62]. Cross-sectional studies suggest that painful midfoot OA can be associated with a flatter foot posture and reduced muscle strength [59, 63].
Midfoot soft tissue pains
Ligament pain in the midfoot usually follows a flexion and rotational sports injury and accounts for a small percentage of visits to emergency departments [64]. These incidents are also known to be associated with high-energy contact injuries, dorsal blunt trauma or higher-energy falls that will often lead to chronic pain and deformity if missed or left untreated [65]. This can present as a persistent dorsal pain aggravated by loading and can overlap with sprain of the ankle or intrinsic foot muscles, but little is known about non-traumatic presentations owing to the complexity of the anatomical structures, poor discernment on foot radiographs and the necessity for MRI investigations for diagnosis [66, 67].
Enthesopathy in the midfoot can be associated with the anterior tibialis, posterior tibialis and peroneus longus tendons, all of which insert within close proximity in the medial arch to support the span of the foot. Studies show that a low degree of tendon effusion and signal at the enthesis can present in healthy non-painful feet, which suggests that this could be a normal variant or a sign of mechanical loading [68, 69]. Enlarged entheses with effusion in multiple locations are found in people with RA and SpA, especially at the peroneus brevis [68, 70, 71]. Tendon enthesopathy can also be a feature of midfoot OA, and this is particularly apparent with the posterior tibialis tendon and peroneus longus tendons, which have insertions into the medial tarsal bones [62].
Pain in the anterior and extensor tendons is often related to acute injury and not commonly reported within sports or running literature [72]. Anecdotally, strains and swelling of these tendons can present in those who adopt an adaptive toe-walking gait style to offload other areas of foot pain or where there is friction with midfoot osteophytosis and footwear. Most of the literature concentrates on the posterior tibialis tendon and flexor longus tendons in dance and sports injuries, which cross the midfoot, and these are described elsewhere [73, 74].
Rearfoot
Rearfoot pain is common. A population-based study of adults demonstrated that one in four cases of foot pain can be attributed to pain in the hindfoot and heel [4]. Common causes of mechanical foot pain for the rearfoot are plantar heel pain, tibialis posterior tendon dysfunction and Achilles tendinopathy.
Plantar heel pain
Plantar heel pain, including plantar fasciitis, plantar fasciopathy, heel pain syndrome and fat pad atrophy [75], affects 4–10% of the population [76] and is more common in people aged >50 years and those who are overweight [76]. Individuals who engage in repetitive weight-bearing activities, such as running [77], or who have occupations that involve standing on hard surfaces for extended periods [78] are at a higher risk of developing plantar heel pain. Plantar heel pain is characterized by pain upon weight-bearing [79] and involves several tissues in the plantar aspect of the heel. However, the insertion of the plantar fascia is considered the main source of the pain for most patients [79].
The diagnosis of plantar heel pain is based on symptoms such as pain and tenderness in the plantar heel, especially after prolonged weight-bearing or when taking the first steps in the morning. During physical assessment, tenderness is elicited upon palpation of the proximal insertion of the plantar fascia at the medial calcaneal tubercle [80]. Radiological assessment is not needed for diagnosis, unless there is diagnostic uncertainty or for surgical planning [81]. Radiography is of limited value because the presence of a calcaneal spur occurs in ~50% of asymptomatic individuals [82]. Musculoskeletal US and MRI are more appropriate when there is diagnostic uncertainty, to help to visualize thickening (>4 mm) of the plantar fascia, a key feature of plantar heel pain [83].
Tibialis posterior tendon dysfunction
Tibialis posterior tendon dysfunction, also known as adult-acquired flatfoot deformity or progressive collapsing foot deformity, is a complex disorder characterized by tibialis posterior weakening and tendinopathy that can be associated with OA changes of the midfoot and hindfoot, and in some cases, this leads to progressive flattening of the midfoot [84, 85]. The prevalence of tibialis posterior tendon dysfunction is unknown, but one study from a general medical clinic in the UK suggested a prevalence of 3% in women aged >40 years of age [86]. It is more common in females, those aged 40–69 years of age and those who are overweight [86, 87].
Key diagnostic features of this condition are pain and swelling along the medial side of the foot, pain with palpation and weakness of the tibialis posterior muscle, difficulty in performing the standing heel raise test (as evidenced by a lack of calcaneal inversion at peak rise, an inability to complete full range of plantarflexion or reduced endurance capacity), and a pronated foot [14, 88–90].
Achilles tendinopathy
Achilles tendinopathy is characterized by degeneration of the Achilles tendon rather than inflammation and is caused by ineffective tendon repair owing to mechanical loading [91]. As a result, the term tendinopathy is used to describe this condition instead of tendinitis [92]. Achilles tendinopathy affects athletes and sedentary individuals [93–95], males and females equally, and those >35 years of age [94, 96]. The condition adversely impacts health-related quality of life and work productivity [97–99].
People with Achilles tendinopathy report pain and stiffness in the Achilles tendon region, with an insidious onset that is aggravated by loading activities, such as running and jumping [92, 100]. During a physical assessment, patients can experience pain and display weakness with single-leg heel raise and hopping. Palpation of the Achilles tendon can reveal pain and localized nodular thickening [92, 100]. The location of the symptoms can help to differentiate the two subtypes of Achilles tendinopathy: mid-portion and insertional. Mid-portion Achilles tendinopathy occurs when pain occurs 2–6 cm proximal to the calcaneal insertion, whereas insertional Achilles tendinopathy occurs at the calcaneal insertion [92, 100]. In cases where insertional Achilles tendinopathy is present, retrocalcaneal bursitis or Haglund’s deformity may co-exist [92]. Musculoskeletal US and MRI are effective diagnostic tools for identifying Achilles tendinopathy when the diagnosis is uncertain. These modalities provide good to excellent diagnostic accuracy and allow for visualization of pathology of the Achilles tendon and surrounding structures, such as the retrocalcaneal bursa [101]. However, although imaging can help to identify the presence and severity of the condition, studies show a poor relationship between imaging features and pain severity or prognosis [101]; therefore, imaging should be used judiciously.
Foot pain and red flags
A painful, inflamed foot with no open wound can be a diagnostic challenge and often leads to a delay in treatment. Inflammatory arthritis should be considered, especially in the forefoot and toes; gout, SpA and RA are the most common presentations. Charcot neuroarthropathy should be considered in cases of midfoot pain, persistent inflammation and walking difficulties. It presents in middle-aged people with diabetes-related peripheral neuropathy and is more commonly misdiagnosed when associated with alcoholism or undiagnosed sensory loss [102], or dismissed as fragility fractures or progressive flat foot deformity [103]. Early diagnosis and intervention are key to stabilize the foot; otherwise, the resultant ‘rocker bottom’ deformity increases the risk of amputation [104].
Other concerns are highly localized foot pains and inflammation at bone sites, which are more likely to represent a stress response or occult stress fracture in the short tarsal bones and second to fourth metatarsal bones [105]. In cases of new persistent pain with unrelenting or firm swelling in people <40 years of age, space-occupying lesions should also be considered to prevent delays in care [106]. Most presentations are benign, and primary soft tissue and malignant tumours of the foot are rare [106]. Compared with sites above the tibia, sarcomas are less invasive and have a reduced mortality rate, which can be attributed to the size of the structures and interference with function, which can lead to early detection [107]. Metastatic foot lesions (most commonly associated with prostate, bladder and breast cancer) tend to present with severe pain and disability and are more likely to be confused with fragility fractures in the metatarsal bones identifiable on radiographs [108].
발 통증과 위험 신호 (Foot pain and red flags)
열린 상처가 없는 통증이 심하고 염증이 있는 발은
진단이 어렵고, 치료가 늦어지는 경우가 많습니다.
특히
앞발(forefoot)과 발가락 부위에서는 염증성 관절염을 반드시 고려해야 하며,
가장 흔한 원인은 통풍(gout), 척추관절염(SpA), 류마티스 관절염(RA)입니다.
Charcot 신경관절병(Charcot neuroarthropathy)은
중족(midfoot) 통증, 지속적인 염증, 걷기 어려움이 있을 때 고려해야 합니다.
이는 주로 당뇨병 관련 말초 신경병증이 있는 중년 환자에게 발생하며,
알코올 중독이나 진단되지 않은 감각 상실과 동반될 때 오진되기 쉽습니다.
또는 취약성 골절(fragility fracture)이나 진행성 편평족 변형으로 치부되기도 합니다.
조기 진단과 개입이 매우 중요합니다.
그렇지 않으면 발이 rocker bottom deformity(바위 바닥처럼 휘어진 변형)로 진행되어 절단(amputation) 위험을 크게 높입니다.
다른 우려 사항으로는
뼈 부위에 국소적으로 심한 통증과 염증이 있는 경우로,
이는 단거리 족근골(short tarsal bones)이나
제2~4 중족골(metatarsal bones)에서 스트레스 반응(stress response) 또는
숨겨진 스트레스 골절(occult stress fracture)일 가능성이 큽니다.
40세 미만에서
새롭게 지속되는 통증과 꾸준하거나 단단한 부종이 있는 경우,
공간 점유 병변(space-occupying lesions)도 고려해야 하며,
치료 지연을 막기 위해 신속히 평가합니다.
대부분은 양성(benign)이지만,
발의 원발성 연조직 종양이나 악성 종양은 드뭅니다.
경골 위 부위와 비교해 발의 육종(sarcomas)은 덜 침습적이고 사망률이 낮은데,
이는 구조물 크기와 기능 장애로 인해 조기 발견이 가능하기 때문입니다.
전이성 발 병변(metastatic foot lesions) (가장 흔히 전립선암, 방광암, 유방암 관련)은
심한 통증과 장애를 유발하며, 중족골의 취약성 골절과 혼동되기 쉽습니다.
이는 방사선 사진으로 확인할 수 있습니다.
Management
Treatment aims to reduce a patient’s symptoms, facilitate healing, promote return to functional activity and prevent re-injury [109]. This can be achieved by managing symptoms, combined with reducing tissue stress of the affected tissue(s) to a tolerable level and improving the ability of the affected tissue(s) to withstand future load/stress [110]. This requires the multifaceted approach described below and, in some cases, multidisciplinary treatment.
Lifestyle and education strategies
Modification of daily activities is important to reduce stress on affected tissues to allow them to heal. Aggravating activities will be unique to each patient but are likely to include occupational activities, caring duties and exercise. It may not always be feasible to avoid or even reduce time spent in these activities. For example, in occupational settings, it may not be possible for an individual not to attend work. In such cases, modification or pacing of activities may be more feasible.
Education, support and referral for weight loss (if appropriate) are important components of management [111]. At present, there are no randomized trials investigating the effectiveness of weight-loss interventions for mechanical foot pain. However, in obese patients with painful foot and ankle arthritis, simulated weight loss to a more normal body mass resulted in a significant improvement in pain [112]. Furthermore, studies of obese patients undergoing bariatric surgery have reported a marked reduction in the prevalence of foot and ankle pain post-operatively [113].
Mechanical strategies
In-shoe foot orthoses, padding and strapping can improve pain by reducing the magnitude of plantar pressure, changing motion of foot joints and reducing tissue stress. Various types of orthotic devices, padding and strapping techniques can be applied for specific purposes, and the interested reader is referred to key texts [114, 115]. The current evidence from randomized trials demonstrates that: for first MTP joint OA, shoe-stiffening inserts are effective for ≤12 months [116], but arch-contouring foot orthoses and cushioning sham showed equal effectiveness [117]; for hallux valgus, arch-contouring foot orthoses are effective at 6 months, but not at 12 months [118]; for midfoot OA, arch-contouring foot orthoses are somewhat effective (in a pilot trial) [119]; for tibialis posterior tendon dysfunction, arch-contouring foot orthoses are effective (provided alongside exercise therapy) [120]; and for mid-portion Achilles tendinopathy, arch-contouring foot orthoses are not effective (≤12 months) [121], but in-shoe heel lifts are effective [122].
Education on and consistent use of appropriate footwear is also crucial. In a randomized trial, appropriately fitting footwear significantly improved foot pain and disability in older people with disabling foot pain [123]. Commonly recommended features of appropriate footwear include [124, 125]: sensible style appropriate for activity; appropriate fixation (lace, buckle, velcro); supportive and appropriately fitting (length, width, toe-box shape and depth); shoes that are not excessively worn (upper, midsole and outsole); heel elevation of 5–10 mm; and sole flexion point at the level of the MTP joints and not excessively flexible.
Appropriate pharmacological management
The appropriate use of pharmacological agents can assist the effective management of mechanical foot pain, although specific drug trials are lacking. To ensure the safe and effective use of medication, relevant prescribing guidelines, such as the Therapeutic Guidelines and national evidence-based formularies, need to be consulted [126]. Short-term relief of symptoms can be achieved using paracetamol and NSAIDs [127]. Most cases of mechanical foot pain are superficial, and topical NSAIDs are preferred over oral NSAIDs owing to their better safety profile [128]. For localized mechanical foot pain that is difficult to manage, CS injections can provide short-term pain relief (≤6 weeks) [129–132]. Although IA hyaluronan injections and autologous growth factor injections might be exciting alternative pharmacological approaches for OA and for tendon and plantar fascia pathology, respectively, their effectiveness has not been established in rigorous randomized trials [133–135]. Opioids have limited benefits and significant risks of harm, hence their use is limited to recalcitrant pain, with close monitoring [126].
Therapeutic exercise
Therapeutic strengthening exercises can be used to target the affected muscles and improve the ability of tissue to withstand future stress and strain, reducing the risk of re-injury. The type, intensity and duration of strengthening exercises needs to be individualized. For Achilles tendinopathy, calf muscle eccentric exercises are supported by the strongest evidence [92]. However, targeted strengthening exercises might be effective for other conditions associated with reduced muscle strength, including hallux valgus [136], midfoot OA [63, 137] and tibialis posterior tendon dysfunction [138]. The role of stretching in the treatment of common conditions causing mechanical foot pain, such as plantar fasciitis, Achilles tendinopathy and adult-acquired flat foot, is less clear [92, 139, 140].
Research and future avenues for development
Several clinical and research organizations have highlighted the lack of research into the diagnosis and treatment of musculoskeletal foot pain, particularly when compared with other equally common sites of pain, such as the hand and hip [141–146]. To overcome this, research priorities have been developed, and the top-rated priorities were as follows: the development of robust outcome measures; development of clinical diagnostic criteria; understanding the impact and burden of foot problems; and further investigations into foot pain treatments [141–146].
This review has highlighted the strong relationships between foot pain and increased body mass, in addition to emerging evidence showing the relationship between foot pain and muscle strength. Further research is needed to identify whether fat loss and increased muscle strength will help mechanical foot pain. This would be particularly important to understand in groups with lower leg and foot pains, because this can compound disability [147–149].
Conclusion
Mechanical foot pain includes a large number of pathologies in the forefoot, midfoot and hindfoot. Traditional treatments foot mechanical foot pain are based on reassurance of healing times, pain management, managing the pain through pacing and activity modification, and offering pressure/load management using orthoses and footwear. More research is needed to explore causes and treatments of mechanical foot pain, with particular emphasis on understanding the role of muscle strengthening and weight-loss interventions.
Data availability
There are no new data associated with this article.
Funding
No funding was received for this article.
Disclosure statement: Both authors declare there are no conflicts of interest.
Acknowledgements
We would like to acknowledge all the researchers and participants whose work we have cited in this manuscript.
References
1
Gates
LS
,
Arden
NK
,
Hannan
MT
et al.
Prevalence of foot pain across an international consortium of population‐based cohorts
.
Arthritis Care Res (Hoboken)
2019
;
71
:
661
–
70
.
2
Garrow
AP
,
Silman
AJ
,
Macfarlane
GJ.
The Cheshire foot pain and disability survey: a population survey assessing prevalence and associations
.
Pain
2004
;
110
:
378
–
84
.
3
Roddy
E
,
Muller
S
,
Thomas
E.
Onset and persistence of disabling foot pain in community-dwelling older adults over a 3-year period: a prospective cohort study
.
J Gerontol Ser A Biol Sci Med Sci
2011
;
66
:
474
–
80
.
4
Hill
CL
,
Gill
T
,
Menz
HB
,
Taylor
AW.
Prevalence and correlates of foot pain in a population-based study: the North West Adelaide health study
.
J Foot Ankle Res
2008
;
1
:
2
–
7
.
5
Finney
A
,
Dziedzic
KS
,
Lewis
M
,
Healey
E.
Multisite peripheral joint pain: a cross-sectional study of prevalence and impact on general health, quality of life, pain intensity and consultation behaviour
.
BMC Musculoskelet Disord
2017
;
18
:
535
–
8
.
6
Menz
HB
,
Marshall
M
,
Thomas
MJ
et al.
Incidence and progression of hallux valgus: a prospective cohort study
.
Arthritis Care Res (Hoboken)
2023
;
75
:
166
–
73
.
7
Menz
HB
,
Jordan
KP
,
Roddy
E
,
Croft
PR.
Characteristics of primary care consultations for musculoskeletal foot and ankle problems in the UK
.
Rheumatology
2010
;
49
:
1391
–
8
.
8
Menz
HB
,
Jordan
KP
,
Roddy
E
,
Croft
PR.
Musculoskeletal foot problems in primary care: what influences older people to consult?
Rheumatology
2010
;
49
:
2109
–
16
.
9
Swain
S
,
Sarmanova
A
,
Mallen
C
et al.
Trends in incidence and prevalence of osteoarthritis in the United Kingdom: findings from the Clinical Practice Research Datalink (CPRD)
.
Osteoarthritis Cartilage
2020
;
28
:
792
–
801
.
10
Munro
BJ
,
Steele
JR.
Foot-care awareness. A survey of persons aged 65 years and older
.
J Am Podiatr Med Assoc
1998
;
88
:
242
–
8
.
11
Marshall
M
,
Blagojevic‐Bucknall
M
,
Rathod‐Mistry
T
et al.
Identifying long‐term trajectories of foot pain severity and potential prognostic factors: a population‐based cohort study
.
Arthritis Care Res (Hoboken)
2023
;
75
:
1123
–
31
.