인체에 대한 모든 탐구는 정상구조로부터 출발한다.
MRI 영상은 구조탐구와 질병 찾기의 출발점이다.
panic bird......
This article illustrates normal spinal anatomy as defined by MR imaging, describes commonly used spinal MR imaging
protocols (Tables 1–3), and discusses associated common artifacts.
SPINAL MR IMAGING TECHNIQUES
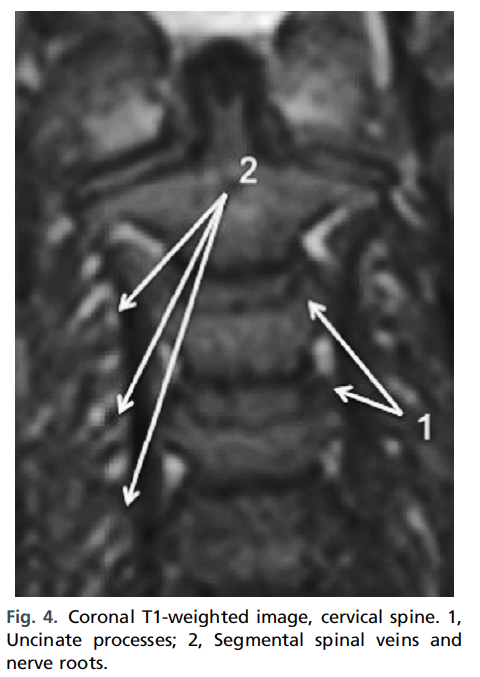
Sagittal and axial magnetic resonance images should be acquired through the cervical, thoracic, and lumbar segments of the spine, as they are generally considered complementary, and imaging the spine in only one plane may result in misinterpretation. The addition of coronal images may also be useful, especially in patients with scoliosis.
Slice thickness from 3 to 4 mm is generally optimal for imaging of the spine.
The pulse sequences used are determined by the clinical indications for the examination based on the following major categories: degenerative disease including radicular symptomatology, trauma, cord compression/bony metastases, and
infection.4
척추 MRI사진 영상은 크게 네가지 목적
1) degenerative disease(radicular pain)
2) trauma
3) cord compression/bony metastases
4) infection
Spin-echo and fast spin-echo sequences are the most common sequences used in spinal MR imaging. Short tau inversion recovery (STIR) imaging is useful to assess the bone marrow5 and in cases of infectious,6 inflammatory,
7 and neoplastic8 lesions. STIR imaging is also useful in the workup of trauma, to assess for ligamentous injury9 and changes from hemorrhage and/or edema. Contrast-enhanced imaging should be used, unless contraindicated, for indications including evaluation of the postoperative spine, suspected infection, or intradural or non traumatic cord lesions.10 Abnormalities within the epidural space identified during unenhanced evaluation for metastases and/or cord compression can be better delineated using contrast-enhanced images.10
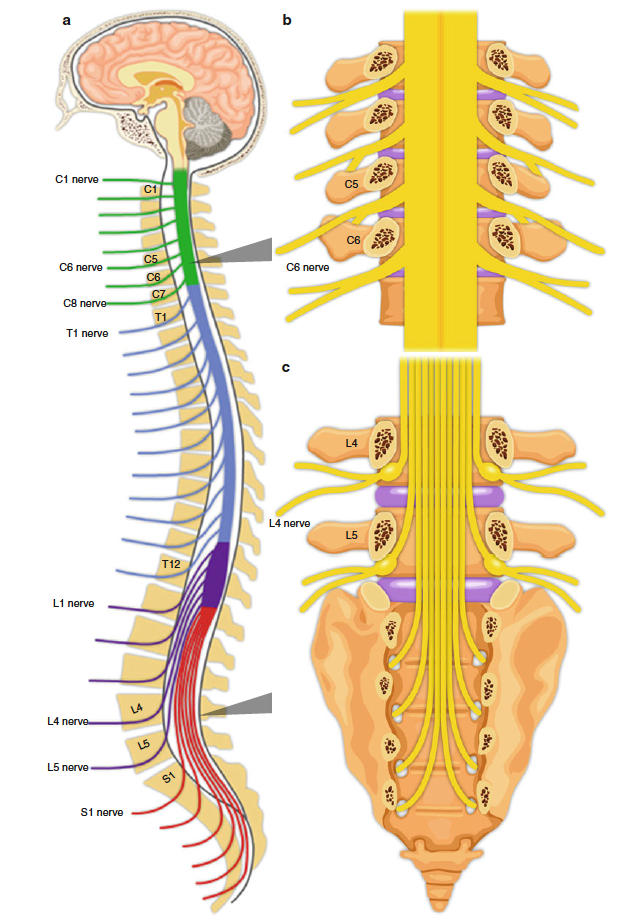
Gradient-recalled echo (GRE), or gradient-echo, sequences allow for delineation of bone and disk margins, provide excellent contrast between the spinal cord and surrounding subarachnoid space, and allow clear visualization of the neural foramina and exiting nerve roots. Gradient-echo axial images are used in the cervical and thoracic spine to detect spinal canal and foramina stenoses11 and serve as an important complement to long repetition time spin-echo imaging, given faster acquisition time of GRE. As a result, GRE images are less susceptible to patient motion artifact.
Although signal-to-noise ratio is increased with GRE, fat is of low signal intensity on GRE sequences compared with T1-weighted spinecho imaging; as a result, morphologic detail defined by fat is not as well demonstrated on GRE images as on spin-echo images.12 Proton density images can be obtained simultaneously (TR 2000 to 3000 milliseconds or greater,
TE 20 to 90 milliseconds) when obtaining T1-weighted images and can also be derived from an earlier (first) echo while generating T2- weighted images. Proton density images of the spine are not routinely obtained but can provide valuable information concerning normal and pathologic spinal morphology.5

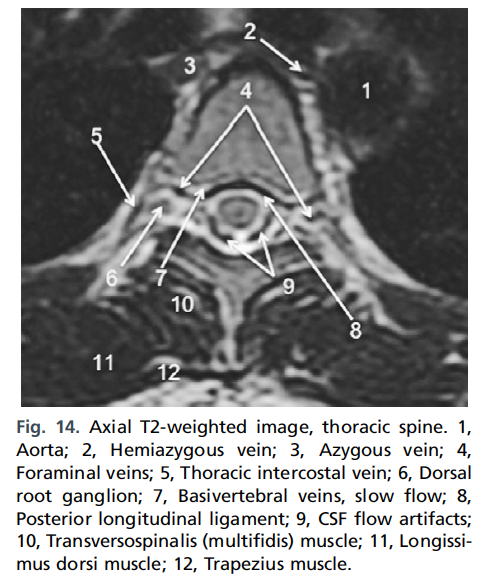
Fig. 1. Sagittal T2-weighted image, cervical spine. 1,Clivus; 2, Atlanto-occipital ligament; 3, Anterior longitudinal ligament; 4, Anterior arch C1; 5, Superior fascicle of cruciform ligament/tectorial membrane; 6, Apical ligament; 7, Transverse ligament (of cruciform ligament); 8, Posterior arch C1; 9, Posterior occipitalatlantal membrane; 10, Nuchal ligament; 11, Semispinalis
capitis muscle; 12, Cervical spinal cord; 13, Posterior longitudinal ligament/anterior thecal sac dura; 14, Posterior dural sac; 15, Interspinous ligament; 16, Gray matter along central canal; 17, Supraspinous ligament; 18, Ligamentum flavum; 19, Dental synchondrosis (disc anlage).
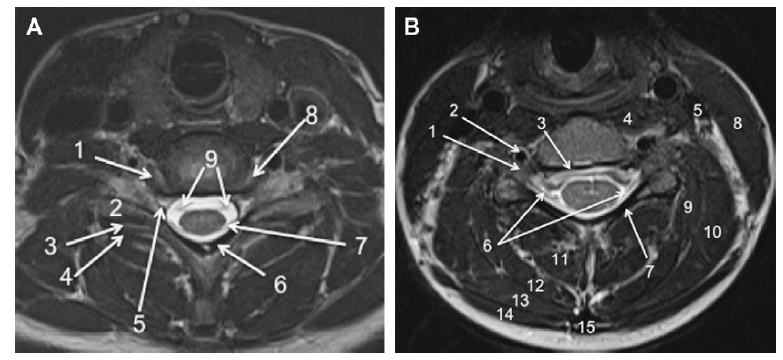
Fig. 3. (A) Axial T2-weighted image, lower cervical spine. 1, Uncinate process C7; 2, Superior articular process C7;
3, Apophyseal (facet) joint; 4, Inferior articular process C6; 5, Foraminal vein; 6, Ligamentum flavum/cortex of
lamina; 7, Dorsal rootlet C7; 8, Uncovertebral joint; 9, Ventral rootlets C7. (B) Axial T2-weighted image, mid
cervical spine. 1, Dorsal root ganglion; 2, Vertebral artery; 3, Posterior longitudinal ligament/anterior thecal
sac dura; 4, Longus colli muscle; 5, Internal jugular vein; 6, Dorsal rootlets; 7, Lamina; 8, Sternocleidomastoid
muscle; 9, Longissimus capitis muscle; 10, Levator scapulae muscle; 11, Semispinalis colli muscle; 12, Semispinalis
capitis muscle; 13, Splenius capitis muscle; 14, Trapezius muscle; 15, Nuchal ligament.