physical rehabilitation of the injured athlete
The cervical spine is one of the most commonly injured areas in the human body, with pathologies ranging from chronic in
nature because of poor postural habits to those occurring as a result of acute, traumatic injuries. Rehabilitation techniques have changed in recent years because of a more thorough understanding of this region. Such understanding has allowed rehabilitation to evolve from structured protocols that have relied solely on static, isometric exercises to programs that address the need for normalization of the tissue's tolerance of functional loading (forces causing stretching or compression) so that dynamic, isotonic exercises can be instituted to restore postural deficits and regain neuromuscular control, strength, and endurance.
- 인체에서 경추는 가장 흔히 손상을 당하는 부위.
- 재활치료 테크닉은 경추생체역학 지식이 깊어짐에 따라 변화함.
- 재활치료는 단순히 정적 운동, 등척성 운동 프로그램을 통해 기능적 부하의 내성을 양측 균형화할 뿐아니라 동적, 등장성 운동프로그램을 통해 자세 틀어짐을 정상화하고 신경근 조절, 근력, 근지구력을 회복하는 것임.
This chapter addresses the anatomic, arthrokinematic, and biomechanical considerations needed during the evaluation and treatment process. Differential assessment of the tissues related to the cervical spine and evaluation of joint play and mobility will allow the clinician to determine whether tissue lesions and pathologic hypermobility or hypo-mobility are present and to address these pathologies with manual techniques and the application of an exercise regimen to expedite the healing process.
- 이 챕터는 autonomic, arthrokinematic, biomechanical 고려를 추가함.
Various special tests are presented that allow the clinician to determine the specific cause of pain and loss of function. By performing a complete evaluation procedure, the sports rehabilitation specialist will develop a better understanding of the exact tissues involved in the pathology. This will allow the clinician to provide the optimal stimulus to facilitate healing of that tissue.
- 다양한 특수검사가 임상의로 하여금 통증의 원인과 기능소실을 결정하도록 함.
- 완전한 검사과정을 통해 스포츠 재활은 병리와 연관된 정확한 조직을 이해함. 이는 치유촉진에 적합한 자극을 제공하게 함.
Anatomy 경추 해부학
It is imperative that the clinician be competent in locating and identifying the anatomic structures of the cervical spine and have
proficient understanding of their biomechanical functions to allow a thorough evaluation and institute a proper rehabilitation program. Therefore, this section addresses the cervical vertebral column and its surrounding ligaments, muscles, and neurovascular
structures. Because various pathologic conditions can affect one or more of these systems, it is important that the rehabilitation
specialist have a thorough functional understanding of these structures.
-임상의사는 경추의 해부학적 구조, 위치확인에 능통하고, 그것의 생체역학적 기능을 잘 알아야 적절한 재활 프로그램을 구성할수 있음.
- 그래서 이 장은 경추와 연관 인대, 근육, 신경, 혈관구조를 탐구함.
- 다양한 병리적 환경은 이 조직 시스템에 하나 이상의 영향을 주기 때문에, 재활 치료사는 모든 조직문제에 능통해야 함.
Bony Configuration
The cervical spine consists of seven vertebrae. The anatomic structure of the mid-cervical spine (C3-C6) is similar to that of the thoracic and lumbar spine in that each vertebra has a vertebral body, pedicle, lamina, and spinous process. However, the mid-cervical spine also has a number of anatomic structures that are unique to this region (Fig. 16-1 ).
- 경추는 7개 척추로 구성. C3-6 경추의 해부학적 구조는 흉추와 요추의 그것과 유사함. 척추체, pedicle, 라미나, 극돌기 등
- 하지만 mid-cervical spine은 또한 독특한 구조를 가짐.
Each mid-cervical vertebra has an uncinate process and a foramen transversarium, and their spinous processes are bifid. The foramen transversarium accommodates the vertebral artery and vein and is found in all cervical vertebrae except C7, although variations do exist. The spinous processes are bifid to allow greater range of motion (ROM) into extension and to provide a mechanical advantage for muscular attachments.
- 각각 mid-cervical 척추는 구상돌기와 foramen transversarium 을 가짐. 그리고 경추 극돌기가 양측으로 갈라져 있음. 경추 6번까지 foramen transversarium은 vertebral artery and vein을 허용함.
- 극돌기가 bifid 되어 있음으로 해서 경추신전을 크게 허용하고, 근육부착의 역학적 이로움을 제공함.
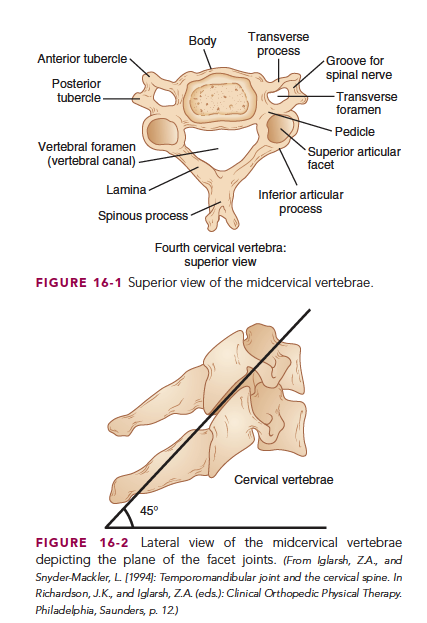
The superior surface of the vertebral bodies in the mid-cervical spine is concave in the frontal plane and convex in the sagittalplane, and the opposite is true for the inferior surfaces. These cervical vertebrae have two superior and two inferior facets that are located on the pedicles. The superior facets are oriented in a posterior direction, whereas the inferior facets are oriented in an anterior direction. The biplanar orientation of these joints requires that rotation and lateral flexion be coupled movements.
- mid cervical spine의 척추체의 상면은 전두면에서는 concave하고, 시상면에서는 convex함.
- 경추는 두개의 superior and inferior facet를 가지고 있음. 후관절을 만듬.
- 경추 후관절은 회전, 측굴에서 짝움직임을 함.
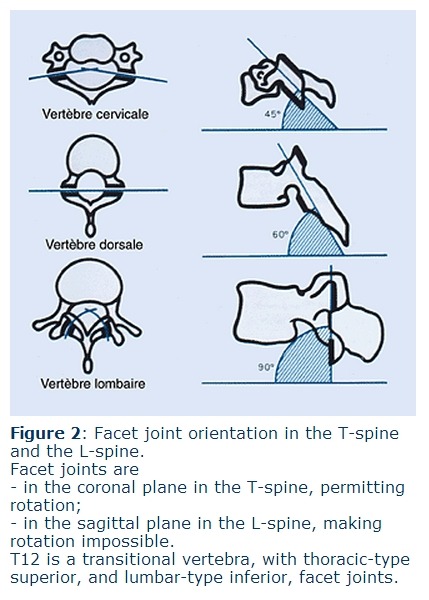
These facets articulate with the adjacent vertebrae to form facet joints (zygapophyseal joints). They have an approximate angle of 45° from the horizontal plane in the mid-cervical region (C3-C6) that decreases to approximately 30° in the lower cervical region (C7-T3) (Fig. 16-2 ).
- 경추 C3-6의 후관절과 수평면이 이루는 각도는 45도
- C7-T3의 각도는 감소되어 30도. 흉추는 60도!!
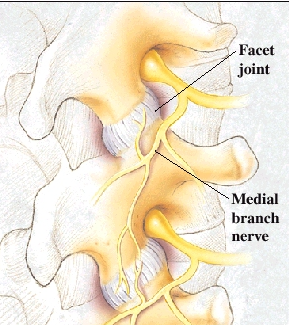
The facet joints are planar synovial joints with articular cartilage on the surfaces that is enclosed in a fibrosis joint capsule. Found within the joint capsule is meniscoid, adipose, and connective tissue.1 The medial branch of the dorsal primary ramus innervates the facet joints.
- 경추 후관절은 편평한 활액관절이고 섬유성 관절낭으로 둘러싸여 있는 관절연골면이 있는 관절.
- 후관절낭 내에서 발견되는 것은 반달모양의, 지방조직이 충만한 결합조직
- 후관절은 dorsal primary ramus의 내측지 신경지배
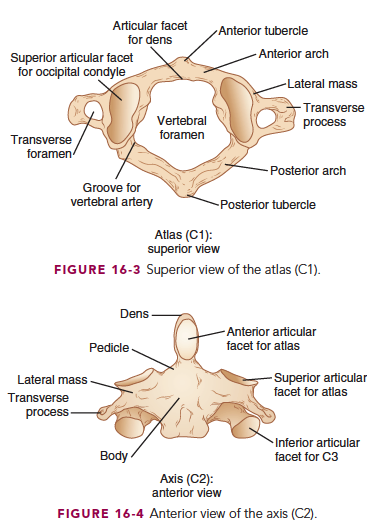
The first cervical vertebra (C1), the atlas, articulates with the occiput superiorly and the axis (C2) inferiorly. The atlas does not have a spinous process or a real vertebral body; however, the odontoid process (dens) of the axis functions as the body of C1 (see Fig. 16-4 ). The atlas consists of two lateral masses connected by anterior and posterior arches and transverse processes that provide for acceptance of weight through the articular processes.
- 환추 C1은 위쪽으로 두개골, 아래쪽으로 축추 C2와 관절함.
- 환추는 극돌기, 진짜 척추체가 없음. 하지만 축추의 odontoid process와 관절함.
- 환추는 양측으로 lateral mass가 있어서 ant and post arche를 연결하고 큰 횡돌기를 만들어 관절면을 통해 체중을 허용하도록 함.
The posterior surface of the anterior arch has a facet lined with hyaline cartilage that articulates with the odontoid process of C2 (Fig. 16-3 ). The superior articular processes are biconcave and articulate with the biconvex occipital condyles, and the inferior articular processes are biconvex and articulate with the biconvex superior facets of the axis.
- 전방 아치의 후면은 초자연골로 축추의 치돌기와 관절을 이룸.
- 환추의 상방관절면은 biconcave하고 biconvex 후두골과 관절함.
- 환추의 하방관절면은 biconvex하고 축추의 상부관절면 또한 biconvex한 관절면으로 이루어짐.
The axis (C2) contains a superior projection, the odontoid process, that articulates with the posterior aspect of the anterior arch of the atlas. The axis, like the atlas, has small transverse processes and a posterior arch instead of pedicles (Fig. 16-4 ).
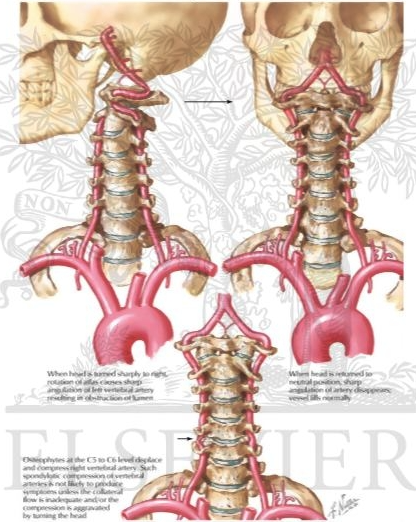
In the upper cervical spine (C1-C2), the foramen transversarium is located more laterally than in the mid-cervical spine, thus requiring the vertebral artery to ascend in a lateral direction in this region. Weight bearing is absorbed superiorly as the axis articulates with the inferior facets located on the lateral masses of the atlas and is transmitted inferiorly through the inferior facet joints, which are located more posteriorly on the axis, similar to those in the mid-cervical region. Uncovertebral joints (joints of Luschka), first described by von Luschka, are believed to develop because of degenerative changes in the annulus fibrosus (Fig. 16-5 ).
- C1-2에서 횡돌기구멍은 중부 경추보다 바깥쪽에 위치하여 Vertebral artery 외측방향으로 돌아 올라감.
- 체중부하는 축추 관절면에서 흡수되고...
- 루시카 관절은 수핵의 퇴행화와 함께 만들어진다고 믿어짐.
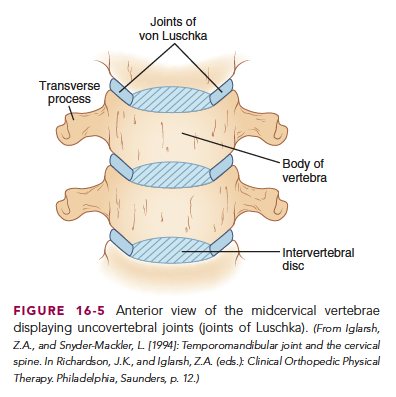
They are located on the lateral aspect of the mid-cervical vertebra and on the posterolateral aspect of C7-T1.2 Uncovertebral joints function to deepen the articular surface and provide stability as they articulate with the adjacent vertebral body. However, because of their close proximity to the spinal nerves, osteophyte formation in this region can encroach on these structures. They also limit motion, especially lateral flexion, and serve to prevent lateral disk herniation.
- 루시카 관절은 C3-7 척추의 외측면에 위치하고, C7-T12번 관절에서는 후외측면에 위치함.
- 루시카 관절은 관절면을 깊게 하고, 이웃 척추체와 관절함으로써 안정성을 제공함.
- 하지만 척추 신경근이 주위에 존재하고, 이 부위에서 골극형성은 추간 구멍을 좁혀 신경을 압박할 수 있음.
- 루시카 관절은 특히 외측굴곡 움직임을 제한하고, 측면으로 디스크 탈출을 막아줌.
Intervertebral Disk
An intervertebral disk (IVD) is present between each cervical vertebra except for the occiput and atlas (C0-C1) and the atlas and axis (C1-C2). The disks in the cervical spine are relatively thicker than those in the thoracic and lumbar spine, which allows greater ROM. The cervical disks are slightly higher anteriorly and thereby contribute to the lordotic curve in the cervical spine. The IVD is divided into a central region, the nucleus pulposus, and a peripheral ring, the annulus fibrosis.
- 추간판은 C0-C1, C1-C2를 제외하고 나머지 경추사이에 존재함.
- 경추의 추간판은 상대적으로 흉추, 요추보다 두꺼워(?) 큰 움직임을 허용함.
- 경추 추간판은 앞쪽면이 약간 높아서 경추의 전만을 만드는데 공헌함.
- 경추 추간판은 중앙의 수핵과 바깥면의 섬유륜으로 나뉨.
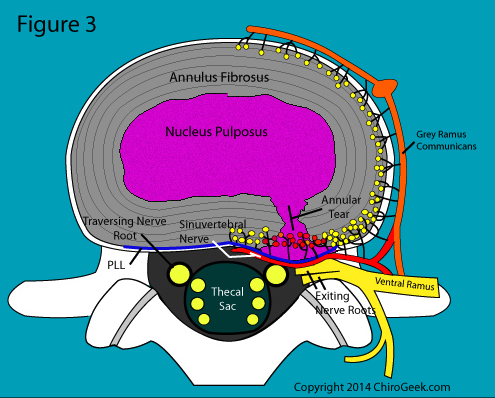
No true demarcation is found between the nucleus and the annulus, but rather a gradual change in tissue structure is seen from the inner layer to the outer ring. Because of the collagenous properties of the nucleus pulposus, which contains primarily type II collagen, it functions to resist axial compression and distributes these forces. The annulus fibrosus is composed of primarily type I collagen and functions to resist tensile forces within the disk.
- 수핵과 섬유륜사이에 분명한 경계가 없음. 하지만 조직의 점차적인 변화가 내측에서 바깥쪽으로 관찰됨.
- 수핵의 콜라겐 성분이 Type2콜라겐을 함유하기 때문에, 축성 압박에 저항하고 힘을 잘 분산함.
- 섬유륜은 type 1콜라겐으로 구성되어 디스크내의 장력에 잘 저항함.
As a person ages, the amount of proteoglycan and therefore the amount of water begin to diminish.3 The IVDs are avascular and depend on diffusion from the vertebral end plates for their nutrition. The disk is innervated along the periphery of the annulus fibrosus through the sinuvertebral nerve.4
- 나이가 들어감에 따라, 프로테오글리칸의 양과 물의 양이 점차적으로 감소함.
- 추간판은 무혈관성이므로 확산에 의해서 영양을 공급받음. 추간판의 바깥쪽 섬유륜에 동추골 신경의 지배하에 놓임.
Nerve Roots
Although there are seven cervical vertebrae, there are eight pairs of nerve roots in the cervical spine. This discrepancy is due to the fact that the first nerve root (C1) exits between the occiput and the atlas and nerves 2 through 7 also exit above the vertebrae for which they are named. The transition of the nerve root exiting below the vertebra for which it derives its name occurs at C8, and this continues throughout the thoracic and lumbar spine. Therefore, because the C5 nerve root exists above the C5 vertebra, protrusion of the C4-C5 IVD would most likely affect this nerve.
- 7개의 경추가 있고, 8개의 신경근이 있음. C0-C1에서 C1 신경근이 나오기 때문.
- 예를들어 C4-5사이에서 C5 nerve root 가 압박됨.
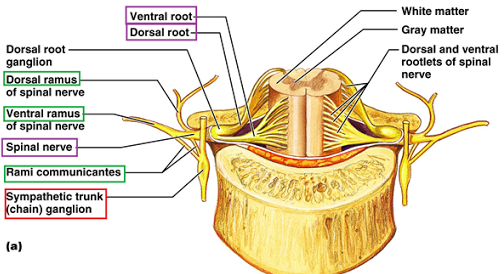
The cervical nerves differ from the lumbar nerves in that the ventral (motor) and dorsal (sensory) roots do not unite to form a mixed spinal nerve until it is in the intervertebral foramen.
- 경추 신경근은 요추신경근과는 다름.
- 경추 신경근은 ventral (motor) and dorsal (sensory) roots가 나누어져 있고, 요추는 추간 구멍에서 척추신경이 혼합되어 형성되어 있음.
Because of this anatomic relationship, cervical disk herniations would be more likely to affect the spinal cord or the ventral root, whereas nerve irritation from the facet or uncovertebral joint could encroach on either the nerve roots or the spinal nerve. The nerve roots then exit the vertebral column in the intervertebral foramen and divide into the anterior (ventral) and posterior (dorsal) primary rami.
- 이러한 해부학적 연관성 때문에 경추 추간판 탈출은 척수 또는 Ventral 신경근에 영향을 줄 수 있고, 반면에 후관절(루시카 관절)로부터 신경압박이 신경근 또는 척수에 영향을 줄 수 있음.
- 신경근은
The posterior primary rami innervate the deep erector spinae muscles and the facet joints. The anterior primary rami of C5-T1 combine to form the brachial plexus supplying the upper part of the arms.5
- post primary rami는 척추기립근 심부근육과 후관절 신경지배
- ant primary rami(C5-T1)는 상완신경총을 이룸.
Ligamentous Support
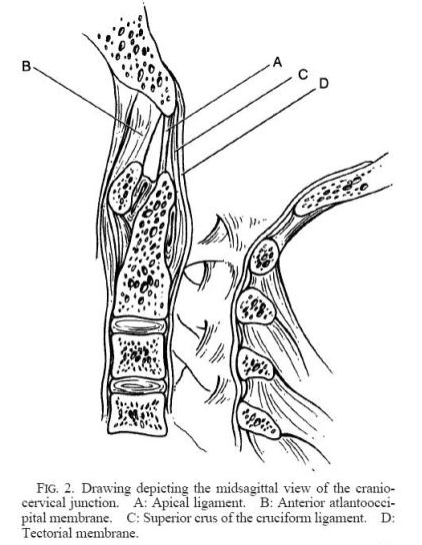
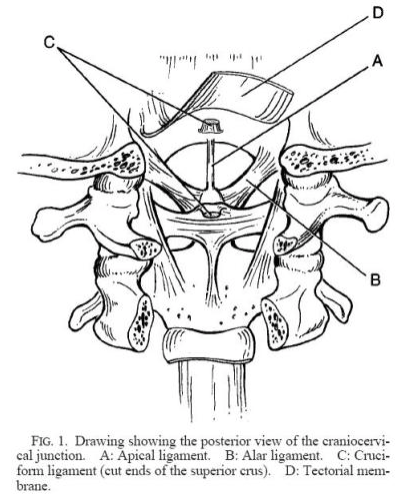
Because the upper cervical spine has sacrificed osteokinematic stability for greater arthrokinematic mobility, it is dependent on ligamentous support to allow basic function and avoid injury. Because of the unique and complex articulations present in the upper cervical region, specialized ligaments provide the needed stability. The dens is connected to the anterior rim of the foramen magnum by the apical ligament and the two obliquely oriented alar ligaments. The alar ligaments limit the amount of contralateral rotation that occurs at the atlantoaxial joint.6
- 상부경추는 Arthrokinematic 움직임을 위해 희생하는 osteokinematic 안정성을 가지기 때문에, 인대의 지지에 의존하여 기본적인 기능을 허용하고 손상을 방지함.
- 상부경추에서 독특하고 복잡한 관절면 때문에, 특별한 인대가 요구되는안정성을 제공함.
- 치돌기 상부(dens)는 foramen magnum의 전방 rim과 연결되는데, apical ligament와 두개의 사선으로 된 alar ligament가 있음.
- alar ligament는 대측 회전의 양을 제한하는 atlantoaxial joint를 만듬.
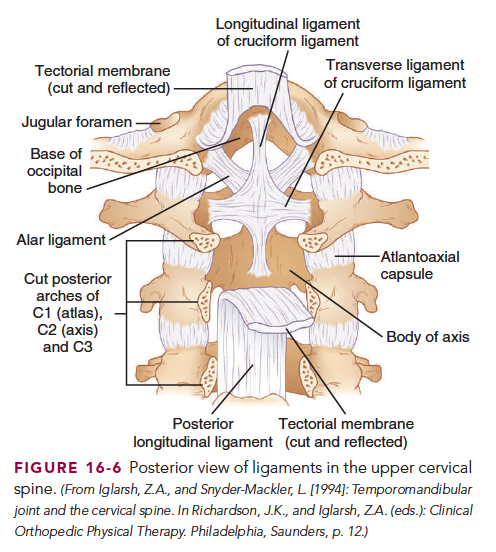
The cruciform (cruciate) ligament consists of three bands of fibers oriented in superior, inferior, and transverse directions (Fig. 16-6). The transverse band is approximately 7 to 8 mm in thickness,2 which makes it the largest and strongest of all the atlantoaxial
ligaments. The cruciform ligament functions to stabilize the dens against the posterior aspect of the anterior arch of the atlas and
to prevent subluxation into the spinal canal. Posterior to the cruciform ligaments is the tectorial membrane. It originates at the basilar occipital bone and forms the continuation of the posterior longitudinal ligament (PLL).
- 십자인대는 위, 아래, 횡방향으로 3개의 밴드를 이룸.
- 횡 밴드는 약 7-8mm 두깨이고 atalantoaxial 인대 중에서 가장 강하고, 큰 인대임.
- 십자인대는 치돌기가 척수내로 아탈구 되는 것을 방지하기 위해 안정성을 만드는 기능.
- 십자인대의 후면부위는 덮개막(tectorial membrane)으로 연결됨.
- 덮개막은 후두골의 basilar 에서 기시하여 후종인대와 연결된 구조를 만듬.
The PLL attaches to the IVD of adjacent vertebrae and their vertebral margins and functions to prevent cervical disk herniation and excessive flexion of the vertebral bodies.7 In the cervical spine the PLL is broader and thicker than in the lumbar spine. The anterior longitudinal ligament (ALL) originates from inferior surface of the basilar occiput bone and extends to the sacrum. It attaches to the vertebral bodies and IVD, but not to the bony rims.8 This ligament functions in preventing hyperextension of the vertebral bodies.
- 후종인대는 인접한 척추사이의 추간판과 부착하고, 추간판이 후방으로 탈출되는 것을 막고, 과도한 척추 굴곡을 억제함.
- 경추에서 후종인대는 요추에서보다 넓고 더 두꺼움.
- 전종인대는 basilar occiput 뼈의 아래면에서 기시하여 천골까지 아래로 연결됨. 전종인대는 척추와 추간판에 부착하지만 bony rim에는 아님. 전종인대는 과도한 신전을 억제함.
The posterior vertebral elements have specialized ligaments to provide stability. The ligamentum flavum connects adjoining laminae, and because of its attachment to the anterior aspect of the facet joint, it serves to prevent entrapment of the facet capsule and meniscus in the facet joints. The ligamentum nuchae is posterior to the ligamentum flavum and is a fibroelastic membrane that functions to limit cervical flexion. The posterior cervical ligament originates at the occiput and inserts into the spinous processes of the cervical spine before terminating at C7. It functions to resist excessive flexion and divides the posterior cervical muscles into right and left sides.
- 척추의 후방구조물은 특별한 인대가 안정성을 제공함.
- 황색인대는 인접한 laminae를 연결하고, 후관절 전면에 부착하기 때문에 그것은 후관절낭과 meniscus 포착을 방지하는데 기여함.
- 항인대는 황색인대 뒤에 존재하는 섬유탄성막(fibroelastic membrane)임. 이는 경추굴곡을 제한하는 기능.
- 후방경추인대는 후두골에서 시작하여 경추 극돌기로 이어져 C7에서 끝남. 그것은 과도한 굴곡을 방지하고 경추 후방의 근육을 좌우로 나누는 역할을 함.
Muscular Arrangement
The cervical spine has numerous muscles that have an influence on proprioceptive input and postural control and provide active
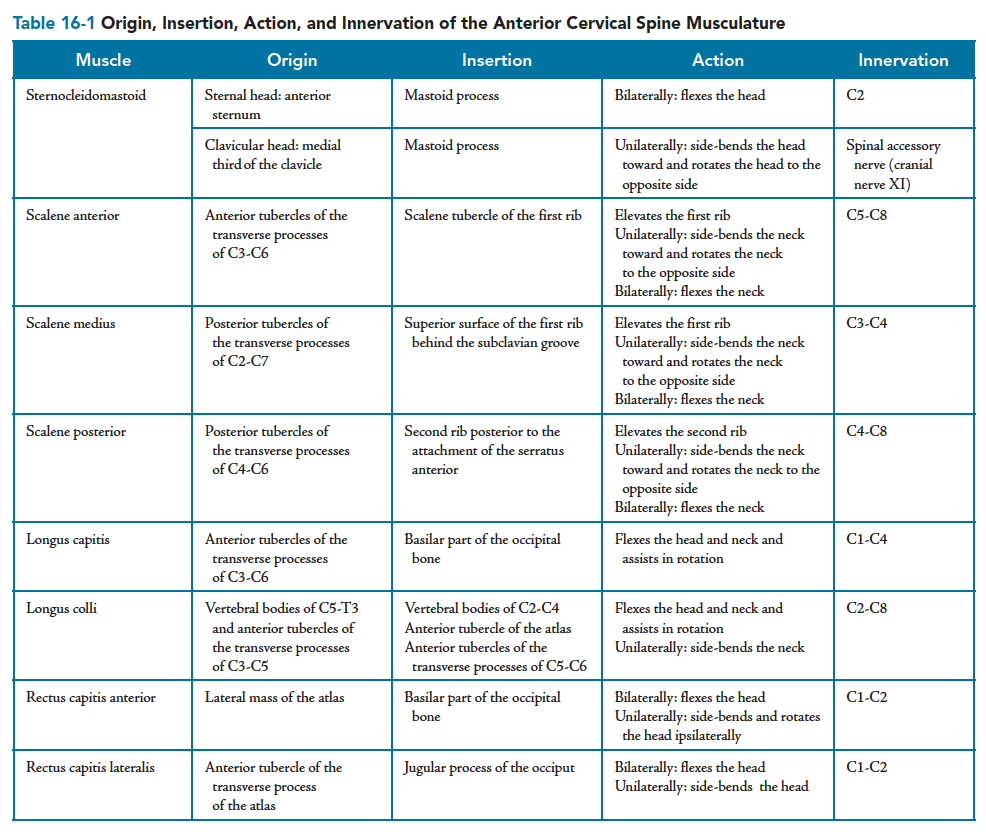
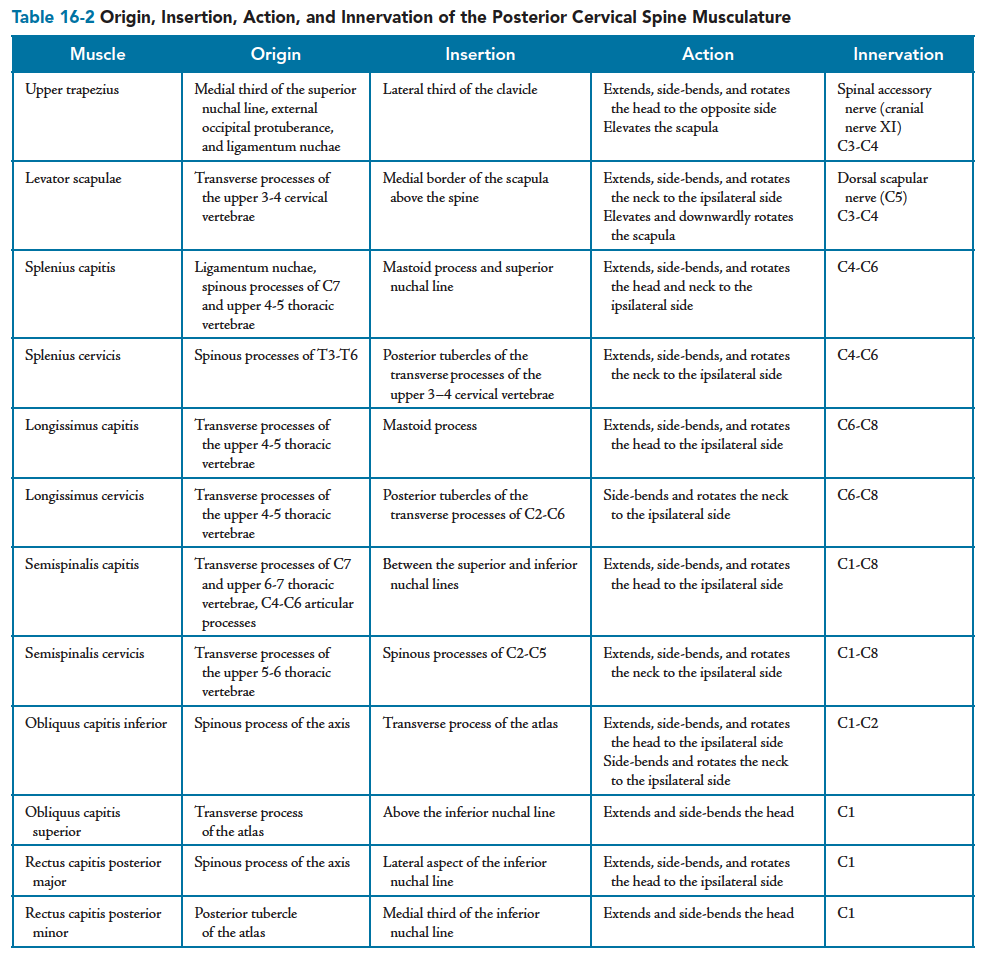
movements for the occiput, cervical spine, and upper part of the trunk. These muscles can be divided into anterior and posterior groups according to their attachment in relation to the transverse processes. Tables 16-1 and 16-2 list these muscles, including their origin, insertion, action, and innervation.
- 경추는 고유수용감각 input에 영향을 주는 많은 근육과 자세를 유지하는 근육을 가짐. 그래서 상부몸통과 경추, 두부의 능동적 움직임을 담당함.
- 이러한 근육은 횡돌기를 기준으로 앞, 뒤 근육으로 나뉨.
경추의 전방 주요 근육
- 흉쇄유돌근, 사각근 전중후방 섬유, longus colli, longus capitus, rectus capitus anterior and lateralis
경추의 후방 주요근육
- 상부승모근, 견갑거근, splenius capitus, longissimus capitis and cervicis, semispinalis capitis and cervicis, oblique capitis inferior and superior, rectus capitis posterior major and minor
경추 생체역학
Biomechanics
The forces and stresses that are controlled and generated by the body ensure the proper histologic, biomechanical,
and physiologic properties of each tissue. “Structure governs function and function dictates structure.”
—Rob Tillman, PT, MOMT
- 인체에 의해서 생성되고 조절되는 힘과 stress는 각 조직의 적절한 조직학, 생역학, 생리적 특성을 확실하게 함.
- 구조는 기능을 지배하고, 기능은 구조를 결정함.
Osteokinematic motion in the cervical spine is a result of interaction of the cervical vertebrae, IVDs, ligaments, joint capsules, and the orientation of the facet joints working together to control and dictate the movements that occur in this region. Active ROM is a result of the interaction of the entire cervical spine to produce a desired movement. However, because of anatomic differences between the upper cervical and midcervical spine, the upper cervical spine is able to perform motions independent of those of the mid-cervical region.
- 경추에서 뼈운동학적 움직임은 경추 척추, 추간판, 인대, 관절낭, 후관절의 방향이 함께 작용하여 경추의 움직임을 조절하고 결정하는 결과임.
- 능동적 ROM은 전체 경추의 상호작용이 원하는 움직임을 생성하는 결과임.
- 하지만 상부경추와 중부경추의 해부학적 구조차이 때문에, 상부경추는 중부경추의 독립적인 움직임을 가능케 함.
This allows the cervical spine to correctly position the head for optimal orientation of the visual, auditory, and olfactory nervous systems. The arthrokinematic motions of the upper cervical spine are discussed in detail because of the complex articulations in this region.
- 이는 경추가 올바른 방향을 위한 시각, 청각, 후각 신경시스템을 위한 머리의 위치를 허용함.
- 상부경추의 관절운동학적 움직임은 복잡한 관절때문에 자세하게 논의됨.
Notably, the desired motion occurs as a result of these actions occurring in unison. The following processes described are a teaching tool that is meant to promote biomechanical understanding of what occurs, although functionally these movements are occurring together and in synchrony. Because normal variations occur in osseous and connective tissue properties and orientation, structural discrepancies can exist and produce altered arthrokinematic movements.
- 분명하게, 올바른 움직임은 이러한 작용이 조화롭게 일어난 결과임.
- 뼈와 결합조직에서 정상적인 변이때문에 구조적 차이는 존재할 수 있고, 변형된 관절운동학적 움직임을 생성함.
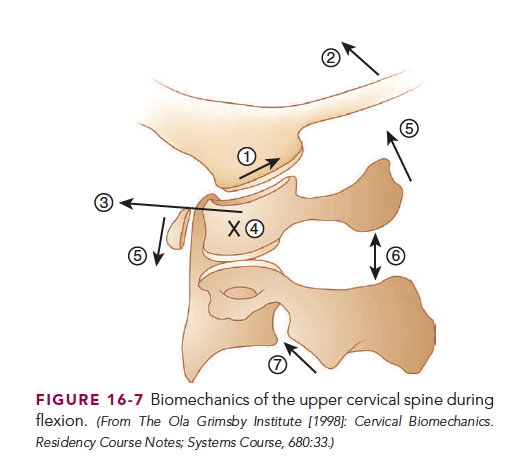
During flexion of the upper cervical spine (Fig. 16-7 ),
(1 ) the convex condyles of the occiput glide in a posterior direction on the concave facets of the atlas, which produces
(2 ) an anterior tilt of the occiput.
(3 ) The atlas is pushed approximately 2 to 3 mm in an anterior direction because of the force created in the facet joints. This translation creates approximation between the dens and the transverse ligament, which restricts further motion.
(4 ) The atlas tilts 15° to 20° anteriorly,
(5 ) thus causing its anterior arch to move inferiorly 2 to 4 mm as the posterior arch is elevated.
(6 ) The superior tilt of the posterior arch increases tension on the posterior ligamentous structures between C1 and C2.
(7 ) The increased tension causes movement between C2 and C3.9
고개를 끄덕이는 굴곡동안
1) Occiput의 볼록한 condyle은 환추의 오목한 면(facet)에서 후방으로 활주함.
2) 이는 occiput의 전방 기울어짐을 야기함.
3) 환추는 대략 2-3mm 앞방향으로 밀림. 왜냐하면 facet joint에서 힘이 생성되기 때문. 이러한 이동은 치돌기와 횡인대의 인접을 야기함.
4) 환추는 15-20도 전방으로 기울어짐
5) 환추의 전방아치가 아래로 2-4mm이동하면서 후방아치가 상승함.
6) 후방아치의 상방 기울어짐은 C1-2사이의 후종인대구조에 장력을 증가시킴.
7) 증가된 장력은 C2-3사이의 움직임을 야기함.
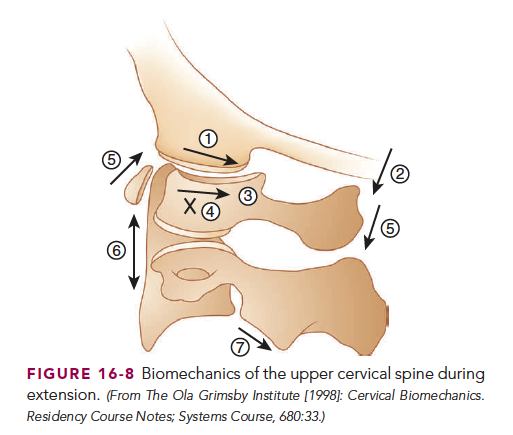
Extension of the upper cervical spine (Fig. 16-8 ) occurs as a result of
(1 ) the convex occipital condyles gliding forward on the concave facet joints of the atlas, which produces
(2 ) a posterior tilt of the occiput.
(3 ) The compressive forces cause the atlas to translate 2 to 3 mm posteriorly, and such translation is restrained by the anterior arch of the atlas approximating against the odontoid process.
(4 ) The atlas tilts posteriorly approximately 12°, which causes
(5 ) its anterior arch to translate 2 to 4 mm superiorly on the dens as the posterior arch moves inferiorly.
(6 ) As the anterior ligamentous structures become taut,
(7 ) the axis glides posteriorly on C3.9
상부경추 신전동안 일어나는 일
1) 볼록한 Occipital condyle은 환추의 오목한 facet joint에서 전방으로 활주함
2) 그 결과 occiput는 후방으로 기울어짐
3) 압박 힘은 환추가 후방으로 2-3mm이동하게 하여, 이러한 이동은 치돌기에 가까워진 환추의 전반아치에 의해서 제한됨.
4) 환추는 후방으로 대략 12도 기울어짐.
5) 그 결과 환추의 전방아치는 2-4mm위로 이동하여 ...
6) 전종인대구조는 taut해짐
7) 축추는 C3 에서 후방으로 활주함.
상부경추 측굴시 일어나는 일
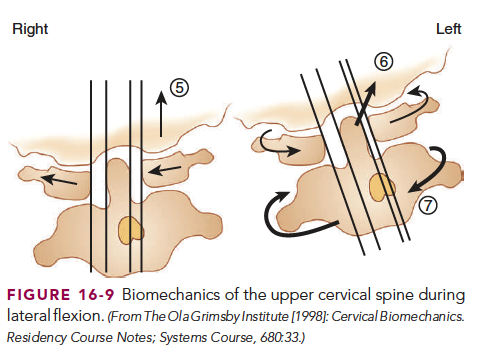
Right lateral flexion of the upper cervical spine (Fig. 16-9 )is produced as the convex condyles of the occiput glide 3° to 5° to the left, which causes a relative right translation of the atlas. This translation is prevented as the dens approximates against the lateral mass of the atlas. Lateral flexion between C1 and C2 does not occur because of the approximation between the odontoid process and the atlas and their biconvex articulating surfaces. Because of the lateral forces exerted by the occiput and atlas, the axis side-bends 5° to the right on C3 as a result of the inability of C1 to glide laterally on C2. The atlas will then rotate immediately to the left on the axis to maintain an anterior orientation of the face. (5 ) The left occipital condyle elevates as a result of the wedge-shaped lateral masses of the atlas gliding to the right. This elevation causes tension in the left alar ligament, which (6 ) produces compression between C2 and C1 as the axis is elevated. (7 ) The joint compression between the biconvex surfaces of both the atlas and the axis produces a right
rotation of the axis. As lateral flexion is increased, the occiput and atlas will rotate to the left on the axis to allow anterior orientation
of the face.9
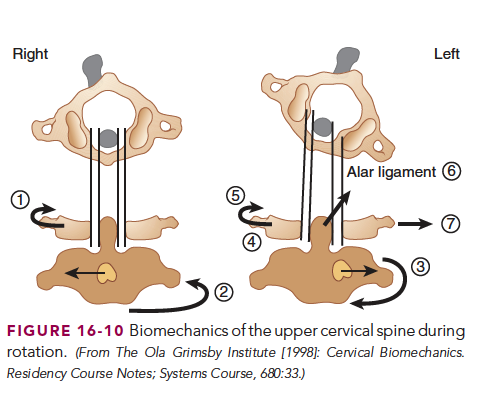
Rotation of the upper cervical spine (Fig. 16-10 ) to the right begins with
(1 ) the occiput rotating on the atlas a minute amount (approximately 1°). As joint approximation occurs, the atlas is pulled into right rotation, thereby bringing the left lateral mass of C1 closer to the dens.
(2 ) The compressive forces that occur between the atlas and the axis produce 2° to 3° of left rotation of C2 as a result of the biconvex surfaces.
(3 ) The occiput and atlas rotate to the right approximately 40° and apply tension on the left alar ligament, which brings the axis into right rotation.
(4 ) The axis will continue to rotate and side-bend to the right approximately 10°,
(5 ) which allows the occiput and atlas to rotate to the available end ROM.
(6 ) The increased tension on the left alar ligament produces left side bending of the occiput.
(7 ) The atlas is forced to glide to the left because of the compressive forces of the left occipital condyle. As the atlas side glides to the left, the amount of left side bending of the occiput is increased as the wedge-shaped lateral masses of the atlas tilt the occiput.9
In the midcervical spine, the superior facets are oriented in a superior, posterior, and medial direction, whereas the inferior facets are oriented in an anterior, inferior, and lateral direction. As a result, during cervical rotation the contralateral inferior facet glides
in a superior and medial direction, which produces lateral flexion in the same direction. Therefore, in the cervical region, rotation
and lateral flexion always occur together in the same direction.
During flexion, the superior vertebral body slides and tilts anteriorly on the inferior vertebra, which causes separation of the facet joints. During extension, the superior vertebral body slides and tilts posteriorly. This motion is limited because of joint approximation and tension in the ALL. The facet joints are oriented to allow an increase in the amount of flexion and extension.