몇가지 자료를 조합해야 ..
palpation technique
인터넷 최신자료
panic bird...
Shoulder Complex Significance and Function of the Shoulder Region
This section examines biomechanical and functional factors in the shoulder complex.
The shoulder complex is one of the largest movement complexes in the musculoskeletal system. It includes:
• The shoulder joint (glenohumeral or GH joint).
• The bony parts and joints in the shoulder girdle.
• The cervicothoracic junction and the superior costal joints.
• The muscles, vessels, and nerves supplying this area.
- 여기서는 어깨복합체의 생체역학적, 기능적 요소에 대한 탐구를 진행
- 어깨복합체는 인체 근골격계 시스템에서 가장 크게 움직이는 복합체 구조물중의 하나임.
- 어깨관절, 견갑대에서 뼈와 관절, 경흉추연결 그리고 상늑골관절. 근육, 혈관, 신경의 지배에 대하여 탐구함.
The arm must be able to move over the largest range of motion. The most important principle of function of the shoulder complex is to provide a mobile and stable base for the arm movements. Apart from the mechanics of locomotion, end range elevation of the shoulder is the most complex movement of the body.
- 팔은 가장 큰 운동범위를 넘어서 움직여야 함. 어깨의 가장 중요한 기능원리는 팔움직임을 위해 안정성과 운동성을 동시에 제공해야 함.
- 이동하는 기계와 별도로 어깨의 끝범위 들기는 인체의 가장 복잡한 움직임임.
The intricate interplay between the individual components of the shoulder complex allows a variety of dysfunctions. The cause of restricted shoulder elevation can be found in every single mobile articulation in the cervicobrachial region. A comparatively large number of causes for shoulder/arm pain exists. Pain may be referred or projected from the cervical spine and the thoracic outlet, or may be due to several other possible causes ranging from arthritis to lesions in the soft tissue. When presented with a "shoulder patient," therapists are often compelled to thoroughly assess all components of the shoulder complex and frequently find it quite difficult to interpret results.
- 어깨복합체의 개별적 구조물의 복잡한 상호작용은 기능부전의 다양성을 허용함.
- 제한된 어깨 상승의 원인은 경완부위에서 움직이는 관절에서 발견될 수 있음.
- 어깨와 팔통증을 위한 많은 원인이 존재함. 통증은 경추에서 팔로 전이될 수 있고 방사될 수 있음. 또는 연부조직의 관절에서 염증이 일어날 수도 있음.
- 어깨환자가 있을때 치료사는 어깨복합체의 모든 요소를 측정하고 자주 그 결과를 완전히 해석하지 못할만큼 어려움.
Common Applications for Treatment in this Region
Techniques used in this region that require knowledge of palpation include:
• Joint play tests and manual therapy techniques (e.g., glenohumeral, acromioclavicular, and sternoclavicular).
• Local cross-frictions according to Cyriax, for example, at the site of insertion for the rotator cuff muscles.
• Local application of electrotherapy and thermotherapy on the muscles and articular structures.
- 관절가동과 수기치료 테크닉(어깨관절, AC, SC joint)
- 시리악스의 국소적 교차마찰마사지(특히 회전근개 부착부)
- 전기치료와 열치료의 국소적 적용.
Required Basic Anatomical and Biomechanical Knowledge
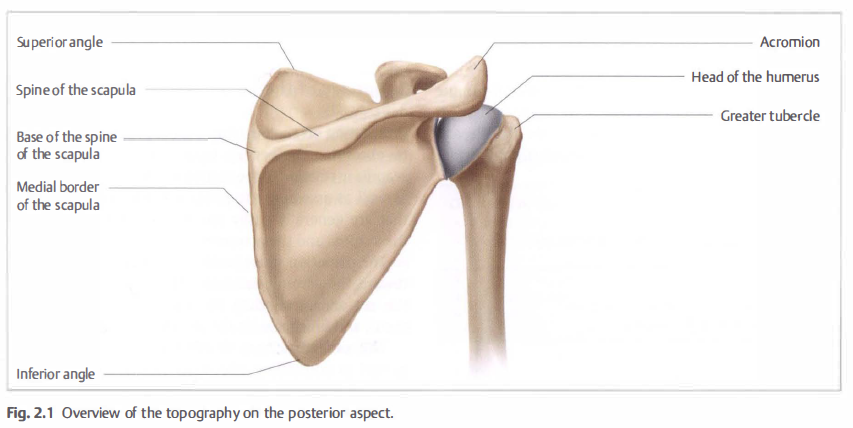
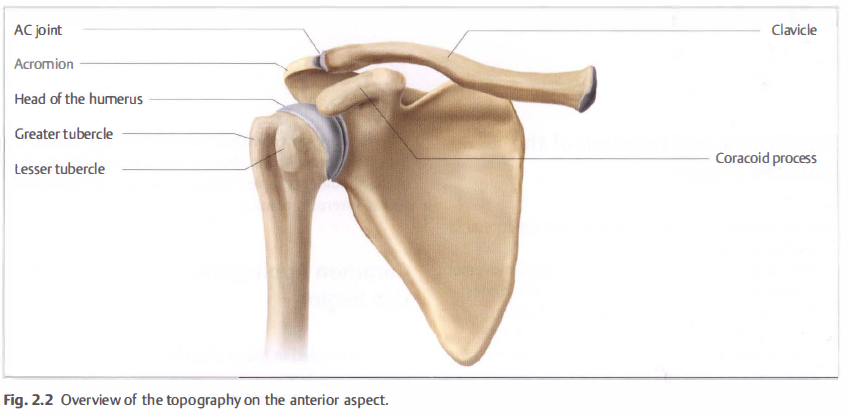
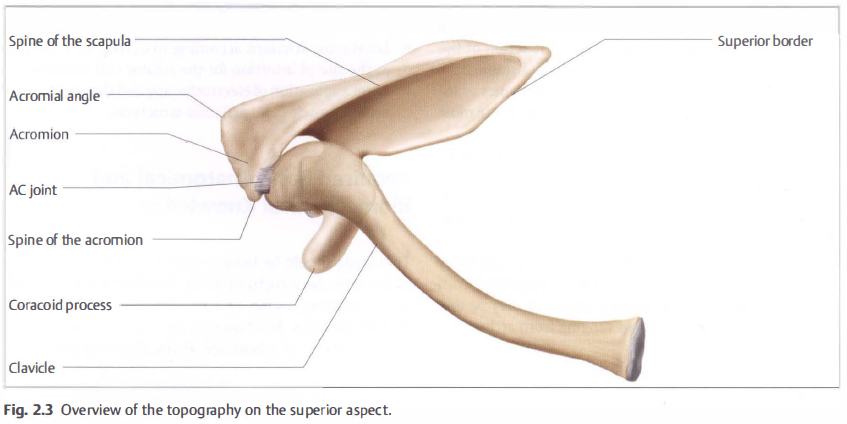
Therapists should be familiar with the location and form of the articular structures in all "shoulder joints," as well as the location, course, and attachments of clinically important muscles, for example, the supraspinatus. Good spatial sense is of advantage as the clinically important structures are found close to each other, especially in the GH joint. Knowledge of the shape of the spine of the scapula and the acromion, the dimensions of the clavicle, and the position of the joint spaces is especially important (Figs. 2.1, 2.2, 2.3).
- 치료사는 모든 어깨관절에서 관절구조의 형태와 위치에 대해 알아야 함. 또한 예를들어 극상근 근육의 부착부 등에 대해서도 잘 알아야 함.
- 어깨관절의 구조를 잘 알고, 견봉, 쇄골의 수치, 관절강의 위치 등이 특히 중요함.
Key Points
The shoulder complex is composed of three bones—the clavicle, the scapula, and the humerus—as well as four articulations—the acromioclavicular (AC), the sternoclavicular (SC), the scapulothoracic, and the glenohumeral (GH) joints.
어깨복합체는 3개의 뼈(쇄골, 견갑골, 상완골)로 구성되고 4개의 관절(AC, SC, Scapulothoracic, and GH joint)를 이룸.
The clavicle serves a variety of functions. It acts as a rigid base for muscular attachments of the shoulder, neck, and chest. It also provides protection for the major vessels at the base of the neck and for the nerves and vessels supplying the upper limb. In addition, it forms a strut that holds the GH joint in the parasagittal plane.
쇄골은 다양한 기능을 제공함. 어깨, 경부, 가슴의 근육부착부를 위한 단단한 기초를 제공하는 역할. 쇄골은 큰 혈관과 신경을 보호함. 게다가 어깨관절을 고정하는 버팀목 역할
The scapula is a flat, triangular-shaped bone that serves as the articulating surface for the head of the humerus as well as provides areas for 17 muscle attachments.
견갑골은 편평하고, 삼각형의 뼈로 상완골두를 위한 관절면을 제공하고, 17개의 근육이 부착함.
The proximal humerus is composed of the humeral head, the lesser and greater tuberosities, the bicipital groove, and the proximal humeral shaft.
상완골은 상완골두, 대소결절, 상완이두근구, shaft로 구성됨
The AC joint is a diarthrodial joint and the only articulation between the clavicle and the scapula. The motion of the AC joint is minimal, involving small translations and, mainly, rotation between the clavicle and the acromion with arm movement.
견쇄관절은 운동성 관절이고, 쇄골과 견갑골이 만나는 관절. 견쇄관절의 움직임은 적음. small translation, 쇄골과 견봉의 회전..
The scapulothoracic articulation is not a true joint, but it represents the space between the concave surface of the anterior scapula and the convex surface of the posterior chest wall. The muscular and ligamentous attachments provide the stability of this articulation as the scapula retracts, protracts, and rotates along the posterior chest wall.
견흉관절은 진짜관절이 아님. 하지만 convex한 늑골과 concave한 견갑골이 만나 관절면을 이룸. 근육과 인대부착이 이 관절이 전인, 후인, 회전, 상승 등의 움직임동안 안정성을 제공함.
The GH joint is a diarthrodial joint with minimal bony constraint, allowing it the largest range of motion of any major diarthrodial joint in the body.
어깨관절은 움직이는 관절로 최소한의 뼈제한 요소를 가지고 인체에서 가장 큰 움직임을 만듬.
The glenoid labrum provides another static restraint to GH motion. The labrum is a fibrous ring that is attached to the glenoid articular surface through a fibrocartilagenous transition zone.
어깨 관절순은 gh 움직임의 정적제한을 제공함. 관절순은 섬유성링으로 섬유관절을 통해 관절면을 만듬.
The rotator cuff (RTC) muscles, as well as the scapular rotators, contribute to GH stability by enhancing the concavity–compression mechanism. Contraction of the long head of the biceps tendon, coordinated scapulothoracic rhythm, and proprioceptive mechanoreceptors in the joint capsule also contribute to the stability.
회전근개 근육은 concavity-compression 기전을 증진시켜 GH 안정성에 공헌함. 상완이두근 장두의 수축와 조화로운 견흉리듬 그리고 고유수용기가 역할을 하여 안정성에 공헌함.
The RTC is composed of the supraspinatus, the infraspinatus, the subscapularis, and the teres minor muscles. The RTC often serves more than one function simultaneously. The muscles act as prime movers if the line of action is within the intended direction of motion.
회전근개은 극상근, 극하근, 견갑하근, 소원근으로 이루어짐. 회전근개는 때로 하나의 기능을 넘어섬.
Nerve injuries can occur with both arthroscopic and open shoulder procedures.
RTC repair using an open technique has been clinically successful in terms of repair, although arthroscopic techniques are now more common.
신경손상은 관절경 수술과 오픈 수술을 하다가 발생할 수 있음. 회전근개 회복은 ...
The shoulder is a complex joint that has the greatest degree of mobility of all major joints in the human body. The osseous and ligamentous structures that comprise the joint, as well as the surrounding musculature, interact to provide a wide range of motion as well as stability. Under normal conditions, four articulations move in synchrony, allowing smooth, unhindered motion of the arm. The control of
glenohumeral (GH) stability is achieved by the complex interaction between the static restraints (i.e., the ligament and tendons) and the dynamic restraints (i.e., muscular contraction acting across the joint).

Osseous Structures and Static Restraints
The shoulder complex is composed of three bones—the clavicle, the scapula, and the humerus—as well as four articulations—the acromioclavicular (AC), the sternoclavicular (SC), the scapulothoracic, and the GH joints
(Fig 10-1).
Clavicle
The clavicle, an “S”-shaped bone, is the only long bone that ossifies by an intramembranous process. It is the first bone in the body to ossify (fifth week of fetal gestation) and is the last bone to fuse (medial epiphysis at 25 years of age). The clavicle consists of cancellous bone surrounded by an outer layer of compact bone, and it is unique in that it does not have a medullary cavity (
1,
2).
The clavicle serves a variety of functions. First, it acts as a rigid base for muscular attachments of the shoulder, neck, and chest. It also provides protection for the major vessels at the base of the neck and for the nerves and vessels supplying the upper limb. In addition, it forms a strut that holds the GH joint in the parasagittal plane, increasing the range of motion of the shoulder as well as the power of the arm in motions above the horizontal (
1).
The clavicle articulates with the manubrium of the sternum through the SC joint and with the acromion at the AC joint. It is attached to the coracoid by the coracoclavicular ligaments, the conoid medially and the trapezoid laterally.
Scapula
The scapula is a flat, triangular-shaped bone that serves as the articulating surface for the head of the humerus as well as provides areas for 17 muscle attachments. With the arm at the side, the scapula overlaps the dorsal surfaces of the second to seventh ribs. It has three prominent projections: the spine, the coracoid process, and the acromion. The scapular spine divides the posterior aspect of the scapula into two depressions, the supraspinatus fossa and the infraspinatus fossa. In addition, the spine serves as a site for insertion of the trapezius muscle and as the origin for the posterior third of the deltoid muscle (
2,
3).
The coracoid process is a hooklike projection that curves anteriorly, upward, and outward in front of the glenoid cavity. The base of the coracoid is the attachment site of the coracoclavicular ligaments. The tip serves as the origin of the short head of the biceps and the coracobrachialis muscles and as the insertion site of the pectoralis minor muscle. The coracoid also serves as the anterior limit of the coracoacromial arch and is a palpable landmark during rotator cuff (RTC) surgery (
2,
3).
The acromion serves as an attachment site for the trapezius muscle above and the deltoid muscle below, and it articulates with the distal clavicle. The acromion usually forms from two or three ossification centers that appear during puberty and that fuse between 18 and 25 years of age. These three ossification centers are described as the preacromion, the mesoacromion, and the meta-acromion. The os acromiale, an unfused secondary ossification, occurs with an incidence of 1% to 15%, and 60% of cases involve bilaterality (
4,
5,
6,
7). The most common location is at the junction of the meso- and meta-acromion (
4,
7). An os acromiale can be identified on an axillary radiograph or magnetic resonance image (MRI) and should not be mistaken for a fracture.
In addition, the acromion has been classified into three morphologic patterns as viewed on a scapular outlet radiograph: flat (Type I), curved (Type II), and hooked (Type III) (
8). A Type III morphology has been implicated in impingement and RTC pathology (
9,
10). Investigators have further classified the acromion based on thickness: Type A, <8 mm; Type B, 8–12 mm; and Type C, >12 mm (
11).
Differences in the size of the acromion have been observed between men and women. Nicholson et al. (
7) observed in men that the average length was 48.5 mm, the average anterior width was 19.5 mm, and the average anterior thickness was 7.7 mm. In women, the acromial length averaged 40.6 mm, the anterior width averaged 18.4 mm, and the
anterior thickness averaged 6.7 mm (
7). That study also determined that basic acromial morphology is a primary anatomical characteristic independent of age and, in contrast, that anterior acromial spurs were dependent on age, because they were present in only 7% of patients <50 years and in 30% of patients >50 years.
The acromion contributes to the coracoacromial arch, or supraspinatus outlet, which consists of the coracoid process, the acromion, and the coracoacromial ligament. This arch marks the superior boundary of the subacromial space. Interest has been focused on the structure and function of the coracoclavicular ligament and the importance of the coracoacromial arch (
12,
13,
14,
15). Although commonly described as having a “Y”-shaped configuration, other morphological types of the coracoclavicular ligament have been described (
13,
14,
15,
16). Soslowsky et al. (
15) identified four types: quadrangular (48%); “Y”-shaped, with a broader lateral band and thinner medial band (42%); broad banded (8%); and with multiple bands (2%). The length of the coracoid attachment averaged 32 mm and the length of the acromial attachment averaged 19 mm. The average midpoint thickness was 1.3 mm. The length of the lateral band was significantly shorter, and the cross-sectional area was significantly larger, in specimens with a tear in the RTC (
15).
The role of the coracoacromial arch as a secondary restraint to anterosuperior migration of the humeral head also has become of interest (
17,
18,
19). The coracoacromial ligament has been shown to provide a static restraint to the GH joint as well as significantly contributing to anterior GH stability at 30 degrees of abduction (
20,
21). Release of the coracoacromial ligament has been suggested to increase both anterior and superior translation of the humeral head. It is important to maintain the integrity of the coracoacromial arch in the cuff-deficient shoulder, because the arch is the last restraint to anterosuperior migration (
12,
20,
22).
The scapula also gives rise to the glenoid cavity, which is situated laterally, below the acromion. This lateral thickening of the scapula provides the bony articulation with the humeral head. The articular surface of the glenoid is concave and covered with hyaline cartilage, which is thinner in the center and thicker toward the periphery. A bare spot exists in the center of the inferior glenoid, which is equidistant to the anterior, posterior, and inferior glenoid rim when viewed with an arthroscope (
23,
24).
Glenoid version has been examined in several studies (
25,
26,
27,
28). In most, the glenoid displayed from 2 to 10 degrees of retroversion in relation to the long axis of the scapula, with an average of superior tilt of 5 degrees (
26,
27,
28,
29,
30,
31). In a study measuring the glenoid version in relation to the supraspinatus fossa, 40% were retroverted, 38% neutral, and 22% anteverted (
32).
In addition, the shape of glenoid also changes from superior to inferior (
28,
33,
34,
35,
36). Inui et al. (
34,
37) have shown that the superior part of glenoid surface is retroverted and that the inferior portion may be anteverted. In an MRI study of 40 subjects, Inui et al. (
34) showed the upper aspect has a large radius of curvature, is convex, and subsequently, becomes flat and then concave in the lower portion with a small radius of curvature.
The shape of the glenoid resembles a pear, being 20% narrower superiorly than inferiorly (
23,
26,
38). The reported average vertical diameter ranges from 33 to 39 mm (
24,
26,
30,
35) and the average transverse diameter from 23 to 29 mm (
24,
26,
30,
35,
39). The distance from the anteroinferior margin of the glenoid to the bare area averages 12.8 mm (
23,
24).
The articular surface of the glenoid is one-third to one-fourth the area of the articular surface of the humeral head, whereas the radius of curvature of the glenoid is 2.3 mm greater than the radius of curvature of the humeral head (
26,
27,
35,
39).
Humerus
The proximal humerus is composed of the humeral head, the lesser and greater tuberosities, the bicipital groove, and the proximal humeral shaft, and it is highly variable. The anatomical neck lies at the junction of the articular surface of the head and the greater tuberosity and humeral shaft. The surgical neck lies below the greater and lesser tuberosities. The major blood supply to the humeral head is through the ascending branch of the anterior humeral circumflex artery, which penetrates the head at the bicipital groove and becomes the arcuate artery. This artery crosses under the tendon of the long head of the biceps, runs proximally just adjacent to the lateral aspect of the bicipital groove, and enters the humeral head at the proximal end of transition from the greater tuberosity to the bicipital groove. The posterior circumflex artery supplies the posterior portion of the greater tuberosity and a small posteroinferior part of the humeral head (
2,
3).
The bicipital groove lies on the anterior proximal humerus, just below the articular surface, and it is defined by the greater and lesser tuberosities. The long head of the biceps tendon lies in this groove and is covered by the transverse humeral ligament.
Both the greater and lesser tuberosities provide attachment for the RTC tendons. The supraspinatus, infraspinatus, and teres minor insert on the greater tuberosity from superior to posterior.
The subscapularis tendon attaches to the lesser tuberosity, also overlying the bicipital groove, and provides additional support to the long head of the biceps tendon (
2,
3).
Multiple studies have been performed to determine the head–neck ratio, the central axis of the humerus, and the anatomical relationships of the greater tuberosity and the bicipital groove assist in prosthetic replacement and design (
22,
26,
40,
41). The articular surface of the humeral head has an average radius of from 42 to 46 mm, whereas the average thickness of the humeral head is 19 mm. The thickness of the humeral head is proportional to both the length of the humerus and the head radius (
41,
42). The humeral head is retroverted from -6.5 to 35 degrees relative to the
transepicondylar axis of the distal humerus (
31,
40,
41). The angle formed by the neck and shaft axes varies from 114 to 147 degrees (
28,
42,
43). No significant differences between genders have been reported; however, a difference in the retroversion angle has been found between dominant and nondominant sides, with a measure of 33 degrees on the dominant side and 29 degrees on the nondominant side (
22).
The humeral head center is offset from the humeral axis by 7 mm medial and 2 mm posterior. A predictable relationship has been found between the central axis of the humeral head and the bicipital groove. In an evaluation of 18 cadavers, the average distance between the central axis of the humeral head and biceps tendon was 9 mm posterior to the posterior margin of the bicipital groove (
44). The superior aspect of the humeral head is 6 mm higher than the superior aspect of the greater tuberosity (
40). Iannotti et al. (
26) reported that the mean distance between the greater tuberosity and the humeral head was 10 mm or less and that this distance was not correlated with other parameters. Takase et al. (
45), however, found a significant correlation between the size of the humeral head and the neck shaft angle regardless of gender or age.
The bicipital groove rotates internally along its course between the upper and lower aspects of the proximal humerus. The mean change in rotation of the lateral lip from the proximal to distal groove was 15.9 degrees (
40,
46). Rotation of the bicipital groove in the proximal-to-distal direction is relevant to shoulder fracture work, particularly fracture arthroplasty, because the groove can assist with proper orientation of humeral head version.
Acromioclavicular Joint
The AC joint is a diarthrodial joint and the only articulation between the clavicle and scapula. Variable inclinations exist, with being nearly vertical to angled downward and medially accounting for up to 50 degrees (
2,
3). The AC joint has an incomplete fibrocartilagenous intra-articular disc, potentially predisposing it to degenerative changes.
Degenerative changes have been shown to occur as early as the second decade of life, with loss of articular cartilage, eburnation of subchondral bone, and formation of marginal osteophytes; however, these changes do not necessarily produce symptoms (
47).
The motion of a normal AC joint is minimal, involving small translations and, mainly, rotation between the clavicle and the acromion with arm movement. The AC ligaments prevent anteroposterior instability
(Fig 10-2). Biomechanical studies have shown that the inferior AC capsular ligaments represent the major restraint against anterior joint translations, whereas the superior and posterior ligaments provide the most stability against posterior translations (56% and 25%, respectively) (
48,
49). Therefore, the posterior and superior capsular ligaments should be spared during distal clavicle excision to prevent excessive posterior clavicle translations after resection (
49,
50). The coracoclavicular ligaments (the trapezoid and the conoid) together resist superior displacement of the joint, but with larger amounts of displacement and induced loads, the conoid ligament contributes the major share (
48,
49).
Sternoclavicular Joint
The SC joint is the only true joint that connects the upper extremity to the axial skeleton. It is a gliding joint with little inherent bony stability. Substantial incongruity exists between the two articular surfaces, but the interposition of an intra-articular disc compensates for this (
2,
3). This disc has not shown severe degenerative alterations until the seventh decade of life, but even then, the joint seems to be well preserved (
47).
The SC joint is enveloped in a loose, fibrous capsule that blends with the margin of the disc (
47). The stability of the joint, which is provided mainly by the surrounding ligaments, protects the important underlying vasculature, pleural domes, trachea, and esophagus. The SC ligaments consist of the anterior and posterior SC and capsular ligaments, the interclavicular ligaments, and the anterior and posterior costoclavicular ligaments (
47,
51). These allow motion in all planes, including rotation. The SC ligaments prevent upward displacement of the medial clavicle caused by downward forces on the lateral end of the clavicle. The posterior capsular ligament is the most important stabilizer (
51). These ligaments allow the clavicle to move 30 degrees upward, 30 degrees in an anteroposterior direction, and rotate 45 degrees about its long axis (
47,
51).
Scapulothoracic Articulation
The scapulothoracic articulation is not a true joint; rather, it represents the space between the concave surface of the anterior scapula and the convex surface of the posterior chest wall. The muscular and ligamentous attachments provide the stability of this articulation as the scapula retracts, protracts, and rotates along the posterior chest wall (
2,
3).
Williams et al. (
52) divided the anatomical structures of this articulation into three layers: superficial, intermediate, and deep. The trapezius and latissimus dorsi muscles and an inconsistent bursa between the latissimus and inferior angle of the scapula comprise the superficial layer. The intermediate layer is composed of the rhomboid major and the rhomboid minor, the levator scapulae muscles, and the spinal accessory nerve and bursa between the superomedial scapula and trapezius muscle. The spinal accessory nerve travels closely along this bursa at an average of 2.7 cm lateral to the superomedial scapular angle. Finally, the deep layer consists of the serratus anterior and subscapularis muscles and the corresponding scapulothoracic and subscapularis bursa (
52,
53).
Glenohumeral Joint
The GH joint is a diarthrodial joint with minimal bony constraint, allowing it the largest range of motion of any major diarthrodial joint in the body (
2,
3,
31,
54). The GH joint has been described as being similar to a golf ball on a tee, with a large humeral head balanced on a smaller glenoid. The GH joint approximates ball-and-socket kinematics, with only one-third of the humeral head being covered by the glenoid in any position of rotation, and the articular surface of the humeral head is threefold that of the glenoid (
2,
43,
55).
In most shoulders, the glenoid and humerus have similar radii of curvature, providing a basically congruent articulation with less than 2 mm of mismatch between the glenoid and the humeral head. This matched concavity–convexity of the articulation provides stability when muscle forces act across the joint. This provides the foundation for the RTC musculature to establish a concavity–compression effect (
33,
54,
55,
56,
57).
The combined version of the glenoid and humeral head results in a retroversion of approximately 30 to 40 degrees (
2,
28,
31,
57). In normal shoulders, the center of the humeral head is usually within 1 mm of the plane of the scapular spine (
58). The spherical humeral articular surface articulates with the spherical concavity of the glenoid, whereas the proximal humeral convexity articulates with the spherical concavity of the coracoacromial arch (
55).
A negative intra-articular pressure exists within the GH joint, creating a vacuumlike effect. The joint acts as a closed compartment with a flexible diaphragm. The weight of the arm tends to pull the joint surfaces away from each other, creating negative pressure (
59,
60). In addition, an adhesion–cohesion effect exists secondary to the viscous and intermolecular properties of the synovial fluid, similar to water keeping two glass surfaces together (
55).
Glenoid Labrum
The glenoid labrum provides another static restraint to GH motion. The labrum is a fibrous ring attached to the glenoid articular surface through a fibrocartilagenous transition zone. The labrum functions as an anchor point for the GH ligaments and the biceps tendon; it also deepens the glenoid socket and enhances stability (
2,
3,
39).
This wedge-shaped, fibrous structure consists of densely packed collagen bundles in a woven pattern within the hyaline cartilage (
61). It is firmly attached to the glenoid rim below the equator, where it appears as a rounded, fibrous elevation. Above the glenoid equator, the glenoid is more mobile and meniscal-like, with a triangular shape (
62). The superior labrum inserts directly into the biceps tendon distal to the insertion of the tendon at the supraglenoid tubercle. The biceps tendon anchor and the superior glenoid cover approximately 1.5 cm of the superior rim of the glenoid (
35).
In addition to greatly increasing the depth of the glenoid socket, the labrum enhances the concavity–compression mechanism that is created as the humeral head is compressed in the glenoid during RTC contraction (
56). Excision of the glenoid labrum decreases the depth of the socket by 50% and reduces the resistance to instability by 20% (
33,
39,
63).
Branches of the suprascapular artery, the circumflex scapular branch of the subscapular artery, and the posterior circumflex artery supply the glenoid labrum as it is vascularized throughout its peripheral attachment to the joint capsule. The superior and anterosuperior portions of the labrum, however, are less vascular than the posterior and inferior parts (
62). This decreased vascularity of the superior labrum may explain the vulnerability of this area to disruption.
Glenohumeral Ligaments and Joint Capsule
The GH joint capsule consists mainly of Type I collagen, with smaller amounts of Types II and III. Localized thickenings of the capsule make up the GH ligaments, which are named according to their attachments on the glenoid rim.
(Fig 10-3). The GH ligaments function as static restraints to shoulder motion. These discrete, capsular thickenings function as checkreins at the limits of rotation, preventing excess GH translation and becoming taut at varying positions of abduction and humeral rotation. Because of the orientation of these ligaments, portions of the capsule reciprocally tighten and loosen as the GH joint rotates, thus limiting translation and rotation by load sharing. Their function is dependent on the arm position and on the direction of the applied force on the joint.
Variation exists in the presence and size of these ligaments. The anatomical configuration of the inferior glenohumeral ligament (IGHL) is fairly consistent, but the configuration of the superior glenohumeral ligament (SGHL) and the middle glenohumeral ligament (MGHL) is variable. In a study of 84 cadaveric shoulders, the MGHL was separate from the origin of the SGHL in 56%, and the remaining
34%, the MGHL originated at the same location as the SGHL (
64). Overall 94% of the specimens had a SGHL. Only 63% had a discrete MGHL, however, and of these, 17.9% had cordlike MGHL.
Normal variants, such as a sublabral foramen, a cordlike MGHL, and a Buford complex, have been reported. A sublabral foramen or sulcus in which the labrum is not attached to the anterosuperior glenoid can be confused with a labral detachment (
62,
64,
65). The prevalence of a sublabral foramen has been reported to be between 12% and 19% (
66,
67). In addition, the medial and lateral edges of the MGHL can appear to be rolled in a cordlike fashion. The Buford complex is a cordlike MGHL originating directly from the superior labrum and crossing the subscapularis tendon to insert on the humerus. With a Buford complex, no anterosuperior labrum is present, and this can be confused with a Bankart lesion. The reported prevalence of a Buford complex has ranged from 1.5% to 6% (
66,
67). It is important to recognize these anatomical variants and not to confuse them with a pathologic lesion.
Superior Glenohumeral Ligament
The SGHL originates on the supraglenoid tubercle, just anterior to the origin of the long head of the biceps, and it inserts on the proximal tip of the lesser tuberosity, on the medial ridge of the intertubercular groove. The SGHL is present in more than 90% of individuals. In an anatomical study, Steinbeck et al. (
68) found the SGHL to be missing in 6% of the specimens, and in 17% of the specimens, the SGHL had a common origin with the MGHL, at the one-o’clock position on the glenoid labrum.
The SGHL runs parallel to the coracohumeral ligament (CHL), and it reflects around the biceps tendon, serving as an internal pulley at the floor of the rotator interval (RTI) (
69,
70). During a selective sectioning study, the SGHL was found to be an important inferior stabilizer of the adducted shoulder (
70). In addition, it limits posterior translation with the arm in forward flexion, adduction, and internal rotation, and it prevents anterosuperior migration of the humeral head.
Coracohumeral Ligament
The CHL originates on the dorsolateral base of the coracoid process and blends with the capsule to the greater and lesser tuberosities (
69). The CHL is present in more than 90% of individuals, and it runs parallel to the SGHL, blending with the superior border of the SGHL inferiorly. Portions of the CHL form the tunnel for the biceps tendon on the anterior side of the joint, and reinforces the RTI. In addition, the CHL reinforces the supraspinatus and infraspinatus tendon insertions as the RTC cable (
71).
The CHL has been reported to have multiple functions, limiting external rotation in the adducted arm as well as inferior translation and preventing anterosuperior migration of the humeral head (
29,
59,
69,
70). In a study of 11 cadaveric specimens that tested the static restraints of the GH joint, however, found that the CHL does not play a suspensory role (
69,
70).
Middle Glenohumeral Ligament
The MGHL originates on the supraglenoid tubercle or anterosuperior labrum, and it inserts on the lesser tuberosity running obliquely to the SGHL and the CHL. It is present between 60% and 80% of individuals as a discrete band or thickening of the anterior capsule confluent with the IGHL.
The MGHL becomes taut at 45 degrees of abduction and 10 degrees of extension and external rotation (
69,
72). Selective sectioning of the MGHL resulted in increased translation at the joint, and abducting the arm to 45 degrees increased the strain in the MGHL (
73,
74). Therefore, the overall function of the MGHL is to support the arm, to limit both anterior and posterior translation of the arm at 45 degrees of abduction and 45 degrees of external rotation, and to provide anterosuperior stability (
69,
70).
Inferior Glenohumeral Ligament
The IGHL originates on the inferior half of the glenoid neck or anterior inferior labrum, and it inserts inferior to the MGHL on the lesser tuberosity (
64). Various descriptions have been used to define this large, ligamentous structure that undergoes reciprocal tightening and loosening, depending on the position of the arm. Some have used the terms superior band, anterior axillary pouch, and posterior axillary pouch to describe the three regions of this ligament; others have described its anatomy as resembling a hammock, with a thick anterior band and a thin posterior band, surrounding the axillary pouch. The axillary pouch runs from the inferior
one-third of the humeral head to the inferior two-third of the anterior glenoid. In external rotation, the IGHL complex moves in the anterior direction, whereas with internal rotation, the complex moves in the posterior direction (
69,
70).
In a cadaveric study by Steinbeck et al. (
68), the IGHL was a clearly defined structure in 72% of the specimens and only a thickening of the inferior joint capsule in 21%. The superior band was the thickest, with an average size of 2.8 mm, whereas the posterior portion was thinner (mean thickness, 1.7 mm). In addition, that study revealed that the IGHL is thicker at the glenoid origin (mean thickness, 2.3 mm) than at the humeral insertion (mean thickness, 1.6 mm). The length and width of the anterior band have been reported to average of 37 and 13 mm, respectively (
75,
76). Histologically, the collagen fibers are predominantly radial fibers that are linked to each other by circular elements (
68,
75,
76,
77).
The IGHL complex functions as the primary restraint to anterior, posterior, and inferior GH translation with the arm at 45 to 90 degrees of abduction and external rotation (
69,
70). The anterior band and axillary pouch are anterior stabilizers, resisting anterior and inferior translation at 45 to 90 degrees degrees of abduction and external rotation, whereas the posterior band resists posterior translation of the humeral head in shoulder flexion and internal rotation (
69,
72,
78,
79).
At the neutral position (0 degrees of abduction, 30 degrees of horizontal extension), the anterior band of the IGHL becomes the primary stabilizer. Sectioning of the anterior band of the IGHL and the anterior half of the axillary pouch resulted in significant increases in anterior, posterior, and total translation at -30 and 0 degrees of flexion and extension, respectively (
80).
The posterior capsule of the GH joint lies proximal to the superior portion of the posterior band of the IGHL. It is the thinnest part of the capsule, being approximately 1 mm in width. It often is blamed for poor results after surgery for posterior instability, and it functions to limit posterior translation of the humeral head with the arm in forward flexion, adduction, and internal rotation (
58,
81).
Rotator Interval
The RTI is an area of shoulder capsule that is bounded by the supraspinatus superiorly, the subscapularis inferiorly, the coracoid process medially, and the long head of the biceps tendon laterally. The floor of the RTI is variably bridged by the GH capsule, the SGHL, the CHL, and occasionally, the MGHL (
82,
83). This area serves as safe portal for arthroscopic entry into the GH joint, because it does not violate the muscles of the RTC.
In a cadaveric study comparing the RTI of fetuses with those of adults, the RTI capsule was found, histologically, to be made of a disorganized system of collagen fibers, and it often contained a congenital hole or defect between the supraspinatus and subscapularis muscles (
82). This evidence suggests that an RTI capsular defect is a normal anatomical variant and not an acquired lesion (
82,
83,
84).
The RTI can thus contribute to inferior instability of the adducted arm. A persistent sulcus sign that does not lessen or disappear with external rotation of the arm suggests a loose or deficient RTI capsule. In patients with multidirectional instability, the RTI is characteristically thinned or absent, and a defect in this area can disrupt the negative intra-articular pressure system that normally exists in the shoulder and contribute further to instability. In contrast, a tight RTI is associated with adhesive capsulitis or postoperative stiffness and may need to be released in order to regain adequate range of motion (
82,
83,
84).
In a biomechanical study using cadaveric specimens, a transverse incision in the RTI allowed for statistically significant increases in humeral head translation in all planes tested. Subsequent imbrication of the RTI decreased inferior translation in adduction and posterior translation in flexion (
85).
Dynamic Restraints
Many dynamic factors contribute to GH stability. The RTC muscles as well as the scapular rotators contribute to stabilization by enhancing the concavity–compression mechanism. In addition, contraction of the long head of the biceps tendon, coordinated scapulothoracic rhythm, and proprioceptive mechanoreceptors in the joint capsule contribute to the dynamic stabilization of the GH joint.
Long Head of the Biceps
The long head of the biceps tendon has a variable origin, with 30% to 40% originating at the supraglenoid tubercle, 45% to 60% directly from the labrum, and 25% to 30% from both (
62,
86,
87). It travels obliquely within the shoulder joint, then turns sharply to exit inferiorly beneath the transverse humeral ligament along the bicipital groove. It decreases in size and shape along its course. The tendon becomes more flat as it progresses over the humeral head and more triangular in the bicipital groove (
88,
89). In abduction, the tendon deforms to follow the shape of the bicipital groove; in adduction, the proximal portion regains its original shape as it exits the groove (
60,
88,
90). The long head of the biceps tendon is covered by a reflection of the synovial sheath, which ends as a blind pouch at the distal part of the bicipital groove, thus making the tendon an intra-articular, but extrasynovial, structure. The tendon has an average length of 102 mm (
86).
The role of the biceps in shoulder function continues to be a topic of debate. Neer (
91) and others have suggested that it functions as a humeral head depressor and, thus, that tenodesis should be avoided, especially in patients with an RTC tear (
92). Electromyographical (EMG) studies have shown that the biceps is extremely active in throwing athletes when the shoulder is placed in the vulnerable position of abduction and external rotation, as during the late cocking phase of pitching (
93,
94). These studies also have shown an
even higher rate of activity of the biceps during this phase in pitchers with anterior instability (
90,
95,
96,
97). In addition, biomechanical studies have shown that the long head of the biceps increased the torsional rigidity of the GH joint by 32%, thus providing greater anterior stability and also serving a protective role by decreasing the load required by the IGHL (
90,
95,
96,
97).
More recent EMG studies, however, have suggested that the biceps shows little action during shoulder motion, acts mainly to control the elbow, and is not active during simple shoulder abduction (
98,
99). This is an important concept, because it has been suggested that the biceps may prevent superior displacement of the humeral head in the case of a massive RTC tear. In contrast, Walch et al. (
100) have had success with tenodesis of the biceps tendon even in patients with RTC tears, and those authors have not observed instability in these patients. It also is possible that the long head of the biceps serves a proprioceptive function and that it may play a role in neuromuscular control and coordination of shoulder motion in relation to the elbow, because the muscle–tendon unit crosses both joints. This theoretical role is supported by the interesting analogy to all the major proximal long bones, because two articulation muscles are a consistent finding in the human body (i.e., triceps in the upper arm and rectus femoris/hamstrings in the thigh). Research concerning—and the debate regarding—the function of the long head biceps tendon will surely continue.
Rotator Cuff Muscles
The RTC is composed of the supraspinatus, the infraspinatus, the subscapularis, and the teres minor muscles
(Table 10-1). The tendinous portion of the supraspinatus interdigitates with the subscapularis and the infraspinatus to form a common, continuous insertion on the humeral head, enveloping approximately 75% of the GH articulation and with a mean area of insertion on the greater tuberosity of approximately 6 cm
2. The mean distance across the insertion is 14.7 mm, and the thickness of the terminal 2 cm of the RTC ranges from 9 to 12 mm (
101,
102). The size and area of supraspinatus insertion (1.55 cm
2) is less than that of the infraspinatus insertion (1.76 cm
2) (
101,
103,
104).
The RTC often serves more than one function simultaneously. The muscles act as prime movers if their line of action is within the intended direction of motion. In addition, they act as joint stabilizers by opposing the action of the deltoid, thereby centering the humeral head against the glenoid during shoulder motion. Loss of RTC function, either from fatigue or from frank tears, can lead to superior translation of the humeral head during arm elevation, because the deltoid is left unopposed (
105).
The thin, crescent-shaped sheet of RTC comprising the distal portions of the supraspinatus and infraspinatus insertions is termed the rotator crescent, and it is bounded on its proximal margin by a thick bundle of fibers called the rotator cable (
2,
71). The rotator cable averages 2.6-fold the thickness of the rotator crescent that it surrounds, and it shields the RTC tendons from excessive stress and is readily seen arthroscopically from within the GH joint.
The supraspinatus muscle is active with any motion involving elevation, and it is the most commonly torn tendon of the cuff (
102,
106,
107). Investigators have described distinct anterior and posterior portions of the supraspinatus tendon. The anterior portion has a larger physiological cross-sectional area, making it better suited to withstand greater mechanical loads (
102,
108). The supraspinatus tendon inserts as a footprint, thickening at its insertion, with an average of 1.55 mm of bone between the cartilage edge and the tendon insertion approximately 2 mm medial to the greater tuberosity. This is important in determining the size of partial-thickness RTC tears (
101,
109).
The posterior portion of the RTC is made up of the infraspinatus and teres minor muscles. The infraspinatus has a pennate architecture with a central raphe that should not be confused with the intermuscular interval between it and the teres minor (
110).
The subscapularis internally rotates the humerus and acts as a passive stabilizer to anterior subluxation and external
rotation (
3,
111,
112,
113). The lower fibers of the subscapularis also contribute to GH stability, resisting the shear forces and superior pull of the deltoid (
114). Tears in the upper portion of the subscapularis can result in dislocation of the long head of the biceps tendon because other structures composing the sling are torn as well.