
https://www.youtube.com/watch?v=AIeRKaGa3IM
Epithelial–immune cell interplay in primary Sjögren syndrome salivary gland pathogenesis
- Review Article
- Published: 28 April 2021
Epithelial–immune cell interplay in primary Sjögren syndrome salivary gland pathogenesis
Nature Reviews Rheumatology volume 17, pages333–348 (2021)Cite this article
Abstract
In primary Sjögren syndrome (pSS), the function of the salivary glands is often considerably reduced. Multiple innate immune pathways are likely dysregulated in the salivary gland epithelium in pSS, including the nuclear factor-κB pathway, the inflammasome and interferon signalling. The ductal cells of the salivary gland in pSS are characteristically surrounded by a CD4+ T cell-rich and B cell-rich infiltrate, implying a degree of communication between epithelial cells and immune cells. B cell infiltrates within the ducts can initiate the development of lymphoepithelial lesions, including basal ductal cell hyperplasia. Vice versa, the epithelium provides chronic activation signals to the glandular B cell fraction. This continuous stimulation might ultimately drive the development of mucosa-associated lymphoid tissue lymphoma. This Review discusses changes in the cells of the salivary gland epithelium in pSS (including acinar, ductal and progenitor cells), and the proposed interplay of these cells with environmental stimuli and the immune system. Current therapeutic options are insufficient to address both lymphocytic infiltration and salivary gland dysfunction. Successful rescue of salivary gland function in pSS will probably demand a multimodal therapeutic approach and an appreciation of the complicity of the salivary gland epithelium in the development of pSS.
원발성 쇼그렌 증후군(pSS)에서는
침샘의 기능이 상당히 저하되는 경우가 많습니다.
핵 인자-κB 경로,
인플라마좀,
인터페론 신호 전달 등 여러 선천 면역 경로가
침샘 상피에서
조절 장애를 일으킬 가능성이 높습니다.
pSS에서 침샘의 관 세포는
특징적으로
CD4+ T 세포가 풍부하고
B 세포가 풍부한 침윤으로 둘러싸여 있어
상피 세포와 면역 세포 간의 어느 정도 소통이 이루어지고 있음을 암시합니다.
관 내 B 세포 침윤은
기저관 세포 증식을 포함한
림프 상피 병변의 발생을 시작할 수 있습니다.
B cell infiltrates within the ducts can initiate the development of lymphoepithelial lesions, including basal ductal cell hyperplasia.
반대로
상피는
grandular B 세포 분획에 만성 활성화 신호를 제공합니다.
이러한 지속적인 자극은
궁극적으로 점막 관련 림프 조직 림프종의 발생을 촉진할 수 있습니다.
이 리뷰에서는
침샘 상피 세포( acinar, ductal and progenitor cells )의 변화와
이러한 세포와 환경 자극 및
면역 체계의 상호 작용에 대해 논의합니다.
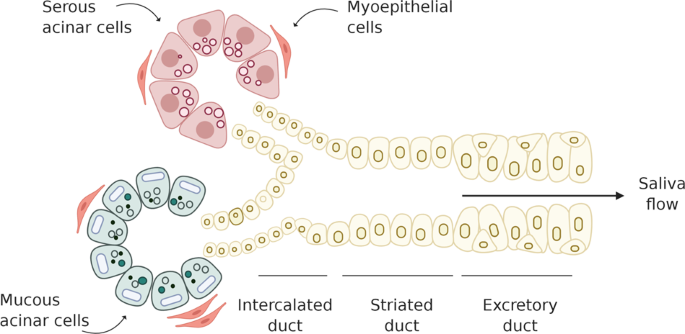
serous acinar cell : 젤과 같은 물질(뮤신 분비), carbohydrate rich substance
mucous acinar cell : 아밀라제와 같은 소화효소 분비, protein rich substance
현재의 치료 옵션은
림프구 침윤과
침샘 기능 장애를 모두 해결하기에는 불충분합니다.
pSS에서 침샘 기능을 성공적으로 회복하려면
복합적인 치료 접근 방식이 필요하며,
침샘 상피가 pSS 발병에 관여한다는 사실을 이해해야 할 것입니다.
Key points
아치니의 기능 조절 장애, 관 세포의 활성화 및 세포 사멸, 전구 세포 항상성의 결함은 모두 원발성 쇼그렌 증후군(pSS)의 침샘 기능 장애에 기여합니다.- 침샘 상피 세포의 알려지지 않은 유발 요인이 선천성 면역 반응을 활성화하고 자가 항원에 대한 적응성 면역 반응을 일으켜 상피 세포가 반응의 매개체이자 표적이 될 수 있습니다.
- 침샘 상피 세포의 선천성 면역 신호 경로의 조절 장애와 그에 따른 상피의 염증성 사이토카인 생산이 침샘 기능 장애의 원인이 될 수 있습니다.
- 자가 항체가 선천성 면역 반응에 직간접적으로 간섭하면 침샘 상피 세포와 면역 세포에서 제1형 인터페론 활성이 지속될 수 있습니다.
- 핵 인자-κB의 활성화와 전생존 인자의 발현 증가는 증식 촉진과 함께 특정 상피내 B 세포가 종양 변화를 일으켜 점막 관련 림프 림프종 발생을 촉진할 수 있습니다.
- pSS 환자의 침샘 기능 회복을 위해서는 침샘 병리에 맞춘 치료와 면역 요법과 세포 요법의 조합과 같은 복합 치료 접근법이 필요할 수 있습니다.
Similar content being viewed by others

CTLA-4-expressing ILC3s restrain interleukin-23-mediated inflammation
Article 12 June 2024

Article Open access20 June 2024

Dictionary of immune responses to cytokines at single-cell resolution
Article Open access06 December 2023
Introduction
Nearly 100 years ago, Henrik Sjögren described a disease whereby patients had a reduced functionality of the salivary glands (xerostomia) and lacrimal glands (xerophthalmia), with accompanying disturbances of the cornea and the conjunctiva (keratoconjunctivitis sicca)1. Sjögren syndrome, named after his work, has since been extensively characterized and is now considered a systemic autoimmune disease. Primary Sjögren syndrome (pSS) typically refers to the occurrence of Sjögren syndrome as the first clinically presenting autoimmune condition in a patient. In terms of clinical presentations, pSS is associated with dryness of the mouth, eyes and vagina, chronic pain and fatigue, and numerous possible extraglandular organ manifestations (including neuropathies, pulmonary manifestations and nephritis)2.
pSS is mirrored in pathological and biological analysis by the presence of lymphocytic infiltration in the salivary glands (focal lymphocytic sialadenitis) and autoantibodies in the blood. The salivary gland biopsy and its analysis have an important role in the diagnosis and classification of pSS3. Introduced in 1974, the focus score (that is, the number of lymphocytic foci per 4 mm2 tissue) has been relied upon heavily for the histological assessment of salivary gland involvement in pSS4. Infiltrating cells, congregated in foci around the striated ducts, consist mostly of CD4+ T cells and B cells, although other immune cells, including (but not limited to) myeloid dendritic cells, plasmacytoid dendritic cells (pDCs) and follicular dendritic cells, might also be present5,6. These infiltrates can develop into ectopic lymphoid structures, even comprising ectopic germinal centres7. Particular attention has been paid to the role of (glandular) B cells in pSS pathogenesis. These cells are hyperactive in pSS and responsible for the formation of autoantibodies, hypergammaglobulinaemia, lymphoepithelial lesions (LELs) and pSS-related mucosa-associated lymphoid tissue (MALT) lymphoma8,9,10,11.
Regarding autoantibodies, anti-SSA/Ro (and to a lesser extent anti-SSB/La) antibodies are present in the majority of patients with pSS3. Serum levels of anti-SSA/Ro and anti-SSB/La antibodies correlate with the number of corresponding plasma cells in the minor salivary glands of patients with pSS, suggesting that salivary glands form an important niche for autoantibody-secreting cells12. The SSA/Ro antigen comprises two ribonucleoproteins, Ro52 and Ro60, which are both present in the cytoplasm of all mammalian cells. Although a direct contribution of autoantibodies to exocrine gland dysfunction in humans has not been proven, they have been linked to glandular immune activation13. The fact that autoantibodies, encompassing anti-SSA/Ro antibodies, anti-SSB/La antibodies and rheumatoid factor, can be present years before pSS diagnosis suggests that an additional trigger is needed in the development towards clinical disease14. The journey towards impaired function of the salivary glands in pSS, resulting in reduced saliva production and a notable decrease in patient quality of life, is most probably multifactorial and still somewhat enigmatic.
Far from being only a site where infiltrating immune cells assemble, the ductal epithelium has a central role in disease pathogenesis. In this Review, we discuss how interactions between the epithelium and the immune system in pSS contribute to both disease initiation and throughout different stages of disease development in patients with pSS. We focus on new insights into the development of abnormalities in epithelial cells, as well as innate immune signalling and T cell and B cell activation within the salivary glands. All studies cited are based on human samples, unless specifically otherwise stated.
거의 100년 전
헨릭 쇼그렌은
침샘(구강건조증)과 눈물샘(안구건조증)의 기능이 저하되고
각막과 결막에 장애(각결막염)가 동반되는 질환에 대해 설명했습니다1.
그의 이름을 딴 쇼그렌 증후군은
이후 광범위하게 특성화되어 현재 전신성 자가면역 질환으로 간주되고 있습니다.
원발성 쇼그렌 증후군(pSS)은
일반적으로 환자에서 임상적으로
처음 나타나는 자가면역 질환으로서
쇼그렌 증후군이 발생하는 것을 말합니다.
임상 증상 측면에서 볼 때,
pSS는 입, 눈, 질의 건조증, 만성 통증 및 피로, 그리고
신경 병증, 폐 증상 및 신장염을 포함한 다양한 선외 장기 증상과 관련이있습니다2.
pSS는
침샘의 림프구 침윤(국소 림프구 시알라덴염)과
혈액 내 자가 항체의 존재로 병리학적 및 생물학적 분석에서 반영됩니다.
침샘 생검과 그 분석은 pSS3의 진단 및 분류에 중요한 역할을 합니다.
1974년에 도입된
초점 점수(즉, 4mm2 조직당 림프구 병소의 수)는
pSS4의 침샘 침범에 대한 조직학적 평가에 크게 의존해 왔습니다.
줄무늬관 주위의 병소에 모여 있는 침윤 세포는
대부분 CD4+ T 세포와 B 세포로 구성되지만
골수성 수지상 세포,
형질세포 수지상 세포(pDC) 및
여포 수지상 세포를 포함한 다른 면역 세포도 존재할 수 있습니다5,6.
이러한 침윤은
이소성 림프 구조로 발전할 수 있으며
심지어 이소성 배아 중심을 포함할 수도 있습니다7.
pSS 발병에서 (선상) B 세포의 역할에 특히 주목하고 있습니다.
이 세포는
pSS에서 과활성이며
자가항체, 고감마글로불린혈증, 림프 상피 병변(LEL) 및
pSS 관련 점막 연관 림프 조직(MALT) 림프종8,9,10,11의 형성에 책임이 있습니다.
자가 항체와 관련하여,
대부분의 pSS3 환자에서 항-SSA/Ro(및 그보다 적은 범위의 항-SSB/La) 항체가 존재합니다.
항-SSA/Ro 및 항-SSB/La 항체의 혈청 수준은
pSS 환자의 소타액선에 있는 해당 혈장 세포 수와 상관관계가 있으며,
이는 침샘이 자가항체 분비 세포의 중요한 틈새를 형성한다는 것을 시사합니다12.
SSA/Ro 항원은
모든 포유류 세포의 세포질에 존재하는 두 개의 리보핵단백질인 Ro52와 Ro60으로 구성됩니다.
자가 항체가
인간의 외분비선 기능 장애에 직접적으로 기여한다는 것은 입증되지 않았지만,
선 면역 활성화와 관련이 있는 것으로 알려져 있습니다13.
항SSA/Ro 항체, 항SSB/La 항체 및 류마티스 인자를 포함하는
자가 항체가 pSS 진단 수년 전부터 존재할 수 있다는 사실은
임상 질환으로 발전하는 데 추가적인 트리거가 필요하다는 것을 시사합니다14.
침샘의 기능이 손상되어
침 생산이 감소하고
환자의 삶의 질이 현저하게 저하되는 pSS의 진행 과정은
다인성일 가능성이 높으며,
아직은 다소 미스테리한 부분이 많습니다.
침샘 상피는
침윤 면역 세포가 모이는 부위일 뿐만 아니라
질병 발병의 중심 역할을 합니다.
이 리뷰에서는
pSS에서 상피와 면역계 사이의 상호작용이
어떻게 질병의 시작과
pSS 환자의 다양한 질병 발병 단계에 기여하는지에 대해 논의합니다.
상피 세포의 이상 발달과
침샘 내 선천성 면역 신호 및
T세포와 B세포 활성화에 대한 새로운 통찰에 초점을 맞춥니다.
인용된 모든 연구는 특별히 달리 명시되지 않는 한 인간 샘플을 기반으로 합니다.
Salivary gland epithelium abnormalities
A complete discussion of the deterioration of salivary gland function in pSS necessitates comprehension of the foundation of the salivary gland: the epithelium. The salivary gland epithelium comprises several cell types, namely acinar, myoepithelial and ductal cells (Fig. 1a). Acinar cells produce and secrete either watery or mucous-rich saliva (referred to as serous or mucous acinar cells, respectively). This secretion is facilitated by the contraction of myoepithelial cells that envelope the acinar cell clusters. The secreted saliva is channelled and simultaneously modified through small intercalated ducts into striated ducts (both consisting of basal and luminal cell types), and finally through the larger excretory ducts into the mouth. This architecture can be applied to both the minor and major (parotid, submandibular and sublingual) salivary glands. Although all salivary glands can be affected in pSS, the minor glands of the lower lip (the labial salivary glands (LSGs)) are most often used in diagnosis and research owing to their relative ease of access. Notably, minor salivary glands, including the LSGs, account for less than 10% of unstimulated whole saliva production15. This caveat aside, the literature suggests that the volume of LSG lymphocytic infiltration correlates only weakly with the reduction in salivary gland function in pSS16,17, implying that additional mechanisms or epithelium-specific deficits are probably important in decreased salivary gland function in pSS.
침샘 상피 이상
pSS에서 침샘 기능 저하에 대한 완전한 논의를 위해서는
침샘의 기초인 상피에 대한 이해가 필요합니다.
침샘 상피는
선상피세포, 근상피세포, 관상피세포 acinar, myoepithelial and ductal cells 등
여러 세포 유형으로 구성되어 있습니다(그림 1a).
선세포는
수성 또는 점액이 풍부한 타액을 생산하고 분비합니다(각각 장액성 또는 점액성 선세포라고 함).
serous or mucous acinar cells
이러한 분비는
침샘 세포 군집을 감싸고 있는
근상피 세포의 수축에 의해 촉진됩니다.
분비된 타액은
작은 간관을 통해 줄무늬관(기저 및 내강 세포 유형으로 구성)으로 이동하고,
마지막으로 더 큰 배설관을 통해 입안으로 배출됩니다.
이 구조는 소타액선과 대타액선(이하선, 턱밑샘, 설하선)
모두에 적용될 수 있습니다.
모든 침샘이 pSS에 영향을 받을 수 있지만,
아랫입술의 소타액선(순순타액선(LSG))은
상대적으로 접근하기 쉽기 때문에 진단 및 연구에 가장 자주 사용됩니다.
특히, LSG를 포함한 소타액선은
자극을 받지 않은 전체 타액 생산량의 10% 미만을 차지합니다15.
이러한 주의 사항을 제쳐두고,
문헌에 따르면 LSG 림프구 침윤의 양은
pSS에서 침샘 기능 감소와 약한 상관관계만 있다고 하는데16,17,
이는 pSS에서 침샘 기능 감소에 추가적인 메커니즘이나 상피 특이적 결핍이 중요할 수 있음을 암시합니다.
Fig. 1: The salivary gland epithelium in health and in pSS.
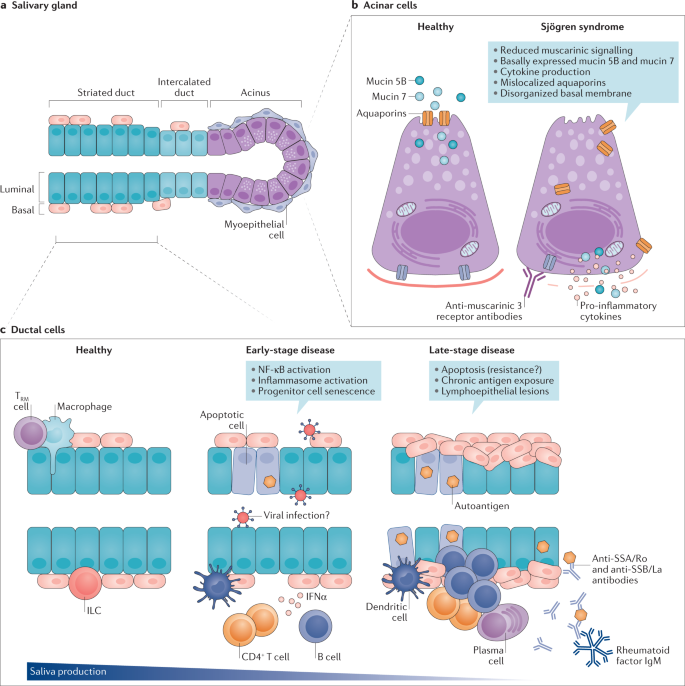
a | The salivary gland epithelium is made up of several cell types, including acinar cells (that cluster to form the acinus), ductal cells (consisting of basal and luminal cell types) that form the striated and intercalated ducts, myoepithelial cells and progenitor cells. Saliva is produced by acinar cells and secreted upon myoepithelial cell contraction. Saliva is then channelled and modified through the intercalated and striated ducts and flows via larger excretory ducts into the mouth. b | Acinar cells contain multiple defects in primary Sjögren syndrome (pSS). c | A number of pathogenic events could take place in the ductal epithelium during pSS development. In a healthy situation, several immune cells (for example, macrophages, innate lymphoid cells (ILCs) and tissue resident memory (TRM) cells) are present for immune surveillance to enable a fast response to injury or infection. In pSS, an unknown trigger (for example, viral infection or tissue damage) might cause activation of innate immune pathways, epithelial cell apoptosis and senescence, which is exacerbated in more severe stages of disease. Late-stage disease is characterized by chronic antigen exposure, local production of autoantibodies, accumulation of CD4+ T cells and B cells, complete loss of progenitor cells and the formation of lymphoepithelial lesions. These lesions are characterized by basal cell hyperplasia and the presence of intraepithelial lymphocytes.
A | 침샘 상피는 침샘을 형성하는 선상 세포, 줄무늬 관과 간관을 형성하는 관상 세포(기저 및 내강 세포 유형으로 구성), 근상피 세포 및 전구 세포를 포함한 여러 세포 유형으로 구성됩니다. 타액은 침샘 세포에서 생성되며 근상피 세포가 수축할 때 분비됩니다. 그런 다음 타액은 상호관 및 줄무늬관을 통해 전달되고 변형되어 더 큰 배설관을 통해 입안으로 흘러 들어갑니다.
b | 선세포는 원발성 쇼그렌 증후군(pSS)의 여러 결함을 포함합니다.
c | pSS가 발생하는 동안 관 상피에서 여러 가지 병원성 사건이 발생할 수 있습니다. 건강한 상황에서는 여러 면역 세포(예: 대식세포, 선천성 림프구(ILC) 및 조직 상주 기억(TRM) 세포)가 면역 감시를 위해 존재하여 부상이나 감염에 빠르게 대응할 수 있습니다. pSS에서는 알 수 없는 유발 요인(예: 바이러스 감염 또는 조직 손상)이 선천성 면역 경로의 활성화, 상피 세포 사멸 및 노화를 유발할 수 있으며, 이는 질병의 더 심각한 단계로 악화됩니다. 말기 질환은 만성 항원 노출, 자가 항체의 국소적 생산, CD4+ T 세포 및 B 세포의 축적, 전구 세포의 완전한 소실 및 림프 상피 병변 형성이 특징입니다. 이러한 병변은 기저 세포 증식과 상피 내 림프구의 존재가 특징입니다.
Changes in acinar cells in pSS
Changes in ductal cells in pSS
Complementing the acinar cells responsible for making saliva are the ductal cells. Aside from the channelling of saliva into the mouth, ductal cells are also responsible for the extraction of sodium from, and the addition of potassium to, the saliva. This process, mediated via calcium-activated sodium and potassium channels, culminates in attainment of the hypotonic sodium and potassium concentrations necessary for the slightly acidic antimicrobial functions of saliva, and for the prevention of mineral loss from dental hard tissues42. In patients with pSS, the concentrations of sodium and chloride in the saliva are higher than in healthy individuals, potentially owing to a reduction in ion resorption by ductal cells and/or because the volume of water secreted from acinar cells is reduced19,20,43,44. The investigation of the role of ductal cells in pSS has centred historically around the striated ducts in histology-based studies or in vitro culture systems of salivary gland epithelial cells (SGECs). Although cultured SGECs might represent ductal cells in general (that is, both striated and intercalated ductal cells), whether they represent striated duct cells specifically has never been proven45. For the purpose of this Review, however, we will treat SGEC cultures as a model for striated duct cells, referred to as SGECs (to mean LSG-derived SGECs) throughout unless mentioned otherwise.
SGECs from patients with Sjögren syndrome respond aberrantly to extrinsic stimuli. For example, SGECs from patients with pSS are more sensitive to FAS/FASL-mediated apoptosis in the presence of TNF and IFNγ than SGECs from healthy individuals46,47. These cells are also more susceptible to other mechanisms of programmed cell death, such as IFNγ-induced or poly (I:C)-induced anoikis (that is, apoptosis due to loss of attachment to the basal membrane)48. However, data from the literature suggest that striated duct cells22,49 and SGECs50 are both resistant and susceptible to apoptosis.
In addition to disturbed apoptosis, SGECs express various TLRs (TLR1, TLR2, TLR3, TLR4 and TLR7) and other pattern recognition receptors (PRRs), implying that these cells have an ability to process pathogen-associated molecular patterns (PAMPs) and danger-associated molecular patterns (DAMPs). Furthermore, TLR3 activation can stimulate the expression of pSS-associated autoantigens SSA/Ro60, SSA/Ro52 and SSB/La by SGECs51. SGECs can also express receptors for cytokines, including receptors for type I interferons and TNF52,53,54. The chemokine receptor CXCR3 might function as a scavenging receptor in the healthy salivary gland, preventing a build-up of surplus pro-inflammatory chemokines such as CXCL9, CXCL10 and CXCL11. In pSS, the function of this receptor is thought to be impaired in the ductal cells; indeed, in SGECs from patients with Sjögren syndrome, intracellular levels of CXCL10 are reduced compared with SGECs from healthy individuals, which is presumed to be a consequence of impaired CXCR3 functionality permitting the accumulation of these chemokines55. In addition to responding aberrantly to extrinsic stimuli, striated duct cells56,57 and SGECs52,58 from patients with Sjögren syndrome also express many cytokines and chemokines (for example, IL-1, IL-6, IL-7, IL-18, TNF, B cell-activating factor (BAFF), CXCL10, CXCL12 and CXCL13) at higher levels than those observed in healthy individuals. Thus, striated ducts and their presumed in vitro counterpart SGECs are capable of regulating the immune response (as discussed in more detail in the section on epithelial cell–lymphocyte crosstalk).
Considering the involvement of striated duct cells in, for example, LELs, the NF-κB pathway and inflammasome activation (as discussed in detail in later sections), we would argue that the role of striated duct cells in the development of pSS pathology cannot be understated. The further roles of smaller, intercalated ducts remain until this point less well understood, and will require further investigation.
침을 만드는 침샘 세포를 보완하는 세포는
관세포입니다.
관상세포는
침을 입안으로 보내는 것 외에도
침에서 나트륨을 추출하고 침에 칼륨을 첨가하는 역할도 담당합니다.
칼슘 활성화 나트륨 및 칼륨 채널을 통해 매개되는 이 과정은 타액의 약산성 항균 기능과 치아 경조직의 미네랄 손실 방지에 필요한 저산성 나트륨 및 칼륨 농도에 도달할 때 절정에 이릅니다42. pSS 환자의 경우 타액 내 나트륨과 염화물 농도가 건강한 사람보다 높은데, 이는 아마도 덕트 세포의 이온 재흡수가 감소하거나 침샘 세포에서 분비되는 물의 양이 감소하기 때문일 가능성이 있습니다19,20,43,44. pSS에서 관 세포의 역할에 대한 연구는 지금까지 조직학 기반 연구 또는 침샘 상피 세포(SGEC)의 체외 배양 시스템에서 줄무늬 관을 중심으로 이루어졌습니다. 배양된 SGEC가 일반적으로 관 세포(즉, 줄무늬 관 세포와 간관 세포 모두)를 나타낼 수 있지만, 줄무늬 관 세포를 구체적으로 나타내는지는 입증된 적이 없습니다45. 그러나 이 검토의 목적상, 별도의 언급이 없는 한, SGEC 배양을 줄무늬관 세포의 모델로 취급하며, 여기서는 줄무늬관 세포(LSG 유래 SGEC를 의미함)라고 합니다.
쇼그렌 증후군 환자의 SGEC는 외부 자극에 비정상적으로 반응합니다. 예를 들어, pSS 환자의 SGEC는 건강한 사람의 SGEC보다 TNF 및 IFNγ가 있을 때 FAS/FASL 매개 세포 사멸에 더 민감합니다46,47. 이러한 세포는 또한 IFNγ 유도 또는 폴리(I:C) 유도 아노이키스(기저막 부착 상실로 인한 세포 사멸)48와 같은 다른 프로그래밍된 세포 사멸 메커니즘에 더 취약합니다. 그러나 문헌에 따르면 줄무늬관 세포22,49 및 SGEC50는 세포 사멸에 저항성이 있고 취약한 것으로 나타났습니다.
세포 사멸 장애 외에도 SGEC는
다양한 TLR(TLR1, TLR2, TLR3, TLR4 및 TLR7)과
기타 패턴 인식 수용체(PRR)를 발현하는데,
이는 이 세포가
병원체 관련 분자 패턴(PAMP)과
손상 관련 분자 패턴(DAMP)을 처리하는 능력을 가지고 있음을 의미합니다.
또한, TLR3 활성화는 SGEC에 의한 pSS 관련 자가 항원 SSA/Ro60, SSA/Ro52 및 SSB/La의 발현을 자극할 수 있습니다51. SGEC는 또한 제1형 인터페론 및 TNF52,53,54 수용체를 포함한 사이토카인 수용체를 발현할 수 있습니다. 케모카인 수용체 CXCR3는 건강한 침샘에서 청소 수용체로 기능하여 CXCL9, CXCL10 및 CXCL11과 같은 전 염증성 케모카인의 과잉 축적을 방지할 수 있습니다. pSS에서는 이 수용체의 기능이 관 세포에서 손상된 것으로 생각되며, 실제로 쇼그렌 증후군 환자의 SGEC에서는 건강한 사람의 SGEC에 비해 CXCL10의 세포 내 수치가 감소하는데, 이는 이러한 케모카인의 축적을 허용하는 CXCR3 기능 장애의 결과로 추정됩니다55. 외부 자극에 비정상적으로 반응하는 것 외에도 쇼그렌 증후군 환자의 줄무늬관 세포56,57 및 SGEC52,58는 건강한 사람에서 관찰되는 것보다 많은 사이토카인과 케모카인(예: IL-1, IL-6, IL-7, IL-18, TNF, B 세포 활성화 인자(BAFF), CXCL10, CXCL12 및 CXCL13)을 높은 수준에서 발현하는 것으로 나타났습니다. 따라서 줄무늬 관과 이에 대응하는 것으로 추정되는 체외 SGEC는 면역 반응을 조절할 수 있습니다(상피세포-림프구 누화에 대한 섹션에서 자세히 설명함).
예를 들어, 줄무늬관 세포가 LEL, NF-κB 경로 및 인플라마좀 활성화(이후 섹션에서 자세히 설명)에 관여하는 것을 고려할 때, pSS 병리의 발달에서 줄무늬관 세포의 역할은 과소평가할 수 없다고 주장할 수 있습니다. 더 작고 상호 연결된 덕트의 역할은 아직까지 잘 알려지지 않았으며 추가 연구가 필요합니다
Salivary gland homeostasis disruption
Mouse studies have shown that a small number of immune cells, including but potentially not limited to tissue-resident memory T (TRM) cells, macrophages, group 1 innate lymphoid cells (ILC1s), natural killer cells and dendritic cells, patrol the salivary glands, scanning for hallmarks of infection and/or epithelial cell damage59,60 (Fig. 1c). TRM cells and macrophages, in particular, have been identified in close association with the mouse acinar epithelium60. In patients with pSS, this homeostatic surveillance system seems to be disturbed, and the salivary gland immune landscape is unbalanced owing to an infiltration of mainly CD4+ T and B cells as well as, in lower abundance, pDCs and other immune cells9. Besides their immune function, these infiltrating cells can affect salivary gland homeostasis in multiple ways, including crosstalk with the salivary gland epithelium (which will be discussed in more detail in the section on epithelial cell–lymphocyte crosstalk).
In normal salivary gland homeostasis, the aforementioned immune cell sentinels are complemented by salivary gland progenitor cells (SGPCs). SGPCs proliferate and differentiate into fresh acinar and ductal cells, to replenish damaged cells and cells reaching the end of their lifespan61,62,63,64. In the major salivary glands, the ductal compartment (both the striated and intercalated ducts) has been proposed to house SGPCs, although progenitor cells might also be present in the acinar compartment61,65,66,67. These progenitor cells can be studied in vitro through organoid cultures61,65,68. The number of SGPCs is much lower in patients with pSS than in healthy salivary glands, and the few that remain have a lower differentiation capacity68. One explanation for this finding is that progenitor cells residing in the basal layer of the parotid gland striated ducts become senescent prematurely in pSS, as a result of the mitotic effects of pro-inflammatory cytokines68. The telomeres of SGPCs from patients with pSS are shorter, suggesting that some SGPCs have indeed undergone replicative senescence68. In one study, the degree of senescence of cells located in the basal layer of the striated ducts (where progenitor cells probably reside), as inferred from the expression of the senescence marker p16, correlated with the production of saliva by the parotid salivary gland, the extent of CD45+ cell infiltration and the ultrasound score69. The expression of p16 by all acinar and ductal cells combined also correlated with saliva production and CD45+ cell infiltration, but to a lesser extent69. Senescent cells in general have a senescence-associated secretory phenotype (SASP), consisting of the expression of a panel of pro-inflammatory cytokines (including IL-1α, IL-1β, IL-6, IL-7, IL-13, IL-15, TGFβ, GM-CSF and TNF), chemokines (including IL-8, GROα, GROβ, CCL2, CCL3, CCL5, CCL16, CCL26 and CCL20), growth factors (including HGF and FGF), matrix metalloproteases and proteases70,71,72. Most interestingly and potentially detrimentally, this SASP enables the active spreading of senescence directly to neighbouring cells72. Therefore, senescent cells might not only reduce the ability of the salivary gland to function, by disabling a potential progenitor cell population, but also augment inflammation and disease progression. Coupled with this effect is the strange persistence of functionally defective acinar cells, whose clearance would otherwise presumably trigger replacement with fresh counterparts by SGPCs, a curious dynamic that requires more investigation.
Of further interest, disruption of salivary gland homeostasis also occurs in patients undergoing immune checkpoint inhibitor (ICI) therapy for the treatment of cancer. Approximately 5% of ICI-treated patients will experience some form of salivary gland dysfunction73,74,75,76. Among these patents, 60% will progress to technically fulfil the ACR–EULAR 2016 criteria for pSS3, owing to the presence of sicca symptoms, immune foci in the salivary glands and/or autoantibody positivity73,74,75,76. The potential mechanism of ICI-induced salivary gland dysfunction is highlighted in Box 1.
마우스 연구에 따르면 조직 상주 기억 T(TRM) 세포, 대식세포, 1군 선천성 림프구(ILC1), 자연 살해 세포 및 수지상 세포를 포함한 소수의 면역 세포가 침샘을 순찰하며 감염 및/또는 상피 세포 손상59,60의 특징을 스캔합니다(그림 1c). 특히 TRM 세포와 대식세포는 마우스 침샘 상피와 밀접한 연관성이 있는 것으로 확인되었습니다60. pSS 환자에서는 이러한 항상성 감시 시스템이 교란된 것으로 보이며, 침샘 면역 환경은 주로 CD4+ T 및 B 세포뿐만 아니라 낮은 농도의 pDC 및 기타 면역 세포의 침윤으로 인해 불균형을 이룹니다9. 이러한 침윤 세포는 면역 기능 외에도 침샘 상피와의 혼선을 포함하여 다양한 방식으로 침샘 항상성에 영향을 미칠 수 있습니다(상피 세포-림프구 혼선에 대한 섹션에서 더 자세히 설명합니다).
정상적인 침샘 항상성에서 앞서 언급한 면역 세포 센티널은 침샘 전구 세포(SGPC)에 의해 보완됩니다. SGPC는 손상된 세포와 수명이 다한 세포를 보충하기 위해 새로운 선세포와 도관 세포로 증식하고 분화합니다61,62,63,64. 주요 침샘에서 덕관 구획(줄무늬 덕관 및 간관 모두)은 SGPC를 수용하는 것으로 제안되었지만, 전구 세포는 선관 구획에도 존재할 수 있습니다61,65,66,67. 이러한 전구세포는 오가노이드 배양을 통해 체외에서 연구할 수 있습니다61,65,68. SGPC의 수는 건강한 침샘에 비해 pSS 환자에서 훨씬 적으며, 남아 있는 소수의 세포는 분화 능력이 더 낮습니다68. 이 결과에 대한 한 가지 설명은 귀밑샘 줄무늬 관의 기저층에 존재하는 전구 세포가 전 염증성 사이토카인의 유사 분열 효과로 인해 pSS에서 조기에 노화된다는 것입니다68. pSS 환자의 SGPC의 텔로미어는 더 짧아져 일부 SGPC가 실제로 복제 노화를 겪었음을 시사합니다68. 한 연구에서는 노화 마커 p16의 발현에서 유추할 수 있는 줄무늬관 기저층(전구 세포가 있을 가능성이 있는 곳)에 위치한 세포의 노화 정도는 이하선 침샘의 타액 생성, CD45+ 세포 침윤 정도 및 초음파 점수69와 상관관계가 있는 것으로 나타났습니다. 모든 침샘 세포와 도관 세포를 합친 p16의 발현도 타액 생성 및 CD45+ 세포 침윤과 상관관계가 있었지만 그 정도는 덜했습니다69. 일반적으로 노화 세포는 전 염증성 사이토카인 패널(IL-1α, IL-1β, IL-6, IL-7, IL-13 포함)의 발현으로 구성되는 노화 관련 분비 표현형(SASP)을 가지고 있습니다, IL-15, TGFβ, GM-CSF 및 TNF), 케모카인(IL-8, GROα, GROβ, CCL2, CCL3, CCL5, CCL16, CCL26 및 CCL20 포함), 성장 인자(HGF 및 FGF 포함), 매트릭스 메탈로 프로테아제 70,71,72) 및 프로테아제. 가장 흥미롭고 잠재적으로 해로울 수 있는 점은 이 SASP가 노화를 주변 세포로 직접 확산시킬 수 있다는 점입니다72. 따라서 노화 세포는 잠재적인 전구 세포 집단을 무력화하여 침샘의 기능을 저하시킬 뿐만 아니라 염증과 질병 진행을 촉진할 수 있습니다. 이러한 효과와 함께 기능적으로 결함이 있는 침샘 세포가 이상하게도 지속되는 현상이 나타나는데, 이는 아마도 SGPC에 의해 새로운 세포로 대체되는 것으로 추정되며, 이는 더 많은 연구가 필요한 흥미로운 역학 관계입니다.
더욱 흥미로운 점은 암 치료를 위해 면역 관문 억제제(ICI) 치료를 받는 환자에서도 침샘 항상성 파괴가 발생한다는 것입니다. ICI 치료를 받은 환자의 약 5%가 어떤 형태의 침샘 기능 장애를 경험합니다73,74,75,76. 이 특허 중 60%는 시카 증상, 침샘의 면역 병소 및/또는 자가항체 양성으로 인해 기술적으로 pSS3에 대한 ACR-EULAR 2016 기준을 충족하는 것으로 진행됩니다73,74,75,76. ICI로 인한 침샘 기능 장애의 잠재적 메커니즘은 상자 1에 강조 표시되어 있습니다.
Box 1 Salivary gland dysfunction following checkpoint inhibition
Both the major and minor salivary glands contain a T cell-rich inflammatory infiltrate following immune checkpoint inhibitor (ICI) use, but the glands do not resemble classical salivary glands of patients with pSS on the infiltration level74,203. Some evidence suggests that ICI therapy induces a considerable shift in the organization of the parenchyma (specifically, a loss of typical saliva-producing acinar cells)203. The mechanism underpinning this effect is as yet unclear, but might encompass acinar cell death followed by aberrant salivary gland progenitor cell compensation, or increased plasticity of salivary gland epithelial cell types. This plasticity could be induced, for example, by the presence of the type II interferon signature associated with cytotoxic T cell activation and checkpoint inhibitor therapy (as opposed to the type I interferon signature most commonly associated with classical pSS), and might explain the notably different morphology observed204. Although presenting potentially with a different phenotype to pSS, deciphering how this epithelial skewing occurs will probably shed light on the mechanism underpinning salivary gland dynamics in general.
Show more
Virus–epithelial cell interactions
Microorganisms are implicated as a potential trigger in the development of pSS. Activation of TLRs that recognize components of bacteria (such as TLR1, TLR2 and TLR4) or viruses (such as TLR3, TLR7 and TLR9) on salivary gland ductal cells, for example, might represent a first step in the initiation of inflammation in the salivary gland in the early stages of disease. However, evidence that conclusively demonstrates the contribution of specific bacteria to salivary gland dysfunction in pSS is lacking77,78,79,80,81. Indeed, the most likely hypothesis is that alterations in the bacteriome in the oral cavity represent a consequence, rather than a cause, of salivary gland dysfunction in pSS82. Nevertheless, the triggering of specific TLRs and other (cytosolic) PPRs on SGECs by viral material might result in type I interferon production, and conceivably contribute to the well-known type I interferon signature associated with pSS. Although intrinsic and other extrinsic triggers might also be responsible for interferon production by epithelial cells (as discussed in the later section on interferon pathways and as reviewed elsewhere83), this common feature of pSS suggests the presence of an initial immune response against viral infection.
To date, infection with three different viruses has been associated with the development of pSS. First, some data suggest that past infection with hepatitis C virus (HCV) is associated with the development of pSS, with estimates suggesting that approximately 14% of patients with pSS test positive for antibodies against HCV in certain pSS populations84,85,86. However, it should be noted that HCV infection (latent or active) is an exclusion criterion in the 2016 ACR-EULAR classification criteria for pSS and debate exists as to whether this patient subgroup truly represents pSS or a Sjögren syndrome-like condition, especially as HCV infection rates vary widely geographically86. Second, chronic infection with human T cell lymphotropic virus type 1 (HTLV1) has also been associated with low-grade salivary gland damage in pSS and increased serum concentrations of TNF and IFNγ, although this virus is not necessarily associated with pSS development87,88. Patients with sicca syndrome and HTLV1 antibody serum positivity, for example, do not tend to have anti-SSA autoantibodies87,88. Third, various evidence points to an association between Epstein–Barr virus (EBV) and pSS, although it should be noted that this virus is very common and present in up to 95% of the general population89. The EBV remains latent in resting memory B cells and requires B cell stimulation and plasma cell differentiation for lytic replication89,90,91. This ability to remain dormant in memory B cells means that the virus poses a persistent threat. EBV DNA has been detected at increased levels in the salivary glands of patients with pSS compared with healthy individuals, with Ro52-reactive perifollicular plasma cells being frequently infected92,93. Furthermore, patients who were also positive for anti-SSA and/or anti-SSB antibodies had higher titres of IgG antibodies against the EBV early antigen than those patients without anti-SSA and anti-SSB antibodies91.
EBV is capable of directly infecting epithelial cells; in these cells, the EBV glycoprotein BMRF2 mediates transport of the virus to the basolateral membrane and seems to facilitate spreading of progeny virions94. In one study, levels of the EBV-derived microRNA ebv-miR-BART13-3p were increased in the salivary glands of patients with pSS compared with healthy individuals95. Interestingly, ebv-miR-BART13-3p was suggested to downregulate the expression of stromal interaction molecule 1 (STIM1), a component of the acinar cell secretory machinery, providing a plausible link between EBV and saliva production95. This microRNA can transfer between cells, such as between B cells (the preferred target cells of EBV) and SGECs, via microvesicles95. Notably, the EBV protein Epstein–Barr nuclear antigen 2 (EBNA2) has a marked degree of protein sequence similarity to Ro60 autoantigens and likewise the protein sequences of Epstein–Barr virus (EBV)-encoded RNA 1 (EBER1) and EBER2 are strikingly similar to La autoantigens96,97. Furthermore, antibodies to Ro60 can cross-react with EBNA1 (ref.98), suggesting that molecular mimicry might trigger immune system activation to self-antigens in pSS. However, no correlation has been found between EBV reactivation periods and the development of pSS symptoms96; furthermore, the molecular mimicry hypothesis does not explain why such a common infection as EBV results in pSS development in only a small proportion of these individuals89.
How viral infections might contribute to pSS remains unclear. In addition to the often touted classical hypotheses, including molecular mimicry or enhanced apoptosis of epithelial cells, evidence would also suggest that viruses are capable of inducing epigenetic changes in epithelial cells99, an exciting new interaction that remains to be investigated in pSS. Virus-induced epigenetic changes might, for example, repress the expression of pro-apoptotic genes. Impaired viral clearance as a mechanism for pSS development has also been inferred from the presence of a less efficient splice variant of the classical type I interferon downstream mediator OAS1 in patients with pSS100,101.
With respect to SARS-CoV-2 viral infections, it is worth considering that a potential pool of patients with sicca complaints might be emerging. The involvement of the salivary gland as a reservoir of this virus has been proposed, following the identification of the ACE2 receptor (an entry receptor for SARS-CoV-2) on SGECs102,103. Close monitoring of this patient pool over the coming years might provide crucial evidence regarding the role of viral infections in the triggering of sicca symptoms and possibly also in the triggering of pSS.
바이러스-상피세포 상호작용
미생물은 pSS 발병의 잠재적 유발 요인으로 알려져 있습니다.
예를 들어
침샘관 세포에서 박테리아(예: TLR1, TLR2, TLR4) 또는
바이러스(예: TLR3, TLR7, TLR9)의 성분을 인식하는
TLR의 활성화는
질병 초기 침샘에 염증이 시작되는 첫 단계로 볼 수 있습니다.
그러나 특정 박테리아가 pSS에서 침샘 기능 장애에 기여한다는 것을 결정적으로 입증하는 증거는 부족합니다77,78,79,80,81. 실제로 가장 유력한 가설은 구강 내 박테리아 군집의 변화가 pSS에서 침샘 기능 장애의 원인이 아니라 결과라는 가설입니다82. 그럼에도 불구하고, 바이러스 물질에 의한 SGEC의 특정 TLR 및 기타 (세포질) PPR의 유발은 제1형 인터페론 생산을 초래할 수 있으며, pSS와 관련된 잘 알려진 제1형 인터페론 시그니처에 기여할 수 있을 것으로 생각됩니다. 내인성 및 기타 외인성 유발 요인도 상피 세포에 의한 인터페론 생성의 원인이 될 수 있지만(인터페론 경로에 대한 뒷부분에서 논의하고 다른 곳에서 검토한 바와 같이83), pSS의 이러한 일반적인 특징은 바이러스 감염에 대한 초기 면역 반응이 존재한다는 것을 시사합니다.
현재까지 세 가지 다른 바이러스에 의한 감염이 pSS의 발병과 관련이 있는 것으로 밝혀졌습니다.
첫째, 일부 데이터에 따르면 과거 C형 간염 바이러스(HCV) 감염이 pSS 발병과 관련이 있으며, 특정 pSS 집단에서 약 14%의 pSS 환자가 HCV 항체 양성 반응을 보인다는 추정이 있습니다84,85,86. 그러나 2016년 ACR-EULAR 분류 기준에서 HCV 감염(잠복성 또는 활동성)은 pSS의 제외 기준이며, 특히 HCV 감염률이 지역적으로 매우 다양하기 때문에 이 환자 하위 그룹이 실제로 pSS 또는 쇼그렌 증후군과 유사한 상태를 나타내는지에 대한 논쟁이 존재한다는 점에 유의해야 합니다86.
둘째, 인간 T 세포 림프구 바이러스 1형(HTLV1)의 만성 감염도 pSS에서 낮은 등급의 침샘 손상 및 혈청 내 TNF 및 IFNγ 농도 증가와 관련이 있지만, 이 바이러스가 반드시 pSS 발병과 연관된 것은 아닙니다87,88. 예를 들어, 시카 증후군 및 HTLV1 항체 혈청 양성 환자는 항-SSA 자가 항체를 보유하지 않는 경향이 있습니다87,88.
셋째, 엡스타인-바 바이러스(EBV)와 pSS 사이의 연관성을 보여주는 다양한 증거가 있지만, 이 바이러스는 매우 흔하며 일반 인구의 최대 95%에 존재한다는 점에 유의해야 합니다89. EBV는 휴면기 기억 B 세포에 잠복해 있으며 용해성 복제를 위해 B 세포 자극과 혈장 세포 분화가 필요합니다89,90,91. 기억 B 세포에서 휴면 상태를 유지하는 이 능력은 이 바이러스가 지속적인 위협을 가한다는 것을 의미합니다. 건강한 사람에 비해 pSS 환자의 침샘에서 EBV DNA가 증가된 수준으로 검출되었으며, Ro52 반응성 융모 주위 혈장 세포가 자주 감염되는 것으로 나타났습니다92,93. 또한 항-SSA 및/또는 항-SSB 항체 양성인 환자는 항-SSA 및 항-SSB 항체가 없는 환자보다 EBV 초기 항원에 대한 IgG 항체 역가가 더 높았습니다91.
EBV는 상피 세포를 직접 감염시킬 수 있으며, 이 세포에서 EBV 당단백질 BMRF2는 기저막으로 바이러스의 이동을 매개하고 자손 비리온의 확산을 촉진하는 것으로 보입니다94. 한 연구에서는 건강한 사람에 비해 pSS 환자의 침샘에서 EBV 유래 마이크로RNA ebv-miR-BART13-3p의 수치가 증가했습니다95. 흥미롭게도 ebv-miR-BART13-3p는 침샘 세포 분비 기계의 구성 요소인 기질 상호작용 분자 1(STIM1)의 발현을 하향 조절하여 EBV와 침 생성 사이의 그럴듯한 연관성을 제공하는 것으로 제안되었습니다95. 이 마이크로RNA는 미세소포를 통해 B세포(EBV의 선호 표적 세포)와 SGEC 사이와 같이 세포 간을 이동할 수 있습니다95. 특히, EBV 단백질 엡스타인-바 핵 항원 2(EBNA2)는 Ro60 자가 항원과 단백질 서열 유사성이 매우 높으며, 엡스타인-바 바이러스(EBV)-코딩된 RNA 1(EBER1) 및 EBER2의 단백질 서열도 마찬가지로 La 자가 항원과 놀라울 정도로 유사합니다96,97. 또한 Ro60에 대한 항체는 EBNA1과 교차 반응할 수 있으며(참조.98), 이는 분자 모방이 pSS에서 자가 항원에 대한 면역 체계 활성화를 유발할 수 있음을 시사합니다. 그러나 EBV 재활성화 기간과 pSS 증상 발생 사이에는 상관관계가 발견되지 않았습니다96; 또한 분자 모방 가설은 EBV와 같은 일반적인 감염이 왜 이들 중 일부에게만 pSS가 발생하는지 설명하지 못합니다89.
바이러스 감염이 어떻게 pSS에 기여하는지는 아직 명확하지 않습니다. 상피 세포의 분자 모방 또는 세포 사멸 강화와 같이 자주 언급되는 고전적 가설 외에도, 바이러스가 상피 세포의 후성 유전적 변화를 유도할 수 있다는 증거도 있으며99, 이는 pSS에서 아직 조사해야 할 흥미로운 새로운 상호 작용입니다. 예를 들어, 바이러스에 의한 후성유전학적 변화는 세포사멸 촉진 유전자의 발현을 억제할 수 있습니다. pSS 발병의 메커니즘으로서 바이러스 제거 장애는 pSS100,101 환자에서 고전적인 1형 인터페론 하류 매개체 OAS1의 덜 효율적인 스플라이스 변이가 존재하는 것으로부터도 유추할 수 있습니다.
SARS-CoV-2 바이러스 감염과 관련하여 식도염을 호소하는 잠재적 환자 풀이 등장할 수 있다는 점을 고려할 필요가 있습니다. 침샘이 이 바이러스의 저장소로 관여한다는 것은 SGECs102,103에서 ACE2 수용체(SARS-CoV-2의 진입 수용체)가 확인된 이후 제안되었습니다. 향후 몇 년 동안 이 환자 풀을 면밀히 모니터링하면 바이러스 감염이 sicca 증상을 유발하고 pSS를 유발하는 역할에 대한 중요한 증거를 제공할 수 있습니다.
Innate immune function of the epithelium
As discussed in the previous sections, the salivary gland epithelium fulfils innate immune functions that are mainly mediated by the expression of PRRs (for example, TLRs)53,54 and the secretion of cytokines. In this section, we discuss the different innate immunological pathways that contribute to dysfunction of the salivary gland epithelium in pSS. Although the initial events that cause innate immune activation in the salivary gland epithelium remain to be identified, several possibilities have been raised. These include the involvement of exogenous antigens (for example, PAMPs from ineffectively cleared viruses) or aberrant expression of endogenous factors (for example, retroelements) that stimulate innate immune responses. Another possibility is that these responses are triggered by DAMPs because of inefficient removal of epithelial cell debris. Interestingly, a patient’s genetic background might predispose them to impaired clearance of cell debris. The genotype and copy gene number of the complement component C4 has a high sex bias and has been linked to pSS susceptibility104. The lower gene copy number and expression of C4A reported for women that increase the risk of SLE or pSS might reduce the capacity of the immune system to clear cell debris, thereby prolonging exposure of intracellular proteins to the immune system104. However, data on the relationship between the C4 genotype and salivary gland pathology are not yet available.
상피의 선천성 면역 기능
이전 섹션에서 논의한 바와 같이
침샘 상피는
주로 PRR(예: TLR)53,54의 발현과 사이토카인의 분비에 의해 매개되는
선천성 면역 기능을 수행합니다.
이 섹션에서는 pSS에서 침샘 상피의 기능 장애에 기여하는 다양한 선천성 면역 경로에 대해 설명합니다. 침샘 상피에서 선천성 면역 활성화를 유발하는 초기 사건은 아직 밝혀지지 않았지만 몇 가지 가능성이 제기되고 있습니다. 여기에는 선천성 면역 반응을 자극하는 외인성 항원(예: 비효율적으로 제거된 바이러스의 PAMP) 또는 내인성 인자의 비정상적인 발현(예: 레트로엘레멘트)의 관여가 포함됩니다. 또 다른 가능성은 상피 세포 잔해의 비효율적인 제거로 인해 DAMP에 의해 이러한 반응이 촉발될 수 있다는 것입니다. 흥미롭게도 환자의 유전적 배경이 세포 잔해 제거에 장애를 일으킬 수 있습니다. 보체 성분 C4의 유전자형과 복제 유전자 수는 성별 편향성이 높으며 pSS 감수성과 관련이 있습니다104. 여성에서 보고된 낮은 유전자 복제 수와 C4A의 발현은 SLE 또는 pSS의 위험을 증가시켜 면역 체계의 세포 파편 제거 능력을 감소시켜 세포 내 단백질이 면역 체계에 노출되는 기간을 연장시킬 수 있습니다104. 그러나 C4 유전자형과 침샘 병리 사이의 관계에 대한 데이터는 아직 없습니다.
NF-κB signalling
The NF-κB family is a group of transcription factors capable of activating an array of inflammatory downstream targets, including pro-inflammatory cytokines105. The canonical NF-κB pathway is activated by binding of PAMPs to the TLRs and by pro-inflammatory cytokines themselves binding to their respective receptors105. Engagement of TLR and cytokine receptors triggers activity of the IκB kinase complex, culminating in phosphorylation of IκBα. In the inactive state, IκBα is in complex with canonical NF-κB members RelA and p50, whereas phosphorylation of IκBα results in degradation of this inhibitor, enabling the release of the RelA–p50 heterodimer and its subsequent translocation to the nucleus, where the dimer activates target gene transcription105. Studies have reported NF-κB activity in the epithelial cells of the salivary glands of patients with pSS, reflected by the expression of NF-κB downstream target genes encoding cytokines such as IL-1α, IL-6 and TNF57. NF-κB is also important for the regulation of cell–cell interactions and is capable of disrupting tight junction integrity106. Mutations that result in overactivity of the NF-κB pathway have been reported in patients with pSS: for example, mutations in genes encoding IκBα or the inhibitor TNFα-induced protein 3 (TNFAIP3; also known as A20)107,108,109. Interestingly, in mice, constitutive activation of the NF-κB pathway via knockout of TNFAIP3 in cytokeratin 14–expressing epithelial cells (including those cells of the striated duct) is sufficient to result in reduced saliva production and infiltration of a T cell-rich infiltrate into the salivary glands110. This finding emphasizes the role of epithelial cells and the NF-κB pathway in pSS development, and the apparent ability of activated epithelial cells to recruit immune cells.
NF-κB 계열은
전 염증성 사이토카인을 포함한 다양한 염증성 하류 표적을 활성화할 수 있는
전사인자 그룹입니다105.
표준 NF-κB 경로는
PAMP가 TLR에 결합하고
전 염증성 사이토카인 자체가 각각의 수용체에 결합함으로써
활성화됩니다105.
TLR과 사이토카인 수용체의 결합은
IκB 키나제 복합체의 활성을 촉발하여
IκBα의 인산화에 이릅니다.
비활성 상태에서 IκBα는 정식 NF-κB 구성원인 RelA 및 p50과 복합체를 이루는 반면, IκBα의 인산화는 이 억제제의 분해를 초래하여 RelA-p50 이합체의 방출과 핵으로의 후속 전위를 가능하게 하고, 이합체는 표적 유전자 전사를 활성화합니다105.
연구에 따르면 pSS 환자의 침샘 상피 세포에서
IL-1α, IL-6 및 TNF57과 같은 사이토카인을 코딩하는
NF-κB 하류 표적 유전자의 발현으로 반영되는
NF-κB 활성이 보고되었습니다.
NF-κB는 또한
세포와 세포 간의 상호작용 조절에 중요하며,
긴밀한 접합부 무결성을 방해할 수 있습니다106.
NF-κB 경로의 과활성화를 초래하는 돌연변이가
pSS 환자에서 보고되었습니다.
예를 들어, IκBα 또는 억제제 TNFα 유도 단백질 3(TNFAIP3; A20이라고도 함)107,108,109을 암호화하는 유전자의 돌연변이 등이 있습니다. 흥미롭게도 생쥐에서 사이토케라틴 14 발현 상피 세포(줄무늬관 세포 포함)에서 TNFAIP3의 녹아웃을 통한 NF-κB 경로의 구성적 활성화는 타액 생성 감소와 침샘에 풍부한 T 세포 침윤을 초래하기에 충분합니다110. 이 발견은 pSS 발생에서 상피 세포와 NF-κB 경로의 역할과 활성화된 상피 세포가 면역 세포를 모집하는 명백한 능력을 강조합니다.
The inflammasome
The inflammasome is an intracellular complex of oligomers that detect and respond to DAMPs and PAMPs to incite inflammation, functioning as an important innate immune system receptor and sensor. Inflammasomes require priming via classical innate immune activation pathways, such as the microbe-activated TLR pathway111. Subsequent to this signal, a second activation signal of inflammasome components via stimuli such as lysosomal disruption, reactive oxygen species production and release of oxidized mitochondrial DNA or microbial nucleic acids is required111. Inflammasomes can be broadly divided into four types: the absent in melanoma 2 (AIM2) inflammasome, the NOD-, LRR- and pyrin domain-containing protein 1 (NLRP1) inflammasome, the NLRP3 inflammasome and the NLRP4 inflammasome. Inflammasome activation ultimately facilitates processing of pre-formed pro-inflammatory cytokines such as pro-IL-1β and pro-IL-18 into their final active forms. Stimulation of the AIM2 inflammasome occurs following binding by cytosolic free DNA (cfDNA) of viral, bacterial or mammalian origin, but not by other triggers112. Some data suggest that the AIM2 inflammasome is highly active in SGECs from patients with pSS, which could be because of defective functioning of DNase 1 resulting in the accumulation of cfDNA113. Patients with pSS and MALT lymphomas, and those patients with pSS judged to be at a high risk of developing MALT lymphomas, have high serum levels of cfDNA and extranuclear DNA accumulations in salivary gland tissue, mostly localized between the striated ducts and lymphocytic infiltrates114. This extracellular DNA, if transported into striated duct cells, might be an important stimulus for the AIM2 inflammasome.
Oligomerization of NRLP1, NRLP3 or NRLP4 results from upregulation of NRLP transcription following signals induced by cfDNA, as is described for AIM2, as well as signals induced by a panoply of DAMPs, PAMPs and other triggers, such as reactive oxygen species, oxidized mitochondrial DNA and lysosomal disruption. Various data suggest that the salivary glands of patients with pSS express higher levels of NLRP3 than healthy individuals, and P2X7, a component of the NRLP3 machinery, is also upregulated in the salivary gland tissue of patients with pSS114,115. However, which specific cell types express the upregulated NRLP3 is unclear, as indeed is the expression of the NRLP1 and NRLP4 inflammasomes in pSS115. However, although perhaps less well-understood than the role of the TLR and NF-κB systems, a central role for the inflammasome in pSS is emerging. Mirroring the NF-κB pathway, the activity of the inflammasome in the salivary gland epithelium reinforces the role of the epithelium, and its crosstalk with the immune system, in pSS. The upregulated inflammasome might contribute to the sustained glandular inflammatory process in pSS, and represents a potential alternative therapeutic target.
인플라마좀은
염증을 유발하는 DAMP와 PAMP를 감지하고
이에 반응하는 올리고머의 세포 내 복합체로,
중요한 선천 면역계 수용체 및 센서로 기능합니다.
인플라마좀은 미생물 활성화 TLR 경로111와 같은
고전적인 선천성 면역 활성화 경로를 통해 프라이밍을 필요로 합니다.
이 신호에 이어
리소좀 파괴,
활성 산소종 생성,
산화 미토콘드리아 DNA 또는
미생물 핵산 방출과 같은 자극을 통한 인플라마솜 구성 요소의
두 번째 활성화 신호가 필요합니다111.
인플라마좀은 크게 4가지 유형으로 나눌 수 있는데,
흑색종에 없는 인플라마좀 2(AIM2), NOD-, LRR- 및
피린 도메인 함유 단백질 1(NLRP1) 인플라마좀,
NLRP3 인플라마좀 및
NLRP4 인플라마좀이 그것입니다.
인플라마좀 활성화는 궁극적으로 프로-IL-1β 및 프로-IL-18과 같이 미리 형성된 전 염증성 사이토카인을 최종 활성 형태로 처리하는 것을 촉진합니다. AIM2 인플라마좀의 자극은 바이러스, 박테리아 또는 포유류 기원의 세포질 유리 DNA(cfDNA)에 결합한 후 발생하지만 다른 트리거에 의한 자극은 아닙니다112. 일부 데이터에 따르면 AIM2 인플라마좀은 pSS 환자의 SGEC에서 매우 활성화되어 있으며, 이는 DNase 1의 기능 결함으로 인해 cfDNA가 축적되기 때문일 수 있습니다113. pSS 및 MALT 림프종 환자, 그리고 MALT 림프종 발병 위험이 높은 것으로 판단되는 pSS 환자는 침샘 조직에서 높은 혈청 수준의 cfDNA와 핵 외 DNA 축적이 있으며, 대부분 줄무늬관과 림프구 침윤 사이에 국한되어 있습니다114. 이 세포 외 DNA가 줄무늬관 세포로 운반되면 AIM2 인플라마좀에 중요한 자극이 될 수 있습니다.
NRLP1, NRLP3 또는 NRLP4의 올리고머화는 AIM2에 대해 설명한 것처럼 cfDNA에 의해 유도된 신호와 활성 산소 종, 산화 미토콘드리아 DNA 및 리소좀 파괴와 같은 다양한 DAMP, PAMP 및 기타 트리거에 의해 유도된 신호에 따른 NRLP 전사의 상향 조절로 인해 발생합니다. 다양한 데이터에 따르면 pSS 환자의 침샘은 건강한 사람보다 더 높은 수준의 NLRP3를 발현하며, pSS114,115 환자의 침샘 조직에서도 NRLP3 기계의 구성 요소인 P2X7이 상향 조절되는 것으로 나타났습니다. 그러나 어떤 특정 세포 유형이 상향 조절된 NRLP3를 발현하는지는 불분명하며, 실제로 pSS115에서 NRLP1 및 NRLP4 인플라마좀의 발현도 마찬가지입니다. 그러나 TLR 및 NF-κB 시스템의 역할보다는 덜 잘 알려져 있지만, pSS에서 인플라마좀의 중심적인 역할이 떠오르고 있습니다. 침샘 상피에서 인플라마좀의 활성은 NF-κB 경로를 반영하여 pSS에서 상피의 역할과 면역계와의 상호 작용을 강화합니다. 상향 조절된 인플라마좀은 pSS에서 지속적인 선염증 과정에 기여할 수 있으며, 잠재적인 대체 치료 표적이 될 수 있습니다.
Interferon pathways
Important signalling pathways that contribute to the disruption of the salivary gland epithelium in pSS involve interferons. The interferon family consists of type I (IFNα and IFNβ), type II (IFNγ) and type III (IFNλ) interferons, which have distinct as well as common functions. Interferons stimulate a wide variety of genes important in innate and adaptive immune responses116. In particular, type I interferons create an anti-viral state by promoting immune responses to viruses117. The important role of interferons in the pathogenesis of pSS is reflected by the elevated transcript levels and altered epigenetic regulation of interferon-stimulated genes (ISGs) in both the blood and salivary gland tissue of patients118,119,120. These ISGs are upregulated in both SGECs and striated ducts, in addition to in immune cells121,122, together accounting for the interferon signature of the glands. Indeed, both type I and type II interferon-induced proteins (IFN-induced protein with tetratricopeptide repeats 3 (IFIT3) and guanylate-binding protein 2 (GBP2), respectively) are expressed in ductal epithelial cells, whereas infiltrating immune cells mainly expressed GBP2 (ref.122). In the following subsections, we discuss both the pathways that result in interferon production (for example, PRR signalling and the overexpression of endogenous retroelements), and the pathways that result from stimulation by interferon (for example, pro-inflammatory cytokine production) in the salivary glands.
pSS에서
침샘 상피의 파괴에 기여하는 중요한 신호 경로는
인터페론과 관련이 있습니다.
인터페론 계열은
제1형(IFNα 및 IFNβ), 제2형(IFNγ) 및
제3형(IFNλ) 인터페론으로 구성되며,
이들은 공통된 기능뿐만 아니라 고유한 기능도 가지고 있습니다.
인터페론은
선천성 및 후천성 면역 반응에 중요한 다양한 유전자를 자극합니다116.
특히, 제1형 인터페론은 바이러스에 대한 면역 반응을 촉진하여 항바이러스 상태를 조성합니다117. pSS의 발병에서 인터페론의 중요한 역할은 환자의 혈액 및 침샘 조직에서 인터페론 자극 유전자(ISG)의 전사체 수준 상승과 후성유전학적 조절 변화로 반영됩니다118,119,120. 이러한 ISG는 면역 세포뿐만 아니라 SGEC와 줄무늬관 모두에서 상향 조절되며121,122, 함께 침샘의 인터페론 시그니처를 설명합니다. 실제로, 제1형 및 제2형 인터페론 유도 단백질(각각 IFIT3(4중사슬펩타이드 반복 3)와 구아닐레이트 결합 단백질 2(GBP2)를 가진 IFN 유도 단백질)은 모두 관 상피 세포에서 발현되는 반면, 침윤 면역 세포는 주로 GBP2를 발현합니다(참조.122). 다음 하위 섹션에서는 침샘에서 인터페론이 생성되는 경로(예: PRR 신호 및 내인성 레트로엘레멘트 과발현)와 인터페론에 의한 자극(예: 전 염증성 사이토카인 생성)으로 인한 경로를 모두 논의합니다
Type I interferons
pDCs are a potent source of IFNα within the inflamed salivary gland6. Activated pDCs are able to migrate to the salivary glands in response to chemokines such as CXCL12, CXCR3 ligands and CCR5 ligands123,124. Within the glands, type I interferon production by pDCs can be sustained in the presence of TLR7 ligands, TLR9 ligands and immune complexes of autoantibodies and autoantigens that contain TLR7 ligands in the form of autoantigen-associated RNA125. Although a strong correlation exists between the presence of Ro/La autoantibodies and the expression of ISGs in the blood and tissue of patients with pSS, the sequence of appearance of these features and their contribution to dysfunction of the salivary gland epithelium need further investigation.
In addition to pDCs, epithelial cells themselves can produce type I interferon after stimulation via PRRs, as demonstrated, for example, in studies of mice and of a human submandibular gland cell line36,126. Furthermore, SGECs respond to TLR signalling by producing IFNβ127,128. Interestingly, interferon production can be augmented by endogenous virus-like genomic repeat elements (‘retroelements’)129. The retroelement long interspersed nuclear element 1 (LINE-1) is overexpressed in the minor salivary gland tissue of patients with pSS, probably owing to hypomethylation in the promoter region of the gene encoding LINE-1 (refs129,130). Importantly, LINE-1 and IFNβ are expressed in the ductal epithelium129,130. Mechanistically, LINE-1 retroelements bind to cytosolic nucleic acid sensors, such as RIG-l-like receptors, and consequently trigger type I interferon production131. Vice versa, signalling downstream of extrinsic interferons can modulate the transcription of retroelements. For example, transcriptional modifications of Alu retroelements, induced by interferon signalling, enables this retroelement to bind to intracellular Ro60 (refs129,132). Ro60 probably has an inhibitory role in type I interferon receptor signalling, as data have shown that deletion of Ro60 in an EBV-transformed B cell line increases interferon-induced pro-inflammatory cytokine production and the expression of retroelements132.
Similar to Ro60, Ro52 (later identified as TRIM21) has a multifaceted role in the innate immune response. TRIM21 primarily functions simultaneously as a cytosolic Fc receptor and as an E3 ubiquitin-protein ligase133,134. An important anti-viral role of TRIM21 is binding the Fc part of intracellular antibodies, directing endocytosed antibody-bound viral particles to the proteasome for degradation and activation of innate immune signalling134. Conversely, TRIM21 can also function as a negative regulator of TLR signalling by mediating ubiquitination (protein inactivation) of interferon-regulating factors (IRFs), such as IRF3, IRF5 and IRF7, thereby inhibiting interferon production135,136,137. An inhibitory role for TRIM21 is supported by studies of TRIM21-deficient C57BL/6 mice, which develop features of systemic autoimmunity upon local tissue injury138. Furthermore, the amount of anti-dsDNA antibody production and plasmablast formation is higher in TRIM21-deficient MRL/lpr mice than in wild type MRL/lpr mice, indicating enhanced B cell activation in the absence of TRIM21 (ref.139). Anti-Ro52/TRIM21 antibodies from patients with pSS can specifically recognize the RING domain of the TRIM21 protein. This RING domain is essential for the E3 ubiquitin ligase activity of TRIM21 and anti-Ro52 antibodies could interfere with this activity in vitro140. Although direct interference of anti-Ro52/TRIM21 antibodies (via their antigen-binding fragment (Fab) domain) with intracellular TRIM21 has not been proven in vivo, and is difficult to reconcile, aberrant function of TRIM21 upon uptake of autoantibody-containing immune complexes cannot be ruled out. For example, a study of mice with lupus-like disease provided evidence of possible leakage of IgG antibodies from phagolysosomes containing endocytosed immune complexes into the cytosol, which stimulated the TRIM21-mediated immune responses141. Furthermore, studies of patients with pSS have shown that TRIM21 can be expressed on the cell surface of antigen-presenting cells142, enabling transport of aggregated immunoglobulins and immune complexes into the cell. In conclusion, aberrant expression of retroelements and (indirect) interference of autoantibodies with the regulation of innate immune responses by TRIM21 (and possibly also Ro60) might result in a feed-forward loop of type I interferon activity in ductal epithelial cells, pDCs and B cells (Fig. 1c). A main consequence for the glandular epithelium is that type I interferons enhance the production of pathogenic chemokines and cytokines (for example, CXCL10, IL-7 and BAFF) by ductal epithelial cells, resulting in the recruitment and activation of T cells and B cells and thereby amplifying the inflammatory response58,143,144.
Type II interferons
In addition to type I interferons, type II interferons have also been implicated in pSS-associated salivary gland pathology. IFNγ is mainly produced by natural killer cells and T cells as part of the innate and adaptive immune responses, respectively. In the salivary glands of patients with pSS, IFNγ is abundantly produced by immune cells and the salivary gland tissue often has a mixed type I and type II interferon signature57,122. IFNγ is not only produced by bona fide TH1 cells in the salivary gland but also by T follicular helper (TFH)-like cells that express both programmed cell death protein 1 (PD1) and inducible T cell costimulator (ICOS) and by CCR9+ T helper cells145,146. IFNγ exerts pro-inflammatory effects on SGECs (including both labial and parotid gland-derived SGECs) by stimulating the production of cytokines and chemokines58,143. IFNγ also induces the expression of MHC class II and co-stimulatory molecules on SGECs47,147,148. Collectively, these effects might result in immune cell activation46. IFNγ can also induce FAS-mediated apoptosis and anoikis in SGECs47,48, although an opposite effect was observed in acinar cells and in an immortalized salivary gland ductal cell line, where IFNγ induced apoptotic resistance25,46. IFNγ has further been implicated in reducing the integrity of the glandular epithelium (that is, the tight junction barrier function), as has been observed in minor salivary gland tissue from patients with pSS106. Together, these results suggest that IFNγ negatively affects SGECs in various ways, dependent on the glandular cell type, and might contribute to salivary gland dysfunction in patients with SS.
Type III interferons
Type III interferon has been added to the interferon family more recently149. Downstream effector genes of type III interferons are similar to those downstream of type I interferons and the functions of both interferon pathways largely overlap. However, an important difference is restricted expression of the type III interferon receptor by epithelial cells of mucosal surfaces and pDCs (reviewed elsewhere150). In the ductal epithelium of patients with pSS, IFNλ2 is upregulated compared with individuals with non-Sjögren syndrome sicca symptoms151. Similar to type I and type II interferons, IFNλ can promote the production of cytokines (for example, IL-7, BAFF and CXCL10) by the salivary gland epithelium58,151. Whether type III interferons notably contribute to salivary gland pathology, either independent or in synergy with other interferons, remains to be elucidated.
Epithelial cell–lymphocyte crosstalk
In healthy salivary glands, a small number of lymphocytes (in the form of TRM cells) are present for immune surveillance60. By comparison, in pSS, CD8+ T cells are located in close association with acini or ducts with a disrupted basal lamina and CD4+ T cells are located in association with the ducts37. B cells can also infiltrate the ductal epithelium, a phenomenon that is specific to pSS10. Such histological findings suggest that crosstalk between the salivary gland epithelium and lymphocytes has a critical role in salivary gland pathology. In this section, we focus on crosstalk between epithelial cells of the salivary glands and lymphocytes (specifically, CD4+ T cells and intraepithelial B cells) in pSS.
건강한 침샘에서는 면역 감시를 위해
소수의 림프구(TRM 세포 형태)가 존재합니다60.
이에 비해,
pSS에서는
CD8+ T 세포가 기저층이 파괴된 아시니 또는 덕관과 밀접하게 연관되어 있고,
CD4+ T 세포가 덕관과 연관되어 있습니다37.
B 세포는 또한
관 상피에 침투할 수 있는데,
이는 pSS10에 특이적인 현상입니다.
이러한 조직학적 결과는
침샘 상피와 림프구 사이의 누화가
침샘 병리에서 중요한 역할을 한다는 것을 시사합니다.
이 섹션에서는
침샘 상피 세포와
림프구(특히, CD4+ T 세포와 상피내 B 세포) 사이의 누화에 초점을 맞춰
pSS에 대해 설명합니다.
Crosstalk with CD4+ T cells
The presence of MHC class II in combination with CD80 and CD86 molecules on the surface of SGECs upon immune activation (for example, following stimulation with IFNγ) infers the ability of the epithelial cells to process antigens for presentation to CD4+ T cells52,152. In the presence of T cell receptor stimulation, constitutive expression of CD86 by SGEC lines could promote CD4+ T cell proliferation by engaging with CD28 (ref.153). SGECs from patients with pSS are also capable of expressing other co-stimulatory molecules such as CD40 and ICOS ligand (ICOSL)49,152,154. In SGECs from patients with pSS, CD40 is spontaneously expressed (at higher levels than in SGECs from patients with sicca symptoms but not diagnosed with pSS) and this expression can be enhanced in the presence of IFNγ or IL-1β148. Ligation of CD40 on SGECs activates the non-canonical NF-κB pathway, resulting in pro-inflammatory cytokine production and either FAS-dependent apoptosis or apoptotic resistance49,155, probably depending on the epithelial cell type and microenvironmental cues. However, although SGECs seem to express all molecules required for antigen presentation, no formal proof is yet available showing that human SGECs actively present antigen to T cells via cognate interaction in vivo.
In addition to the provision of co-stimulatory signals to T cells, SGECs can produce several cytokines and chemokines, as shown for both labial and parotid gland-derived SGECs. These can include chemokines that attract T cells (for example, CCL19 and CXCL10), as well as cytokines that promote local T cell proliferation and/or differentiation56,58,143,154. For example, SGECs can produce IL-6, a pleiotropic cytokine that can promote the differentiation of TFH cells (as well as B cells)156. IL-6 production by SGECs, together with ICOSL expression on these SGECs, can support the differentiation of TFH cells in vitro154. This finding is notable as the expansion of both glandular and circulating TFH cells in pSS is associated with more severe disease, that is, increased ESSDAI scores, IgG antibody production and ectopic lymphoid structure formation146,157,158.
Another potentially relevant cytokine for salivary gland epithelium–T cell crosstalk is IL-7. This cytokine is produced by non-haematopoietic cells and has an important role in T cell homeostasis159. Although a histological study in minor salivary glands found that IL-7 was mostly expressed by cells with a fibroblast morphology in the interstitium, and not by acinar or ductal cells160, more recent findings suggest that IL-7 is also expressed by SGECs58,121. Cultured SGECs from patients with pSS produce IL-7 after stimulation with poly(I:C), IFNα or IFNγ58. Data from the B6.NOD‐Aec mouse model of pSS suggest that IL-7 also has an indirect role in salivary gland pathology, by enhancing TH1 responses and IFNγ‐dependent CXCL10 expression in the salivary gland161. Thus, activation of TH1 cells by IL-7 can propagate IFNγ production, creating a pro-inflammatory loop. Although the epithelial source of IL-7 production (for example, ductal or acinar cells) has not been studied, various data suggest that the IL-7–IL-7Rα axis contributes to T cell-driven autoimmune pathology in pSS. For example, the amount of IL-7R-positive T cells in the salivary glands of patients with pSS correlates with IL-7 expression and the severity of sialadenitis162. In addition, CCR9+ T helper cells typically express high levels of the IL-7 receptor and stimulation of these cells with IL-7 induces IFNγ, IL-17 and IL-21 production, thereby also supporting B cell activation145.
면역 활성화 시(예: IFNγ 자극 후) SGEC 표면에 CD80 및 CD86 분자와 결합된 MHC 클래스 II의 존재는 상피 세포가 항원을 처리하여 CD4+ T 세포에 제시할 수 있는 능력을 유추할 수 있습니다52,152. T 세포 수용체 자극이 있는 경우, SGEC주에 의한 CD86의 구성적 발현은 CD28과 결합하여 CD4+ T 세포 증식을 촉진할 수 있습니다(참조.153). pSS 환자의 SGEC는 또한 CD40 및 ICOS 리간드(ICOSL)49,152,154와 같은 다른 공동 자극 분자를 발현할 수 있습니다. pSS 환자의 SGEC에서 CD40은 자발적으로 발현되며(시카 증상이 있지만 pSS로 진단되지 않은 환자의 SGEC보다 높은 수준에서), 이 발현은 IFNγ 또는 IL-1β148이 존재할 때 강화될 수 있습니다. SGEC에서 CD40의 결합은 비정식적인 NF-κB 경로를 활성화하여 염증성 사이토카인을 생성하고 상피 세포 유형과 미세 환경 신호에 따라 FAS 의존적 세포 사멸 또는 세포 사멸 저항을 유발합니다49,155. 그러나 SGEC가 항원 제시를 위해 필요한 모든 분자를 발현하는 것으로 보이지만, 인간 SGEC가 생체 내에서 상동 상호작용을 통해 T세포에 항원을 적극적으로 제시한다는 공식적인 증거는 아직 없습니다.
음순 및 이하선 유래 SGEC 모두에서 볼 수 있듯이 SGEC는 T세포에 공동 자극 신호를 제공하는 것 외에도 여러 사이토카인과 케모카인을 생성할 수 있습니다. 여기에는 T 세포를 유인하는 케모카인(예: CCL19 및 CXCL10)과 국소 T 세포 증식 및/또는 분화를 촉진하는 사이토카인56,58,143,154이 포함될 수 있습니다. 예를 들어, SGEC는 TFH 세포(B 세포뿐만 아니라)156의 분화를 촉진할 수 있는 형질 전환성 사이토카인인 IL-6를 생성할 수 있습니다. SGEC에 의한 IL-6 생산은 이러한 SGEC의 ICOSL 발현과 함께 시험관 내 TFH 세포의 분화를 지원할 수 있습니다154. 이 발견은 pSS에서 선상 및 순환 TFH 세포의 확장이 더 심각한 질병, 즉 ESSDAI 점수 증가, IgG 항체 생산 및 이소성 림프 구조 형성과 관련이 있기 때문에 주목할 만합니다146,157,158.
침샘 상피-T 세포 누화에 잠재적으로 관련된 또 다른 사이토카인은 IL-7입니다. 이 사이토카인은 비조혈 세포에서 생성되며 T 세포 항상성 유지에 중요한 역할을 합니다159. 소타액선의 조직학적 연구에 따르면 IL-7은 주로 간질에서 섬유아세포 형태를 가진 세포에 의해 발현되고 선상 또는 관상 세포에는 발현되지 않는 것으로 밝혀졌지만160, 최근의 연구 결과에 따르면 IL-7은 SGEC에서도 발현되는 것으로 나타났습니다58,121. pSS 환자에서 배양한 SGEC는 폴리(I:C), IFNα 또는 IFNγ58로 자극한 후 IL-7을 생성합니다. pSS의 B6.NOD-Aec 마우스 모델 데이터에 따르면 IL-7은 침샘에서 TH1 반응과 IFNγ 의존성 CXCL10 발현을 강화함으로써 침샘 병리에도 간접적인 역할을 하는 것으로 나타났습니다161. 따라서 IL-7에 의한 TH1 세포의 활성화는 IFNγ 생산을 전파하여 염증성 루프를 생성할 수 있습니다. IL-7 생산의 상피 공급원(예: 덕트 또는 선상 세포)은 연구되지 않았지만, 다양한 데이터에 따르면 IL-7-IL-7Rα 축이 pSS에서 T 세포 주도 자가 면역 병리에 기여하는 것으로 나타났습니다. 예를 들어, pSS 환자의 침샘에 있는 IL-7R 양성 T 세포의 양은 IL-7 발현 및 시알라덴염의 중증도와 상관관계가 있습니다162. 또한, CCR9+ T 헬퍼 세포는 일반적으로 높은 수준의 IL-7 수용체를 발현하며 이러한 세포를 IL-7로 자극하면 IFNγ, IL-17 및 IL-21 생성을 유도하여 B 세포 활성화도 지원합니다145.
Crosstalk with B cells
Available evidence indicates that the salivary gland epithelium is able to promote B cell hyperactivity in pSS and forms a niche for autoantibody-producing plasma cells. Chronic B cell hyperactivity in the salivary glands is demonstrated, amongst others findings, by the frequent occurrence of ectopic lymphoid structures in the glandular tissue, which might even contain germinal centres7, and by the high risk of patients with pSS developing B cell non-Hodgkin lymphomas in these glands163. Several mechanisms underlying B cell hyperactivity in pSS have been described and reviewed elsewhere8,9. In this section, we focus on the crosstalk between epithelial cells and B cells and highlight novel insights into the development of LELs and MALT lymphoma in pSS.
이용 가능한 증거에 따르면
침샘 상피는
pSS에서 B 세포 과잉 활동을 촉진할 수 있으며
자가 항체 생산 형질 세포를 위한 틈새를 형성할 수 있습니다.
침샘 조직에서 이소성 림프 구조가 빈번하게 발생하고
심지어 배아 중심을 포함할 수도 있는 것으로 밝혀진
점7과 침샘에서 B세포 비호지킨 림프종이 발생할 위험이 높은 pSS 환자163을 통해
침샘의 만성 B세포 과활동성이 입증되었습니다.
pSS에서
B 세포 과잉 활동의 기저에 있는 몇 가지 메커니즘은
이 섹션에서는
상피 세포와 B 세포 사이의 누화에 초점을 맞추고
pSS에서 LEL 및 MALT 림프종의 발병에 대한 새로운 통찰력을 강조합니다.

B cell activation by the salivary gland epithelium
Epithelial cells can contribute to B cell activity through the production of cytokines, including IL-6 and BAFF121,154,164. Both IL-6 and BAFF are involved in B cell activation and homeostasis, and BAFF is critically important for B cell survival156,165,166. Previous reports have shown that type I interferon is an important promoter of BAFF production by SGECs6,144,167. The expression of interferon-inducible genes was indeed increased in EpCAM-positive epithelial cells in biopsy samples from patients with pSS compared with biopsy samples from individuals with non-Sjögren syndrome sicca symptoms121. In one study that employed co-cultures of B cells and SGECs, poly(I:C) stimulated the production of soluble factors by SGECs from patients with pSS, which enhanced the survival of the B cells121. Surprisingly, blockade of a proliferation-inducing ligand (APRIL) or BAFF alone had no effect on B cell survival121, suggesting that other factors might be responsible for enhanced B cell survival under this experimental condition.
The epithelium not only affects B cells, but B cells can also, vice versa, have effects on epithelial cells. For example, B cells can induce epigenetic modifications in SGECs168. B cell-induced transcriptional changes in epithelial cells might contribute to the formation of LELs, as discussed in the next section.
상피 세포는
IL-6 및 BAFF를 포함한 사이토카인 생성을 통해
B 세포 활동에 기여할 수 있습니다121,154,164.
IL-6와 BAFF는
모두 B 세포 활성화와 항상성에 관여하며,
BAFF는 B 세포 생존에 매우 중요합니다156,165,166.
이전 보고에 따르면
제1형 인터페론은 SGEC에 의한 BAFF 생성의 중요한 촉진제입니다6,144,167.
인터페론 유도 유전자의 발현은
실제로 비쇼그렌증후군 시카 증상이 없는 사람의 생검 샘플과 비교하여
pSS 환자의 생검 샘플에서 EpCAM 양성 상피 세포에서 증가했습니다121.
B 세포와 SGEC의 공동 배양을 사용한 한 연구에서
폴리(I:C)는
pSS 환자의 SGEC에서 용해성 인자의 생성을 자극하여
B 세포의 생존을 향상시켰습니다121. 놀
랍게도
증식 유도 리간드(APRIL) 또는
BAFF만 차단해도 B 세포 생존에 영향을 미치지 않았으며121,
이는 이 실험 조건에서 다른 요인이 B 세포 생존을 향상시키는 원인이 될 수 있음을 시사합니다.
상피는
B 세포에 영향을 미칠 뿐만 아니라, B
세포가 상피 세포에 영향을 미칠 수도 있습니다.
예를 들어,
B 세포는 SGECs168에서 후성유전학적 변형을 유도할 수 있습니다.
다음 섹션에서 설명하는 것처럼
상피 세포에서
B 세포가 유도하는 전사적 변화는 LEL 형성에 기여할 수 있습니다.
Lymphoepithelial lesion development
The intimate relationship between the salivary gland epithelium and B cells in pSS is most clearly demonstrated by the presence of LELs (Fig. 2). These LELs develop exclusively in the striated ducts and are a characteristic histological feature of pSS11. LELs are formed in close association with the periductal infiltrate10,11. Although these lesions are found in both the minor and major salivary glands, they are more pronounced in the major (parotid) glands10. LELs consist of hyperplastic duct cells in the epithelial cell lining and infiltrating lymphocytes within the contour of the basement membrane11. This hyperplasia might result in complete occlusion of the ducts, potentially contributing to hyposalivation. Evidence suggests that LELs nearly always harbour B cells in between the hyperplastic basal cells and that a small proportion of the striated ducts without hyperplasia already contain some B cells10. In addition, some intraepithelial T cells are also found in LELs; however, unlike B cells, which are completely absent from the salivary gland ducts of patients with non-Sjögren syndrome sicca symptoms, the presence of intraepithelial T cells is not specific to pSS10. Together these findings suggest that LEL formation starts with the infiltration of B cells into the ductal epithelium. The severity of the LEL (stage of duct occlusion) increases with the absolute and relative number of intraepithelial B cells10. How B cells are attracted into the epithelium is not fully understood, but the expression of CXCR3 probably has an important role, as intraepithelial B cells express CXCR3 and the salivary gland epithelium produces CXCL10 and other CXCR3 ligands upon activation143. These intraepithelial B cells, which are probably already activated before they migrate to the epithelium, can expand locally, as demonstrated by the high proportion of Ki67-staining cells and the expansion of clonal B cells within the striated ducts169,170. The latter finding suggests that additional activation and proliferation signals might be derived from epithelial cells, and possibly also from other intraepithelial immune cells, such as T cells and dendritic cells.
림프상피 병변 발생
pSS에서
침샘 상피와 B 세포 사이의 밀접한 관계는
LEL의 존재로 가장 명확하게 입증됩니다(그림 2).
이러한
LEL은
줄무늬 관에서만 발생하며 pSS11의 특징적인 조직학적 특징입니다.
LEL은 관 주위 침윤과 밀접하게 연관되어 형성됩니다10,11.
이러한 병변은
소타액선과 대타액선 모두에서 발견되지만,
대타액선(이하선)에서 더 두드러지게 나타납니다10.
LEL은
상피 세포 내벽의 과형성 관 세포와 기저막 윤곽 내 림프구 침윤으로 구성됩니다11.
이러한 과형성은
덕트의 완전한 폐색을 초래하여
잠재적으로 타액 분비 저하를 일으킬 수 있습니다.
증거에 따르면 LEL은
거의 항상 과형성 기저 세포 사이에
B 세포를 보유하고 있으며,
과형성이 없는 줄무늬 관의 일부에는 이미 일부 B 세포가 포함되어 있습니다10.
또한 일부 상피 내 T 세포도
LEL에서 발견되지만 비쇼그렌 증후군 시카 증상이 있는 환자의 침샘 관에는 완전히 없는 B 세포와는 달리 상피 내 T 세포의 존재는 pSS10에 특이적이지 않습니다.
이러한 결과를 종합해 볼 때
LEL 형성은
B세포가 관 상피에 침윤하는 것으로 시작됩니다.
LEL(관 폐색 단계)의 심각도는
상피내 B 세포의 절대적 및 상대적 수에 따라 증가합니다10.
B 세포가 상피로 유인되는 방법은
완전히 이해되지 않았지만
상피내 B 세포가 CXCR3를 발현하고
침샘 상피가 활성화되면 CXCL10 및 기타 CXCR3 리간드를 생성하므로 CXCR3의 발현이 중요한 역할을 할 수 있을 것으로 생각됩니다143. 상피로 이동하기 전에 이미 활성화된 것으로 추정되는 이러한 상피내 B 세포는 줄무늬관 내에서 높은 비율의 Ki67 염색 세포와 클론 B 세포의 확장으로 입증된 것처럼 국소적으로 확장될 수 있습니다169,170. 후자의 발견은 추가적인 활성화 및 증식 신호가 상피 세포에서 파생될 수 있으며, 아마도 T 세포 및 수지상 세포와 같은 다른 상피 내 면역 세포에서도 파생될 수 있음을 시사합니다.
Fig. 2: Lymphoepithelial lesions in the salivary glands of a patient with primary Sjögren syndrome.
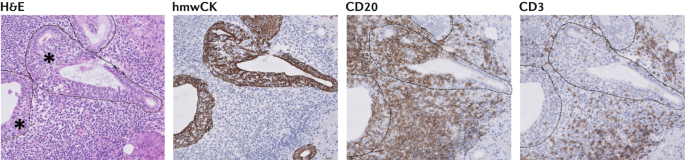
Consecutive sections of parotid gland tissue from a patient with primary Sjögren syndrome are shown. Lymphoepithelial lesions are indicated by an asterisk on the haematoxylin and eosin (H&E)-stained section. Consecutive sections were stained with antibodies to reveal either epithelial cells (using antibodies against high molecular weight cytokeratin (hmwCK)), B cells (using antibodies against CD20) or T cells (using antibodies against CD3). B cells dominate the lymphoepithelial lesions, whereas T cells are rarely detected within these structures. Image courtesy of M.S. van Ginkel and B. van der Vegt.
원발성 쇼그렌 증후군 환자의 귀밑샘 조직 연속 단면이 표시되어 있습니다. 림프상피 병변은 헤마톡실린 및 에오신(H&E) 염색 섹션에 별표로 표시되어 있습니다. 연속된 섹션을 항체로 염색하여 상피 세포(고분자량 사이토케라틴(hmwCK) 항체 사용), B 세포(CD20 항체 사용) 또는 T 세포(CD3 항체 사용)를 확인했습니다. 림프상피 병변은 B 세포가 지배적인 반면, T 세포는 이러한 구조 내에서 거의 발견되지 않습니다. M.S. van Ginkel 및 B. van der Vegt 이미지 제공.
Interestingly, the majority, if not all, of the intraepithelial B cells in the minor (labial) and major (parotid) glands express the inhibitory Fc-receptor like 4 (FcRL4) protein (Fig. 3), which is abundantly expressed by MALT lymphoma B cells of patients with pSS169, and is also expressed on activated B cells171. Gene expression profiling of FcRL4+ B cells from parotid gland tissue of patients with pSS has further revealed that these cells express transcripts of chronic activation markers, such as T-bet and CD11c172. T-bet expression might be the result of a type II interferon response, as the expression of IFNGR1 and IL27RA is upregulated in FcRL4+ B cells172. Indeed, signalling downstream of the IFNγ receptor and IL-27 receptor in B cells induces the expression of T-bet, via STAT1, and such signalling pathways have been implicated in the development of autoimmunity in mice173,174,175,176. FcRL4+ B cells also have increased expression of TACI (encoding the receptor for BAFF and APRIL), CXCR3, CCR5, NF-κB-related genes (NFKB1 and MAP3K14) and IL6, and reduced expression of negative regulators of NF-κB (NFKBIA and NFKBID, encoding IκBα and IκBNS, respectively), CD40 and CXCR5 compared with FcRL4− glandular B cells. These phenotypical characteristics suggest that FcRL4+ B cells are activated cells that persist in inflamed tissue and are sustained by pro-inflammatory cytokines (in particular IFNγ, IL-27, BAFF and APRIL) and CD40-independent stimulation.
흥미롭게도,
소(순순샘) 및 대(이하선)의 상피내 B 세포의 전부는 아니더라도
대다수가 억제성 Fc 수용체 유사 4(FcRL4) 단백질을 발현하는데(그림 3),
이는 pSS 환자의 MALT 림프종 B 세포에서 풍부하게 발현되며169
활성화된 B 세포에서도 발현됩니다171.
pSS 환자의 이하선 조직에서 추출한
FcRL4+ B 세포의 유전자 발현 프로파일링 결과,
이 세포는 T-bet 및 CD11c172와 같은 만성 활성화 마커의 전사를 발현하는 것으로 밝혀졌습니다.
IFNGR1 및 IL27RA의 발현이 FcRL4+ B 세포172에서 상향 조절되기 때문에
T-bet 발현은 유형 II 인터페론 반응의 결과일 수 있습니다.
실제로 B 세포에서 IFNγ 수용체와 IL-27 수용체의 하류 신호는 STAT1을 통해 T-bet의 발현을 유도하며, 이러한 신호 경로는 생쥐의 자가 면역 발달과 관련이 있습니다173,174,175,176. 또한 FcRL4+ B 세포는 FcRL4- 선상 B 세포에 비해 TACI (BAFF 및 APRIL 수용체 암호화), CXCR3, CCR5, NF-κB 관련 유전자(NFKB1 및 MAP3K14) 및 IL6의 발현이 증가하고, NF-κB의 음성 조절자(각각 IκBα 및 IκBNS 암호화), CD40 및 CXCR5의 발현은 감소되어 있습니다. 이러한 표현형적 특성은 FcRL4+ B 세포가 염증 조직에서 지속되고 전 염증성 사이토카인(특히 IFNγ, IL-27, BAFF 및 APRIL) 및 CD40 독립적 자극에 의해 지속되는 활성화된 세포라는 것을 시사합니다.
Fig. 3: Interactions between FcRL4+ B cells and the ductal epithelium in primary Sjögren syndrome.
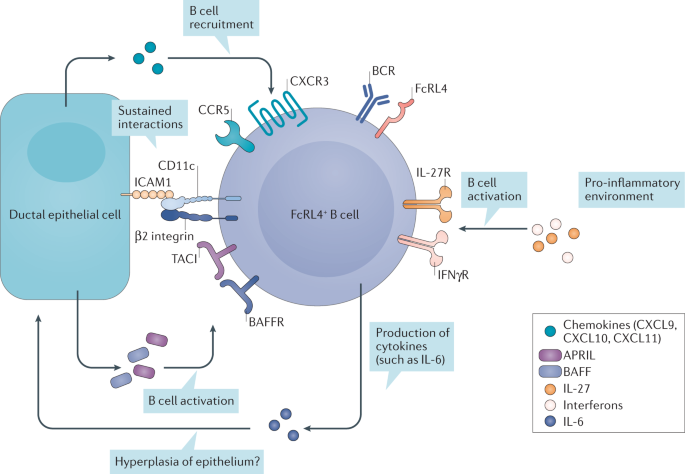
a | Activated epithelial cells secrete CXCL10 and attract Fc-receptor like 4-positive (FcRL4+) B cells. These cells are further activated by B cell-activating factor (BAFF) and a proliferation-inducing ligand (APRIL), secreted by epithelial cells, and other stimuli from the pro-inflammatory environment. Upon activation, FcRL4+ B cells express CD11c, which can form an integrin together with the β2 integrin. This integrin can bind to intercellular adhesion molecule 1 (ICAM1) on epithelial cells and sustain their interaction. The production of IL-6 and possibly also other pro-inflammatory cytokines by FcRL4+ B cells might result in hyperplasia of the epithelium.
활성화된 상피 세포는 CXCL10을 분비하고 Fc-수용체 유사 4 양성(FcRL4+) B 세포를 끌어들입니다. 이러한 세포는 상피 세포에서 분비되는 B 세포 활성화 인자(BAFF)와 증식 유도 리간드(APRIL), 그리고 염증 유발 환경의 다른 자극에 의해 더욱 활성화됩니다. 활성화되면 FcRL4+ B 세포는 CD11c를 발현하여 β2 인테그린과 함께 인테그린을 형성할 수 있습니다. 이 인테그린은 상피 세포의 세포 간 접착 분자 1(ICAM1)에 결합하여 상호 작용을 유지할 수 있습니다. FcRL4+ B 세포에 의한 IL-6 및 기타 염증성 사이토카인의 생성은 상피의 과증식을 초래할 수 있습니다.y토카인(특히 IFNγ, IL-27, BAFF 및 APRIL) 및 CD40 독립적 자극을 유발할 수 있습니다.
Glandular FcRL4+ B cells resemble double-negative (IgD−CD27−) B cells (called DN2 B cells), a cell type also characterized by T-bet and CD11c expression that is associated with the pathogenesis of SLE177,178. In patients with SLE, CD11c+T-bet+ B cells are poised to differentiate into plasmablasts outside of the follicles177,178. However, glandular FcRL4+ B cells in patients with pSS lack the expression of plasma cell markers, such as B lymphocyte-induced maturation protein 1 (BLIMP1; also known as PRDM1)169. Available evidence indicates that binding of soluble IgA to FcRL4 results in a switch from B cell receptor (BCR)-mediated activation to TLR-mediated activation179. This functional switch of the B cells probably results in enhanced NF-κB pathway activation and cytokine production. Secreted cytokines of intraepithelial B cells, such as IL-6, might affect epithelial homeostasis and lead to the proliferation of epithelial cells and ultimately to LEL formation. Direct proof that B cells are involved in LEL formation comes from trials of rituximab (a B cell-depleting agent) in patients with pSS. Treatment of patients with pSS with rituximab not only led to a strong reduction of B cells within the salivary gland, including B cells located within the epithelium, but concomitantly also led to a reduction in the severity of the LELs and the partial restoration of the epithelium after 12 weeks of treatment180. Notably, salivary gland B cell depletion was more variable at week 24 in this study181, suggesting that in some patients, B cells have started to repopulate the glands at this time point. Although rituximab treatment had clear effects on salivary gland histopathology, in particular at early time points, these effects unfortunately did not translate into rituximab having a proven clinical efficacy in pSS182,183,184.
The effects of B cell depletion therapy on the epithelium using rituximab, together with the cytokine profiles of intraepithelial B cells and SGECs, suggest that some crosstalk occurs between B cells and striated duct epithelial cells, leading to sustained activation and proliferation of both cell types. Upregulation of CXCR3 and CD11c, and possibly also other integrins, on the B cell surface might have a role in keeping the cells within the epithelial layer. However, in addition to being present in ductal areas, B cell clones are also present, to some extent, in the periductal areas, suggesting that some cellular exchange occurs between these areas170.
The lack of mRNA and protein expression of plasma cell markers by glandular FcRL4+ B cells suggest that these cells rarely differentiate into plasmablasts and instead the cells are maintained in a state of chronic activation and continue to proliferate at a high rate169,172. These cells might undergo extrafollicular somatic hypermutation; indeed, activation induced deaminase (AID), the enzyme responsible for initiating diversity in immunoglobulin genes during somatic hypermutation (and class switching), is expressed by FcRL4+ B cells in the tonsils (and possibly also in salivary glands)185. Notably, AID expression, which can be induced by T-bet186, might not only result in hypermutation of immunoglobulin variable region genes, but also in off-target mutations (that is, non-immunoglobulin genes)187. Thus, a pathogenic combination of increased NF-κB activation, pro-survival factors, proliferation and possibly also AID expression in FcRL4+ intraepithelial B cells could make these cells prone to neoplastic changes and promote progression towards MALT lymphoma, as discussed in the next section.
선상 FcRL4+ B 세포는
이중 음성(IgD-CD27-) B 세포(DN2 B 세포라고 함)와 유사하며,
이 세포 유형도 SLE의 발병과 관련된 T-bet 및 CD11c 발현이 특징입니다177,178.
SLE 환자에서
CD11c+T-bet+ B 세포는
난포 외부에서 형질 모세포로 분화할 준비가 되어 있습니다177,178.
그러나 pSS 환자의 선상 FcRL4+ B 세포는 B 림프구 유도 성숙 단백질 1(BLIMP1; PRDM1이라고도 함)169와 같은 형질 세포 마커의 발현이 부족합니다. 이용 가능한 증거에 따르면 가용성 IgA와 FcRL4의 결합은 B 세포 수용체(BCR) 매개 활성화에서 TLR 매개 활성화로의 전환을 초래합니다179. 이러한 B 세포의 기능적 전환은 아마도 NF-κB 경로 활성화와 사이토카인 생성을 강화하는 결과를 가져올 것입니다. 상피 내 B 세포에서 분비되는 IL-6와 같은 사이토카인은 상피 항상성에 영향을 미치고 상피 세포의 증식을 유도하여 궁극적으로 LEL 형성을 유도할 수 있습니다. B세포가 LEL 형성에 관여한다는 직접적인 증거는 pSS 환자를 대상으로 한 리툭시맙(B세포 파괴제)의 임상시험에서 나왔습니다. pSS 환자를 리툭시맙으로 치료한 결과 상피 내에 위치한 B 세포를 포함하여 침샘 내 B 세포가 크게 감소했을 뿐만 아니라 치료 12주 후 LEL의 중증도가 감소하고 상피가 부분적으로 회복되는 결과를 가져왔습니다180. 특히, 이 연구에서 24주차에 침샘 B 세포 고갈이 더 다양하게 나타났는데181, 이는 일부 환자에서 이 시점에 B 세포가 침샘에 다시 채워지기 시작했음을 시사합니다. 리툭시맙 치료는 특히 초기 시점에서 침샘 조직 병리학에 분명한 영향을 미쳤지만, 안타깝게도 이러한 효과가 pSS182,183,184에서 입증된 임상적 효능으로 이어지지는 못했습니다.
리툭시맙을 사용한 상피에 대한 B 세포 고갈 치료의 효과와 상피 내 B 세포 및 SGEC의 사이토카인 프로파일은 B 세포와 줄무늬관 상피 세포 사이에 일부 누화가 발생하여 두 세포 유형의 지속적인 활성화와 증식으로 이어진다는 것을 시사합니다. B 세포 표면에서 CXCR3와 CD11c, 그리고 아마도 다른 인테그린의 상향 조절은 세포를 상피층 내에 유지하는 데 중요한 역할을 할 수 있습니다. 그러나 B 세포 클론은 관 영역에 존재할 뿐만 아니라 관 주위 영역에도 어느 정도 존재하며, 이는 이들 영역 간에 일부 세포 교환이 발생한다는 것을 시사합니다170.
선상 FcRL4+ B 세포에 의한 형질 세포 마커의 mRNA 및 단백질 발현 부족은 이러한 세포가 형질 모세포로 거의 분화하지 않고 대신 세포가 만성 활성화 상태로 유지되고 빠른 속도로 계속 증식한다는 것을 시사합니다169,172. 실제로 체세포 과돌연변이(및 클래스 전환) 동안 면역글로불린 유전자의 다양성을 개시하는 효소인 활성화 유도 탈아미나제(AID)는 편도선(및 침샘)의 FcRL4+ B 세포에서발현됩니다185. 특히, T-bet186에 의해 유도될 수 있는 AID 발현은 면역글로불린 가변 영역 유전자뿐만 아니라 표적 외 돌연변이(즉, 비면역글로불린 유전자)187의 과돌연변이도 초래할 수 있습니다. 따라서, 다음 섹션에서 설명하는 것처럼 FcRL4+ 상피내 B 세포에서 NF-κB 활성화, 친생존 인자, 증식 및 AID 발현 증가의 병원성 조합은 이러한 세포가 종양 변화를 일으키기 쉽고 MALT 림프종으로의 진행을 촉진할 수 있습니다.
.
MALT lymphoma and rheumatoid factor-expressing B cells
Non-Hodgkin lymphomas arise in 5–10% of patients with pSS, and the majority of these lymphomas are MALT lymphomas that develop preferentially within the parotid glands163. A hallmark of salivary gland MALT lymphomas is their association with LELs, highlighting the dependency of these lymphomas on epithelial cells. MALT lymphomas are considered to arise as a consequence of chronic B cell stimulation and, in pSS, these neoplastic cells often express stereotypic rheumatoid factors that have a high affinity for the Fc region of IgG antibodies188,189,190. In patients with pSS, non-neoplastic rheumatoid factor-expressing B cells are enriched within the circulating CD21−/low B cell population191, a phenotype that is associated with impaired BCR stimulation (similar to FcRL4+ B cells) and frequent polyreactivity or self-reactivity192,193. The phenotype of CD21−/low B cells partially overlaps with DN2 B cells194. Notably, IL-21 and TLR7 ligands together promote the expansion and differentiation of DN2 B cells178 and are both readily available in the inflamed salivary gland in patients with pSS146. While the frequency of rheumatoid factor-expressing B cells in the inflamed salivary glands of patients with pSS without MALT lymphoma seems to be low195,196, these cells might expand after dual engagement of the BCR and TLRs with immune complexes that contain RNA-associated autoantigens197. Although the role of the BCR in lymphomatous escape remains enigmatic, rheumatoid factor expressed on the surface of B cells might simply trap immune complexes of autoantibodies and RNA-associated autoantigens, which stimulate TLRs, with or without further BCR-mediated activation of the cells. In the inflamed salivary gland, these immune complexes might provide chronic B cell stimulation and a strong selection advantage of incidental stereotypic rheumatoid factor-expressing B cells. Simultaneous engagement of FcRL4 on these B cells might inhibit differentiation towards plasma cells and in turn enable ongoing proliferation.
Rheumatoid factor-expressing B cells frequently express IGHV1-69, a immunoglobulin heavy-chain variable region variant that can be detected by the monoclonal antibody G6 (ref.198). Compared with healthy individuals, patients with pSS and cryoglobulinaemic vasculitis have an increased frequency of G6-positive memory B cells on the periphery, which exclusively express kappa light chains191. Interestingly, all MALT lymphomas that have rheumatoid factor activity are IgM clones with kappa light chains188,190, suggesting that G6+ B cells might form a pool of potential precursor cells to MALT lymphomas. Furthermore, researchers have shown that G6+ B cells incidentally contain somatic mutations in genes involved in B cell proliferation, such as TNFAIP3 (ref.191). A specific germline polymorphism of TNFAIP3 is associated with MALT lymphoma development in pSS199, underlining the importance of intact NF-κB regulation in preventing B cell dysregulation. Variations in B cell-regulating genes, such as TNFAIP3, might result in the escape of autoreactive cells from tolerance checkpoints191. Although the presence of G6+ B cells that contain lymphoma-associated mutations in the peripheral blood of patients with pSS has not been linked directly to MALT lymphoma development, these cells might migrate to the salivary glands, where they could be further activated.
Taken together, an attractive hypothesis is that the highly proliferative, intraepithelial FcRL4+ B cells are the glandular counterparts of DN2 B cells, incidentally displaying rheumatoid factor reactivity and forming a pool of lymphoma precursor cells in the salivary glands of patients with pSS. The notion that FcRL4+ B cells are more frequently observed in parotid glands compared with labial glands might explain the preferential development of MALT lymphoma in parotid glands169. Although the critical steps towards neoplastic dysregulation of glandular B cells remain unknown, somatic mutations within and outside of the immunoglobulin variable region genes are probably involved. We postulate that therapeutic targeting of intraepithelial B cells might prevent the development of MALT lymphoma in patients with pSS.
MALT 림프종 및 류마티스 인자 발현 B 세포
비호지킨 림프종은
pSS 환자의 5~10%에서 발생하며,
이러한 림프종의 대부분은
귀밑샘에서 우선적으로 발생하는 MALT 림프종입니다 163.
침샘 MALT 림프종의 특징은 상피 세포에 대한 이러한 림프종의 의존성을 강조하는 LEL과의 연관성입니다. MALT 림프종은 만성 B 세포 자극의 결과로 발생하는 것으로 간주되며, pSS에서 이러한 종양 세포는 종종 IgG 항체의 Fc 영역에 높은 친화력을 갖는 고정 관념의 류마티스 인자를 발현합니다188,189,190. pSS 환자에서 비종양성 류마티스 인자 발현 B 세포는 순환하는 CD21-/저 B 세포 집단191 내에서 풍부하며, 이는 BCR 자극 장애(FcRL4+ B 세포와 유사) 및 빈번한 다반응성 또는 자가 반응성과 관련된 표현형입니다192,193. CD21-/낮은 B 세포의 표현형은 DN2 B 세포와 부분적으로 겹칩니다194. 특히 IL-21과 TLR7 리간드는 함께 DN2 B 세포의 확장 및 분화를 촉진하며178, 둘 다 pSS146 환자의 염증 침샘에서 쉽게 구할 수 있습니다. MALT 림프종이 없는 pSS 환자의 염증 침샘에서 류마티스 인자를 발현하는 B 세포의 빈도는 낮은 것으로 보이지만195,196, 이러한 세포는 RNA 관련 자가 항원을 포함하는 면역 복합체와 BCR 및 TLR의 이중 결합 후 확장될 수 있습니다197. 림프종 탈출에서 BCR의 역할은 여전히 수수께끼이지만, B 세포 표면에 발현된 류마티스 인자는 세포의 추가 BCR 매개 활성화 여부에 관계없이 자가항체와 RNA 관련 자가항원의 면역 복합체를 가두어 TLR을 자극하는 역할을 할 수 있습니다. 염증이 있는 침샘에서 이러한 면역 복합체는 만성 B 세포 자극과 부수적으로 정형 류마티스 인자 발현 B 세포의 강력한 선택 이점을 제공할 수 있습니다. 이러한 B 세포에 FcRL4를 동시에 결합하면 형질 세포로의 분화를 억제하고 지속적인 증식을 가능하게 할 수 있습니다.
류마티스 인자를 발현하는 B 세포는 단클론 항체 G6에 의해 검출될 수 있는 면역글로불린 중쇄 가변 영역 변이체인 IGHV1-69를 자주 발현합니다(참조.198). 건강한 개인과 비교하여 pSS 및 냉동 글로불린혈증 혈관염 환자는 말초에서 카파 경쇄를 독점적으로 발현하는 G6 양성 기억 B 세포의 빈도가 증가합니다191. 흥미롭게도 류마티스 인자 활성을 갖는 모든 MALT 림프종은 카파 경쇄를 가진 IgM 클론으로188,190, 이는 G6+ B 세포가 MALT 림프종의 잠재적 전구 세포 풀을 형성할 수 있음을 시사합니다. 또한, 연구자들은 G6+ B 세포가 TNFAIP3와 같은 B 세포 증식에 관여하는 유전자의 체세포 돌연변이를 우연히 포함하고 있음을 보여주었습니다(참조.191). TNFAIP3의 특정 생식세포 다형성은 pSS199에서 MALT 림프종 발생과 관련이 있으며, 이는 B세포 조절 장애를 예방하는 데 있어 온전한 NF-κB 조절이 중요하다는 점을 강조합니다. TNFAIP3와 같은 B 세포 조절 유전자의 변이는 내성 체크포인트에서 자가 반응 세포의 탈출을 초래할 수 있습니다191. pSS 환자의 말초 혈액에서 림프종 관련 돌연변이를 포함하는 G6+ B 세포의 존재가 MALT 림프종 발병과 직접적으로 연관되지는 않았지만, 이러한 세포는 침샘으로 이동하여 더욱 활성화될 수 있습니다.
종합해 보면,
증식성이 높은 상피내 FcRL4+ B 세포는
DN2 B 세포의 선상 대응 세포로,
우연히 류마티스 인자 반응성을 나타내며
pSS 환자의 침샘에서 림프종 전구 세포 풀을 형성한다는 가설이 매력적입니다.
FcRL4+ B 세포가 순순샘에 비해 귀밑샘에서 더 자주 관찰된다는 개념은
귀밑샘에서 MALT 림프종이 우선적으로 발생하는 것을 설명할 수 있습니다169.
선상 B 세포의 종양 조절 장애를 향한 중요한 단계는
아직 알려지지 않았지만
면역 글로불린 가변 영역 유전자 내부 및 외부의 체세포 돌연변이가 관련되어 있을 가능성이 있습니다.
우리는 상피내 B 세포의 치료적 표적이
pSS 환자에서 MALT 림프종의 발병을 예방할 수 있다고 가정합니다.
Future directions
Over the past decade, the attenuation of sicca symptoms and, more recently, the attenuation of systemic disease activity have evolved as main treatment targets in pSS. As the epithelium is the functional backbone of the salivary gland, its restoration must be a central determinant of future therapies aimed at targeting hyposalivation in pSS. We hypothesize that therapies that target, for example, only the immune system might reduce glandular inflammation but not necessarily rescue salivary gland function, as demonstrated in existing clinical trials200. Although the targeting of the immune system is a valid approach in pSS, considering the typical (auto)immune manifestations and systemic nature of the disease, more attention should be paid to the correction of epithelial defects. Multifaceted approaches that consist of both an anti-inflammatory and a pro-epithelial component — for example, immunotherapy combined with cell therapy — might provide the crucial regenerative stimuli required to correct these defects.
With regard to cell therapy, fresh, patient-matched induced pluripotent stem cells might be used to derive untainted salivary gland acinar and/or ductal cells, which could subsequently be transplanted back into the patient. The relatively new drug class senolytics (a class of drugs that selectively induce death of senescent cells) might also prove therapeutically useful in the depletion of senescent epithelial progenitor cells, limiting further damage that would otherwise be inflicted by these cells201,202. The timing of therapy application is probably an important consideration, given the general early loss of salivary gland function in pSS. More advanced stages of glandular disease are characterized by the dominance of B cells and the presence of LELs, and in these patients, glandular B cells are an important treatment target. As previously highlighted, B cell depletion therapy with rituximab reduced the severity of LELs180, but whether other B cell-directed therapies also target these pathogenic structures remains to be examined. In-depth histological evaluation of glandular tissue in clinical trials is, in this context, a valuable outcome measure of clinical trials.
Dissection and identification of specific defects at the individual patient level might be the key to successful treatment, given the variety of inflammatory pathways involved in the pathogenesis of pSS. Therefore, treatment decisions guided by the clinical picture of the salivary gland hold promise. To define the clinical picture of the salivary gland in individual patients, imaging and in-depth histopathological examinations of salivary gland biopsy samples are needed, going beyond measuring the focus score. In addition, tissue transcriptomics, in particular at the single-cell level, might be useful to identify dysregulated pathways. Lastly, the scientific community is advancing with the establishment of in vitro models of salivary gland disease (for example, co-cultures of organoids or explants with immune cells)58,68,121 to screen for new drug targets and to examine the effect of immunomodulatory treatments on salivary gland function.
지난 10년 동안 시카 증상의 약화와 최근에는 전신 질환 활동의 약화가 pSS의 주요 치료 목표로 발전해 왔습니다. 침샘 상피는 침샘의 기능적 중추이므로 침샘 상피의 회복은 향후 타액 분비 저하를 목표로 하는 치료의 핵심 결정 요인이 될 것입니다. 예를 들어 면역계만을 표적으로 하는 치료법은 기존 임상시험에서 입증된 바와 같이 침샘 염증을 감소시킬 수 있지만 침샘 기능을 반드시 회복시키지는 못할 수 있다는 가설을 세우고 있습니다200. 면역 체계를 표적으로 삼는 것은 pSS에서 유효한 접근 방식이지만, 질환의 전형적인 (자가) 면역 증상과 전신적 특성을 고려할 때 상피 결함의 교정에 더 많은 주의를 기울여야 합니다. 항염증제와 친상피 성분으로 구성된 다각적인 접근법(예: 세포 치료와 결합된 면역 요법)은 이러한 결함을 교정하는 데 필요한 중요한 재생 자극을 제공할 수 있습니다.
세포 치료의 경우, 환자와 일치하는 신선한 유도 만능 줄기세포를 사용하여 오염되지 않은 침샘 선상 및/또는 도관 세포를 추출한 후 환자에게 다시 이식할 수 있습니다. 비교적 새로운 약물 계열인 세놀라아제(노화 세포의 사멸을 선택적으로 유도하는 약물 계열)도 노화 상피 전구 세포의 고갈에 치료적으로 유용할 수 있으며, 이러한 세포에 의해 발생할 수 있는 추가 손상을 제한할 수 있습니다201,202. pSS에서 침샘 기능이 일반적으로 조기에 상실된다는 점을 고려할 때 치료 적용 시기는 중요한 고려 사항일 수 있습니다. 더 진행된 단계의 선 질환은 B 세포의 우세와 LEL의 존재를 특징으로 하며, 이러한 환자에서 선상 B 세포는 중요한 치료 표적입니다. 앞서 강조한 바와 같이 리툭시맙을 사용한 B세포 고갈 치료는 LEL의 중증도를 감소시켰지만180 다른 B세포 표적 치료법도 이러한 병원성 구조를 표적으로 하는지 여부는 아직 검토해야 할 사항입니다. 이러한 맥락에서 임상시험에서 선 조직에 대한 심층적인 조직학적 평가는 임상시험의 중요한 결과 척도입니다.
pSS의 발병에 관여하는 다양한 염증 경로를 고려할 때 개별 환자 수준에서 특정 결함을 해부하고 식별하는 것이 성공적인 치료의 열쇠가 될 수 있습니다. 따라서 침샘의 임상 양상에 따라 치료 결정을 내리는 것이 유망합니다. 개별 환자에서 침샘의 임상상을 정의하기 위해서는 초점 점수를 측정하는 것 이상으로 침샘 생검 샘플의 영상 및 심층적인 조직 병리 검사가 필요합니다. 또한, 특히 단일 세포 수준에서의 조직 전사체학은 조절 장애 경로를 식별하는 데 유용할 수 있습니다. 마지막으로, 과학계는 새로운 약물 표적을 선별하고 면역 조절 치료가 침샘 기능에 미치는 영향을 조사하기 위해 타액선 질환의 체외 모델(예: 오가노이드 또는 면역 세포와 이식체의 공동 배양)58,68,121을 확립하는 데 발전하고 있습니다.
ial B 세포가 pSS 환자에서 MALT 림프종의 발병을 예방할 수 있습니다.
Conclusions
Overall, a multitude of pathways, systems and processes are probably dysregulated in the salivary gland in pSS, including defects that affect the epithelium, innate immune signalling and adaptive immune activation. In an ideal world, each defect would be corrected, and the salivary gland restored to its naive state. Although the initial triggers that activate the salivary gland epithelium remain undetermined, the nature of the local immune response, including dominant type I interferon activity, hints at the involvement of a viral infection. Subsequent dysregulation of the immune response, possibly owing to interference of type I interferon signalling by autoantibodies and chronic autoantigen exposure by apoptotic epithelial cells, results in a pro-inflammatory feedback loop. Various immune cells (such as lymphocytes, dendritic cells and macrophages) might interact with the epithelium and contribute to the inflammatory response. In particular, crosstalk between the ductal epithelium and B cells, and consequently the formation of LELs, negatively affects salivary gland morphology and might result in MALT lymphoma development. Finally, as a scientific community, we need to think more abstractly, and consider combining immunotherapy with cell therapies to provide an unfettered source of SGECs, although preventing continual resurgence of the same epithelial problems will remain a challenge.
전반적으로,
상피,
선천성 면역 신호 및 적응성 면역 활성화에 영향을 미치는 결함을 포함하여
pSS에서 침샘의 여러 경로,
시스템 및 과정이 조절 장애를 일으킬 수 있습니다.
이상적인 세계에서는 각 결함이 교정되고 침샘이 순진한 상태로 회복될 것입니다.
침샘 상피를 활성화하는 초기 유발 요인은
아직 밝혀지지 않았지만,
우성 1형 인터페론 활성을 포함한 국소 면역 반응의 특성은
바이러스 감염의 관여를 암시합니다.
자가 항체에 의한 제1형 인터페론 신호의 간섭과
세포 사멸 상피 세포에 의한 만성 자가 항원 노출로 인해
면역 반응의 후속 조절 장애가 발생하면 염증성 피드백 루프가 발생합니다.
림프구, 수지상 세포 및 대식세포와 같은
다양한 면역 세포가 상피와 상호 작용하여
염증 반응에 기여할 수 있습니다.
특히,
침샘 상피와
B 세포 사이의 누화는
침샘의 형태에 부정적인 영향을 미치고
결과적으로 LEL의 형성을 초래하여
MALT 림프종 발병을 초래할 수 있습니다.
마지막으로,
과학계는 보다 추상적으로 생각하고
면역 요법과 세포 요법을 결합하여
SGEC의 자유로운 공급원을 제공하는 것을 고려해야 하지만,
동일한 상피 문제의 지속적인 재발을 막는 것은 여전히 어려운 과제로 남을 것입니다.
References