
Review
June 28, 2004
Clinical Manifestations and Early Diagnosis of Sjögren Syndrome
Stuart S. Kassan, MD; Haralampos M. Moutsopoulos, MD, FRCP(Edin)
Author Affiliations
Arch Intern Med. 2004;164(12):1275-1284. doi:10.1001/archinte.164.12.1275
Abstract
Sjögren syndrome (SS) is a common autoimmune disease evidenced by broad organ-specific and systemic manifestations, the most prevalent being diminished lacrimal and salivary gland function, xerostomia, keratoconjunctivitis sicca, and parotid gland enlargement. Primary SS presents alone, and secondary SS occurs in connection with autoimmune rheumatic diseases. In addition, symptoms do not always present concurrently. This diversity of symptomatic expression adds to the difficulty in initial diagnosis. Armed with the recently refined criteria for diagnosis, specialists, such as rheumatologists, primary care physicians, ophthalmologists, and dentists, who would otherwise focus only on those symptoms that encompass their areas of expertise, can get a comprehensive image of the presenting patient, leading to earlier identification and treatment of SS.
Sjögren syndrome (SS) is a common, slowly progressive autoimmune disease that exhibits a wide range of organ-specific and systemic manifestations. B-cell activation is a consistent finding in patients with SS, and B and T cells invade and destroy target organs. Patients with SS (most commonly, perimenopausal women) have symptoms related to diminished lacrimal and salivary gland function and frequently present with xerostomia, keratoconjunctivitis sicca, and parotid gland enlargement. Although SS affects approximately 2% of the adult population,1 it remains undiagnosed in more than half.
Oral dryness can profoundly affect quality of life, interfering with basic daily functions such as eating, speaking, and sleeping. Reduction of salivary volume and subsequent loss of the antibacterial properties of saliva may accelerate infection, tooth decay, and periodontal disease. Ocular complaints by SS patients include sensations of itching, grittiness, soreness, and dryness, despite the eyes having a normal appearance. Diminished secretion of tears may lead to chronic irritation and destruction of corneal and bulbar conjunctival epithelium (keratoconjunctivitis sicca). Salivary gland swelling, which may start unilaterally but becomes bilateral, can be chronic or episodic.
Mucous gland secretions of the upper and lower respiratory tract may decrease in patients with SS, producing dryness of the nose, throat, and trachea; xerotrachea may result in a chronic dry cough. Diminished secretions of the exocrine glands of the skin may lead to dry skin, and vaginal dryness may cause pruritus, irritation, and dyspareunia. Systemic manifestations of SS may involve the lungs, liver, kidneys, vasculature, and blood.2-6 A small percentage of SS patients with certain adverse prognostic factors (purpura, low C4 complement levels, and mixed monoclonal cryoglobulinemia) experience increased mortality.7
Sjögren syndrome can occur alone (primary SS) or in association with systemic autoimmune rheumatic diseases (secondary SS). Because the variegated symptoms of SS are not always present at the same time, physicians and dentists sometimes treat each symptom individually, unaware that a systemic disease is present. In the past, people with SS were frequently misdiagnosed because their symptoms were considered minor or vague or mimicked those of other diseases (See Differential Diagnosis). Consequently, the interval between the onset of SS and its diagnosis is frequently long—10 years, on average, according to one estimate.8
Early diagnosis and appropriate treatment are essential for optimal management of SS. This article will present current data on the pathophysiology, clinical complaints, diagnosis, and often neglected treatment of this disease, the onset of which is typically insidious.
쇼그렌 증후군(SS)은
광범위한 장기별 및 전신 증상으로 나타나는 흔한 자가 면역 질환으로,
눈물샘과 침샘 기능 저하,
구강 건조증,
각결막염,
이하선 비대가 가장 흔한 증상입니다.
원발성 SS는 단독으로 나타나며,
이차성 SS는 자가면역성 류마티스 질환과 연관되어 발생합니다.
또한
증상이 항상 동시에 나타나는 것은 아닙니다.
이러한 다양한 증상 발현은
초기 진단의 어려움을 가중시킵니다.
최근 세분화된 진단 기준을 통해
류마티스 전문의, 1차 진료 의사, 안과 전문의, 치과의사 등 전문의는
자신의 전문 분야에 해당하는 증상에만 집중할 수 있었던 기존 방식에서 벗어나
환자의 증상을 종합적으로 파악할 수 있어
쇼그렌 증후군을 조기에 발견하고 치료할 수 있게 되었습니다.
쇼그렌 증후군(SS)은
흔하고 서서히 진행되는 자가면역 질환으로
광범위한 장기별 및 전신 증상을 나타냅니다.
B세포 활성화는
쇼그렌 증후군 환자에게서 일관되게 발견되며,
B세포와 T세포는 표적 장기를 침범하여 파괴합니다.
SS 환자(대부분 폐경 전후 여성)는
눈물샘 및 침샘 기능 저하와 관련된 증상을 보이며
구강 건조증, 각결막염, 이하선 비대가 자주 나타납니다.
구강건조증은
성인 인구의 약 2%가 앓고 있지만,1
절반 이상이 진단되지 않은 채로 지내고 있습니다.
구강 건조증은
식사, 말하기, 수면과 같은 기본적인 일상 기능을 방해하여
삶의 질에 심각한 영향을 미칠 수 있습니다.
침의 양이 감소하고
침의 항균성이 상실되면
감염, 충치, 치주 질환이 가속화될 수 있습니다.
SS 환자의 안구 증상으로는
눈은 정상적으로 보이지만
가려움증, 이물감, 따가움, 통증, 건조감 등이 있습니다.
눈물 분비 감소는
각막과 구결막 상피의 만성적인 자극과 파괴(유행성 각결막염)로
이어질 수 있습니다.

침샘 부종은
일방적으로 시작되지만
양측으로 퍼질 수 있으며
만성적이거나 일시적일 수 있습니다.

SS 환자의 경우
상기도 및 하기도 점액 분비물이 감소하여
코, 인후, 기관이 건조해지고
구강 건조증으로 인해
만성 마른 기침이 발생할 수 있습니다.
피부의 외분비샘 분비 감소는
피부 건조로 이어질 수 있으며,
질 건조는
소양증, 자극, 성교통을 유발할 수 있습니다.
쇼그렌 증후군의 전신 증상은
폐, 간, 신장, 혈관계, 혈액에 나타날 수 있습니다.2-6
특정 예후 불량 요인(자반증, 낮은 C4 보체 수치, 혼합 단클론성 냉동 글로불린혈증)이 있는
쇼그렌 증후군 환자의 일부는
사망률이 증가할 수 있습니다.7

쇼그렌 증후군은 단독으로 발생하거나(원발성 쇼그렌 증후군)
전신성 자가면역 류마티스 질환과 연관되어
발생할 수 있습니다(이차성 쇼그렌 증후군).
쇼그렌 증후군의 다양한 증상이
항상 동시에 나타나는 것은 아니기 때문에
의사와 치과의사는 전신 질환이 있다는 사실을 모르고
각 증상을 개별적으로 치료하는 경우가 있습니다.
과거에는
증상이 경미하거나 모호하거나
다른 질병의 증상과 비슷하다고 여겨져 오진되는 경우가 많았습니다(감별 진단 참조).
그 결과,
한 추정에 따르면
쇼그렌 증후군 발병과
진단 사이의 간격이 평균 10년으로 길어지는 경우가 많았습니다.8
조기 진단과 적절한 치료는
쇼그렌 증후군을 최적으로 관리하기 위해 필수적입니다.
이 글에서는
일반적으로 발병이 교묘한
이 질환의 병태생리, 임상 증상, 진단 및 종종 방치되는 치료에 대한
최신 데이터를 소개합니다.
Prevalence
An estimated 2 to 4 million persons in the United States have SS. Approximately 1 million have an established diagnosis; however, because of the heterogeneity and often nonspecific nature of its clinical manifestations, it is likely that the disease remains undiagnosed in most cases. Sjögren syndrome primarily affects women, with a female-male ratio of 9:1, and may occur in patients of all ages but typically has its onset in the fourth to sixth decades of life. Approximately 60% of SS patients have the disease secondary to an accompanying autoimmune disorder such as rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), or systemic sclerosis. Although estimates vary, information from rheumatology clinics suggests that approximately 25% of patients with RA or SLE have histologic evidence of SS.6
미국에서는
약 200만 명에서 400만 명이
쇼그렌 증후군을 앓고 있는 것으로 추정됩니다.
약 100만 명이 진단을 받았지만,
임상 증상의 이질성과 종종 비특이적인 특성으로 인해
대부분의 경우 진단되지 않은 채로 남아 있을 가능성이 높습니다.
쇼그렌 증후군은
여성과 남성의 비율이 9:1로 여성에게 주로 발생하며,
모든 연령대의 환자에게서 발생할 수 있지만
일반적으로 4~60대에 발병합니다.
SS 환자의 약 60%는
류마티스 관절염(RA),
전신 홍반성 루푸스(SLE) 또는
전신 경화증과 같은 자가 면역 질환으로 인해
이 질환이 이차적으로 발생합니다.
추정치는 다양하지만,
류마티스 클리닉의 정보에 따르면
RA 또는 SLE 환자의 약 25%가
조직학적으로 SS의 증거를 가지고 있다고 합니다.6
Pathophysiology
Central to the pathophysiology of SS is chronic immune system stimulation. The processes that underlie the humoral and cellular autoimmune reactions observed in patients with SS are not known, but both B and T lymphocytes are involved. B-cell hyperreactivity is expressed through hypergammaglobulinemia and circulating autoantibodies.9 Organ-specific autoantibodies include antibodies to cellular antigens of salivary ducts, the thyroid gland, the gastric mucosa, erythrocytes, the pancreas, the prostate, and nerve cells. Non–organ-specific autoantibodies are found in approximately 60% of patients with SS. These autoantibodies include rheumatoid factors, antinuclear antibodies, and antibodies to the small RNA-protein complexes Ro/SS-A and La/SS-B. These autoantibodies may contribute to tissue dysfunction before inflammation is evident.10
Histopathologic findings in SS include focal lymphocytic infiltrates, located mainly around the glandular ducts. These pathologic findings include lymphocyte infiltration of the salivary and lacrimal glands and other exocrine glands of the respiratory and gastrointestinal tracts and vagina. The infiltrate contains T cells, B cells, and plasma cells, with a predominance of activated CD4+ helper T cells.11 These T cells produce interleukin (IL)-2, IL-4, IL-6, IL-1β, and tumor necrosis factor α (TNF-α).12 Approximately 20% of the infiltrate population is made up of B cells, which locally produce immunoglobulins that have autoantibody reactivity.13 Eventually, the infiltrate extends to occupy the acinar epithelium, leading to glandular dysfunction that manifests as dry eyes and mouth, and enlargement of the major salivary glands.14
The inflammatory processes of SS occur primarily via glandular epithelial cells, which can express antigen-presenting proteins, promote adhesion, and costimulate T lymphocytes. Cytokines such as interferon (IFN)-γ and TNF-α may enhance the antigen-presenting function of epithelial cells or, in the case of IFN-γ, induce apoptosis of salivary gland epithelial cells (SGECs), through up-regulation of the Fas protein, a cell surface receptor whose activation leads to programmed cell death.15 A recently published study of the expression of CD40 protein (associated with B-cell activation) in a cultured, nonneoplastic SGEC line found that expression was significantly higher in cells derived from patients with SS compared with control subjects; CD40 could be further induced in SGECs by IFN-γ and IL-1β. These findings suggest the intrinsically activated status of these cells and provide additional evidence that SGECs have a pivotal role in the induction and maintenance of lymphocytic infiltrates in SS patients.16
ss의 병리 생리학의 핵심은
만성 면역계 자극입니다.
SS 환자에서 관찰되는
체액성 및 세포성 자가 면역 반응의 근간이 되는 과정은 알려져 있지 않지만,
B 림프구와 T 림프구가 모두 관련되어 있습니다.
B세포 과반응성은
고감마글로불린혈증과
순환 자가항체를 통해 발현됩니다.9
장기 특이적 자가항체에는
침샘, 갑상선, 위 점막, 적혈구, 췌장, 전립선, 신경 세포의 세포 항원에 대한
항체가 포함됩니다.
비장기 특이적 자가항체는
ss 환자의 약 60%에서 발견됩니다.
이러한 자가항체에는
류마티스 인자, 항핵 항체,
작은 RNA-단백질 복합체 Ro/SS-A 및 La/SS-B에 대한 항체가 포함됩니다.
이러한 자가 항체는
염증이 나타나기 전에
조직 기능 장애를 일으킬 수 있습니다.10
SS의 조직 병리학적 소견에는
주로 선관 주변에 위치한
국소 림프구 침윤이 포함됩니다.
이러한 병리학적 소견에는
침샘과 눈물샘, 호흡기 및 위장관, 질의
기타 외분비샘의 림프구 침윤이 포함됩니다.
침윤물에는
T 세포, B 세포 및 형질 세포가 포함되며
활성화된 CD4+ 헬퍼 T 세포가 우세합니다.11
이러한
T 세포는
인터루킨 IL-2, IL-4, IL-6, IL-1β 및 TNF-α를 생성합니다.12
침윤물 인구의 약 20%는
자가 항체 반응성을 갖는
면역 글로불린을 국소적으로 생산하는
B 세포로 구성됩니다.13
결국,
침윤물은
침샘 상피를 점유하기 위해 확장되어
눈과 입이 건조해지고
주요 침샘이 비대해지는 선 기능 장애를 유발합니다.14
SS의 염증 과정은
주로 선 상피 세포를 통해 발생하며,
선 상피 세포는 항원 제시 단백질을 발현하고,
접착을 촉진하며,
T 림프구를 자극할 수 있습니다.
인터페론(IFN)-γ 및 TNF-α와 같은 사이토카인은
상피 세포의 항원 제시 기능을 강화하거나
IFN-γ의 경우 세포 표면 수용체인 Fas 단백질의 상향 조절을 통해
침샘 상피 세포(SGEC)의 세포 사멸을 유도할 수 있으며,
활성화되면 프로그램된 세포 사멸로 이어집니다.15
최근에 발표된 배양된 비종양성 SGEC 라인에서 CD40 단백질(B세포 활성화와 관련)의 발현에 대한 연구에 따르면, 대조군에 비해 SS 환자에서 유래한 세포에서 발현이 유의하게 높았으며, CD40은 IFN-γ 및 IL-1β에 의해 SGEC에서 추가로 유도될 수 있는 것으로 나타났습니다. 이러한 결과는 이러한 세포의 본질적으로 활성화된 상태를 시사하며, SGEC가 SS 환자에서 림프구 침윤의 유도 및 유지에 중추적인 역할을 한다는 추가적인 증거를 제공합니다.16
Systemic disease
Sjögren syndrome is a systemic disease strongly associated with organ-specific and systemic autoimmunity. For example, thyroid dysfunction and/or autoimmune thyroid disease was found in 45% of one series of patients with primary SS.17 Vascular involvement in patients with SS may result in peripheral neuropathy, glomerulonephritis, and gastrointestinal lesions.3 Numerous systemic manifestations of SS exist that can contribute to difficulty of diagnosis.
쇼그렌 증후군은
장기 특이적 및 전신 자가면역과
밀접한 관련이 있는 전신 질환입니다.
예를 들어,
원발성 쇼그렌 증후군 환자의 45%에서
갑상선 기능 장애 및/또는
자가면역성 갑상선 질환이 발견되었습니다.17
쇼그렌 증후군 환자의 혈관 침범은
말초 신경병증,
사구체신염,
위장병변을 유발할 수 있습니다.3
쇼그렌 증후군의 전신 증상은
진단을 어렵게 할 수 있는
수많은 증상이 존재합니다.
Fatigue
Extreme, debilitating fatigue occurs in approximately 50% of patients with primary SS,18 and many patients find this feature of the disease more troublesome than the exocrine symptoms. Patients spend several extra hours in bed trying to rest or sleep, but most report that they do not feel refreshed on awakening.8 Although the cause of this fatigue is undetermined, hypothyroidism (usually subclinical), which is frequently associated with SS, may contribute to it.1 Seven percent of patients with fibromyalgia have been shown to also have SS,19 and fibromyalgia has been reported to be present in 22% of patients with primary SS.20
원발성 ss 환자의 약 50%에서
극심한 쇠약 피로가 발생하며,18
많은 환자가 외분비 증상보다
이 질환의 이러한 특징을 더 괴롭게 여깁니다.
환자들은
휴식이나 수면을 취하기 위해
침대에서 몇 시간을 더 보내지만
대부분 잠에서 깨어나도 상쾌하지 않다고 보고합니다.8
이러한 피로의 원인은 밝혀지지 않았지만,
갑상선 기능 저하증(보통 무증상)이
SS와 관련이 있을 수 있습니다.1
섬유 근육통 환자의 7%가
SS를 동반하는 것으로 나타났으며,19
섬유 근육통 환자의 22%에서
원발성 SS가 나타나는 것으로 보고되었습니다.20
Musculoskeletal Involvement
Joint disease in primary SS is typically an intermittent polyarticular arthropathy primarily affecting small joints, asymmetrically at times. Joint deformity and mild erosions occur uncommonly, and a nonerosive arthritis, resembling that of SLE, may occur transiently.21 Arthralgias exist in as many as 53% of patients and myalgias in as many as 22%.22 Primary SS is often confused with RA both clinically and serologically, whereas secondary SS is often found in patients with RA.
원발성 강직성 관절염의 관절 질환은
일반적으로 간헐적인 다관절성 관절병증으로
주로 작은 관절에 비대칭적으로 영향을 미칩니다.
관절 변형과 경미한 미란은 드물게 발생하며,
SLE와 유사한 비미란성 관절염이
일시적으로 발생할 수 있습니다.21
환자의
53%에서관절통이,
22%에서 근육통이 나타납니다.22
원발성 SS는 임
상적으로나 혈청학적으로 RA와 혼동되는 경우가 많지만,
이차성 SS는 RA 환자에서 종종 발견됩니다.
Dermatologic Involvement
Dry skin, another exocrine manifestation of SS, was found to affect 55% of SS patients in a recent study. More than 10% of SS patients reported a skin rash (compared with 0% of control subjects), and 18% of SS patients reported "burning skin."23 In a study that examined the histologic classification and clinical presentation of vasculitis in SS patients, 9 of 70 patients with primary SS developed vasculitis of small- or medium-sized vessels. Of these 9 cases, 8 involved the skin. In addition to the typical hypersensitivity-type rash, 3 of the SS patients with vasculitis had ulcerative lesions or violaceous discoloration of the digits.3 It is important to differentiate these dermatological findings from those of SLE and scleroderma, with which patients with secondary SS are often comorbidly afflicted. Raynaud phenomenon, usually mild, can be observed in nearly 30% of patients with primary SS.1
최근 연구에 따르면
SS의 또 다른 외분비 증상인
피부 건조증은
SS 환자의 55%에서 나타나는 것으로 밝혀졌습니다.
SS 환자의 18%는 "피부가 타는 듯한 느낌"을 호소
SS 환자의 10% 이상이
피부 발진을 보고했으며(대조군의 0%에 비해),
SS 환자의 18%는 "피부가 타는 듯한 느낌"을 호소 했습니다.23
burning skin
SS 환자의 혈관염의 조직학적 분류와 임상 양상을 조사한 연구에서
원발성 SS 환자 70명 중 9명이
중소형 혈관 혈관염을 일으켰습니다.
이 9건 중 8건은 피부와 관련이 있었습니다.
전형적인 과민성 발진 외에도
혈관염을 앓은 SS 환자 중 3명은
궤양성 병변 또는 손가락의 심한 변색이 있었습니다.3
이러한 피부과적 소견은
이차성 SS 환자에게 흔히 동반되는
SLE 및 경피증과 구별하는 것이 중요합니다.
레이노 현상은 일반적으로 경미하지만
원발성 전신 홍반 환자의
약 30%에서 관찰될 수 있습니다.1
Pulmonary Involvement
Although common, pulmonary involvement is seldom clinically significant in patients with SS.2 Cough is often the main respiratory symptom and is usually a symptom of xerotrachea. Other potential pulmonary complications include lymphocytic alveolitis, lymphocytic interstitial pneumonitis and fibrosis, and pseudolymphoma. Findings of high-resolution chest computed tomography during the expiratory phase of respiration suggest that up to 30% of patients with SS have subclinical pulmonary disease.24 Although pulmonary function test results may show small-airway obstruction, β-agonists or corticosteroids produce little significant benefit.
폐 침범은 흔하지만,
SS 환자에서 임상적으로 중요한 경우는 드뭅니다.2
기침이
주요 호흡기 증상인 경우가 많으며
대개 건조 기관지의 증상입니다.
다른 잠재적인 폐 합병증으로는
림프구 폐포염,
림프구 간질성 폐렴 및 섬유증,
가성 림프종 등이 있습니다.
호흡 호기 단계의 고해상도 흉부 컴퓨터 단층 촬영 결과에 따르면 SS 환자의 최대 30%가 무증상 폐 질환을 가지고 있는 것으로 나타났습니다.24 폐 기능 검사 결과 소기도 폐색이 나타날 수 있지만 β- 작용제나 코르티코스테로이드는 큰 효과가 없는 것으로 나타났습니다.
Gastroenterologic Involvement
Patients with SS may have involvement of their entire gastrointestinal tract. Malabsorption due to lymphocytic infiltrates of the intestine rarely occurs in patients with SS, and esophageal dysmotility has been reported in 36% to 90% of patients.25,26 Routine laboratory testing frequently reveals mild pancreatitis and hepatitis; the latter requires differentiation from hepatitis C and organ-specific autoimmune hepatitis. Hepatitis C virus infection is not associated with typical primary SS, but a lymphocytic sialadenitis occurs with increased prevalence in patients with chronic hepatitis C infection. These patients will also have xerostomia but will not exhibit xerophthalmia and will not have anti-Ro/SS-A antibodies.27 Hepatic involvement is indicated in approximately 7% of patients with primary SS by the presence of antimitochondrial antibodies and, less frequently, by abnormal liver enzyme levels. The histopathologic appearance is similar to that of early (stage 1) primary biliary cirrhosis.14
SS 환자는
위장관 전체가 침범될 수 있습니다.
장의 림프구 침윤으로 인한 흡수 장애는
SS 환자에서 드물게 발생하며
식도 운동 장애는 환자의 36%~90%에서 보고되었습니다.25,26
일상적인 실험실 검사에서
경미한 췌장염과 간염이 종종 발견되며,
후자는 C형 간염 및 장기 특이 자가 면역 간염과의 감별이 필요합니다.
C 형 간염 바이러스 감염은
전형적인 원발성 SS와 관련이 없지만
만성 C 형 간염 감염 환자에서 유병률이 증가하면서
림프구 성 시알 라덴염이 발생합니다.
이 환자들은 또한
구강 건조증이 있지만
안구 건조증은 나타나지 않으며
항-Ro/SS-A 항체가 없습니다.27
원발성 SS 환자의
약 7%에서 항미토콘드리아 항체의 존재로 간 침범이 나타나며,
드물게는 간 효소 수치 이상이 나타나기도 합니다.
조직 병리학적 양상은 초기(1기) 원발성 담즙성 간경변증과 유사합니다.14
Renal Involvement
Patients with SS may have tubulointerstitial involvement of the kidneys affecting the tubules (eg, distal renal tubular acidosis, impaired concentrating ability, hypercalcinuria, or proximal tubule defects).28-31 Pathologic examination often shows tubulointerstitial nephritis with sparing of the glomeruli.9,28,32-34 The interstitial inflammation is predominantly lymphocytic with interstitial fibrosis and tubular atrophy. In SS patients who show evidence of glomerular lesions, hematuria, proteinuria, and renal insufficiency may be exhibited. Some patients may progress to nephrotic syndrome. A number of patients may develop renal vasculitis with significant hypertension and renal insufficiency.
SS 환자는
세뇨관에 영향을 미치는
신장의 세뇨관 간질 침범
(예: 원위 신장 세뇨관 산증, 집중력 장애, 고칼슘뇨증 또는 근위 세뇨관 결손)이
있을 수 있습니다.28-31
병리 검사 결과
사구체가 보존된
세뇨관 간질 신염이 종종 나타납니다.9,28,32-34
간질 염증은 주로 간질성 섬유증과 세뇨관 위축이 있는 림프구성 염증입니다.
사구체 병변의 증거를 보이는 SS 환자의 경우
혈뇨, 단백뇨 및
신부전이 나타날 수 있습니다.
일부 환자는
신증후군으로 진행될 수 있습니다.
많은 환자에서
심각한 고혈압과 신부전을 동반한
신장 혈관염이 발생할 수 있습니다.
Neurologic Involvement
One of the most common significant systemic manifestations of SS is neurologic disease, which can involve the cranial and peripheral nerves and, infrequently, the central nervous system. Peripheral neuropathy, primarily sensory, was found in 22% (10/46) of one series of patients with primary SS; it was the presenting manifestation in 5 patients (11%). The neuropathy was associated with alterations of the endoneurial microvessels, but necrotizing vasculitis was not seen.35 Central nervous system disease in patients with SS is believed to be very rare, but its incidence is controversial.36 In a study of 30 women with primary SS, 14 (46%) had sensorineural hearing loss, which was significant in 5. Hearing loss in these patients was correlated with the presence of anticardiolipin antibodies, suggesting an underlying autoimmune cause.4
다발성 경화증의 가장 흔한 전신 증상 중 하나는
신경 질환으로,
뇌신경과 말초 신경,
드물게는 중추 신경계가 관련될 수 있습니다.
말초 신경병증(주로 감각)은
원발성 SS 환자 중 22%(10/46)에서 발견되었으며,
5명의 환자(11%)에서 증상이 나타났습니다.
신경 병증은
척수 내 미세 혈관의 변화와 관련이 있었지만
괴사성 혈관염은 보이지 않았습니다.35
SS 환자의 중추 신경계 질환은 매우 드문 것으로 여겨지지만
그 발생률에 대해서는 논란이 있습니다.36
원발성 SS 여성 30명을 대상으로 한 연구에서
14명(46%)이 감각 신경성 난청이 있었고,
5명에서 유의미한 청력 손실이 있었습니다.
이 환자들의 난청은
항카디오리핀 항체의 존재와 관련이 있어
기저 자가 면역 원인을 시사하는 것으로 보입니다.4
Hematologic/Oncologic Involvement
Compared with age-, sex-, and race-matched controls, patients with SS in one study had a 44 times higher relative risk of lymphoma, and clinically identifiable lymphoma occurs in approximately 5% of patients with SS.37 Malignant lymphoproliferation may be present initially or may develop later in the disease. An essential process in the transition from the autoimmune state to non-Hodgkin lymphoma is monoclonality, and monoclonal B-cell expansion occurs in some patients with SS, arising mainly from exocrine glands and less frequently from visceral organs or lymph nodes.38 Monoclonal B-cell proliferation may initially present as Waldenström macroglobulinemia.37
Patients with SS having risk factors for progression to lymphoma (Table 1) should be closely monitored. Those with persistent gland enlargement, purpura, low levels of C4, and monoclonal cryoglobulinemia are at increased risk.1,7,40
Most lymphomas in patients with SS are of B-cell lineage and are of low- or intermediate-grade malignancy. These lymphomas are usually localized in extranodal areas such as the salivary glands, gastrointestinal tract, thyroid gland, lung, kidney, or orbit. Localized, low-grade lymphoma affecting exocrine glands can be managed by watchful waiting; disseminated lymphoma may be treated with combination chemotherapy.1
한 연구에서
연령, 성별, 인종이 일치하는 대조군과 비교했을 때,
SS 환자는
림프종에 걸릴 상대적 위험이 44배 높았으며
임상적으로 확인 가능한 림프종은
SS 환자의 약 5%에서 발생합니다.37
악성 림프 증식은
초기에 나타나거나 질병의 후반부에 발생할 수 있습니다.
자가면역 상태에서
비호지킨 림프종으로 이행하는 필수 과정은
단클론성이며,
단클론성 B세포 증식은
주로 외분비샘에서 발생하고
내장 기관이나 림프절에서 덜 자주 발생하는
일부 SS 환자에서 발생합니다.38
단클론성 B세포 증식은
처음에 발덴스트롬 거대글로불린혈증으로 나타날 수 있습니다.37
림프종으로 진행될 위험 요인이 있는
전신 홍반성 낭창 환자(표 1)는
면밀히 관찰해야 합니다.
지속적인 샘 비대, 자반증, 낮은 수준의 C4, 단클론성 냉동 글로불린혈증이 있는 환자는 위험이 높습니다.1,7,40
SS 환자의 림프종은
대부분 B 세포 계통이며
저등급 또는 중간 등급의 악성 종양입니다.
이러한
림프종은 일
반적으로 침샘, 위장관, 갑상선, 폐, 신장 또는 안와와 같은
림프절 외 부위에 국한되어 발생합니다.
외분비선에 영향을 미치는
국소 저등급 림프종은 경과 관찰로 관리할 수 있으며,
파종성 림프종은 화학 요법을 병용하여 치료할 수 있습니다.1

Diagnosis of ss
Clinical Signs and Symptoms
Many symptoms of SS are deceptively nonspecific, and the spectrum of clinical manifestations is very broad. Because SS is frequently seen in middle-aged women, symptoms of cutaneous, oral, and vaginal dryness may initially be attributed to menopause. The early symptoms of dry eyes and mouth may be confused with atopic disease and anxiety, respectively. Additionally, xerostomia symptoms are common to many conditions and are, in part, subjective. In a study of more than 600 patients, 15% of those with primary SS and 26% of those with secondary SS did not complain of xerostomia.41
Signs suggestive of lymphoproliferation include significant enlargement of the salivary glands, lymphadenopathy, splenomegaly, and pulmonary infiltrates. Longitudinal monitoring of laboratory parameters in patients with SS may reveal findings associated with the development of lymphoma, such as the appearance of a monoclonal protein, new-onset leukopenia and anemia, and a loss of specific autoantibodies.42 In a recent study of 261 Greek patients, low C4 levels and mixed monoclonal cryoglobulinemia were linked with an approximately 6- to 8-fold relative risk for the development of lymphoma.7
ss의 많은 증상은
놀라울 정도로 비특이적이며
임상 증상의 스펙트럼이 매우 광범위합니다.
중년 여성에게 자주 나타나기 때문에
피부, 구강 및 질 건조 증상은
처음에는 폐경으로 인한 것으로 생각될 수 있습니다.
안구 건조증과 구강 건조증의 초기 증상은
각각 아토피 질환 및 불안증과 혼동될 수 있습니다.
또한 구강 건조증 증상은
여러 질환에 공통적으로 나타나며
부분적으로는 주관적일 수 있습니다.
600명 이상의 환자를 대상으로 한 연구에서
원발성 SS 환자의 15%와
이차성 SS 환자의 26%는 구강 건조증을 호소하지 않았습니다.41
림프 증식을 암시하는 징후로는
침샘의 현저한 비대,
림프절 병증,
비장 비대,
폐 침윤 등이 있습니다.
SS 환자의 실험실 매개변수를 장기적으로 모니터링하면
단클론 단백질의 출현,
새로 발병한 백혈구 감소증 및 빈혈,
특정 자가항체 소실 등
림프종 발병과 관련된 소견을 발견할 수 있습니다.42
그리스 환자 261명을 대상으로 한 최근 연구에서 낮은 C4 수치와 혼합 단클론 냉동 글로불린혈증이 림프종 발병의 약 6~8배 상대 위험과 관련이 있는 것으로 나타났습니다.7
Characteristic Clinical Findings
An analysis of symptoms in 169 patients with SS and 44 control subjects found that 93.5% of patients with SS and 2.3% of controls had dry mouth; 67.5% and 13.6%, respectively, had dry eyes.23 In this same study, stepwise discriminant analysis of individual symptoms suggested that the combined symptoms of dry mouth, sore mouth, and dry eyes correctly classified 93% of patients with SS and 97.7% of control subjects.23
SS 환자 169명과 대조군 44명의 증상을 분석한 결과,
SS 환자의 93.5%와
대조군의 2.3%가 구강 건조증을,
각각 67.5%와 13.6%가 안구 건조증을 앓고 있었습니다.23
같은 연구에서
개별 증상에 대한 단계적 판별 분석 결과
구강 건조증, 입 통증, 안구 건조증의 복합 증상으로
SS 환자의 93%와
대조군의 97.7%를 정확하게 분류할 수 있는 것으로 나타났습니다.23

Ocular Manifestations.
Dry eye is the most prominent ocular manifestation of SS. Symptoms of dry eye may include sensations of itching, grittiness, or soreness, even though the eyes' appearance is normal. Ocular complaints may include photosensitivity, erythema, eye fatigue, decreased visual acuity, a discharge in the eyes, and the sensation of a film across the visual field.1,23 Ocular symptoms may be exacerbated by the low levels of humidity that prevail in air-conditioned environments and dry climates, exposure to cigarette smoke, and drugs with anticholinergic effects.1
Although diminished tear secretion is characteristic of SS, the actual tear flow rates are not well correlated with ocular discomfort. Because of decreased tear film and an abnormal mucus component, thick, rope-like secretions may accumulate along the inner canthus. Small superficial erosions of the corneal epithelium may result from desiccation; in severe cases, slitlamp examination may reveal filamentary keratitis, marked by mucus filaments that adhere to damaged areas of the corneal surface. Conjunctivitis due to Staphylococcus aureus infection may also occur. Enlargement of the lacrimal glands is rare. Ocular complications may include corneal ulceration, vascularization, opacification, and, rarely, perforation.1
안구 건조증은
SS의 가장 두드러진 안구 증상입니다.
안구 건조증의 증상으로는
눈의 외관은 정상인데도
가려움, 뻑뻑함, 따가움 등이 있을 수 있습니다.
안구 증상으로는
광과민증, 홍반, 눈의 피로, 시력 저하, 눈의 분비물, 시야에 막이 끼는 느낌 등이
안구 증상은 냉방 환경과 건조한 기후, 담배 연기 노출, 항콜린 효과가 있는 약물에 의해 악화될 수 있습니다.1
눈물 분비 감소는 안구건조증의 특징이지만, 실제 눈물 유속은 안구 불편감과 잘 상관관계가 없습니다. 눈물막의 감소와 비정상적인 점액 성분으로 인해 두꺼운 밧줄 모양의 분비물이 안검을 따라 쌓일 수 있습니다. 각막 상피의 작은 표면 미란은 건조로 인해 발생할 수 있으며, 심한 경우 세극등 검사에서 각막 표면의 손상된 부위에 점액 필라멘트가 달라붙어 있는 필라멘트 각막염이 나타날 수 있습니다. 황색포도상구균 감염으로 인한 결막염도 발생할 수 있습니다. 눈물샘 비대는 드물게 발생합니다. 안구 합병증으로는 각막 궤양, 혈관 형성, 혼탁, 드물게 천공이 발생할 수 있습니다.1
Oral Manifestations.
Although the presenting symptoms of SS are frequently those of xerostomia, the patient may complain not of oral dryness, but of an unpleasant taste, difficulty eating dry food, such as crackers, soreness, or difficulties in controlling dentures. In the early stages of SS, the mouth may appear moist, but as the disease progresses, the usual pooling of saliva in the floor of the mouth becomes absent and lines of contact between frothy saliva and the oral soft tissue are seen. In advanced disease, the oral mucosa appears dry and glazed and tends to form fine wrinkles. Extreme dryness of the mouth, causing the tongue to stick to the palate, may lead to a "clicking" quality in the speech of patients with SS. Typically, the surface of the tongue becomes red and lobulated, with partial or complete depapillation.
In patients with SS, chronic salivary gland inflammation leads to loss of function and decreased salivary flow rates, which are associated with an increased frequency of dental caries.43-45 The salivary glands normally produce 1 to 1.5 L of saliva daily. Saliva contains lysozyme, lactoferrin, lactoperoxidase, and histidine-rich polypeptides, which inhibit bacteria and fungi.46,47 Furthermore, salivary glycoproteins are thought to play a role in inhibition of microbial attachment to oral epithelium.48,49 Saliva is cleared from the mouth by reflex swallowing. This swallowing eliminates food debris, microorganisms, and loose cells from the mouth, providing a continuous "flushing" system that keeps the mouth clean and prevents colonization by bacteria. In patients with SS and severe salivary hypofunction, the mean number and proportion of Streptococcus mutans and Lactobacillus organisms and the frequency of Candida organisms are reported to be increased.50 Patients with SS have also been reported to have an increased risk of periodontal disease, but this association has not been as firmly established as that with dental caries. A recent trial compared the periodontal condition of 24 patients with SS, 27 patients with an autoimmune disease with SS, and 29 control subjects with subjective complaints of xerostomia only. No significant difference in the periodontal condition of the 3 groups was found.51 Xerostomia can lead to difficulty with dentures and the need for expensive dental restorations, particularly in elderly patients with SS.52
Additional oral symptoms may include soreness, adherence of food to buccal surfaces, fissuring of the tongue, and dysphagia. In addition to the appearance of dental caries, angular cheilitis associated with candidiasis may exist.1 The taste buds also may be abnormal, resembling those of patients with idiopathic hypogeusia, and their number decrease.53 Gross accumulation of plaque may exist. In ambulatory patients, SS is the most common underlying cause of acute bacterial sialadenitis, usually staphylococcal or pneumococcal. Typically, affected patients have acute pain, trismus, and a tender swelling of the salivary gland. The regional lymph nodes may be enlarged and tender, and fever and malaise may exist in severe cases.
구강 건조증의 증상은
구강 건조증과 유사한 경우가 많지만,
환자는 구강 건조증이 아니라
불쾌한 맛, 크래커와 같은 건조한 음식 섭취의 어려움,
통증 또는 틀니 조절의 어려움 등을 호소할 수 있습니다.
구강건조증 초기에는
입안이 촉촉해 보일 수 있지만
질병이 진행됨에 따라 입 바닥에 타액이 고이는 현상이 사라지고
거품이 있는 타액과
구강 연조직 사이의 접촉선이 보입니다.
질환이 진행되면 구강 점막이 건조하고 윤이 나며 잔주름이 생기는 경향이 있습니다. 입안이 극도로 건조하여 혀가 입천장에 달라붙으면 SS 환자의 말에서 "딸깍"하는 소리가 날 수 있습니다. 일반적으로 혀의 표면이 붉어지고 소엽화되며 부분적으로 또는 완전히 탈모됩니다.
SS 환자의 경우 만성 침샘 염증은
기능 상실과 타액 유량 감소로 이어지며,
이는 충치 발생 빈도 증가와 관련이 있습니다.43-45
침샘은
일반적으로
매일 1~1.5L의 타액을 생성합니다.
침에는
박테리아와 곰팡이를 억제하는
리소자임, 락토페린, 락토페록시다제, 히스티딘이
또한 타액 당단백질은 미생물이 구강 상피에 부착하는 것을 억제하는 역할을 하는 것으로 생각됩니다.48,49 침은 반사 삼킴으로 입에서 제거됩니다. 이러한 삼킴은 입안의 음식물 찌꺼기, 미생물 및 느슨한 세포를 제거하여 입안을 청결하게 유지하고 박테리아의 식민지를 방지하는 지속적인 "플러싱" 시스템을 제공합니다. SS 및 중증 타액 기능 저하 환자에서 스트렙토코커스 뮤탄스균과 락토바실러스균의 평균 수와 비율, 칸디다균의 빈도가 증가하는 것으로 보고되었습니다.50 SS 환자도 치주 질환의 위험이 증가하는 것으로 보고되었지만 이러한 연관성은 충치만큼 확실하게 밝혀지지는 않았습니다. 최근의 한 임상시험에서는 24명의 SS 환자, 27명의 자가면역질환 환자, 그리고 주관적인 구강 건조증만 호소하는 29명의 대조군을 대상으로 치주 상태를 비교했습니다. 세 그룹의 치주 상태에는 유의미한 차이가 발견되지 않았습니다.51 구강 건조증은 특히 고령의 SS 환자에서 틀니 사용의 어려움과 고가의 치과 수복물의 필요성으로 이어질 수 있습니다.52
추가적인 구강 증상으로는 통증, 음식물이 협측 표면에 달라붙는 현상, 혀의 갈라짐, 연하곤란 등이 있을 수 있습니다. 충치 외에도 칸디다증과 관련된 각성 치은염이 나타날 수 있습니다.1 특발성 미각 저하증 환자의 미각과 유사하게 미뢰가 비정상적으로 나타나고 그 수가 감소할 수 있습니다.53 플라그가 심하게 축적될 수 있습니다. 외래 환자에서 SS는 급성 세균성 시알라덴염의 가장 흔한 근본 원인이며, 일반적으로 포도상구균 또는 폐렴구균입니다. 일반적으로 감염된 환자는 급성 통증, 삼차신경통, 침샘의 부드러운 부종이 나타납니다. 국소 림프절이 커지고 압통이 있을 수 있으며 심한 경우 발열과 불쾌감이 나타날 수 있습니다.
Additional Xeroses.
In female patients with SS, desiccation of the vagina and vulva may result in dyspareunia and pruritus.1 One study of 169 patients with SS found that vaginal symptoms existed in 26%.23 However, an earlier study that compared 51 women with SS with 57 healthy control subjects found no difference in fertility, parity, or reproductive success between the 2 groups. Vaginal atrophy and reduced cervical mucus production correlated with age and menopause in this study, but not with any clinical or serologic manifestation of SS.54
In patients with SS, diminution or absence of glandular secretions of the respiratory tract can lead to dryness of the nose, throat, and trachea that results in persistent hoarseness and a chronic, nonproductive cough. Involvement of the exocrine glands of the skin leads to skin dryness in patients with SS. Vasculitis limited to the skin may manifest as purpura or urticaria and is sometimes associated with other systemic manifestations and the presence of anti-Ro/SS-A antibodies. The most frequent histologic finding is leukocytoclastic vasculitis,22 characterized by necrotizing neutrophilic inflammation of small dermal blood vessels, usually resulting in palpable purpura, with slightly raised hemorrhagic skin lesions.
여성 ss 환자의 경우
질과 외음부의 건조증으로
성교통과 가려움증이 발생할 수 있습니다.1
ss 환자 169명을 대상으로 한 연구에 따르면
26%에서 질 증상이 나타난 것으로 나타났습니다.23
그러나 51명의 ss 여성과 57명의 건강한 대조군을 비교한 이전 연구에서는 두 그룹 간에 생식 능력, 성 평등 또는 생식 성공에 차이가 없는 것으로 밝혀졌습니다. 이 연구에서 질 위축과 자궁경부 점액 생산 감소는 연령 및 폐경과 상관관계가 있었지만, SS의 임상적 또는 혈청학적 증상과는 상관관계가 없었습니다.54
SS 환자의 경우 호흡기의 선 분비
물이 감소하거나 없으면
코, 인후 및 기관이 건조해져 쉰 목소리가 지속되고
만성적이고 비생산적인 기침이 발생할 수 있습니다.
피부의 외분비샘이 침범하면
SS 환자의 피부가 건조해집니다.
피부에 국한된 혈관염은
자반증이나 두드러기로 나타날 수 있으며
때때로 다른 전신 증상 및 항-Ro/SS-A 항체의 존재와 관련이 있습니다.
가장 흔한 조직학적 소견은 작은 피부 혈관의 괴사성 호중구 염증을 특징으로 하는 백혈구 세포성 혈관염으로,22 일반적으로 약간 융기된 출혈성 피부 병변과 함께 만져지는 자반을 유발합니다.
Importance of Diagnostic Accuracy
Although often elusive, an early, accurate diagnosis of SS can help prevent or ensure timely treatment of many of the complications associated with the disease. For example, early restoration of salivary function can relieve symptoms of dry mouth and may prevent or slow the progress of the oral complications of SS, including dental caries, oral candidiasis, and periodontal disease. Untreated severe dry eye can result in corneal perforation in the patient with SS, which may eventually lead to loss of the eye. Early diagnosis may contribute to prompt recognition and treatment of serious systemic complications of SS such as malignant lymphoma and interstitial lung disease. Additionally, an extensive delay in diagnosis can affect the patient's psychological well-being because of the anxiety that accompanies an undiagnosed illness.
An appropriate diagnosis of SS depends on recognition of its clinical manifestations, elimination of alternative differential diagnoses, and distinguishing primary from secondary SS. For example, recurrent parotid gland enlargement is more often found in patients with SS alone than in patients with RA plus SS. In addition, lymphadenopathy, purpura, Raynaud phenomenon, renal involvement, and myositis occur more often in patients with SS alone than in patients with RA plus SS.
진단이 어려운 경우가 많지만,
구강건조증을 조기에 정확하게 진단하면
이 질환과 관련된 많은 합병증을 예방하거나 적시에 치료하는 데 도움이 될 수 있습니다.
예를 들어, 타액 기능을 조기에 회복하면 구강 건조 증상을 완화하고 충치, 구강 칸디다증, 치주 질환 등 구강 건조증의 구강 합병증을 예방하거나 진행 속도를 늦출 수 있습니다. 중증 안구건조증을 치료하지 않으면 각막 천공이 발생할 수 있으며, 이는 결국 실명으로 이어질 수 있습니다. 조기 진단은 악성 림프종 및 간질성 폐질환과 같은 심각한 전신성 안구건조증 합병증을 조기에 인지하고 치료하는 데 기여할 수 있습니다. 또한 진단이 늦어지면 진단되지 않은 질병에 수반되는 불안감으로 인해 환자의 심리적 안녕에 영향을 미칠 수 있습니다.
SS의 적절한 진단은
임상 증상에 대한 인식,
대체 감별 진단의 제거,
일차성 및 이차성 SS의 구별에 달려 있습니다.
예를 들어, 재발성 이하선 비대는 RA와 SS가 동반된 환자보다 SS만 있는 환자에서 더 자주 발견됩니다. 또한 림프절 병증, 자반증, 레이노 현상, 신장 침범, 근염은 RA와 SS를 동반한 환자보다 SS만 있는 환자에서 더 자주 발생합니다.
Diagnostic Criteria
Although minor salivary gland biopsy traditionally has been considered the "gold standard" for the diagnosis of SS, newer criteria permit classification of SS without necessarily performing this procedure. An American-European consensus committee recently modified and reapproved criteria that exhibit approximately 95% sensitivity and specificity for SS55 (Table 2). These criteria encompass the presence of subjective and objective sicca manifestations, antibodies to Ro/SS-A and La/SS-B antigens, and characteristic histopathologic findings in minor salivary glands. Of the 6 criteria given in Table 2, 4 must be present to establish a diagnosis of SS, with 1 of the 4 being an objective measurement (ie, by histopathologic examination or antibody screening).57 Use of the modified European criteria55 should assist early and accurate diagnosis of SS, and they will likely be used to define eligible patients in future therapeutic trials.
전통적으로
경미한 침샘 생검이
SS 진단의 "황금 표준"으로 여겨졌지만,
최신 기준에서는 이 절차를 수행하지 않고도
SS를 분류할 수 있습니다.
최근 미국-유럽 합의 위원회는 SS55에 대해 약 95%의 민감도와 특이도를 보이는 기준을 수정하고 재승인했습니다(표 2). 이러한 기준에는 주관적 및 객관적 시카 증상, Ro/SS-A 및 La/SS-B 항원에 대한 항체, 경미한 침샘의 특징적인 조직 병리학적 소견이 포함됩니다.
표 2에 제시된 6가지 기준 중
4가지를 충족해야만 SS 진단을 내릴 수 있으며,
4가지 중 1가지는
조직병리학적 검사 또는 항체 검사를 통한 객관적인 측정입니다.57
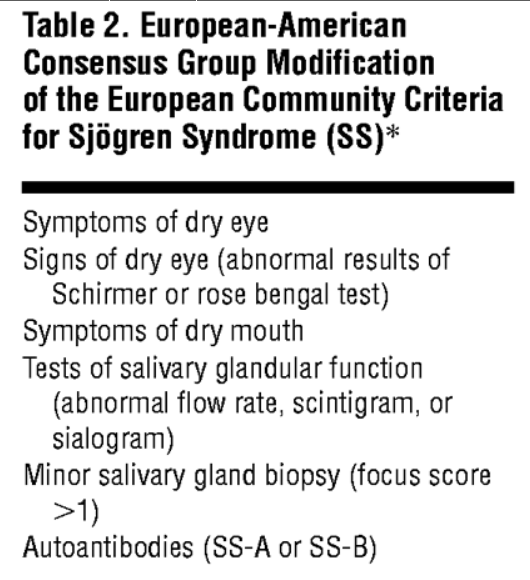
수정된 유럽 기준55을 사용하면 SS를 조기에 정확하게 진단하는 데 도움이 될 것이며 향후 치료 임상시험에서 대상 환자를 정의하는 데 사용될 가능성이 높습니다.
Diagnostic Methods
As assessment of oral and ocular involvement is essential to the accurate diagnosis of SS. The Schirmer test for the eye quantitatively measures tear formation via placement of filter paper in the lower conjunctival sac. If less than 5 mm of paper is wetted after 5 minutes, the test result is positive. Rose bengal scoring involves placement of 25 mL of rose bengal solution in the inferior fornix of each eye and having the patient blink twice. Slitlamp examination detects destroyed conjunctival epithelium caused by desiccation. The rose bengal score—the sum of scores assigned to damage found in 3 regions of the eye—can define the presence of keratoconjunctivitis sicca.
Sialometry measures unstimulated salivary flow into a calibrated tube for 15 minutes; normal flow is more than 1.5 mL. While being simple and noninvasive, sialometry alone does not distinguish between causes of xerostomia. Other tests used to evaluate salivary gland involvement include parotid sialography and salivary gland scintigraphy. Patients with SS show gross distortion of the normal pattern of parotid ductules on sialogram, with marked retention of contrast medium. Scintigraphic findings in patients with SS include decreased uptake and release of technetium Tc 99m pertechnetate, with the extent of decrease paralleling the degree of xerostomia and salivary flow rate.
Minor salivary gland biopsy remains a highly specific test for the salivary component of SS. When performed properly, the patient experiences no more than temporary soreness, and healing without significant scarring is rapid. Focal lymphocytic sialadenitis, defined as multiple, dense aggregates of 50 or more lymphocytes (1 focus) in perivascular or periductal areas in the majority of sampled glands, is a characteristic histopathologic feature of SS. Patients with SS whose main complaint is persistent parotid gland swelling may have a parotid biopsy substituted for a salivary biopsy if lymphoma is suspected.44
Serologic and laboratory findings associated with SS include diffuse hypergammaglobulinemia, which is found in approximately 80% of patients with the disease. Several autoantibodies are among the immunoglobulins whose levels are elevated, including rheumatoid factors, antinuclear antibodies, and antibodies to the extractable cellular antigens Ro/SS-A and La/SS-B. Anti-Ro/SS-A is not specific for SS and occurs in other autoimmune disorders, particularly SLE. However, patients with SLE who have anti-La/SS-B antibodies usually have SS. In approximately 20% of patients with SS, cryoglobulins are present and consist of monoclonal IgMκ cryoprecipitable immunoglobulins that have rheumatoid factor activity.40
구강 및 안구 침범에 대한 평가는
SS의 정확한 진단에 필수적입니다.
눈의 쉬르머 검사는
하부 결막낭에 여과지를 넣어
눈물 형성을 정량적으로 측정합니다.
5분 후 여과지가 5mm 미만으로 젖으면
검사 결과는 양성입니다.
로즈벵갈 검사는 각 눈의 하륜에 로즈벵갈 용액 25mL를 넣은 후 환자가 눈을 두 번 깜빡이게 하는 방식으로 진행됩니다. 세극등 검사는 건조증으로 인한 결막 상피의 파괴를 감지합니다. 눈의 세 부위에서 발견된 손상에 부여된 점수의 합인 로즈 벵갈 점수로 유행성 각결막염의 존재를 정의할 수 있습니다.
시알로메트리는 보정된 튜브에 15분 동안 자극하지 않은 타액의 흐름을 측정하며, 정상 흐름은 1.5mL 이상입니다. 타액 측정은 간단하고 비침습적이지만, 타액 측정만으로는 구강 건조증의 원인을 구분할 수 없습니다. 침샘 침범을 평가하는 데 사용되는 다른 검사로는 이하선 조영술과 침샘 신티그래피가 있습니다. SS 환자는 시알로그램에서 귀밑샘관의 정상 패턴이 심하게 왜곡되어 있으며 조영제가 현저하게 남아 있는 것을 볼 수 있습니다. SS 환자의 신티그래피 소견에는 테크네튬 Tc 99m 퍼테크네테이트의 흡수 및 방출 감소가 포함되며, 감소 정도는 구강건조증 및 타액 유속의 정도와 비례합니다.
경미한 침샘 생검은
SS의 침 성분에 대한 매우 구체적인 검사로 남아 있습니다.
제대로 시행하면 환자는 일시적인 통증만 경험하고 큰 흉터 없이 빠르게 치유됩니다. 국소 림프구 샘샘염은 샘플링된 대부분의 샘에서 혈관 주위 또는 관 주위 부위에 50개 이상의 림프구(1개 초점)가 다발적으로 밀집된 응집체로 정의되며, SS의 특징적인 조직 병리학적인 특징입니다. 지속적인 이하선 부종이 주된 증상인 SS 환자는 림프종이 의심되는 경우 침샘 생검 대신 이하선 생검을 받을 수 있습니다.44
SS와 관련된 혈청학적 및 실험실 소견으로는 미만성 고감마글로불린혈증이 있으며, 이는 이 질환 환자의 약 80%에서 발견됩니다. 류마티스 인자, 항핵 항체, 추출 가능한 세포 항원 Ro/SS-A 및 La/SS-B에 대한 항체 등 여러 자가 항체가 면역글로불린 수치 상승의 원인이 됩니다. 항 Ro/SS-A는 SS에 특이적이지 않으며 다른 자가면역질환, 특히 SLE에서 발생합니다. 그러나 항-La/SS-B 항체를 가진 SLE 환자는 일반적으로 SS를 가지고 있습니다. SS 환자의 약 20%에서 냉동 글로불린이 존재하며 류마티스 인자 활성을 갖는 단일 클론 IgMκ 냉동 침전성 면역 글로불린으로 구성됩니다.40
Differential Diagnosis
The differential diagnosis of SS includes conditions and medications that can produce keratoconjunctivitis sicca, xerostomia, and parotid gland enlargement. Xerostomia may be caused by amyloidosis, diabetes mellitus, sarcoidosis, SS, viral infections, trauma, or irradiation or may be psychogenic. Additionally, certain drugs may produce xerostomia, including antihypertensive, parasympatholytic, and psychotherapeutic agents.
Dry eyes can be caused by amyloidosis, inflammation (chronic blepharitis or conjunctivitis, pemphigoid, or Stevens-Johnson syndrome), SS, neurologic conditions that impair eyelid or lacrimal gland function, sarcoidosis, toxicity (burns or drugs), and a variety of other conditions (corneal anesthesia, blink abnormality, hypovitaminosis A, eyelid scarring, or trauma).
Bilateral parotid gland enlargement may be the result of endocrine disorders (acromegaly or gonadal hypofunction), metabolic diseases (chronic pancreatitis, diabetes mellitus, hepatic cirrhosis, or hyperlipoproteinemias), SS, or viral infections (human immunodeficiency virus infection, hepatitis C, or mumps).
When keratoconjunctivitis sicca or xerostomia occurs in isolation, it is necessary to exclude potential causes, such as deficiency disorders or drugs, and medical conditions, such as infection, endocrinopathies, or degenerative diseases.
The differential diagnosis is especially important to therapy for systemic manifestations of SS. Differentiation of SS from RA, SLE, scleroderma, and other rheumatic disorders can be problematic, since all of these conditions can start with nonspecific manifestations such as arthralgias, myalgias, low-grade fever, and Raynaud phenomenon. It is also extremely important to exclude other systemic disorders that can affect exocrine glands, such as sarcoidosis, amyloidosis, human immunodeficiency virus infection, and lymphoma.
The goal of the workup for SS is to eliminate differential diagnostic possibilities and to document the key features of SS (Table 3). A complete workup for SS frequently involves the coordination of multiple specialists, in addition to the rheumatologist, to appropriately assess the eyes, oral cavity, and head and neck.
SS의 감별 진단에는
유행성 각결막염,
구강 건조증,
이하선 비대를 유발할 수 있는 질환과 약물이 포함됩니다.
구강 건조증은
아밀로이드증, 당뇨병, 유육종증, SS, 바이러스 감염, 외상 또는 방사선 조사로 인해
발생하거나 심인성일 수 있습니다.
또한
항고혈압제,
부교감신경용해제,
정신치료제 등 특정 약물에 의해 안구건조증이 발생할 수 있습니다.
안구 건조증은
아밀로이드증, 염증(만성 안검염 또는 결막염, 천포창 또는 스티븐스-존슨 증후군),
SS, 눈꺼풀 또는 눈물샘 기능을 손상시키는 신경학적 질환,
유육종증, 독성(화상 또는 약물), 기타 다양한 질환(각막 마취, 눈 깜박임 이상, 저 비타민 A증, 눈꺼풀 흉터 또는 외상) 등으로
인해 발생할 수 있습니다.
양측 이하선 비대는
내분비 장애(비대증 또는 생식선 기능 저하),
대사 질환(만성 췌장염, 당뇨병, 간경변증, 고지 단백 혈증),
SS 또는 바이러스 감염(인간 면역 결핍 바이러스 감염, C형 간염 또는 볼거리)으로 인해
발생할 수 있습니다.
유행성 각결막염이나 구강건조증이
단독으로 발생하는 경우에는
결핍 장애나 약물, 감염, 내분비 질환, 퇴행성 질환 등의
잠재적 원인을 배제해야 합니다.
감별 진단은
특히 전신성 다발성 경화증 증상에 대한 치료에 중요합니다.
이러한 질환은
모두 관절통, 근육통, 미열, 레이노 현상과 같은 비특이적 증상으로 시작될 수 있기 때문에
RA, SLE, 경피증 및 기타 류마티스 질환과의 감별이
어려울 수 있습니다.
또한
유육종증, 아밀로이드증, 인간 면역결핍 바이러스 감염, 림프종 등
외분비선에 영향을 미칠 수 있는
다른 전신 질환을 배제하는 것도 매우 중요합니다.
SS에 대한 정밀 검사의 목표는 감별 진단 가능성을 없애고 SS의 주요 특징을 문서화하는 것입니다(표 3). 류마티스 전문의 외에도 눈, 구강, 두경부 등을 적절히 평가하기 위해 여러 전문의의 협진이 필요한 경우가 많습니다.
Treatment
Treatment of SS is mainly symptomatic and is directed toward recognizing and treating complications of the disease early. Treatment is typically intended to limit the damage resulting from chronic xerostomia and keratoconjunctivitis. Moisture replacement products can be effective for patients with mild or moderate symptoms.18 The muscarinic M3 receptor, located on acinar cells of both lacrimal and salivary glands, is involved in tearing and salivation. Because most patients with SS have some residual acinar cell function, treatment with muscarinic agonists such as pilocarpine hydrochloride and cevimeline hydrochloride has therapeutic effects on xerostomia and keratoconjunctivitis sicca.58,59
SS의 치료는 주로 증상에 따라 이루어지며,
질병의 합병증을 조기에 인지하고 치료하는 데 중점을 둡니다.
치료는 일반적으로
만성 건조증과 각결막염으로 인한
손상을 제한하기 위한 것입니다.
경증 또는 중등도 증상을 보이는 환자에게는
수분 보충제가 효과적일 수 있습니다.18
눈물샘과 침샘의 눈물샘 세포에 있는 무스카린 M3 수용체는 눈물과 타액 분비에 관여하는 수용체입니다. 대부분의 SS 환자는 눈물샘 세포 기능이 어느 정도 남아 있기 때문에 필로카르핀 염산염 및 세비멜린 염산염과 같은 무스카린 작용제로 치료하면 구강건조증과 각결막염에 치료 효과가 있습니다.58,59
Ocular Disease
Frequent use of tear substitutes will help replace moisture, and preservative-free formulations help avoid the irritation that can occur with frequent use. Although lubricating ointments and methylcellulose inserts may be longer lived, they are usually reserved for nocturnal use because of the potential for significant blurring of vision.
Temporary occlusion of the puncta through the insertion of plugs (collagen or silicone) or permanent occlusion by electrocautery can be used to block tear drainage and thus retain existing tears. Existing moisture can also be preserved by goggles or glasses with specially constructed side chambers. Despite a low acceptance by patients, these devices can be valuable in certain environmental conditions, such as wind. Soft contact lenses may be helpful but pose a risk of infection. Infection, which may present with sudden aggravation of symptoms and/or excessive mucus production, should be promptly treated. Corticosteroid-containing ophthalmic solutions should be avoided because they may induce corneal lesions or promote infection.
Blepharitis, or inflammation of the meibomian glands, is a possible complication of dry eye and can be treated with warm compresses, cleansing of the eyelids, and a topical antibiotic, if needed.
For patients whose eye dryness is not adequately controlled by moisture preservation or replacement methods, secretagogues are a potential treatment. Secretagogues can enhance secretion through the stimulation of the muscarinic receptors of the salivary glands and other organs. Because of this stimulation, however, caution is advised in administering secretagogues to patients with asthma, narrow-angle glaucoma, acute iritis, severe cardiovascular disease, biliary disease, nephrolithiasis, diarrhea, or ulcer disease. Currently, 2 agents are approved and available for use as secretagogues in patients with SS—pilocarpine and cevimeline.45,60
By stimulating the M3 and M1 receptor subtypes on acinar and ductal cells of the salivary and lacrimal glands, pilocarpine and cevimeline are therapeutic options for the relief of dry mouth and eyes that accompany SS. Their mechanism of action may help prevent apoptosis and blunt the damage caused by proinflammatory cytokines, while optimizing the function of residual glandular cells in patients with SS. The muscarinic agonist pilocarpine hydrochloride (Salagen; MGI Pharma Inc, Bloomington, Minn) is a potent stimulant of exocrine secretion, and its sialogogue activity has been known for more than a century.61,62 Adverse effects of pilocarpine, primarily excessive sweating and nausea, are related to its secretory-stimulating properties. As a parasympathomimetic agent, pilocarpine has potential cardiovascular and pulmonary effects, which may limit its use in certain patients (eg, those taking β-blockers and those with asthma).45 Bradycardia and tachycardia have both been reported with the use of pilocarpine.63
In phase 3 trials of the newer selective muscarinic agonist cevimeline hydrochloride (Evoxac; Daiichi Pharmaceutical Corporation, Montvale, NJ), excessive sweating of mild to moderate severity was the common adverse effect, with an incidence approximately half that reported with the use of pilocarpine.64 A comparison of the pharmacologic properties of these agents is given in Table 4.
Pilocarpine hydrochloride, 5 mg 4 times daily for 12 weeks, improved global assessments of dry eyes statistically significantly better than did placebo in 373 patients with primary or secondary SS. The most common adverse effect of treatment was sweating.62 A trial comparing cevimeline, 30 or 15 mg 3 times daily, with placebo found statistically significant improvement in dry eye conditions among SS patients with keratoconjunctivitis sicca. Patients treated with 30 mg 3 times daily for 12 weeks reported improvement in global evaluation of dry eyes vs placebo-treated patients (P = .0453). Patients with the most persistent and troublesome dry eyes had the highest rate of improvement (43% and 26% of the most severely affected patients treated with cevimeline and placebo, respectively, reported that their dry eye condition improved after 12 weeks [P = .008]). The incidence of serious adverse events was comparable in the cevimeline and placebo groups, with the most frequently reported adverse events due to the expected muscarinic effects of cevimeline (eg, nausea and sweating).65
눈물 대체제를 자주 사용하면 수분을 보충하는 데 도움이 되며, 무방부제 제형은 잦은 사용으로 발생할 수 있는 자극을 피하는 데 도움이 됩니다. 윤활 연고와 메틸셀룰로오스 삽입물은 더 오래 사용할 수 있지만, 시야가 크게 흐려질 수 있기 때문에 일반적으로 야간에 사용하는 것이 좋습니다.
플러그(콜라겐 또는 실리콘) 삽입을 통한 일시적 누공 폐색 또는 전기 소작술을 통한 영구 폐색으로 눈물 배출을 차단하여 기존 눈물을 유지할 수 있습니다. 특수 제작된 측면 챔버가 있는 고글이나 안경으로 기존 수분을 보존할 수도 있습니다. 이러한 장치는 환자들의 수용도가 낮지만 바람과 같은 특정 환경 조건에서 유용할 수 있습니다. 소프트 콘택트렌즈는 도움이 될 수 있지만 감염의 위험이 있습니다. 갑작스러운 증상 악화 및/또는 과도한 점액 생성으로 나타날 수 있는 감염은 즉시 치료해야 합니다. 코르티코스테로이드 함유 안약은 각막 병변을 유발하거나 감염을 촉진할 수 있으므로 피해야 합니다.
안검염 또는 마이봄샘의 염증은 안구건조증의 합병증으로 발생할 수 있으며 온찜질, 눈꺼풀 세척, 필요한 경우 국소 항생제 투여로 치료할 수 있습니다.
수분 보존 또는 대체 방법으로 안구 건조증이 적절히 조절되지 않는 환자의 경우, 분비 촉진제가 잠재적인 치료법이 될 수 있습니다. 분비 촉진제는 침샘 및 기타 기관의 무스카린 수용체를 자극하여 분비를 촉진할 수 있습니다. 그러나 이러한 자극으로 인해 천식, 협각 녹내장, 급성 홍채염, 중증 심혈관 질환, 담도 질환, 신결석증, 설사 또는 궤양 질환이 있는 환자에게 분비 촉진제를 투여할 때는 주의가 필요합니다. 현재 SS-필로카르핀과 세비마인 두 가지 약제가 승인되어 환자의 분비 촉진제로 사용할 수 있습니다.45,60
필로카르핀과 세비믈린은 침샘과 눈물샘의 선상 및 관상 세포의 M3 및 M1 수용체 아형을 자극하여 SS에 동반되는 구강 및 눈 건조증 완화를 위한 치료 옵션입니다. 이들의 작용 메커니즘은 세포 사멸을 방지하고 염증성 사이토카인으로 인한 손상을 둔화시키는 동시에 SS 환자의 잔류 선 세포의 기능을 최적화하는 데 도움이 될 수 있습니다. 무스카린 작용제인 필로카르핀 염산염(살라젠, MGI Pharma Inc, 미네소타주 블루밍턴)은 강력한 외분비 자극제로, 시알로고그 작용은 한 세기 이상 알려져 왔습니다.61,62 주로 과도한 발한과 메스꺼움 등 필로카르핀의 부작용은 분비를 자극하는 특성과 관련이 있습니다. 부교감신경 모방제인 필로카르핀은 심혈관 및 폐에 영향을 미칠 수 있으므로 특정 환자(예: β 차단제 복용 환자 및 천식 환자)에게는 사용이 제한될 수 있습니다.45 필로카르핀 사용 시 서맥과 빈맥이 모두 보고된 바 있습니다.63
새로운 선택적 무스카린 작용제인 세비멜린 염산염(Evoxac, 다이이찌 제약, 뉴저지주 몽베일)의 3상 임상시험에서 경증에서 중등도의 과도한 발한이 흔한 부작용이었으며, 발생률은 필로카핀 사용 시 보고된 부작용의 약 절반이었습니다.64 이러한 약제의 약리학적인 특성을 비교하면 표 4에 나와 있습니다.
필로카르핀 염산염을 12주 동안 1일 4회 5mg씩 12주간 복용한 373명의 원발성 또는 이차성 SS 환자에서 위약보다 안구건조증의 전반적인 평가가 통계적으로 유의하게 더 개선되었습니다. 치료의 가장 흔한 부작용은 발한이었습니다.62 세비마인 30mg 또는 15mg을 1일 3회 투여한 시험과 위약을 비교한 시험에서 유행성 각결막염이 있는 SS 환자의 안구 건조증이 통계적으로 유의미하게 개선된 것으로 나타났습니다. 12주 동안 1일 3회 30mg을 투여한 환자들은 위약을 투여한 환자들에 비해 안구 건조증에 대한 전반적인 평가에서 개선된 것으로 나타났습니다(P = .0453). 가장 지속적이고 문제가 심한 안구건조증 환자의 개선율이 가장 높았습니다(세비마인과 위약으로 치료받은 가장 심한 환자 중 각각 43%와 26%가 12주 후 안구건조증 상태가 개선되었다고 보고했습니다[P = .008]). 심각한 이상반응 발생률은 세비마인과 위약 그룹에서 비슷했으며, 세비마인의 예상되는 무스카린 효과(예: 메스꺼움, 발한)로 인한 이상반응이 가장 자주 보고되었습니다.65
Oral Disease
Oral manifestations of SS are due to decreased saliva secretions, and treatment is intended to minimize xerostomia by the use of saliva substitutes, stimulating saliva secretion, and preventing dental caries and infections that may result from xerostomia.66 Although available, saliva substitutes are not generally accepted by patients because they consider these products to be short-lived and unappetizing. Saliva substitutes should, however, be prescribed for patients with severe dryness and no residual salivary function. The oral moisturizing gel, Oralbalance 7 (Laclede Inc, Rancho Dominguez, Calif), lasts longer and appears to be best suited for nocturnal use.
Fastidious dental care is required, including frequent dental examinations and office and home fluoride application. Some severe symptoms can occur as a result of intraoral candidiasis, which should be treated with nystatin. Because the oral suspension of nystatin that is commonly used contains a significant amount of sucrose, which is not appropriate for patients with SS, an alternative is nystatin vaginal tablets dissolved orally. In addition, clotrimazole lozenges, taken 5 times daily for 14 days, may also be used.56 Nystatin or clotrimazole cream can also be used to treat angular cheilitis.67 Patients with SS should, if possible, avoid diuretics, antihypertensive drugs, antidepressants, and antihistamines, all of which may worsen salivary hypofunction.
Generally, salivary flow rate increases within 15 minutes after oral pilocarpine administration and peak flow rate is maintained for 4 hours or longer.66 A recent Spanish trial tested pilocarpine hydrochloride, 5 mg, in ophthalmic solution, administered sublingually, for xerostomia in 60 patients with primary SS. Of 46 patients with low pretreatment salivary flow (<1.5 mL), 22 had increased flows (>1.5 mL) after treatment. Investigators surmised that responding patients maintained some residual capacity of their salivary glands.68
A recently reported, placebo-controlled trial of cevimeline hydrochloride, 30 or 60 mg 3 times daily, found that patients in both dosage groups experienced statistically significant improvement in dry mouth after 6 weeks of therapy. Of the patients who received 30 mg and 60 mg of cevimeline hydrochloride, 66% and 67%, respectively, reported improvement from pretreatment self-assessment of dry mouth; 35% of placebo-treated patients reported improvement (P = .004 and .02, respectively). Decreased use of artificial saliva was found by the trial's end in 19% and 4% of patients treated with 60 mg and 30 mg of cevimeline hydrochloride, respectively; none of the placebo-treated patients decreased their use of artificial saliva.61
Natural human interferon alfa, given as 150 IU 3 times daily for 12 weeks, has been shown to significantly improve stimulated whole saliva output and decrease complaints of xerostomia compared with placebo treatment.69 While oral interferon alfa in this trial was free of the significant adverse effects associated with the high-dose parenteral form of the drug, additional clinical trials are needed to confirm the safety and efficacy of interferon alfa for treatment of SS.
Patients should be educated about and use environmental measures that can enhance moisture, such as the use of a humidifier. Likewise, patients should avoid forced hot air heating systems and excessive air conditioning, which cause drying. Patients with SS should use sugar-free products. Highly flavored lemon lozenges and chewing gum are useful. Additionally, patients with SS should drink water regularly.
구강건조증의 구강 증상은 타액 분비 감소로 인한 것으로, 치료는 타액 대체제를 사용하여 타액 분비를 촉진하고 구강건조증으로 인한 충치 및 감염을 예방하여 구강건조증을 최소화하는 것입니다.66 타액 대체제를 사용할 수 있지만, 일반적으로 환자들은 이러한 제품이 지속 시간이 짧고 맛이 없다고 생각하기 때문에 잘 사용하지 않습니다. 그러나 타액 대체제는 건조증이 심하고 타액 기능이 잔존하지 않는 환자에게 처방되어야 합니다. 구강 보습 젤인 Oralbalance 7(캘리포니아주 랜초 도밍게즈 소재 Laclede Inc)은 효과가 오래 지속되며 야간에 사용하기에 가장 적합한 것으로 보입니다.
잦은 치과 검진과 사무실 및 가정에서의 불소 도포 등 까다로운 치과 관리가 필요합니다. 구강 내 칸디다증으로 인해 일부 심각한 증상이 나타날 수 있으며, 이 경우 니스타틴으로 치료해야 합니다. 일반적으로 사용되는 니스타틴 경구 현탁액에는 상당한 양의 자당이 포함되어있어 SS 환자에게는 적합하지 않기 때문에 경구 용해 된 니스타틴 질 정제가 대안이 될 수 있습니다. 또한, 14일 동안 매일 5회 복용하는 클로트리마졸 로젠지도 사용할 수 있습니다.56 니스타틴 또는 클로트리마졸 크림은 각성 구순염 치료에도 사용할 수 있습니다.67
SS 환자는
침샘 기능 저하를 악화시킬 수 있는
이뇨제, 항고혈압제, 항우울제 및 항히스타민제를 가능하면 피해야 합니다.
일반적으로 경구용 필로카르핀 투여 후 15분 이내에 타액 유량이 증가하고 최고 유량은 4시간 이상 유지됩니다.66 최근 스페인의 한 시험에서는 원발성 SS 환자 60명을 대상으로 구강 건조증에 대해 염산 필로카르핀 5mg을 점안액에 담아 설하 투여하는 실험을 실시했습니다. 치료 전 타액 분비량이 적었던(<1.5mL) 46명의 환자 중 22명은 치료 후 타액 분비량이 증가(>1.5mL)했습니다. 연구자들은 반응한 환자들이 침샘의 잔여 용량을 어느 정도 유지한 것으로 추측했습니다.68
최근 보고된 세비멜린 염산염 30mg 또는 60mg을 1일 3회 복용한 위약 대조 임상시험에 따르면 두 용량 그룹 모두 치료 6주 후 구강 건조증이 통계적으로 유의하게 개선된 것으로 나타났습니다. 세비멜린 염산염 30mg과 60mg을 투여한 환자 중 각각 66%와 67%가 치료 전 구강 건조증 자가 평가에서 개선되었다고 보고했으며, 위약을 투여한 환자의 35%가 개선되었다고 보고했습니다(각각P = .004 및 .02). 시험 종료 시점에 세비멜린 염산염 60mg과 30mg으로 치료받은 환자의 각각 19%와 4%에서 인공 타액 사용이 감소한 것으로 나타났으며, 위약으로 치료받은 환자 중 인공 타액 사용을 줄인 환자는 한 명도 없었습니다.61
천연 인간 인터페론 알파를 12주 동안 매일 3회 150 IU씩 투여하면 위약 치료와 비교하여 자극된 전체 타액 분비가 유의하게 개선되고 구강 건조증 증상이 감소하는 것으로 나타났습니다.69 이 임상시험에서 경구 인터페론 알파는 고용량 비경구 형태의 약물과 관련된 중대한 부작용이 없었지만, SS 치료에 대한 인터페론 알파의 안전성과 효능을 확인하려면 추가 임상시험이 필요합니다.
환자는 가습기 사용과 같이 습도를 높일 수 있는 환경적 조치에 대해 교육받고 이를 사용해야 합니다. 마찬가지로, 환자는 건조를 유발하는 강제 온풍 난방 시스템과 과도한 에어컨 사용을 피해야 합니다. SS 환자는 무설탕 제품을 사용해야 합니다. 향이 강한 레몬 사탕과 껌이 유용합니다. 또한 SS 환자는 정기적으로 물을 마셔야 합니다.
Systemic Disease
Nonsteroidal anti-inflammatory drugs usually provide relief from the minor musculoskeletal symptoms of SS, as well as painful parotid swelling. Disease-modifying antirheumatic agents are seldom used because erosive disease is uncommon. Hydroxychloroquine has been reported to improve features of immunologic hyperreactivity in patients with primary SS; however, a demonstrated clinical benefit is lacking.70 Hydroxychloroquine is used also for the treatment of arthralgias, myalgias, and constitutional symptoms. In an initial small open study, hydroxychloroquine improved features of immunologic hyperreactivity, that is, hypergammaglobulinemia and autoantibody levels, but the long-term efficacy of the drug needs to be assessed further.71 Corticosteroid use is generally limited to the treatment of severe extraglandular manifestations of SS. In rare cases, a short course of low-dose corticosteroid may relieve very painful or disabling joint symptoms. Pruritus and mild leukocytoclastic vasculitis may be treated with the intermittent use of a low-dose corticosteroid cream. Moderate doses of oral corticosteroids can be used to achieve initial suppression in more severe cases with necrotic or ulcerating lesions and vasculitis. Corticosteroids can also be considered when renal tubular acidosis that is resistant to replacement therapy or evidence of renal insufficiency is present. Membranoproliferative glomerulonephritis may initially be treated with prednisone.
Low dosages of tricyclic antidepressants can be helpful to improve sleep in patients with fibromyalgia, but the use of these drugs may be problematic for many patients with SS because of their tendency to cause dry mouth. Other hypnotic, anxiolytic, and antidepressant agents may be appropriate. Patients with fibromyalgia should be advised of the importance of regular exercise, including fast walking and stretching exercises, and may benefit from referral to a physical therapist or exercise physiologist. Myofascial therapy, which includes modalities such as passive stretching, massage, heat treatment, acupuncture, and injection of a local anesthetic such as lidocaine at tender points, can often ameliorate the muscle pain of fibromyalgia.72
Although still being investigated,73 long-term immunosuppressive therapy for SS has, thus far, not resulted in the hoped-for benefit.5 In previous trials, neither oral cyclosporine nor methotrexate, despite improvement of subjective symptoms, has been shown to affect lacrimal or parotid flow significantly; these agents also have moderately toxic effects. Immunosuppressive drugs should be used with caution in patients with chronic, nonfatal disorders such as SS.
Hepatic involvement is rare, affecting 5% of patients with SS. Patients with mild primary biliary cirrhosis may be treated with ursodeoxycholic acid.66 For persistent and progressive liver enzyme elevation, prednisone and azathioprine may be required. Also rare, chronic atrophic gastritis occurs in some patients with SS.66 Gastroesophageal reflux disease may be managed with antacids, histamine2 blockers, or proton pump inhibitors.
Nonpharmacologic measures to ameliorate skin dryness include gently blotting dry after bathing, leaving a small amount of moisture, and then applying a moisturizer. Additionally, loose, non–form-fitting clothing should be worn in cases of hypergammaglobulinemic purpura. Humidification, secretagogues, and guaifenesin can help manage xerotrachea.
비스테로이드성 항염증제는
일반적으로 경미한 근골격계 증상과
고통스러운 이하선 부종을 완화하는 데 도움이 됩니다.
미란성 질환은 흔하지 않기 때문에 질병을 조절하는 항류마티스제는 거의 사용되지 않습니다. 하이드록시클로로퀸은 원발성 SS 환자에서 면역학적 과민 반응의 특징을 개선하는 것으로 보고되었지만 임상적 이점이 입증되지 않았습니다.70 하이드록시클로로퀸은 관절통, 근육통 및 체질적 증상의 치료에도 사용됩니다. 초기 소규모 공개 연구에서 하이드록시클로로퀸은 면역학적 과민 반응의 특징, 즉 고감마글로불린혈증과 자가항체 수치를 개선했지만 약물의 장기 효능은 추가 평가가 필요합니다.71 코르티코스테로이드 사용은 일반적으로 심각한 SS의 선외 증상을 치료하는 데 제한됩니다. 드물게 저용량의 코르티코스테로이드를 단기간 사용하면 매우 고통스럽거나 장애를 초래하는 관절 증상이 완화될 수 있습니다. 소양증과 경미한 백혈구 혈관염은 저용량 코르티코스테로이드 크림을 간헐적으로 사용하여 치료할 수 있습니다. 괴사성 또는 궤양성 병변과 혈관염이 더 심한 경우에는 중간 용량의 경구용 코르티코스테로이드를 사용하여 초기 억제를 달성할 수 있습니다. 대체 요법에 내성이 있는 신세뇨관 산증이나 신부전증의 증거가 있는 경우에도 코르티코스테로이드 투여를 고려할 수 있습니다. 막 증식성 사구체신염은 초기에 프레드니손으로 치료할 수 있습니다.
저용량의 삼환계 항우울제는 섬유근육통 환자의 수면 개선에 도움이 될 수 있지만, 이러한 약물의 사용은 구강 건조를 유발하는 경향이 있기 때문에 많은 SS 환자에게 문제가 될 수 있습니다. 다른 최면제, 불안 완화제, 항우울제 등이 적절할 수 있습니다. 섬유근육통 환자는 빨리 걷기, 스트레칭 등 규칙적인 운동의 중요성을 알려야 하며, 물리치료사나 운동생리학자에게 의뢰하는 것이 도움이 될 수 있습니다. 수동 스트레칭, 마사지, 온열 치료, 침술, 압통점에 리도카인과 같은 국소 마취제 주사 등의 근막 치료는 종종 섬유근육통의 근육통을 개선할 수 있습니다.72
아직 연구 중이지만,73 다발성 경화증에 대한 장기 면역 억제 요법은 지금까지 기대했던 효과를 얻지 못했습니다.5 이전 임상 시험에서 경구용 사이클로스포린이나 메토트렉세이트는 주관적인 증상의 개선에도 불구하고 눈물샘이나 이하선 흐름에 큰 영향을 미치는 것으로 나타났으며 이러한 약제는 중간 정도의 독성 효과도 있는 것으로 나타났습니다. 면역억제제는 SS와 같은 치명적이지 않은 만성 질환이 있는 환자에게는 주의해서 사용해야 합니다.
간 침범은 드물게 발생하며 SS 환자의 5%에게 영향을 미칩니다. 경증의 원발성 담즙성 간경변증 환자는 우르소데옥시콜산으로 치료할 수 있습니다.66 지속적이고 점진적인 간 효소 상승의 경우 프레드니손과 아자티오프린이 필요할 수 있습니다. 또한 드물게 만성 위축성 위염이 일부 SS 환자에서 발생합니다.66 위식도 역류 질환은 제산제, 히스타민2 차단제 또는 양성자 펌프 억제제로 관리할 수 있습니다.
피부 건조를 개선하기 위한 비약물적 조치로는 목욕 후 부드럽게 물기를 닦아내고 소량의 수분을 남겨둔 다음 보습제를 바르는 것이 있습니다. 또한 고감마글로불린혈증성 자반증의 경우 몸에 꼭 맞지 않는 헐렁한 옷을 입어야 합니다. 가습기, 분비 촉진제, 구아이페네신은 건조 기관지 관리에 도움이 될 수 있습니다.
Summary
Sjögren syndrome is a common autoimmune disease, the diagnosis and treatment of which are frequently delayed. Because this disease is systemic, it can exhibit a wide range of clinical manifestations that contribute to confusion and delay in diagnosis. Patients with SS are often referred to several specialists including rheumatologists, primary care physicians, ophthalmologists, and dentists. Frequently these clinicians see only a small part of the entire picture, making diagnosis extremely difficult. An increased awareness of SS and its many and varied manifestations encourages a more expansive approach to diagnosing this disease. The use of recently refined criteria for diagnosis can assist in identifying patients with SS early.
Although SS is a benign and non–life-threatening disorder, patients should be prescribed appropriate treatments to improve quality of life and avoid complications. Unfortunately, no treatment is currently available to decrease the glandular lymphocytic infiltration that contributes to the exocrine gland dysfunction of SS. Moisture replacement and preservation methods, such as tear and saliva substitutes and moisturizing lotions, can help to relieve oral and ocular dryness by stimulating exocrine secretions. Corticosteroids and therapies specific to affected organs or systems (eg, ursodeoxycholic acid and intravenous immunoglobulin for liver and neurologic involvement, respectively) can be used to treat systemic manifestations of disease. The use of all available diagnostic and treatment modalities will help to reduce the time to diagnosis and preserve the health and quality of life of patients with SS.
쇼그렌 증후군은
흔한 자가 면역 질환으로 진단과 치료가 자주 지연되는 질환입니다.
이 질환은 전신성 질환이기 때문에
다양한 임상 증상을 보여
진단에 혼란을 주고
지연을 초래할 수 있습니다.
ss 환자는
류마티스 전문의, 주치의, 안과 전문의, 치과 전문의 등
여러 전문의에게 의뢰되는 경우가 많습니다.
이러한 임상의들은
전체 상황의 일부만 보는 경우가 많기 때문에
진단이 매우 어렵습니다.
ss와 그 다양하고 많은 증상에 대한 인식이 높아지면서
이 질환을 진단하기 위한 보다 광범위한 접근 방식이 장려되고 있습니다.
최근 세분화된 진단 기준을 사용하면 SS 환자를 조기에 식별하는 데 도움이 될 수 있습니다.
ss은 생명을 위협하지 않는 양성 질환이지만,
삶의 질을 개선하고 합병증을 예방하기 위해 적절한 치료법을 처방받아야 합니다.
안타깝게도 현재로서는
외분비샘 기능 장애의 원인이 되는
선상 림프구 침윤을 감소시킬 수 있는 치료법은 없습니다.
눈물 및 타액 대체제,
보습 로션과 같은 수분 대체 및 보존 방법은
외분비 분비를 자극하여
구강 및 안구 건조를 완화하는 데 도움이 될 수 있습니다.
코르티코스테로이드 및 영향을 받는 장기 또는 시스템에
특정한 치료법(예: 간 및 신경계 침범에 대한 우르소데옥시콜산 및 정맥 내 면역글로불린)을 사용하여
질병의 전신 증상을 치료할 수 있습니다.
사용 가능한 모든 진단 및 치료 방식을 사용하면
진단 시간을 단축하고
SS 환자의 건강과 삶의 질을 보존하는 데 도움이 될 것입니다.
Corresponding author and reprints: Stuart S. Kassan, MD, Clinical Professor of Medicine (Rheumatic Disease), University of Colorado Health Sciences Center, 4200 W Conejos Pl, Suite 314, Denver, CO 80204-1333 (e-mail: s.kassan@juno.com).
Accepted for publication June 30, 2003.
We thank Daiichi Pharmaceutical Corporation, Montvale, NJ, for funding and IMPRINT Publication Science, New York, NY, for their editorial assistance.
References
1.
Anaya JMTalal N Sjögren's syndrome. Kassirer JPGreene HLeds. Current Therapy in Adult Medicine. Baltimore, Md4th ed. Mosby1997;1291- 1298Google Scholar
2.
Papiris SAManiati MConstantopoulos SH et al. Lung involvement in primary Sjögren's syndrome is mainly related to the small airway disease. Ann Rheum Dis. 1999;5861- 64PubMedGoogle ScholarCrossref
3.
Tsokos MLazarou SAMoutsopoulos HM Vasculitis in primary Sjögren's syndrome: histologic classification and clinical presentation. Am J Clin Pathol. 1987;8826- 31PubMedGoogle Scholar
4.
Tumiati BCasoli PParmeggiani A Hearing loss in the Sjögren syndrome. Ann Intern Med. 1997;126450- 453PubMedGoogle ScholarCrossref
5.
Vlachoyiannopoulos PG Therapy of Sjögren's syndrome: new aspects and future directions. Ann Med Interne (Paris). 1998;14949- 53PubMedGoogle Scholar
6.
Dafni UGTzioufas AGStaikos P et al. Prevalence of Sjögren's syndrome in a closed rural community. Ann Rheum Dis. 1997;56521- 525PubMedGoogle ScholarCrossref
7.
Skopouli FNDafni UIoannidis JPMoutsopoulos HM Clinical evolution, and morbidity and mortality of primary Sjögren's syndrome. Semin Arthritis Rheum. 2000;29296- 304PubMedGoogle ScholarCrossref
8.
Manthorpe RAsmussen KOxholm P Primary Sjögren's syndrome: diagnostic criteria, clinical features, and disease activity. J Rheumatol. 1997;24 (suppl) 8- 11PubMedGoogle Scholar
9.
Strand VTalal N Advances in the diagnosis and concept of Sjögren's syndrome (autoimmune exocrinopathy). Bull Rheum Dis. 1979-1980;301046- 1052PubMedGoogle Scholar
10.
Robinson CPYamachika SBounous DI et al. A novel NOD-derived murine model of primary Sjögren's syndrome. Arthritis Rheum. 1998;41150- 156PubMedGoogle ScholarCrossref
11.
Fox RIKang HI Pathogenesis of Sjögren's syn