- nature
- scientific reports
- articles
- article
Exploring the impact of integrated polyvagal exercises and knee reinforcement in females with grade II knee osteoarthritis: a randomized controlled trial
- Article
- Open access
- Published: 03 November 2023
Exploring the impact of integrated polyvagal exercises and knee reinforcement in females with grade II knee osteoarthritis: a randomized controlled trial
- Moattar Raza Rizvi,
- Ankita Sharma,
- Shahnaz Hasan,
- Fuzail Ahmad,
- Mohammad Rehan Asad,
- Amir Iqbal &
- Ahmad H. Alghadir
Scientific Reports volume 13, Article number: 18964 (2023) Cite this article
5773 Accesses
5 Citations
Abstract
This study aimed to compare the effects of knee strengthening exercises to those of polyvagal theory–based exercises combined with knee strengthening exercises on selected outcomes in women with grade II knee osteoarthritis (OA). A randomized controlled trial was conducted, in which 60 female participants diagnosed with grade II knee OA, with a mean age of 57.27 ± 7.81 years and knee pain rated between 4 and 7 on the visual analog scale (VAS), were assigned to either the knee strengthening exercise group (Group 1, n = 30) or the polyvagal theory–based exercise plus knee strengthening exercise group (Group 2, n = 30). Pre- and posttreatment assessment of outcome variables, including WOMAC scores (joint pain, joint stiffness, functional limitations, and the overall index), WHOQOL scores (overall quality of life, general health, physical, psychological, social, and environmental domains), and heart rate variability (HRV, time and frequency domains), were analyzed. Group 2 demonstrated significantly greater reductions in joint pain, stiffness, and functional limitations than Group 1 after the intervention. Group 2 presented with significantly improved WOMAC scores, indicating better overall outcomes. Group 2 showed significant improvements in the psychological and social domains regarding quality of life. There were no significant differences in the physical domain or the environmental domain. Group 2 showed a significant increase in high-frequency power (HF) and a significant decrease in the LF/HF ratio, suggesting improved autonomic regulation. A combination of polyvagal exercise and knee strengthening training resulted in superior outcomes compared to knee strengthening exercises alone in women with grade II knee OA. These findings support the potential effectiveness of incorporating polyvagal exercises as an adjunctive intervention for osteoarthritis management.
초록
본 연구는 2등급 무릎 골관절염(OA) 여성 환자를 대상으로
무릎 강화 운동과 다중미주신경 이론 기반 운동을 병행한 경우의 효과를 비교하는 것을 목표로 하였다.
무작위 대조 시험을 실시하였으며,
2등급 무릎 OA로 진단받은 60명의 여성 참가자(평균 연령 57.27±7.81세,
시각적 유사 척도(VAS) 기준 무릎 통증 4~7점)를
무릎 강화 운동군(그룹 1) 또는
다중미주신경 이론 기반 운동군(그룹 2)으로 배정하였다.
평균 연령 57.27±7.81세, 시각적 유사 척도(VAS) 기준 무릎 통증 4~7점인 참가자를 무작위 배정하여 무릎 강화 운동군(그룹 1, n=30)과 다중미주신경이론 기반 운동+무릎 강화 운동군(그룹 2, n=30)으로 나누었다. 치료 전후 결과 변수 평가에는 WOMAC 점수(관절 통증, 관절 강직, 기능적 제한, 종합 지수), WHOQOL 점수(종합 삶의 질, 일반 건강, 신체적, 심리적, 사회적, 환경적 영역), 심박 변이도(HRV, 시간 및 주파수 영역)가 포함되었으며 분석되었다.
개입 후 그룹 2는 그룹 1에 비해
관절 통증, 뻣뻣함, 기능적 제한에서 유의미하게 더 큰 감소를 보였다.
그룹 2는 WOMAC 점수가 유의미하게 개선되어
전반적인 결과가 더 우수함을 나타냈다.
그룹 2는 삶의 질 측면에서
심리적 및 사회적 영역에서 유의미한 개선을 보였다.
신체 영역과 환경 영역에서는 유의미한 차이가 없었다.
그룹 2는
고주파 전력(HF)의 유의미한 증가와 LF/HF 비율의 유의미한 감소를 보여
자율신경 조절이 개선되었음을 시사했다.
2등급 무릎 골관절염 여성에서
다중미주신경 운동과 무릎 강화 훈련의 병행은
무릎 강화 운동 단독 대비 우수한 결과를 초래했다.
이러한 결과는
골관절염 관리에 보조적 중재로
다중미주신경 운동을 통합하는 잠재적 효과성을 뒷받침한다.
Similar content being viewed by others
Article Open access27 May 2025
Article Open access16 August 2021
Article Open access23 May 2024
Introduction
Osteoarthritis (OA) is one of the most prevalent degenerative conditions resulting in disability, particularly among the elderly population. OA is the most common articular disease in the developed world and a leading cause of chronic disability, primarily due to knee OA and hip OA1. The prevalence of osteoarthritis (OA) is significantly higher in women than in men, and the disease significantly affects both physical and autonomic functions2.
Women are particularly susceptible to OA, accounting for approximately 60% of all OA patients3. Age is a major risk factor, with the prevalence in women escalating from approximately 10% at ages 25–34 to over 50% at ages 75 and older2. Exercise plays a pivotal role in sustaining overall well-being and enhancing quality of life, particularly among older women4. The physical implications of OA in women include pain, stiffness, limited mobility, and a reduced capacity to perform daily activities, leading to compromised quality of life5. Autonomic dysfunction, characterized by irregularities in heart rate variability and blood pressure, has been reported in patients with OA, suggesting a link between chronic pain and cardiovascular risk 6.
서론
골관절염(OA)은 특히 노인 인구에서 장애를 초래하는 가장 흔한 퇴행성 질환 중 하나입니다. OA는 선진국에서 가장 흔한 관절 질환이며, 주로 무릎 OA와 고관절 OA로 인해 만성 장애의 주요 원인입니다1. 골관절염(OA)의 유병률은 남성보다 여성에서 현저히 높으며, 이 질환은 신체 기능과 자율 신경 기능 모두에 상당한 영향을 미칩니다2.
여성은 특히 OA에 취약하여 전체 OA 환자의 약 60%를 차지한다3. 연령은 주요 위험 요인으로, 여성의 유병률은 25-34세 약 10%에서 75세 이상 50% 이상으로 급증한다2. 운동은 전반적인 건강 유지와 삶의 질 향상에 핵심적인 역할을 하며, 특히 고령 여성에게 중요합니다4. 여성의 골관절염이 신체에 미치는 영향으로는 통증, 뻣뻣함, 이동성 제한, 일상생활 수행 능력 저하 등이 있으며, 이는 삶의 질 저하로 이어집니다5. 심박 변이도와 혈압의 불규칙성을 특징으로 하는 자율신경계 기능 장애가 골관절염 환자에서 보고되어 만성 통증과 심혈관 위험 간의 연관성을 시사합니다 6.
The pathogenesis of knee OA involves a complex interplay of mechanical, genetic, and biochemical factors. It typically begins with cartilage degradation, leading to changes in the subchondral bone, inflammation, and alterations in joint tissues. As the cartilage wears down, the joint space narrows, bone spurs (osteophytes) may form, and the synovium (joint lining) may become inflamed. These processes collectively contribute to pain, stiffness, and functional limitations associated with knee OA7. The inflammatory response can be sustained by the release of additional pro-inflammatory factors from immune cells that have infiltrated the site, specifically neutrophils and monocytes. The persistent inflammatory response is a factor contributing to the degradation of cartilage and other joint components, exacerbating the discomfort and functional limitations associated with knee OA8. Grade II OA is characterized by mild to moderate joint damage. At this stage, the joint deterioration and functional limitations are significant enough to warrant intervention, yet the condition has not progressed to the extent that more invasive treatments, such as surgery, become necessary. Strengthening exercises can help improve muscle strength and joint stability, while vagal nerve stimulation may aid in regulating the autonomic nervous system and reducing pain perception9.
무릎 OA의 병리 기전은 기계적, 유전적, 생화학적 요인의 복잡한 상호작용을 포함한다. 일반적으로 연골 퇴화로 시작되어 하연골골 변화, 염증, 관절 조직 변형을 초래한다. 연골이 마모되면 관절 간격이 좁아지고, 골극(골극)이 형성될 수 있으며, 활막(관절 내막)에 염증이 생길 수 있다. 이러한 과정들이 종합적으로 작용하여 무릎 OA와 관련된 통증, 뻣뻣함 및 기능적 제한을 유발한다7. 염증 반응은 해당 부위에 침윤한 면역 세포, 특히 호중구와 단핵구로부터 추가적인 염증 유발 인자가 방출됨으로써 지속될 수 있다. 지속적인 염증 반응은 연골 및 기타 관절 구성 요소의 분해를 촉진하는 요인으로 작용하여 무릎 OA와 관련된 불편감과 기능적 제한을 악화시킨다8. 2등급 OA는 경증에서 중등도의 관절 손상이 특징이다. 이 단계에서는 관절 악화와 기능적 제한이 중재가 필요한 수준이지만, 수술과 같은 더 침습적인 치료가 필요할 정도로 진행되지는 않았습니다.
근력 강화 운동은 근력과 관절 안정성 향상에 도움이 될 수 있으며,
미주신경 자극은
자율신경계 조절과 통증 감지 감소에 기여할 수 있습니다9.
Strength training exercises effectively manage knee OA by improving muscle strength and function, thereby reducing pain and enhancing quality of life10. Studies consistently reveal increased rates of depression among individuals with OA compared to the general population. The chronic pain, functional limitations, and reduced quality of life associated with OA can contribute to the development or exacerbation of depressive symptoms11.
근력 강화 운동은
근력과 기능을 향상시켜 통증을 줄이고 삶의 질을 높임으로써
무릎 OA를 효과적으로 관리합니다10.
연구에 따르면
일반 인구 대비 골관절염 환자의 우울증 발생률이 지속적으로 높은 것으로 나타납니다.
골관절염과 관련된 만성 통증, 기능적 제한, 삶의 질 저하는
우울 증상의 발현 또는 악화에 기여할 수 있습니다11.
According to the polyvagal theory, the vagus nerve plays a role in a hierarchical model of reactions to stress and social interaction, which consists of two primary branches: the ventral vagus and the dorsal vagus. Vagal nerve stimulation (VNS) is employed to regulate the vagus nerve's function, aiming to achieve equilibrium between the ventral and dorsal vagus responses9. VNS has demonstrated the capacity to modulate neural activity, influence neurotransmitter release, and facilitate neuroplasticity. The research that has been conducted to date on VNS not only offers valuable insights into the complex interplay involving the vagus nerve, autonomic regulation, and social behavior but also sheds light on the intricate connection between VNS and the activity of norepinephrine, serotonin, and other neurotransmitters implicated in mood disorders and depression, which are common in patients with knee OA12.
다중 미주 신경 이론에 따르면,
미주 신경은 스트레스와 사회적 상호작용에 대한 반응의 계층적 모델에서 역할을 수행하며,
이는 복부 미주 신경과 등부 미주 신경이라는 두 가지 주요 분지로 구성됩니다.
미주신경자극(VNS)은
미주신경 기능을 조절하여
복부 미주신경과 등쪽 미주신경 반응 간의 균형을 이루는 것을 목표로 사용됩니다9.
VNS는
신경 활동을 조절하고,
신경전달물질 방출에 영향을 미치며,
신경가소성을 촉진하는 능력을 입증했습니다.
지금까지 수행된 VNS 연구는
미주신경, 자율신경 조절, 사회적 행동 간의 복잡한 상호작용에 대한
귀중한 통찰력을 제공할 뿐만 아니라,
무릎 골관절염 환자에게 흔히 나타나는
기분 장애 및 우울증과 관련된 노르에피네프린, 세로토닌 및 기타 신경전달물질의 활동과 VNS 간의 복잡한 연관성을 밝혀내고 있다12.
Strengthening exercises and vagal nerve stimulation are noninvasive interventions that can be implemented without the need for medications or surgical procedures. This makes them attractive treatment options for individuals with grade II knee OA who prefer a conservative approach or have contraindications for other treatments. Combining strengthening exercises with polyvagal exercises may offer potential synergistic effects in the management of OA symptoms. Strengthening exercises can help improve joint stability, reduce stress on the joint, and enhance overall physical function. Vagal nerve stimulation techniques following polyvagal exercises may help regulate autonomic function, reduce pain perception, and promote relaxation and emotional well-being. This study hypothesized that the combination of these interventions would lead to improved overall outcomes for individuals diagnosed with grade II knee OA.
Based on the above, the primary objective of this study was to investigate the potential benefits of combining strengthening exercises with polyvagal theory–based exercises as a noninvasive intervention for females diagnosed with grade II knee OA. Specifically, we aimed to assess whether the synergistic effects of these interventions could lead to improved joint stability, reduced pain perception, enhanced autonomic regulation, and improved overall physical function and emotional well-being among females with Grade II knee OA.
근력 강화 운동과 미주신경 자극은
약물이나 수술적 시술 없이 시행 가능한 비침습적 중재법입니다.
이는 보존적 접근을 선호하거나 다른 치료법에 금기 사항이 있는 2등급 무릎 골관절염 환자에게 매력적인 치료 옵션이 됩니다.
근력 강화 운동과 다중미주신경 운동을 병행하면
골관절염 증상 관리에 시너지 효과를 발휘할 가능성이 있습니다.
근력 강화 운동은 관절 안정성 향상, 관절 부하 감소, 전반적인 신체 기능 증진에 도움이 될 수 있습니다.
다중미주신경 운동 후 시행하는 미주신경 자극 기법은
자율신경 기능 조절, 통증 인식 감소, 이완 및 정서적 안녕 증진에 기여할 수 있습니다.
본 연구는 이러한 중재의 결합이 2등급 무릎 골관절염 진단을 받은 개인의 전반적인 결과 개선으로 이어질 것이라는 가설을 세웠습니다.
이에 따라 본 연구의 주요 목적은 2등급 무릎 OA 진단을 받은 여성을 대상으로 비침습적 중재로서 근력 강화 운동과 다중미주신경 이론 기반 운동의 병용이 가져올 잠재적 이점을 조사하는 것이었습니다. 구체적으로, 이러한 중재의 시너지 효과가 2등급 무릎 OA 여성 환자에서 관절 안정성 향상, 통증 인식 감소, 자율신경 조절 증진, 전반적인 신체 기능 및 정서적 웰빙 개선으로 이어질 수 있는지 평가하고자 했습니다.
Materials and methods
Study design
The study employed a two-arm parallel-group randomized comparative design. In this study, females (n = 60) diagnosed with grade II knee OA according to the Kellgren-Lawrence (KL) scale13 were randomized into two groups: Group 1 was assigned to perform knee strengthening exercises (n = 30), and Group 2 was assigned to perform both knee strengthening exercises and exercises based on polyvagal theory to stimulate the vagal nerve (n = 30).
Sample size
G*Power software version 3.1.9.4 (Heinrich-Heine-Universität Düsseldorf, Germany) was used to calculate the sample size. An a priori power analysis was performed for a repeated-measures analysis of variance examining within-groups and between-groups interactions with two groups and two repeated measures. For an effect size = 0.25, α = 0.05 and power = 0.95, the required sample size was n = 54 in total or 27 participants in each group. Considering an anticipated dropout rate of 10%, our study was designed to include a total of n = 60 participants at the start, distributed evenly (n = 30 individuals in each group).
Procedure
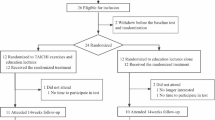
Ninety-four patients with complaints of knee pain underwent screening for grade II knee OA. However, thirty-four patients were excluded during the initial evaluation because they did not meet the inclusion criteria. The remaining 60 patients were randomly allocated into two intervention groups (with each group consisting of 30 patients): Group 1 performed only knee strengthening exercises, and Group 2 performed both knee strengthening exercises and polyvagal theory–based exercises. Randomization was performed at a 1:1 allocation ratio using sealed envelopes. Figure 1 illustrates the study procedures comprehensively through a CONSORT (2010) flow chart, outlining key stages such as assessment, enrollment, randomization, intervention allocation, follow-up, and data analysis.
재료 및 방법연구 설계
본 연구는 두 군 병렬 무작위 비교 설계를 채택하였다. 본 연구에서는 Kellgren-Lawrence (KL) 척도13에 따라 2등급 무릎 골관절염으로 진단된 여성(n=60)을 두 그룹으로 무작위 배정하였다: 그룹 1은 무릎 강화 운동(n=30)을 수행하도록 배정되었고, 그룹 2는 무릎 강화 운동과 미주신경 자극을 위한 다중미주신경이론 기반 운동(n=30)을 모두 수행하도록 배정되었다.
표본 크기
표본 크기는
G*Power 소프트웨어 버전 3.1.9.4(독일 뒤셀도르프 하인리히 하이네 대학교)를 사용하여 계산하였다. 사전 검정력 분석은 두 그룹과 두 반복 측정을 대상으로 그룹 내 및 그룹 간 상호작용을 검토하는 반복 측정 분산 분석을 위해 수행되었다. 효과 크기 0.25, α=0.05, 검정력 0.95 조건에서 필요한 표본 크기는 총 n=54명 또는 각 그룹당 27명이었다. 예상 탈락률 10%를 고려하여, 본 연구는 시작 시 총 n=60명의 참가자를 포함하도록 설계되었으며, 각 그룹에 균등하게 배정되었다(각 그룹당 n=30명).
절차
무릎 통증을 호소하는 94명의 환자를 대상으로
2등급 무릎 골관절염 선별 검사를 실시했습니다.
그러나 초기 평가 과정에서 포함 기준을 충족하지 못한 34명의 환자가 제외되었습니다.
남은 60명의 환자는
무작위로 두 개 중재군(각 군 30명)으로 배정되었습니다:
1군은 무릎 강화 운동만 수행했고,
2군은 무릎 강화 운동과 다중미주신경이론 기반 운동을 병행했습니다.
무작위 배정은 밀봉된 봉투를 사용하여 1:1 배정 비율로 수행되었습니다. 그림 1은 평가, 등록, 무작위 배정, 중재 배정, 추적 관찰, 데이터 분석과 같은 주요 단계를 개요로 제시하는 CONSORT(2010) 흐름도를 통해 연구 절차를 종합적으로 보여줍니다.
Figure 1
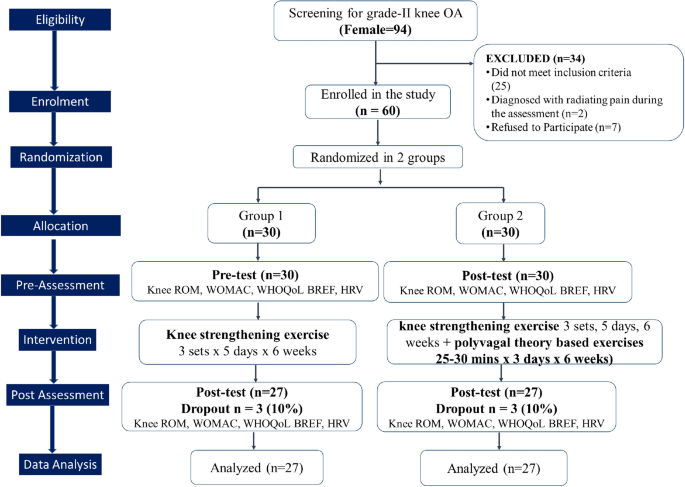
A CONSORT (2010) flow chart of the study design.
Study participantsInclusion criteria
This study included women between 45 and 60 years of age who had knee pain and were diagnosed with grade II unilateral knee OA. The decision was made to exclusively enroll female patients in this study because the incidence of knee osteoarthritis is higher in women than in men. Additionally, this approach was taken to address the potential impact of sex-related differences in critical factors such as muscle strength and mass.
Exclusion criteria
The criteria for exclusion were as follows: (i) engagement in physical exercise training within the previous year; (ii) the presence of cardiovascular diseases and/or musculoskeletal disorders that would hinder participation in exercises; (iii) a radiographic grade of 1 or > 2 according to the Kellgren-Lawrence scale; (iv) a history of knee joint surgery; (v) consumption of nonsteroidal anti-inflammatory drugs within the preceding three months for knee pain; and (vi) intra-articular administration of hyaluronic acid and/or corticosteroids within the preceding six months.
그림 1
연구 설계의 CONSORT(2010) 흐름도.
연구 참여자포함 기준
본 연구는 무릎 통증이 있고 2등급 일측성 무릎 골관절염(OA) 진단을 받은 45세에서 60세 사이의 여성을 포함했습니다.
무릎 골관절염 발생률이 남성보다 여성에서 더 높기 때문에
본 연구에는 여성 환자만을 등록하기로 결정했습니다.
또한 근력 및 근량과 같은 중요한 요인에 대한
성별 관련 차이의 잠재적 영향을 고려하기 위해 이러한 접근 방식을 채택했습니다.
제외 기준
제외 기준은 다음과 같습니다:
(i) 지난 1년 이내에 신체 운동 훈련을 받은 경우;
(ii) 운동 참여를 방해할 수 있는 심혈관 질환 및/또는 근골격계 장애가 있는 경우;
(iii) 켈그렌-로렌스 척도에 따른 방사선학적 등급 1 또는 2 이상인 경우;
(iv) 무릎 관절 수술 이력;
(v) 무릎 통증으로 인해 지난 3개월 이내에 비스테로이드성 항염증제 복용;
(vi) 지난 6개월 이내에 관절 내 히알루론산 및/또는 코르티코스테로이드 투여.
Outcome measuresRange of motion
The angle of knee flexion was measured using an app-based goniometer (DrGoniometers, CDM S.r.L), a tool that has been established as reliable and validated14. The participants lay in a supine position with the hip and knee of the affected limb flexed to a 90-degree angle while the feet were relaxed. The smartphone containing the accelerometer-based goniometer application was placed on the middle third of the anterior tibia and held in place by the examiner during the movement from the initial position to the final position. The "initial position" refers to the starting point where the hip and knee of the affected limb are flexed to a 90-degree angle, while the feet remain relaxed. A touch on the screen at this position established the 0-degree reference point. Subsequently, as the leg is moved in flexion, the examiner touches the screen again, representing the "terminal position." This terminal position signifies the final point of knee flexion in the movement and is measured while the hip maintains the same 90-degree angle of flexion.
Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)
The WOMAC is a self-administered validated questionnaire used for the assessment of hip and knee OA15. The WOMAC consists of 24 items divided into three subscales: pain (5 questions), stiffness (2 questions), and physical function (17 questions). The subscale scores can vary from 0 to 20 for pain, 0– to 8 for stiffness, and 0–68 for physical function, with higher scores (out of a maximum score of 96) indicating worse outcomes16. After signing the consent form, the patients filled out the questionnaire questions related to pain, function and stiffness at 0 days and after 6 weeks.
Abbreviated WHO quality of life scale (WHOQOL-Bref)
To assess patients’ quality of life, the WHOQOL-Bref questionnaire was used17. This contains questions focusing on QoL related to the physical, psychological, social and environmental domains. The questionnaire comprises 26 questions on the individual's self-perceived health and well-being over the previous two weeks. Responses to questions are on a 1–5 Likert scale, where 1 represents “disagree” or “not at all” and 5 represents “completely agree” or “extremely”. The possible score in each case ranges from 0 to 100 points, with 100 points indicating no restrictions at all due to the affected knee, while a score of 0 points indicates the worst possible health status.
결과 측정 항목
관절 가동 범위
무릎 굴곡 각도는 신뢰성과 타당성이 입증된 앱 기반 각도계(DrGoniometers, CDM S.r.L)를 사용하여 측정하였다14. 참가자는 앙와위 자세로 누운 상태에서, 영향을 받은 사지의 고관절과 무릎을 90도 각도로 굴곡시키고 발은 이완된 상태로 유지하였다. 가속도계 기반 관절측정기 애플리케이션이 설치된 스마트폰은 전경골 중간 1/3 부위에 위치시켰으며, 검사자가 초기 위치에서 최종 위치로의 움직임 동안 고정했다. “초기 위치”란 환측의 고관절과 무릎이 90도 굴곡된 상태에서 발이 이완된 시작점을 의미한다. 이 위치에서 화면을 터치하여 0도 기준점을 설정했다. 이후 다리를 굴곡시키며 움직일 때 검사자가 화면을 다시 터치하여 “종말 위치”를 표시했다. 이 종말 위치는 운동 중 무릎 굴곡의 최종 지점을 의미하며, 고관절이 동일한 90도 굴곡 각도를 유지한 상태에서 측정되었다.
웨스턴 온타리오 및 맥마스터 대학 골관절염 지수(WOMAC)
WOMAC은 고관절 및 무릎 골관절염 평가에 사용되는 검증된 자가 평가 설문지입니다15. WOMAC은 통증(5문항), 경직(2문항), 신체 기능(17문항)의 세 가지 하위 척도로 구성된 24개 문항으로 이루어져 있습니다.
하위 척도 점수는
통증 0~20점,
뻣뻣함 0~8점,
신체 기능 0~68점으로,
점수가 높을수록(최대 96점) 결과가 나쁘다는 것을 나타냅니다16.
동의서에 서명한 후, 환자들은 0일차와 6주 후에 통증, 기능 및 뻣뻣함과 관련된 설문지 질문을 작성했습니다.
WHO 삶의 질 척도 요약판(WHOQOL-Bref)
환자의 삶의 질을 평가하기 위해 WHOQOL-Bref 설문지를 사용하였다17. 이 설문지는 신체적, 심리적, 사회적, 환경적 영역과 관련된 삶의 질에 초점을 맞춘 질문들로 구성되어 있다. 설문지는 지난 2주 동안 개인이 스스로 인식한 건강 및 웰빙에 관한 26개 문항으로 이루어져 있다. 질문 응답은 1~5점 리커트 척도로, 1점은 “전혀 그렇지 않다” 또는 “전혀 동의하지 않는다”를, 5점은 “완전히 동의한다” 또는 “매우 그렇다”를 나타냅니다. 각 항목의 점수 범위는 0점에서 100점까지이며, 100점은 해당 무릎으로 인한 제한이 전혀 없음을, 0점은 최악의 건강 상태를 의미합니다.
Resting heart rate
Resting heart rate (RHR) was assessed using the Omron HEM 742 automated oscillometric sphygmomanometer18. Participants followed specific instructions, including resting quietly for at least five minutes in a calm environment with an empty bladder. They were also advised not to engage in any physical activity; smoke; or consume alcohol, coffee, or tea for specific timeframes before the measurement. During RHR measurement, participants sat with their backs supported and arms at a 90° angle. RHR was measured twice, 15 min apart, and we used the average of these two measurements in beats per minute (bpm).
휴식 시 심박수
휴식 시 심박수(RHR)는 Omron HEM 742 자동 오실로메트릭 혈압계18을 사용하여 측정했습니다. 참가자들은 방광을 비운 상태에서 조용한 환경에서 최소 5분간 안정적으로 휴식하는 등 특정 지침을 따랐습니다. 또한 측정 전 특정 시간 동안 신체 활동, 흡연, 알코올·커피·차 섭취를 하지 않도록 권고받았습니다. RHR 측정 시 참가자는 등받이에 기대어 앉은 상태에서 팔을 90° 각도로 유지했습니다. RHR은 15분 간격으로 두 번 측정되었으며, 이 두 측정값의 평균을 분당 박동수(bpm)로 사용했습니다.
Heart rate variability
On the day of the assessment, participants were asked to lie supine for 10 min or more to attain complete relaxation. Their skin was prepared by using a razor to remove the hair from the intended site of the HR sensor (in males only), cleaning the skin and drying it with gauze. They were asked to sit in a chair with armrests. The participants were instructed to wear an HR sensor on an elastic chest strap around the thorax in direct contact with the skin. RR intervals (the time elapsed between two successive R-waves of the QRS signal on the electrocardiogram) were recorded at a sampling frequency of 1000 Hz using the HR sensor (Polar H7, Polar Electro Oy, Kempele, Finland), which was connected via Bluetooth to an Android smartphone application (Elite HRV, Asheville, NC, USA). A digital electrocardiogram (ECG) was recorded for 5 min, and blood pressure was assessed in a sitting position19.
Time-domain analysis of HRV offers insights into the heart rate's temporal characteristics and the autonomic nervous system's influence on cardiac regulation. The time-domain measures of HRV were derived from a series of RR intervals. Various time-domain HRV indices were examined, including the mean of the normal-to-normal RR interval (MeanRR), the root mean square of successive differences between adjacent RR intervals (RMSSD), and the standard deviation of normal-to-normal RR intervals (SDNN). Additionally, frequency-domain indices were explored to analyze the distribution of power spectra across different frequency bands, revealing sympathetic-parasympathetic balance and autonomic heart rate control. These indices included total power (TP), reflecting overall signal variability (0.003–0.4 Hz); low-frequency spectral power (LF), associated with both sympathetic and parasympathetic activity (0.04 and 0.15 Hz); high-frequency spectral power (HF), mainly linked to parasympathetic activity (0.15 and 0.4 Hz); normalized unit of low frequency (nuLF), representing the percentage of total power in the LF band and indicating the sympathetic-parasympathetic balance; normalized unit of high frequency (nuHF), expressing the percentage of total power in the HF band and signifying parasympathetic activity; and the ratio of low frequency to high frequency (LF/HF), frequently employed as an indicator of sympathetic-parasympathetic balance. A higher LF/HF ratio implies greater sympathetic activity, while a lower ratio indicates higher parasympathetic activity. Collectively, these HRV variables provide comprehensive insights into the relative contributions of the sympathetic and parasympathetic branches of the autonomic nervous system to heart regulation. All HR recordings underwent meticulous visual inspection to ensure stationarity and were corrected for artifacts and ectopic beats using Kubios' built-in piecewise cubic spline interpolation19.
심박 변이도
평가 당일 참가자들은 완전한 이완 상태를 위해 10분 이상 엎드린 자세로 누워있도록 요청받았습니다. 심박 센서 부착 예정 부위의 털을 면도기로 제거한 후(남성 참가자만 해당), 피부를 세척하고 거즈로 건조시켰습니다. 참가자들은 팔걸이가 있는 의자에 앉도록 안내받았습니다. 참가자들은 탄성 가슴 밴드를 가슴에 직접 부착하여 심박 센서를 착용하도록 지시받았습니다. (남성만 해당). 피부를 세척하고 거즈로 건조시킨 후 팔걸이가 있는 의자에 앉도록 안내했습니다. 참가자들은 탄성 가슴 스트랩을 흉부에 착용하여 피부에 직접 접촉하도록 지시받았습니다. RR 간격(심전도상 QRS 신호의 연속적인 두 R파 사이의 경과 시간)은 HR 센서(Polar H7, Polar Electro Oy, Kempele, Finland)를 사용하여 1000Hz의 샘플링 주파수로 기록되었으며, 이 센서는 블루투스를 통해 안드로이드 스마트폰 애플리케이션(Elite HRV, Asheville, NC, USA)에 연결되었습니다.
5분간 디지털 심전도(ECG)를 기록하고, 앉은 자세에서 혈압을 측정하였다19.
시간 영역 기반 HRV 분석은
심박수의 시간적 특성과 자율신경계가 심장 조절에 미치는 영향을 파악하는 데 유용하다.
시간 영역 기반 HRV 지표는 일련의 RR 간격으로부터 도출되었다. 다양한 시간 영역 HRV 지표를 검토했는데, 여기에는 정상 RR 간격의 평균(MeanRR), 인접 RR 간격 간의 연속적 차이의 제곱평균근(RMSSD), 정상 RR 간격의 표준편차(SDNN)가 포함되었습니다. 또한, 교감-부교감 균형과 자율적 심박 조절을 드러내는 다양한 주파수 대역에 걸친 파워 스펙트럼 분포를 분석하기 위해 주파수 영역 지표도 탐구했습니다. 이러한 지표에는 전체 신호 변동성을 반영하는 총 파워(TP)(0.003–0.4 Hz), 교감 및 부교감 활동과 연관된 저주파 스펙트럼 파워(LF)(0.04 및 0.15 Hz), 주로 부교감 활동과 연결된 고주파 스펙트럼 전력(HF, 0.15~0.4Hz); LF 대역의 총 전력 비율을 나타내며 교감-부교감 균형을 시사하는 저주파 정규화 단위(nuLF); 고주파 대역의 정규화 단위(nuHF), HF 대역의 총 전력 비율을 나타내며 부교감신경 활동을 의미함; 그리고 교감신경-부교감신경 균형의 지표로 자주 사용되는 저주파 대 고주파 비율(LF/HF). 높은 LF/HF 비율은 교감신경 활동이 더 강함을 의미하는 반면, 낮은 비율은 부교감신경 활동이 더 높음을 나타냅니다. 이러한 HRV 변수들은 종합적으로 자율신경계의 교감신경과 부교감신경 분지가 심장 조절에 기여하는 상대적 비중에 대한 포괄적인 통찰을 제공한다. 모든 HR 기록은 정적 상태를 보장하기 위해 세심한 시각적 검사를 거쳤으며, Kubios의 내장된 부분별 3차 스플라인 보간법19을 사용하여 인공 신호와 이소성 박동을 보정하였다.
InterventionsKnee strengthening exercise program
The targeted muscles, levels, types of exercises, and progression strategies are presented in Table 1. Each exercise was performed in 3 sets, and each repetition was held for 3 s. Both groups performed the exercises under the active supervision of the therapist 5 days a week for 6 weeks. The exercises were discontinued if an increase in pain was reported. The knee extensors, knee flexors, and gluteal muscles were targeted to improve the symptoms related to knee OA20.
무릎 강화 운동 프로그램
표적 근육, 수준, 운동 유형 및 진행 전략은 표 1에 제시되어 있습니다. 각 운동은 3세트씩 수행되었으며, 각 반복은 3초 동안 유지되었습니다. 두 그룹 모두 치료사의 적극적인 감독 하에 주 5일, 6주간 운동을 수행했습니다. 통증 증가가 보고될 경우 운동은 중단되었습니다. 무릎 외전근, 무릎 굴곡근 및 둔근을 표적으로 하여 무릎 골관절염(KOA) 관련 증상을 개선하기 위함입니다20.
표 1 무릎 관절염 환자를 위한 무릎 강화 운동 프로그램.
Table 1 Knee strengthening exercise program for patients with KOA.
Targeted musclesLevelType of exerciseSetsRepsProgression
| Knee extensors-open kinetic chain | Level 1 | Isometric quads sets | 3 | 10 | Progress to level 2 when 3 sets of 10 is no longer challenging, and the patient is performing the activity with ease and good form |
| Level 2 | Terminal knee extension | 3 | 10 | Progress to level 3 when 3 sets of 10 are no longer challenging, and the patient is performing the activity with ease and good form | |
| Level 3 | Terminal knee extension with weight | 3 | 10 | The weight was increased to 2 kgs depending upon the ease of the patient | |
| Knee extensors-closed kinetic chain | Level 1 | Terminal knee extension in standing with resistance band | 3 | 10 | The level of the resistance band is progressed sequentially progressing to squats |
| Level 2 | Supported half Squats | 1 | 10 | Deep squats with reduced weight | |
| Level 3 | Step-ups with the affected limb | 1 | 10 | Progress to 13 cm step if knee pain was not increased | |
| Hip extensors strengthening | Level 1 | Supine glut sets | 3 | 10 | Progress to level 2 when 3 sets of 10 is no longer challenging, and the patient is performing the activity with ease and good form |
| Level 2 | Supine bridging | 3 | 10 | Progress to level 3 when 3 sets of 10 are no longer challenging, and the patient is performing an activity with ease and good form | |
| Level 3 | Supine unilateral bridging | 3 | 10 | A 1 kg weight cuff was added when the patient was doing it with ease | |
| Knee flexors strengthening | Level 1 | Prone hamstrings curl up to 90 degrees | 3 | 10 | Progress to level 2 when 3 sets of 10 are no longer challenging, and the patient is performing the activity with ease and good form |
| Level 2 | Prone hamstrings curl with a weight | 3 | 10 | Progress to level 3 when 3 sets of 10 are no longer challenging, and the patient is performing the activity with ease and good form | |
| Level 3 | Standing hip extension with resistance band | 3 | 10 | The resistance of the band was increased when the patient was able to perform the exercises well |
Polyvagal exercise protocol
The polyvagal exercises were aimed at activating and regulating the autonomic nervous system, which plays a crucial role in physiological and emotional responses. These exercises were tailored and customized to stimulate the vagus nerve and thereby promote relaxation and improve social interaction following the principles of polyvagal theory9,21. The domains of exercise, types of exercise, procedure and duration of polyvagal exercise are presented in Table 2.
다중미주신경 운동 프로토콜
다중미주신경 운동은 생리적 및 정서적 반응에 중요한 역할을 하는 자율신경계를 활성화하고 조절하는 것을 목표로 한다. 이 운동들은 미주신경을 자극하여 이완을 촉진하고 사회적 상호작용을 개선하기 위해 다중미주신경 이론의 원칙에 따라 맞춤화 및 조정되었다9,21. 운동 영역, 운동 유형, 절차 및 다중미주신경 운동의 지속 시간은 표 2에 제시되어 있습니다.
Table 2 Tailored polyvagal exercise protocol 9,21.
Domains of exercisesType of exerciseProcedureDuration
| Sensory awareness exercises | Breathing exercises | In a calm position, focusing on breathing and keeping the awareness of inhalation and exhalation | 20–30 breaths (2–3 min) |
| Stand upright postures | Awareness of different standing postures like standing tall, standing with a broad base, and standing with arms overhead were given focusing on the body sensations and thoughts | 2–3 min | |
| Lying Calmly | Lying in a supine posture with eyes closed focusing on breathing and the positive thoughts | 3–4 min | |
| Mindfully walking | Walking in a calm area by keeping the awareness of the physical sensations and engaging the senses by looking and feeling the different senses | 3–4 min | |
| Progressive muscle relaxation | Systematic muscle tensing and relaxation | Starting from toes to head for tensing each muscle group for 5–10 secs and sequentially promoting the same | 3–4 min |
| Guided imagery | Envision of mind to a calm scene and scenario and engage the senses to bring life into it | 3–4 min | |
| Vocal toning exercises | Tongue trills | Touching the tongue on top of front teeth and making the sound of "I" | 1–2 min |
| Humming sounds | Sitting in a relaxed position and making humming sounds by keeping mouth closed | (10–12 breaths)1–2 min | |
| Vowel sounds | In relaxed sitting, during exhalation making a long vowel sound | (10–12 breaths)1–2 min | |
| Self-soothing touch exercises | Foot massage | Massaging your foot while paying attention to the sensations and feeling of touch | 1–2 min |
| Havening touch | Sitting in a calm place, keeping a positive mind away from distractions and touching your arms, face, and palms | 1–2 min | |
| Belly breathing | Place one hand on your abdomen, just below the ribcage. Take slow, deep breaths, allowing your belly to rise and fall with each inhalation and exhalation | 1–2 min |
Statistical analysis
In this study, data analysis was conducted using SPSS version 23.0 (IBM Corp, Armonk, NY). Descriptive statistics, such as the mean and standard deviation (SD), were employed to present quantitative variables. The normality of data was assessed using the Shapiro‒Wilk test. An independent t test was applied to assess whether the means of the two groups were significantly different from each other, given the variation within each group. Cohen's d was employed to estimate effect size, with a confidence interval of 95% and a significance level of p < 0.05. Based on Cohen's d as a measure of effect size, the differences were classified as small (d < 0.2), moderate (0.2 < d < 0.5) and large (d ≥ 0.5). Additionally, a 2 (group) × 2 (time) repeated-measures ANOVA was utilized to examine the simple effects of time and group as well as the time × group interaction effect on outcome variables. Subsequently, post hoc pairwise comparisons were conducted to further investigate significant findings.
Ethical approval and consent to participate
The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki and was reviewed and approved by the ethics subcommittee of King Saud University, Riyadh, Saudi Arabia, under file ID RRC-2019-14, dated 22-04-2019. In addition, the Institutional Ethical Committee at Manav Rachna International Institute of Research & Studies approved the study protocol under reference number EC/2023-24/033, since the participants included patients visiting the OPD. Each participant was asked to submit a signed informed consent form as proof of consent to participate in the study. To ensure transparency and accountability, the study protocol was registered in the clinical trial registry at https://www.ctri.nic.in/ with the identifier CTRI/2023/08/056055.
통계 분석
본 연구에서는 SPSS 버전 23.0(IBM Corp, Armonk, NY)을 사용하여 데이터 분석을 수행하였다. 평균 및 표준편차(SD)와 같은 기술통계량을 사용하여 정량적 변수를 제시하였다. 데이터의 정규성은 Shapiro‒Wilk 검정을 통해 평가하였다. 각 그룹 내 변동성을 고려하여 두 그룹의 평균이 서로 유의미하게 다른지 평가하기 위해 독립 표본 t-검정을 적용하였다. 효과 크기를 추정하기 위해 코헨의 d를 사용하였으며, 신뢰 구간은 95%, 유의 수준은 p<0.05로 설정하였다. 효과 크기 측정 지표인 코헨의 d를 기준으로 차이를 소효과(d<0.2), 중등도 효과(0.2<d<0.5), 대효과(d≥0.5)로 분류하였다. 추가로, 결과 변수에 대한 시간과 집단의 단순 효과 및 시간×집단 상호작용 효과를 분석하기 위해 2(집단)×2(시간) 반복측정 분산분석(ANOVA)을 활용하였다. 이후 유의한 결과를 추가로 조사하기 위해 사후 쌍간 비교를 수행하였다.
윤리적 승인 및 참여 동의
본 연구 설계는 1975년 헬싱키 선언의 윤리 지침을 준수하였으며, 사우디아라비아 리야드 소재 킹사우드대학교 윤리소위원회(파일 ID: RRC-2019-14, 2019년 4월 22일자)의 검토 및 승인을 받았습니다. 또한, 참가자 중 외래환자가 포함되었으므로 마나브 라크나 국제 연구 및 학문 연구소(Manav Rachna International Institute of Research & Studies)의 기관윤리위원회가 연구 프로토콜을 승인번호 EC/2023-24/033으로 승인하였습니다. 각 참가자는 연구 참여 동의 증빙으로 서명된 사전동의서를 제출하도록 요청받았습니다. 투명성과 책임성을 보장하기 위해 연구 프로토콜은 임상시험 등록기관 https://www.ctri.nic.in/에 CTRI/2023/08/056055 식별번호로 등록되었습니다.
Results
Table 3 presents the results of an independent t test to assess whether the mean values of the two groups (Group 1 and Group 2) were significantly different from each other for various outcome variables, specifically WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) and WHOQOL (World Health Organization Quality of Life) scores. On a comparison of the mean values of WOMAC subscales, although there was no significant difference in joint pain (t = − 1.06, p = 0.30), joint stiffness (t = − 1.08, p = 0.29) or functional limitations (t = − 1.38, p = 0.17) before the intervention, Group 2 demonstrated significantly greater reductions in joint pain (t = 11.55, p < 0.001), joint stiffness (t = 2.5, p = 0.02) and functional limitations (t = 5.17, p < 0.001) than Group 1 after the intervention. The effect size suggests a large difference, with Group 2 experiencing more substantial decreases in joint pain (d = 3.27), joint stiffness (d = 0.71) and functional limitations (d = 1.46). There was no significant difference in the mean WOMAC Index scores between Group 1 (68.60 ± 5.07) and Group 2 (71.32 ± 5.93) before the intervention (t = − 2.00, p = 0.05). However, after the intervention, Group 2 (30.60 ± 5.55) showed a significantly greater improvement in WOMAC scores than Group 1 (43.72 ± 5.12) (t = 8.69, p < 0.001). The effect size (Cohen's d) was 2.46, indicating a large difference between the groups. This suggests that Group 2 exhibited outcomes that were more favorable and were more effective in reducing the impact of the condition being assessed.
Table 3 Independent t test applied to compare the mean WOMAC and WHOQOL scores between Group 1 and Group 2.
Furthermore, independent t tests were conducted to compare the mean values of the WHOQOL variable; there were no significant differences in the ratings of overall quality of life and general health between the pre- and post-intervention timepoints in Group 1 and Group 2. In a comparison of the physical and environmental subdomains of the WHOQOL between Group 1 and Group 2, the difference was not significant for either pre- or post-intervention assessments. In a comparison of the psychological subdomain of the WHOQOL between Group 1 and Group 2, for the pre-intervention assessment, the difference in the mean scores was not statistically significant (t = − 1.39, p = 0.17), and the effect size was small. However, for the post-intervention assessment, there was a significant difference in the mean scores for the psychological domain between Group 1 and Group 2 (t = − 6.72, p < 0.001), with a large effect size (Cohen's d = − 1.9). Additionally, in the social domain of the WHOQOL, the two groups presented similar results in the pre-intervention assessment, with no significant difference in the mean scores (t = 0.12, p = 0.91) between Group 1 and Group 2. However, for the post-intervention assessment, there was a significant difference in the mean scores for the social domain between Group 1 and Group 2 (t = − 8.89, p < 0.001), with a large effect size (Cohen's d = − 2.51), indicating a substantial difference.
The t test results indicate that there were no significant differences in resting HR between Group 1 and Group 2 at either the pre-intervention or post-intervention assessment (Table 4). There were significant differences in the RR interval between Group 1 and Group 2 at both the pre- (t = 3.3, p < 0.001) and post-intervention (t = − 2.65, p = 0.01) assessments. Furthermore, the independent t test results indicated no significant differences between Group 1 and Group 2 in terms of SDNN or RMSSD measures at either timepoint.
Table 4 Independent t test applied to compare the mean values of HRV (time and frequency domains) between Group 1 and Group 2.
Independent t tests showed that there were no significant differences between Group 1 and Group 2 in LF, TP, nuLF, or nuHF at either the pretreatment or posttreatment timepoint. There was no significant difference in the pre-intervention comparison of HF between Group 1 (295.23 ± 72.19) and Group 2 (286.68 ± 90.47) (t = 0.37, p = 0.71, d = 0.1). However, Group 2 showed a significant increase in HF compared to Group 1 (t = − 4.08, p < 0.001, d = − 1.15) in the post-intervention assessment.
Before the intervention, there was no significant difference in the LF/HF ratio between Group 1 (1.89 ± 0.42) and Group 2 (2.04 ± 0.52) (t = − 1.1, p = 0.28, d = − 0.31). However, after the intervention, there was a significant difference in the LF/HF ratio between the groups (t = 3.87, p < 0.001, d = 1.09). Before the intervention, there were no significant differences in nuHF (Group 1: 21.56 ± 3.64, Group 2: 21.09 ± 4.03) between the groups (nuHF: t = 0.44, p = 0.66, d = 0.12). This suggests that the two groups initially had similar normalized HF values. After the intervention, there was a significant difference in nuHF (t = − 3.87, p < 0.001, d = − 1.1) between the groups.
Table 5 presents the results of repeated-measures ANOVA comparing outcome measures between Group 1 and Group 2, with time (pre- or post-intervention measurement) as the within-subjects factor and the outcome measure as the between-subjects factor.
Table 5 A repeated-measures ANOVA to compare outcome measures between two groups (1 and 2), with time (pre- or post-intervention measurement) as the within-subjects factor and the outcome measure as the between-subjects factor.
Both groups showed significant improvements in range of motion (ROM) after the intervention, with the mean difference in ROM being greater in Group 2. There was a significant effect of time, suggesting an overall improvement in ROM. Both Group 1 and Group 2 experienced significant improvements in joint pain, stiffness, functional limitations, and the WOMAC index. Group 2 exhibited larger mean differences and more substantial improvements in all assessed outcome measures than Group 1.
Both groups showed significant improvements in overall quality of life; general health; and the physical, psychological, social, and environmental domains. The time effects were significant, indicating an overall improvement in quality of life across all domains. Group effects were significant for the psychological domain and the social domain.
For resting HR (beats/min), there was a significant time effect between the pre- and post-intervention timepoints; however, the group effect (Group 1 vs. 2) was not significant. Regarding the time-domain HRV measures of Mean RR (ms), SDNN (ms), and RMSSD, both Group 1 and Group 2 showed significant improvements (a time effect) after the intervention. The interaction effects were significant for Mean RR, indicating that the change in Mean RR differed between the two groups. Comparing the mean differences, it appears that Group 2 had larger improvements in Mean RR, SDNN, and RMSSD than Group 1. Therefore, Group 2 generally showed changes that were more favorable in the HRV time domain variables, indicating a potential improvement in cardiovascular health. In the HRV frequency-domain analysis, there were no significant time or group effects for LF or HF. There was a significant time effect of TP but no group effect or time × group interaction. There was a significant time effect as well as a significant time × group interaction for the LF/HF ratio. There was a significant time effect for nuLF but no significant group or interaction effect. On the other hand, nuHF showed a significant time effect, group effect and time × group interaction.
결과
표 3은 두 그룹(그룹 1과 그룹 2)의 평균값이 다양한 결과 변수, 특히 WOMAC(웨스턴 온타리오 및 맥마스터 대학 골관절염 지수) 및 WHOQOL (세계보건기구 삶의 질) 점수에 대해 두 그룹(그룹 1과 그룹 2)의 평균값이 서로 유의미하게 다른지 평가한 독립 표본 t-검정 결과를 제시합니다. WOMAC 하위 척도의 평균값을 비교했을 때, 중재 전 관절 통증(t = -1.06, p = 0.30), 관절 경직(t = -1.08, p = 0.29) 또는 기능적 제한(t = -1.38, p = 0.17)에서는 유의미한 차이가 없었으나, 그러나 개입 후 그룹 2는 그룹 1에 비해 관절 통증(t=11.55, p<0.001), 관절 강직(t=2.5, p=0.02), 기능적 제한(t=5.17, p<0.001)에서 유의미하게 더 큰 감소폭을 보였다. 효과 크기는 큰 차이를 시사하며, 그룹 2는 관절 통증(d = 3.27), 관절 강직(d = 0.71), 기능적 제한(d = 1.46)에서 더 현저한 감소를 경험했다 . 중재 전 그룹 1(68.60±5.07)과 그룹 2(71.32±5.93)의 평균 WOMAC 지수 점수 간 유의한 차이는 없었다(t=−2.00, p=0.05). 그러나 중재 후 그룹 2(30.60±5.55)는 그룹 1(43.72±5.12)보다 WOMAC 점수에서 유의하게 더 큰 개선을 보였다(t=8.69, p<0.001). 효과 크기(Cohen's d)는 2.46으로, 두 그룹 간 큰 차이를 나타냈다. 이는 그룹 2가 더 유리한 결과를 보였으며 평가 대상 질환의 영향을 줄이는 데 더 효과적이었음을 시사한다.
표 3 그룹 1과 그룹 2 간 평균 WOMAC 및 WHOQOL 점수 비교를 위한 독립 표본 t-검정.
또한 WHOQOL 변수의 평균값을 비교하기 위해 독립 표본 t-검정을 수행한 결과, 그룹 1과 그룹 2 모두에서 중재 전후 시점 간 전반적 삶의 질 및 일반 건강 상태 평가에 유의미한 차이는 없었다. 그룹 1과 그룹 2 간 WHOQOL의 신체적 및 환경적 하위 영역 비교에서는 중재 전후 평가 모두에서 차이가 유의하지 않았다. 그룹 1과 그룹 2 간 WHOQOL 심리적 하위 영역 비교에서, 개입 전 평가 시 평균 점수 차이는 통계적으로 유의하지 않았으며(t = -1.39, p = 0.17), 효과 크기는 작았다. 그러나 개입 후 평가에서는 그룹 1과 그룹 2 간 심리적 영역의 평균 점수에 유의미한 차이가 있었으며(t = -6.72, p < 0.001), 효과 크기는 컸다(Cohen's d = -1.9). 또한 WHOQOL의 사회적 영역에서 두 그룹은 개입 전 평가에서 유사한 결과를 보였으며, 그룹 1과 그룹 2 간의 평균 점수에는 유의한 차이가 없었습니다(t=0.12, p=0.91). 그러나 중재 후 평가에서는 그룹 1과 그룹 2 간의 사회적 영역 평균 점수에 유의미한 차이가 있었으며(t = -8.89, p < 0.001), 효과 크기가 컸습니다(Cohen's d = -2.51). 이는 상당한 차이를 나타냅니다.
t-검정 결과, 개입 전 및 개입 후 평가에서 그룹 1과 그룹 2의 안정시 심박수에는 유의한 차이가 없었습니다(표 4). RR 간격은 개입 전(t = 3.3, p < 0.001)과 개입 후(t = -2.65, p = 0.01) 평가 시점 모두에서 그룹 1과 그룹 2 간 유의미한 차이가 있었다. 또한 독립 표본 t-검정 결과, SDNN 또는 RMSSD 측정값 측면에서 두 시점 모두 그룹 1과 그룹 2 간 유의미한 차이는 없었다.
표 4 그룹 1과 그룹 2 간 HRV(시간 및 주파수 영역) 평균값 비교를 위한 독립 표본 t-검정.
독립 표본 t-검정 결과, 치료 전후 시점에서 LF, TP, nuLF 또는 nuHF에 대해 그룹 1과 그룹 2 간 유의한 차이는 없었습니다. 개입 전 HF 비교에서 그룹 1(295.23±72.19)과 그룹 2(286.68±90.47) 간 유의한 차이는 없었다(t=0.37, p=0.71, d=0.1). 그러나 그룹 2는 개입 후 평가에서 그룹 1에 비해 HF가 유의하게 증가한 것으로 나타났습니다 (t = -4.08, p < 0.001, d = -1.15).
중재 전에는 그룹 1(1.89±0.42)과 그룹 2(2.04±0.52)의 LF/HF 비율에 유의한 차이가 없었습니다(t=−1.1, p=0.28, d=−0.31). 그러나 중재 후, 그룹 간 LF/HF 비율에 유의한 차이가 나타났다(t=3.87, p<0.001, d=1.09). 중재 전, 두 그룹 간 nuHF(그룹 1: 21.56 ± 3.64, 그룹 2: 21.09 ± 4.03)에는 유의한 차이가 없었습니다(nuHF: t = 0.44, p = 0.66, d = 0.12). 이는 두 그룹이 초기에는 유사한 정규화된 HF 값을 가졌음을 시사합니다. 개입 후, 두 집단 간 nuHF에 유의한 차이가 나타났다(t=−3.87, p<0.001, d=−1.1).
표 5는 시간(개입 전 또는 후 측정)을 내적 요인으로, 결과 측정을 외적 요인으로 하여 그룹 1과 그룹 2 간의 결과 측정을 비교한 반복측정 분산분석(ANOVA) 결과를 제시한다.
표 5 두 그룹(1과 2) 간 결과 측정을 비교하기 위한 반복측정 분산분석(ANOVA). 시간(개입 전 또는 후 측정)을 내적 요인으로, 결과 측정을 외적 요인으로 설정.
두 그룹 모두 중재 후 관절 가동 범위(ROM)에서 유의미한 개선을 보였으며, 그룹 2의 ROM 평균 차이가 더 컸다. 시간의 유의미한 효과가 관찰되어 ROM의 전반적 개선을 시사했다. 그룹 1과 그룹 2 모두 관절 통증, 뻣뻣함, 기능적 제한, WOMAC 지수에서 유의미한 개선을 경험했다. 그룹 2는 그룹 1보다 모든 평가된 결과 측정에서 더 큰 평균 차이와 더 상당한 개선을 보였다.
두 그룹 모두 전반적 삶의 질, 일반 건강, 신체적·심리적·사회적·환경적 영역에서 유의미한 개선을 보였다. 시간 효과는 유의하여 모든 영역에서 삶의 질이 전반적으로 개선되었음을 나타냈다. 그룹 효과는 심리적 영역과 사회적 영역에서 유의했다.
휴식 시 심박수(회/분)의 경우, 중재 전후 시점 간 유의한 시간 효과가 관찰되었으나, 그룹 효과(그룹 1 대 그룹 2)는 유의하지 않았다. 시간 영역 심박변이도 측정값인 평균 RR 간격(ms), SDNN(ms), RMSSD에 대해서는 그룹 1과 그룹 2 모두 중재 후 유의한 개선(시간 효과)을 보였다. 평균 RR에 대한 상호작용 효과는 유의하여, 평균 RR의 변화가 두 그룹 간에 차이가 있음을 나타냈다. 평균 차이를 비교해 보면, 그룹 2가 그룹 1보다 평균 RR, SDNN, RMSSD에서 더 큰 개선을 보인 것으로 보인다. 따라서 그룹 2는 전반적으로 HRV 시간 영역 변수에서 더 유리한 변화를 보였으며, 이는 심혈관 건강의 잠재적 개선을 시사한다. HRV 주파수 영역 분석에서는 LF 또는 HF에 대해 유의한 시간 효과나 그룹 효과가 없었다. TP에는 유의한 시간 효과가 있었으나 그룹 효과나 시간×그룹 상호작용은 없었다. LF/HF 비율에서는 유의한 시간 효과와 시간×그룹 상호작용이 관찰되었습니다. nuLF에서는 유의한 시간 효과가 있었으나 그룹 효과나 상호작용 효과는 없었습니다. 반면 nuHF는 유의한 시간 효과, 그룹 효과 및 시간×그룹 상호작용을 보였습니다.
Discussion
This study aimed to compare the effects of knee strengthening exercises (Group 1) and exercises based on polyvagal theory combined with knee strengthening exercises (Group 2) in females with grade II knee OA. The study assessed various outcome variables, including WOMAC scores (joint pain, joint stiffness, functional limitations, and the overall index) and WHOQOL scores measuring QoL; general health; and the physical, psychological, social, and environmental domains. Additionally, autonomic function was measured by heart rate variability (HRV) measures, which were analyzed in the time and frequency domains.
Polyvagal theory, proposed by Porges, suggests that the vagus nerve plays a crucial role in regulating the autonomic nervous system and influencing emotional states, stress responses, and social engagement. Engaging in activities that stimulate the vagus nerve, such as the exercises described, may promote relaxation, reduce anxiety, and enhance emotional regulation. These outcomes could ultimately contribute to a reduction in perceived pain and an increase in quality of life in patients with knee osteoarthritis9. Vagus nerve stimulation has multifaceted mechanisms that could explain its potential benefits for individuals with knee osteoarthritis. It activates the parasympathetic nervous system, increasing vagal tone while reducing sympathetic activity, which might lead to pain reduction and enhanced well-being9. Moreover, vagal stimulation exhibits anti-inflammatory effects, regulating immune responses and potentially alleviating arthritic joint inflammation, thus contributing to pain relief22. Additionally, by influencing central pain mechanisms and neural pathways, VNS can modulate pain perception and processing, thereby potentially enhancing pain relief22. Finally, vagal stimulation's impact on neuroplasticity could lead to lasting improvements in pain and quality of life for those with knee osteoarthritis5.
The WOMAC assessment for knee OA is a sensitive tool, well suited for detecting changes in symptoms and function over time or in response to interventions. This evaluation captures the patient's perspective, facilitating a comprehensive assessment of the impact of knee OA on daily life and functioning16. In the present study, both groups displayed effects as measured by WOMAC subscales; however, the group that performed VNS exercises demonstrated notable improvements in pain, stiffness and functional limitations. Notably, the results indicated that Group 2 exhibited significantly greater reductions in joint pain, joint stiffness, and functional limitations than Group 1 after 6 weeks. Group 2 also exhibited significant improvements in the WOMAC index scores, reflecting favorable overall outcomes. In terms of quality of life, Group 2 demonstrated marked enhancements in the psychological and social domains compared to Group 1. However, there were no significant differences observed in the physical domain or the environmental domain.
Muscle and skeletal problems constitute over a quarter of nonlethal health losses, with pain being the most significant contributor23. Chronic pain related to OA not only restricts social functioning but also heightens the risk of psychological issues24, depression25 and diminished work capabilities26. The finding of this study underscores the favorable response observed with polyvagal exercises, which predominantly focus on relaxation. As a nonpharmacological intervention, relaxation is increasingly employed to alleviate pain and enhance pain management27. This finding aligns with Turk and Winter’s research, illustrating that achieving a state of physical and mental relaxation influences psychological and bodily well-being, fostering calmness and contributing to the reduction of pain28. Further reinforcement is derived from a study by Onivea-Zefra et al., who demonstrate the potential of guided imagery relaxation in reducing pain levels among fibromyalgia patients. Through the utilization of visualizations and mental imagery techniques, this approach promotes relaxation and helps in alleviating pain perception29.
Another study by Morone and Greco reinforces the findings that guided imagery and relaxation offer clinical pain management benefits for individuals with knee OA30. The reduction in pain, functional limitations and stiffness could also be attributed to the effects of strengthening exercises. Strength training has been linked to potential disease-modifying impacts in OA. Regular exercise can promote joint health, stimulate cartilage metabolism, and improve muscle strength and joint stability31.
In individuals with osteoarthritis, pain is the most prevalent complaint and a primary contributor to reduced health-related quality of life (HRQoL). In this study, both groups demonstrated significant improvements across various domains of quality of life, including overall quality; general health; and physical, psychological, social, and environmental aspects. Notably, Group 2 exhibited more substantial enhancements in overall quality of life, general health, psychological, social, and environmental domains than Group A, which underwent vagal nerve stimulation-based exercise. The improvement in the physical domain is attributed to the 6-week exercise regimen, a sentiment that aligns with Smith et al.’s findings, emphasizing the efficacy of a scalable exercise program in enhancing the well-being and function of hip and knee OA patients32. Various techniques, including deep breathing, meditation, relaxation exercises, and specific physical activities, can stimulate the vagus nerve and enhance its functionality. These exercises may facilitate relaxation, stress reduction, and overall well-being. Goff et al.’s findings agree with ours, suggesting that patient education positively impacts conservative treatment and can be productively used in concert with it33. Our results are corroborated by Ebenezer et al.’s study, which revealed that patients treated with yoga experienced substantial improvements in QoL, paralleling the effects of therapeutic exercise on OA patients. The shared impact of yoga on emotional stability and quality of life, a factor pivotal in pain reduction and enhanced quality of life, is a significant highlight of their research34.
Vagal stimulation, in line with the polyvagal theory, is also emphasized by Wang et al., who suggest that practices such as yoga—a form of physical and relaxation exercise—have a systemic effect. By stimulating parasympathetic pathways, yoga reduces perceived pain and improves QoL35. Regarding heart rate variability (HRV), Group 2 exhibited a notable increase in high-frequency power (HF) and a significant decrease in the LF/HF ratio, indicating enhanced autonomic regulation. These outcomes imply that the combination of polyvagal exercises and knee-strengthening training yields a favorable impact on HRV, reflecting improved cardiovascular health. Interestingly, a positive correlation exists between disability and cardiovascular health in patients with knee OA. This is underscored by Tsubio et al.’s discovery of a connection between degenerative diseases and causes of death in Japan, revealing that individuals with knee OA are at an elevated risk of heart attacks leading to mortality36. This underscores the imperative for enhanced autonomic regulation in knee OA patients.
The observed changes in HRV parameters can be attributed to the stimulation of the vagal nerve. This emphasizes the contention of the polyvagal theory that the physiological state is not merely a correlate but a fundamental component of emotions and moods. Within this theoretical framework, the autonomic state functions as an intermediary variable that influences our perception and evaluation of environmental stimuli. The reflexive assessment of cues as neutral, positive or threatening can vary based on an individual's physiological state. Functionally, changes in an individual’s state can lead to a shift in the accessibility of different brain structures, facilitating social communication or eliciting defensive responses such as fight/flight or shutdown37. Goldbeck et al. also emphasized the importance of yoga-based exercises in enhancing HRV parameters, consequently improving parasympathetic activity38.
The study had a few limitations that should be noted. It had a small sample size, exclusively female participants, and a lack of long-term follow-up. While generalization to the wider population should be approached with caution, the study's findings still contribute to a broader understanding of the potential benefits of the interventions within this specific subset of patients. The decision to include female participants only was driven by the fact that knee osteoarthritis is more commonly observed in females than in males. Evaluating the sustainability and durability of the benefits conferred by polyvagal exercises in the long term could provide a more comprehensive understanding of their effects and guide clinical recommendations. Furthermore, there was no control group, and blinding procedures were not implemented. The inability to implement blinding in this study is attributable to the nature of the interventions employed, which made it a practical challenge to blind participants and researchers to the group assignments, as the participants themselves needed to be aware of the specific exercises they were performing. The study relied on self-reported measures and did not use objective measures. A total reliance on self-reported measures, without the use of objective assessments, introduces the potential for measurement bias due to participants' subjective perceptions and recall biases. Integrating objective measures such as biomechanical assessments or biomarkers would offer a more comprehensive understanding of the interventions' effects. Finally, the dropout rate was 10%, which may have affected the representativeness of the final sample and introduced potential bias.
논의
본 연구는 2등급 무릎 골관절염을 가진 여성 대상에서 무릎 강화 운동(그룹 1)과 다중미주신경이론 기반 운동과 무릎 강화 운동을 병행한 그룹(그룹 2)의 효과를 비교하는 것을 목표로 하였다. 연구에서는 WOMAC 점수(관절 통증, 관절 뻣뻣함, 기능적 제한, 종합 지수) 및 삶의 질(QoL), 일반 건강, 신체적, 심리적, 사회적, 환경적 영역을 측정하는 WHOQOL 점수를 포함한 다양한 결과 변수를 평가하였다. 또한 자율신경 기능은 심박 변이도(HRV) 측정을 통해 평가되었으며, 시간 영역과 주파수 영역에서 분석되었다.
Porges가 제안한 다중미주신경 이론은 미주신경이 자율신경계 조절과 정서 상태, 스트레스 반응, 사회적 참여에 중요한 역할을 한다고 제안한다. 본 연구에서 설명된 운동과 같이 미주신경을 자극하는 활동은 이완 촉진, 불안 감소, 정서 조절 향상에 기여할 수 있다. 이러한 결과는 궁극적으로 무릎 골관절염 환자의 통증 감지 감소와 삶의 질 향상에 기여할 수 있다9. 미주신경 자극은 무릎 골관절염 환자에게 잠재적 이점을 제공할 수 있는 다각적인 기전을 지닙니다. 이는 부교감신경계를 활성화하여 미주신경 긴장도를 높이고 교감신경 활동을 감소시켜 통증 감소와 웰빙 증진으로 이어질 수 있습니다9. 또한 미주신경 자극은 항염증 효과를 나타내며, 면역 반응을 조절하고 관절염성 관절 염증을 완화시켜 통증 경감에 기여할 수 있습니다22. 추가로, 중추 통증 기전과 신경 경로에 영향을 미침으로써 VNS는 통증 인식과 처리를 조절하여 잠재적으로 통증 완화를 강화할 수 있습니다22. 마지막으로, 미주 자극이 신경가소성에 미치는 영향은 무릎 골관절염 환자의 통증과 삶의 질에 지속적인 개선을 가져올 수 있습니다5.
무릎 골관절염에 대한 WOMAC 평가는 시간 경과에 따른 증상 및 기능 변화 또는 중재에 대한 반응을 감지하는 데 적합한 민감한 도구입니다. 이 평가는 환자의 관점을 포착하여 무릎 OA가 일상생활과 기능에 미치는 영향을 포괄적으로 평가할 수 있게 합니다16. 본 연구에서 두 그룹 모두 WOMAC 하위 척도로 측정된 효과를 보였으나, VNS 운동을 수행한 그룹은 통증, 뻣뻣함 및 기능적 제한에서 현저한 개선을 보였습니다. 특히, 결과는 6주 후 그룹 2가 그룹 1보다 관절 통증, 관절 뻣뻣함 및 기능적 제한에서 유의미하게 더 큰 감소를 보였음을 나타냈습니다. 그룹 2는 WOMAC 지수 점수에서도 유의미한 개선을 보였으며, 이는 전반적으로 긍정적인 결과를 반영한다. 삶의 질 측면에서 그룹 2는 그룹 1에 비해 심리적 영역과 사회적 영역에서 현저한 향상을 보였다. 그러나 신체적 영역이나 환경적 영역에서는 유의미한 차이가 관찰되지 않았다.
근골격계 문제는 비치명적 건강 손실의 4분의 1 이상을 차지하며, 그중 통증이 가장 큰 요인이다23. 골관절염 관련 만성 통증은 사회적 기능을 제한할 뿐만 아니라 심리적 문제24, 우울증25 및 업무 능력 저하26의 위험을 높입니다. 본 연구 결과는 주로 이완에 초점을 맞춘 다중 미주신경 운동의 긍정적 반응을 강조합니다. 비약물적 중재로서 이완은 통증 완화 및 통증 관리 향상을 위해 점점 더 많이 활용되고 있습니다27. 이 결과는 Turk와 Winter의 연구와 일치하며, 신체적·정신적 이완 상태를 달성하는 것이 심리적·신체적 웰빙에 영향을 미쳐 평온함을 조성하고 통증 감소에 기여함을 보여준다28. Onivea-Zefra 등의 연구는 섬유근통 환자의 통증 수준 감소에 있어 유도 이미지 이완법의 잠재력을 입증함으로써 이를 더욱 강화한다.
시각화 및 정신적 이미지 기법을 활용하는 이 접근법은 이완을 촉진하고 통증 인식을 완화하는 데 도움을 준다29. 모로네(Morone)와 그레코(Greco)의 또 다른 연구는 무릎 골관절염 환자에게 유도 이미지 및 이완이 임상적 통증 관리 혜택을 제공한다는 결과를 재확인한다30. 통증, 기능적 제한 및 뻣뻣함의 감소는 강화 운동의 효과에도 기인할 수 있다. 근력 운동은 골관절염에서 잠재적인 질병 수정 효과를 보인 것으로 알려져 있다.
규칙적인 운동은 관절 건강 증진, 연골 대사 촉진, 근력 및 관절 안정성 향상에 기여할 수 있다31.
골관절염 환자에게 통증은 가장 흔한 증상이자 건강 관련 삶의 질(HRQoL) 저하의 주요 원인이다. 본 연구에서 두 그룹 모두 전반적 삶의 질, 일반 건강, 신체적·심리적·사회적·환경적 측면 등 삶의 질의 다양한 영역에서 유의미한 개선을 보였다. 특히, 미주신경 자극 기반 운동을 시행한 그룹 A에 비해 그룹 2는 전반적 삶의 질, 일반 건강, 심리적, 사회적, 환경적 영역에서 더 큰 향상을 보였다. 신체적 영역의 개선은 6주간의 운동 프로그램 덕분으로, 이는 Smith 등의 연구 결과와 일치하며, 확장 가능한 운동 프로그램이 고관절 및 무릎 골관절염 환자의 웰빙과 기능 향상에 효과적임을 강조한다32. 심호흡, 명상, 이완 운동 및 특정 신체 활동을 포함한 다양한 기법은 미주 신경을 자극하고 그 기능을 향상시킬 수 있습니다. 이러한 운동은 이완, 스트레스 감소 및 전반적인 웰빙을 촉진할 수 있습니다. Goff 등의 연구 결과는 우리의 결과와 일치하며, 환자 교육이 보존적 치료에 긍정적인 영향을 미치고 이를 함께 효과적으로 활용할 수 있음을 시사합니다33. 에베네저(Ebenezer) 등의 연구는 요가 치료를 받은 환자들이 골관절염 환자에 대한 치료적 운동과 유사한 삶의 질(QoL)의 상당한 개선을 경험했음을 밝혀 우리 결과를 뒷받침한다. 요가가 정서적 안정성과 삶의 질에 미치는 공통된 영향은 통증 감소와 삶의 질 향상에 핵심적인 요소로서, 이들의 연구에서 중요한 강조점이다34.
왕(Wang) 등의 연구에서도 다중미주신경 이론에 부합하는 미주신경 자극이 강조되며, 신체적 이완 운동 형태인 요가와 같은 실천이 전신적 효과를 가질 수 있다고 제안한다. 요가는 부교감 신경 경로를 자극하여 인지된 통증을 감소시키고 삶의 질을 향상시킵니다35. 심박 변이도(HRV) 측면에서, 그룹 2는 고주파 전력(HF)의 현저한 증가와 LF/HF 비율의 유의미한 감소를 보였는데, 이는 자율 신경 조절 기능이 향상되었음을 시사합니다. 이러한 결과는 다중미주신경 운동과 무릎 강화 훈련의 병행이 심박 변이도에 긍정적인 영향을 미쳐 심혈관 건강 개선을 반영함을 의미합니다. 흥미롭게도 무릎 골관절염 환자에게서 장애 정도와 심혈관 건강 사이에는 양의 상관관계가 존재한다. 이는 쓰비오(Tsubio) 등이 일본에서 퇴행성 질환과 사망 원인 간의 연관성을 발견한 연구에서 무릎 골관절염 환자가 사망으로 이어지는 심장마비 위험이 높다는 사실36을 밝혀낸 것으로도 입증된다. 이는 무릎 골관절염 환자에게 자율신경 조절 능력 향상이 시급함을 강조한다.
관찰된 HRV 매개변수 변화는 미주신경 자극에 기인할 수 있다. 이는 생리적 상태가 단순히 정서 및 기분과 연관된 것이 아니라 그 근본 구성 요소라는 다중미주신경 이론의 주장을 뒷받침한다. 이 이론적 틀 안에서 자율신경 상태는 환경 자극에 대한 우리의 인식과 평가에 영향을 미치는 매개변수 역할을 한다. 신호를 중립적, 긍정적 또는 위협적으로 반사적으로 평가하는 방식은 개인의 생리적 상태에 따라 달라질 수 있다. 기능적으로 개인의 상태 변화는 다양한 뇌 구조의 접근성 변화를 초래하여 사회적 소통을 촉진하거나 싸움/도피 또는 셧다운과 같은 방어 반응을 유발할 수 있다37. Goldbeck 등은 또한 요가 기반 운동이 HRV 매개변수를 향상시켜 부교감신경 활동을 개선하는 데 중요함을 강조했다38.
본 연구에는 몇 가지 한계점이 존재한다. 표본 크기가 작고, 참가자가 여성으로만 구성되었으며, 장기 추적 관찰이 부족했다. 일반화에는 신중을 기해야 하지만, 연구 결과는 특정 환자 집단 내에서 개입의 잠재적 이점에 대한 폭넓은 이해에 기여한다. 여성 참가자만 포함시킨 결정은 무릎 골관절염이 남성보다 여성에서 더 흔히 관찰된다는 사실에 근거한다. 다중미주신경 운동이 제공하는 혜택의 장기적 지속성과 내구성을 평가한다면 그 효과에 대한 보다 포괄적인 이해를 제공하고 임상적 권고사항을 안내할 수 있을 것이다. 또한 대조군이 없었으며, 맹검 절차가 시행되지 않았다. 본 연구에서 맹검을 시행하지 못한 것은 사용된 중재의 특성 때문으로, 참가자 스스로 수행 중인 특정 운동을 인지해야 했기에 참가자와 연구자가 그룹 배정을 알지 못하도록 하는 것이 실질적으로 어려웠다. 연구는 자기보고식 측정법에 의존했으며 객관적 측정법을 사용하지 않았다. 객관적 평가 없이 자기보고식 측정법에만 전적으로 의존하면 참가자의 주관적 인식과 회상 편향으로 인한 측정 편향 가능성이 발생한다. 생체역학적 평가나 생체표지자 같은 객관적 측정법을 통합하면 중재 효과에 대한 보다 포괄적인 이해를 제공할 수 있을 것이다. 마지막으로, 중도 이탈률이 10%로 최종 표본의 대표성에 영향을 미쳤을 수 있으며 잠재적 편향을 초래했을 수 있다.
결론
본 연구는 2등급 무릎 골관절염 관리에서 강화 운동과 다중미주신경 이론 기반 운동을 결합할 때의 잠재적 이점을 강조한다. 근력 강화 운동은 관절 안정성을 향상시키고 관절에 가해지는 스트레스를 줄일 수 있으며, 다중미주신경 치료 기반 운동은 자율신경 기능을 조절하고 통증 인식을 감소시키며 이완과 정서적 안녕을 촉진하는 데 도움이 될 수 있습니다. 이러한 중재의 결합은 무릎 골관절염 환자에게 우수한 전반적 결과와 삶의 질 개선으로 이어질 수 있습니다. 이러한 결과는 골관절염 관리를 위한 보조적 중재로 다중미주신경 운동을 통합하는 잠재적 효과성을 뒷받침합니다.
Conclusions
The study highlights the potential benefits of combining strengthening exercises with exercises based on polyvagal theory in the management of grade II knee OA. Strengthening exercises can improve joint stability and reduce stress on the joint, while exercises based on polyvagal therapy may help regulate autonomic function, reduce pain perception, and promote relaxation and emotional well-being. The combination of these interventions may lead to superior overall outcomes and improved quality of life for individuals with knee osteoarthritis. These results support the potential effectiveness of incorporating polyvagal exercise as an adjunctive intervention for osteoarthritis management.
Future scope
The study opens up several potential avenues for future research. First, conducting a larger-scale study with a more diverse participant pool, including both genders, would help establish the generalizability of the findings. Long-term follow-up assessments could be incorporated to examine the sustainability and durability of the effects observed. Additionally, incorporating a control group and implementing blinding procedures would enhance the study's internal validity. Objective measures, such as physiological recordings, could be used in conjunction with self-report measures to provide a more comprehensive understanding of the outcomes. Exploring different stimulation parameters and investigating the mechanisms underlying vagal nerve stimulation could further elucidate its therapeutic potential. Overall, future research should build upon these limitations to strengthen the evidentiary base and better inform clinical applications of VNS.
Data availability
All data generated or analyzed during this study are presented in the manuscript. Please contact the corresponding author for access to the data from this study.
References
Grazio, S. & Balen, D. Obesity: Risk factor and predictor of osteoarthritis. Lijec. Vjesn. 131(1–2), 22–26 (2009).
Cui, A., Li, H., Wang, D., Zhong, J., Chen, Y. & Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine. 29 (2020).
Kaur, R., Ghosh, A. & Singh, A. Prevalence of knee osteoarthritis and its determinants in 30–60 years old women of Gurdaspur, Punjab. Int. J. Med. Sci. Public Health 7(10), 825–831 (2018).
Taheri, M., Farzian, S., Esmaeili, A. & Shabani, E. The effect of water therapy and jogging exercises on the health-related factors of physical fitness of elderly women. Int. J. Sport Stud. Health. 3(2) (2020).
Alves, J. C. & Bassitt, D. P. Quality of life and functional capacity of elderly women with knee osteoarthritis. Einstein (Sao Paulo). 11, 209–215 (2013).
Arslan D, ÜNAL ÇEVİK I. Interactions between the painful disorders and the autonomic nervous system. Agri J. Turk. Soc. Algol. 34(3) (2022).
Mora, J. C., Przkora, R., Cruz-Almeida, Y. Knee osteoarthritis: Pathophysiology and current treatment modalities. J. Pain Res. 2189–2196 (2018).
Richebé, P., Capdevila, X. & Rivat, C. Persistent postsurgical pain: Pathophysiology and preventative pharmacologic considerations. Anesthesiology 129(3), 590–607 (2018).
Porges, S. W. & Dana, D. Clinical Applications of the Polyvagal Theory: The Emergence of Polyvagal-Informed Therapies (Norton Series on Interpersonal Neurobiology) (WW Norton & Company, 2018).
Farr, J. N. et al. Progressive resistance training improves overall physical activity levels in patients with early osteoarthritis of the knee: A randomized controlled trial. Phys. Ther. 90(3), 356–366 (2010).
Wang, S.-T. & Ni, G.-X. Depression in osteoarthritis: Current understanding. Neuropsychiatr. Dis. Treat. 18, 375 (2022).
Ruffoli, R. et al. The chemical neuroanatomy of vagus nerve stimulation. J. Chem. Neuroanat. 42(4), 288–296 (2011).
Kumar, H., Pal, C. P., Sharma, Y. K., Kumar, S. & Uppal, A. Epidemiology of knee osteoarthritis using Kellgren and Lawrence scale in Indian population. J. Clin. Orthop. Trauma 11, S125–S129 (2020).
Dunlevy, C., Cooney, M. & Gormely, J. Procedural considerations for photographic-based joint angle measurements. Physiother. Res. Int. 10(4),