30~40대 단백뇨 환자가 폭증하고 있다.
건생병사 4과제와 발효 프로그램으로 쉽게 치료할 수 있는 단백뇨 환자를 방치하면
그 끝은 신장투석이다!!
그 이유가 바로 'CKM cardiovascular kidney metabolic syndrome'이다.
- nature
- scientific reports
- articles
- article
Elevated triglyceride glucose index is associated with advanced cardiovascular kidney metabolic syndrome
- Article
- Open access
- Published: 28 December 2024
Elevated triglyceride glucose index is associated with advanced cardiovascular kidney metabolic syndrome
Scientific Reports volume 14, Article number: 31352 (2024) Cite this article
10k Accesses
12 Citations
1 Altmetric
Abstract
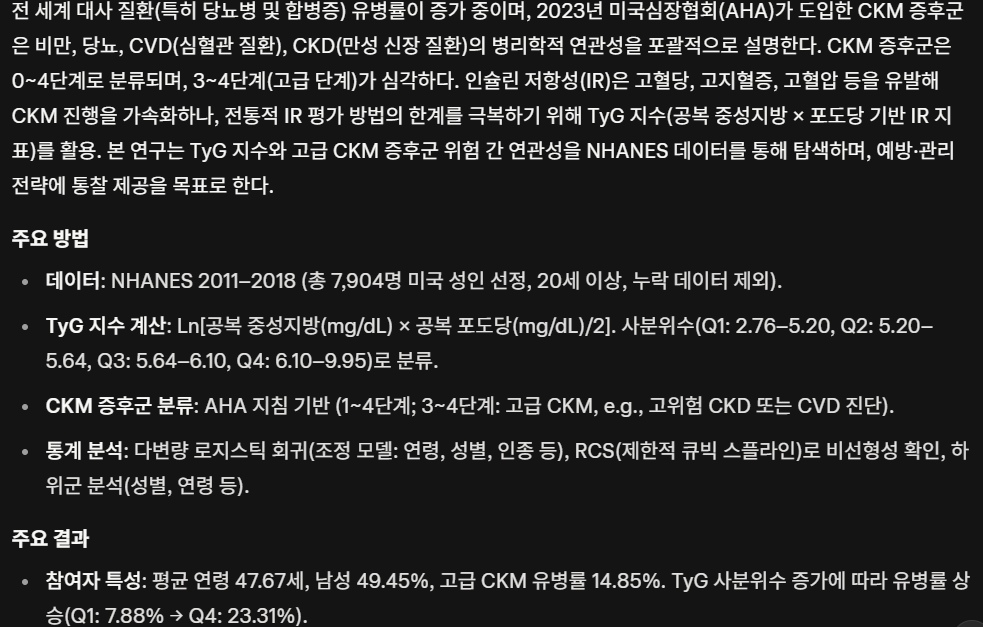
The cardiovascular kidney metabolic (CKM) syndrome is a dynamic geriatric condition that has received limited research attention regarding its potential associations with the triglyceride glucose (TyG) index. This study aims to explore the potential association between the TyG index and advanced CKM syndrome. Data for this cross-sectional study were obtained from the National Health and Nutrition Examination Survey (NHANES) conducted between 2011 and 2018. The association between the TyG index and the risk of advanced CKM syndrome was investigated using multivariable logistic regression models. Additionally, a restricted cubic spline (RCS) analysis was employed to assess the dose-response relationship between the TyG index and the risk of advanced CKM syndrome. A total of 7904 participants were included in this study, with a mean TyG index of 5.04 ± 0.41. The prevalence of advanced CKM syndrome among the participants was 14.85%. Our findings indicated that as the TyG index quartiles increased, the risk of advanced CKM syndrome also increased. The results from the three regression analysis models indicated a positive association between the continuous TyG index and advanced CKM syndrome. Furthermore, the quartiles of the TyG index were significantly associated with an increased prevalence of advanced CKM syndrome in the fully adjusted models (TyG index Q4 vs. Q1, OR = 1.94, 95% CI 1.37–2.75, P < 0.001). The results of the RCS analysis indicated a linear and positive association between the TyG index and advanced CKM syndrome. The results indicated that elevated TyG index is associated with an increased prevalence of advanced CKM syndrome. This suggests that the TyG index may be a useful tool for assessing the risk of advanced CKM syndrome.
초록
심혈관 신장 대사(CKM) 증후군은 동적 노인성 질환 dynamic geriatric condition 으로,
트리글리세라이드-포도당(TyG) 지수와의 잠재적 연관성에 대한 연구는
제한적으로 이루어져 왔다.
본 연구는
TyG 지수와 진행성 CKM 증후군 간의 잠재적 연관성을 탐구하는 것을 목표로 한다.
이 횡단면 연구의 데이터는
2011년부터 2018년 사이에 수행된 국민건강영양조사(NHANES)에서 얻었다.
TyG 지수와 진행성 CKM 증후군 위험 간의 연관성은
다변량 로지스틱 회귀 모델을 사용하여 조사하였다.
또한 제한적 큐빅 스플라인(RCS) 모델을 사용하여 Ty (NHANES)에서 수집되었다.
TyG 지수와 진행성 CKM 증후군 위험 간의 연관성은 다변량 로지스틱 회귀 모델을 사용하여 분석하였다. 또한 제한적 큐빅 스플라인(RCS) 분석을 통해 TyG 지수와 진행성 CKM 증후군 위험 간의 용량-반응 관계를 평가하였다.
총 7904명의 참가자가 본 연구에 포함되었으며,
평균 TyG 지수는 5.04±0.41이었다.
참가자 중 진행성 CKM 증후군 유병률은
14.85%였다.
연구 결과 TyG 지수 사분위수가 증가함에 따라
진행성 CKM 증후군 위험도 증가하는 것으로 나타났다.
세 가지 회귀 분석 모델 결과는 연속형 TyG 지수와 진행성 CKM 증후군 간 양의 상관관계를 나타냈다. 또한 완전 조정 모델에서 TyG 지수 사분위수는 진행성 CKM 증후군 유병률 증가와 유의미한 연관성을 보였다(TyG 지수 Q4 대 Q1, 오즈비(OR) = 1.94, 95% 신뢰구간(CI) 1.37–2.75, P < 0.001).
RCS 분석 결과는
TyG 지수와 진행성 CKM 증후군 사이에
선형적이고 양의 상관관계가 있음을 나타냈다.
결과는 TyG 지수 상승이
진행성 CKM 증후군 유병률 증가와 연관되어 있음을 시사한다.
이는 TyG 지수가
진행성 CKM 증후군 위험 평가에 유용한 도구가 될 수 있음을 시사한다.
Similar content being viewed by others
Article Open access16 May 2025
Article Open access05 August 2025
Article Open access04 September 2024
Introduction
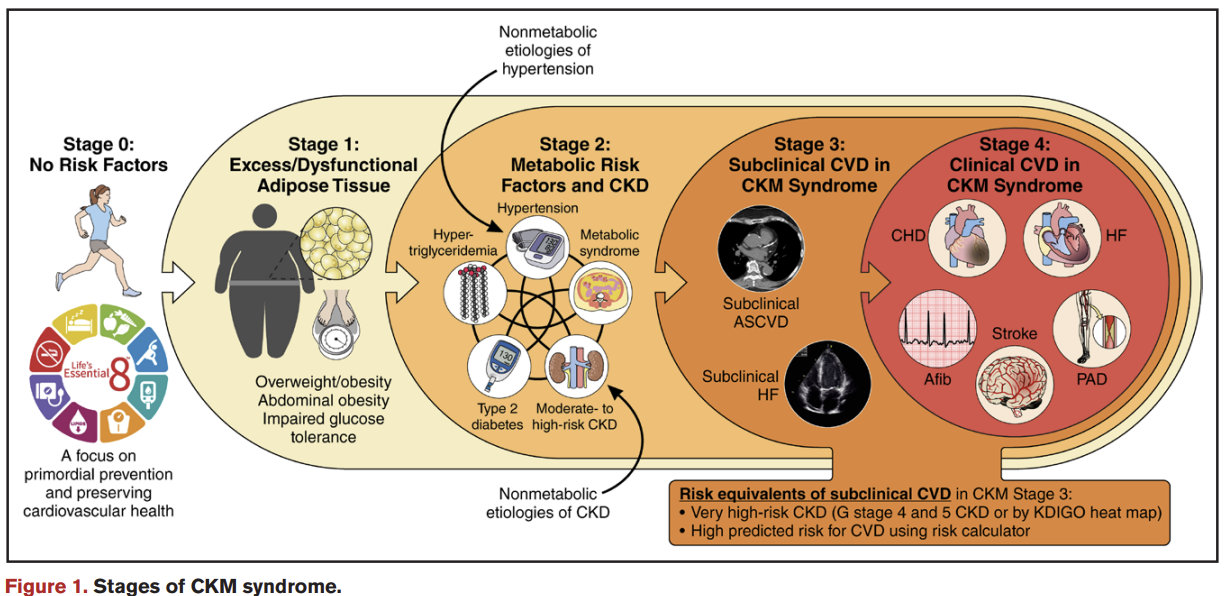
The prevalence of metabolic diseases, particularly diabetes and its associated complications, is increasing globally. According to the 10th edition of the Diabetes Atlas in 2021, approximately 537 million people worldwide have diabetes, with about one-third of them suffering from cardio-renal disease1. In 2023, the American Heart Association introduced the concept of Cardiovascular-Kidney-Metabolic (CKM) syndrome to comprehensively reveal the pathological links between metabolic risk factors such as obesity, diabetes mellitus (DM), cardiovascular disease (CVD), chronic kidney disease (CKD), and other metabolic conditions2. The stages of CKM syndrome and its pathological features have been classified from stage 0 (no risk factors present) to stage 4 (CVD diagnosed) to fully illustrate the dynamic progression of the syndrome, with stages 3 and 4 being labeled as advanced CKM syndrome3. Stage 3 CKM syndrome is marked by significant metabolic dysfunction, including dyslipidemia, hyperglycemia, and hypertension, coupled with declining kidney function and an increased cardiovascular burden. In Stage 4, cardiovascular disease becomes established, signaling further progression and representing the most severe stage of CKM syndrome. Aggarwal et al. found that nearly 90% of U.S. adults suffer from CKM syndrome (stage 1 or higher), with 15% of them in advanced stages3.
서론
대사성 질환,
특히 당뇨병 및 관련 합병증의 유병률은 전 세계적으로 증가하고 있습니다.
2021년 당뇨병 아틀라스 제10판에 따르면,
전 세계적으로 약 5억 3,700만 명이 당뇨병을 앓고 있으며,
이 중 약 1/3이 심장-신장 질환을 앓고 있습니다1.
2023년 미국심장협회(AHA)는
비만, 당뇨병(DM), 심혈관질환(CVD), 만성신장질환(CKD) 및 기타 대사성 질환과 같은
대사 위험 요인 간의 병리학적 연관성을 포괄적으로 규명하기 위해
심혈관-신장-대사(CKM) 증후군 개념을 도입하였다2.
CKM 증후군의 단계와 병리학적 특징은
0단계(위험 인자 없음)부터 4단계(CVD 진단)까지 분류되어
증후군의 역동적 진행을 완전히 설명하며,
3단계와 4단계는 진행성 CKM 증후군으로 분류됩니다3.
3단계 CKM 증후군은
이상지질혈증, 고혈당증, 고혈압을 포함한 중대한 대사 기능 장애와 함께
신기능 저하 및 심혈관 부담 증가가 동반됩니다.
4단계에서는
심혈관 질환이 확립되어 추가 진행을 알리며
CKM 증후군의 가장 심각한 단계를 나타낸다.
Aggarwal 등은 미국 성인의 약 90%가
CKM 증후군(1단계 이상)을 앓고 있으며,
그중 15%가 진행된 단계에 있다고 보고했다3.
In terms of disease mechanisms, Kadowaki et al. concluded that diabetes mellitus impairs the cardio-renal system through a series of complex mechanisms4, including hyperglycemia, the formation of advanced glycation end products, insulin resistance, aberrant activation of the renin-angiotensin-aldosterone system, lipotoxicity, oxidative stress, and chronic inflammatory response. These pathophysiological changes are also observed in the context of CVD and CKD, which accelerate the progression of type 2 diabetes mellitus (T2DM), creating a vicious cycle. The importance of insulin resistance (IR) in various chronic diseases has been increasingly recognized through more in-depth research. IR not only leads to a significant reduction in insulin sensitivity but also induces a series of metabolic abnormalities, including hyperglycemia, hyperlipidemia, and hypertension. These metabolic abnormalities may exacerbate pathological changes such as endothelial cell dysfunction, vascular inflammation, and atherosclerosis, further contributing to the onset and progression of CKM syndrome.
However, traditional methods of assessing IR, such as the euglycemic-hyperinsulinemic clamp, intravenous glucose tolerance testing, and HOMA-IR, have limitations in practical application due to their invasive nature, high cost, and inapplicability to patients receiving insulin therapy or suffering from β-cell insufficiency5,6. Guerrero et al.7 proposed a novel assessment method, the TyG index, designed to be used as a potential index for assessing IR. While both fasting glucose and triglyceride levels require blood sampling, the TyG index has been validated in multiple studies as a cost-effective and accessible metric, offering comparable predictive accuracy for insulin resistance with excellent sensitivity and specificity8,9,10.
Given the significant efficacy of the TyG index in assessing IR and its potential value in predicting cardio-metabolic diseases, it was initially hypothesized that there might be an association between the TyG index and the risk of CKM syndrome at different stages of the disease. Therefore, the present study was designed to explore in depth the potential association between the TyG index and the risk of advanced CKM syndrome in the general population, aiming to provide new insights and inform future research on the prevention, diagnosis, and management of CKM syndrome.
질병 메커니즘 측면에서, Kadowaki 등은
당뇨병이 고혈당, 고급 당화 최종 생성물 형성, 인슐린 저항성,
레닌-안지오텐신-알도스테론 시스템의 비정상적 활성화,
지질 독성, 산화 스트레스 및 만성 염증 반응을 포함한
일련의 복잡한 메커니즘4을 통해 심장-신장 시스템을 손상시킨다고 결론지었습니다.
이러한 병리생리학적 변화는
심혈관 질환(CVD) 및 만성 신장 질환(CKD)에서도 관찰되며,
이는 제2형 당뇨병(T2DM)의 진행을 가속화하여 악순환을 초래합니다.
다양한 만성 질환에서 인슐린 저항성(IR)의 중요성은
심층 연구를 통해 점차 인식되고 있다.
IR은
인슐린 감수성의 현저한 감소를 초래할 뿐만 아니라
고혈당, 고지혈증, 고혈압을 포함한 일련의 대사 이상을 유발한다.
이러한 대사 이상은
내피세포 기능 장애, 혈관 염증, 동맥경화증과 같은 병리학적 변화를 악화시켜
CKM 증후군의 발병 및 진행에 더욱 기여할 수 있다.
그러나
정상혈당-고인슐린 클램프법, 정맥 내 포도당 내성 검사, HOMA-IR과 같은
전통적인 IR 평가 방법은
침습적 성격, 높은 비용,
인슐린 치료를 받는 환자나 β-세포 기능 부전 환자5,6에게 적용 불가능하다는 한계로 인해
실제 적용에 제약이 있다.
Guerrero 등7은
IR 평가를 위한 잠재적 지표로 활용될 수 있도록 고안된
새로운 평가 방법인 TyG 지수를 제안했다.
공복 혈당과 중성지방 수치 모두 혈액 채취가 필요하지만,
TyG 지수는 여러 연구에서 비용 효율적이고 접근성이 뛰어난 지표로 검증되었으며,
우수한 민감도와 특이도를 바탕으로 인슐린 저항성에 대해 비교 가능한 예측 정확도를 제공합니다8,9,10.
TyG 지수가 인슐린 저항성 평가에 있어 상당한 효능을 보이며
심혈관 대사 질환 예측에 잠재적 가치를 지닌다는 점을 고려하여,
본 연구에서는 TyG 지수와 CKM 증후군의 다양한 단계별 위험 간 연관성이 존재할 수 있다는 가설을 세웠다.
따라서 본 연구는
일반 인구 집단에서 TyG 지수와 진행성 CKM 증후군 위험 간의 잠재적 연관성을 심층적으로 탐구하여
CKM 증후군의 예방, 진단 및 관리에 관한 향후 연구에
새로운 통찰력을 제공하고 정보를 제공하기 위해 설계되었습니다.
Methods
Study design and participants
The data for this study were obtained from the NHANES, a nationally representative survey conducted by the Centers for Disease Control and Prevention in the United States. NHANES assesses nutrition and health conditions in the country and provides reliable, authoritative, and precise health statistics. Written informed consent was obtained from all participants involved in NHANES, and the survey received approval from the Ethics Review Board of the National Center for Health Statistics. The NHANES data are publicly accessible and available online at (https://www.cdc.gov/nchs/nhanes/index.htm).
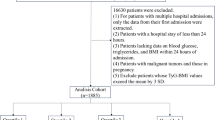
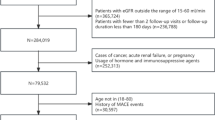
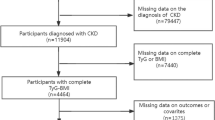
In this study, data were selected from four NHANES survey cycles spanning from 2011 to 2018. The data collection methods included questionnaires, interview transcripts, physical examinations, and laboratory tests. Initially, the study included a total of 39,156 participants from the continuous NHANES dataset. After a rigorous screening process, participants under the age of 20 years and individuals with missing sample weights (WTSAF2YR) and survival status were excluded. Additionally, participants lacking data related to CKM syndrome and TyG index, as well as covariates, were excluded, ultimately identifying 7904 eligible participants. Figure S1 presents a flowchart that illustrates the participant selection process.
방법
연구 설계 및 참가자
본 연구 데이터는 미국 질병통제예방센터(CDC)에서 실시한 전국 대표 조사인 NHANES(National Health and Nutrition Examination Survey)에서 획득하였습니다. NHANES는 국가의 영양 및 건강 상태를 평가하며 신뢰할 수 있고 권위적이며 정확한 건강 통계를 제공한다. NHANES에 참여한 모든 참가자로부터 서면 동의서를 받았으며, 이 조사는 국립보건통계센터(National Center for Health Statistics)의 윤리 심사 위원회(Ethics Review Board)의 승인을 받았다. NHANES 데이터는 공개적으로 접근 가능하며 온라인(https://www.cdc.gov/nchs/nhanes/index.htm)에서 이용할 수 있다.
본 연구에서는 2011년부터 2018년까지의 네 차례 NHANES 조사 주기에서 데이터를 선별하였다. 데이터 수집 방법에는 설문지, 인터뷰 기록, 신체 검사 및 실험실 검사가 포함되었다. 초기 연구에는 연속 NHANES 데이터셋에서 총 39,156명의 참가자가 포함되었다. 엄격한 선별 과정을 거쳐 20세 미만 참가자와 표본 가중치(WTSAF2YR) 및 생존 상태 정보가 누락된 개인을 제외했습니다. 또한 CKM 증후군 및 TyG 지수와 관련된 데이터, 그리고 공변량이 부족한 참가자들도 제외하여 최종적으로 7904명의 적격 참가자를 선정했습니다. 그림 S1은 참가자 선정 과정을 보여주는 흐름도입니다.
Ascertainment of TyG index
The TyG index was calculated using the formula: TyG index = Ln [fasting TG (mg/dL) × fasting glucose (mg/dL)/2]. The measurement of triglycerides and fasting glucose was conducted through enzymatic assays using the Roche Modular P and Roche Cobas 6000 chemistry analyzers, respectively. The hexokinase-mediated reaction was used to assess fasting glucose on the Roche/Hitachi Cobas C 501 chemistry analyzer 11. Participants were categorized into four groups based on the quartiles of the TyG index, with Q1 serving as the reference group for comparative analysis. The quartile cut points were as follows: Q1 (2.76–5.20], Q2 (5.20–5.64], Q3 (5.64–6.10], and Q4 (6.10–9.95].
TyG 지수 확인
TyG 지수는 다음 공식으로 계산되었습니다:
TyG 지수 = Ln [공복 중성지방(mg/dL) × 공복 혈당(mg/dL)/2].
중성지방과 공복 혈당 측정은 각각 Roche Modular P 및 Roche Cobas 6000 화학 분석기를 이용한 효소 분석법으로 수행되었습니다. 공복 혈당 측정은 Roche/Hitachi Cobas C 501 화학 분석기에서 헥소키나제 매개 반응을 활용하여 평가했습니다 11. 참가자들은 TyG 지수의 사분위수를 기준으로 4개 그룹으로 분류되었으며, Q1 그룹이 비교 분석을 위한 기준 그룹으로 설정되었습니다. 사분위수 구분점은 다음과 같습니다: Q1 (2.76–5.20], Q2 (5.20–5.64], Q3 (5.64–6.10], Q4 (6.10–9.95].
Ascertainment of CKM syndrome stages
CKM syndrome stages were classified as follows: CKM Stage 1 was characterized by elevated BMI (≥ 23 kg/m² for Asians, > 25 kg/m2 for other populations), increased waist circumference (≥ 80 cm for women and ≥ 90 cm for men in Asians; ≥88 cm for women and ≥ 102 cm for other populations), or prediabetes (HbA1c 5.7-6.4%, fasting glucose 100–125 mg/dL). CKM Stage 2 was categorized by the presence of multiple metabolic risk factors, such as elevated triglycerides, hypertension, diabetes, or metabolic syndrome, or moderate-to-high-risk CKD according to KDIGO guidelines. Stages 3 and 4 were collectively classified as Advanced CKM Syndrome, encompassing individuals diagnosed with or at high risk of developing cardiovascular disease 3. CKM Stage 3 included participants with very-high-risk CKD based on KDIGO criteria or those with a predicted 10-year CVD risk of 20% or greater using AHA PREVENT equations12. CKM Stage 4 comprised participants with self-reported cardiovascular diseases, such as coronary heart disease, angina, myocardial infarction, heart failure, and cerebrovascular accidents. Detailed descriptions of stage definitions are shown in the Supplemental Methods.
CKM 증후군 단계 확인
CKM 증후군 단계는 다음과 같이 분류되었습니다:
CKM 1단계는
BMI 상승(아시아인 기준 ≥23 kg/m², 기타 인종 기준 >25 kg/m²),
증가된 허리둘레 (아시아인 여성 ≥80 cm, 남성 ≥90 cm;
기타 인종 여성 ≥88 cm, 남성 ≥102 cm) 또는 당뇨병 전단계(HbA1c 5.7-6.4%, 공복 혈당 100–125 mg/dL)를 나타냈다.
CKM 2단계는
고중성지방혈증, 고혈압, 당뇨병 또는 대사증후군과 같은 다중 대사 위험 인자의 존재,
또는 KDIGO 지침에 따른 중등도-고위험 CKD로 분류되었습니다.
3단계와 4단계는
심혈관 질환 진단 또는 고위험군으로 분류된 개인을 포괄하는
진행성 CKM 증후군으로 통합 분류되었습니다 3.
CKM 3단계는
KDIGO 기준에 따른 초고위험 CKD 환자 또는
AHA PREVENT 방정식12을 사용해 예측된 10년 CVD 위험이 20% 이상인 참가자를 포함했다.
CKM 4단계는
관상동맥질환, 협심증, 심근경색, 심부전, 뇌혈관사고 등
자가보고된 심혈관질환이 있는 참가자로 구성되었다.
단계 정의에 대한 상세한 설명은 보충 방법론에 제시되어 있다.
Ascertainment of covariates
Demographic information on participants was collected from the NHANES database, including gender, age, race and ethnicity (Asian, Black, Hispanic, White, Other), educational level (less than high school, high school or equivalent, or college or above), and marital status (Married, Single/Separated). Further information on lifestyle habits and comorbidities was also collected, such as smoking status categorized as never smoked, ever smoked, and current smoker, and intensity of physical activity (vigorous/moderate exercise, mild exercise) with reference to the World Health Organization guidelines on physical activity status13,14. Self-reported general health condition was classified into three groups: very good to excellent, good, and poor to fair. Physical and laboratory tests such as body mass index (BMI), systolic and diastolic blood pressure measurements, serum creatinine and uric acid levels, total cholesterol, glycohemoglobin, and albumin/creatinine ratio (ACR) were selected as potential confounders. The details of relevant definitions were shown in the Supplementary Method. Additionally, mortality status was ascertained by probabilistic matching to the National Death Index through December 31, 2019. The primary outcome of this study was mortality from all causes.
공변량 확인
참가자의 인구통계학적 정보는 NHANES 데이터베이스에서 수집되었으며, 여기에는 성별, 연령, 인종 및 민족(아시아인, 흑인, 히스패닉, 백인, 기타), 교육 수준(고등학교 미만, 고등학교 또는 동등, 대학 이상), 혼인 상태(기혼, 미혼/별거)가 포함되었습니다. 생활습관 및 동반질환에 대한 추가 정보도 수집되었으며, 흡연 상태는 ‘비흡연자’, ‘과거 흡연자’, ‘현재 흡연자'로 분류되었고, 신체 활동 강도는 세계보건기구(WHO) 신체 활동 지침13,14에 따라 '고강도/중등도 운동’, ‘경도 운동'으로 구분되었습니다. 자가보고 일반 건강 상태는 '매우 좋음~우수’, ‘좋음’, '나쁨~보통'의 세 그룹으로 분류되었습니다. 신체 및 실험실 검사 항목으로는 체질량지수(BMI), 수축기 및 이완기 혈압 측정, 혈청 크레아티닌 및 요산 수치, 총 콜레스테롤, 당화혈색소, 알부민/크레아티닌 비율 (ACR) 등이 잠재적 혼란 요인으로 선정되었다. 관련 정의의 세부 사항은 보충 방법론에 제시되었다. 또한 사망 여부는 2019년 12월 31일까지 국가 사망자 정보 시스템(National Death Index)과의 확률적 매칭을 통해 확인하였다. 본 연구의 주요 결과는 모든 원인에 의한 사망률이었다.
Statistical analysis
The statistical analysis was conducted using R 4.2.1 and the Free Statistics software (version 1.9). Complex survey design factors, including sample weights, clustering, and stratification, were considered for all analyses with instructions for using NHANES data. Baseline characteristics were compared by CKM syndrome stages in the two intervals using the Rao-Scott chi-square test for categorical variables and ANOVA and the Kruskal-Wallis test adjusted for sampling weights for continuous variables. Continuous variables were reported as means accompanied by standard errors, while categorical variables were presented as percentages, based on quartiles (Q1–Q4) of the TyG index and CKM syndrome stages. Descriptive analyses were performed using weighted one-way ANOVA for continuous variables and weighted chi-square tests for categorical variables. To explore the association between the TyG index and advanced CKM syndrome, multivariate logistic regression analyses were conducted, and three different statistical inference models were constructed. Crude model was unadjusted, model 1 was adjusted for age, sex, and ethnicity, and model 2 was further adjusted for education level, marital status, BMI, serum creatinine, serum uric acid, total cholesterol, HDL-C, glycohemoglobin, ACR, systolic blood pressure, diastolic blood pressure, smoking status, general health condition, and physical activity based on model 1. RCS analysis was performed to explore the possible relationship between the TyG index and the likelihood of advanced CKM syndrome. P value of less than 0.05 was considered statistically significant in this study.
통계 분석
통계 분석은 R 4.2.1 및 Free Statistics 소프트웨어(버전 1.9)를 사용하여 수행되었습니다. 모든 분석에는 표본 가중치, 군집화, 계층화를 포함한 복잡한 조사 설계 요소가 고려되었으며, NHANES 데이터 사용 지침이 적용되었습니다. 기초 특성은 두 기간 동안 CKM 증후군 단계별로 비교되었으며, 범주형 변수는 Rao-Scott 카이제곱 검정을, 연속형 변수는 표본 가중치를 조정된 ANOVA 및 크루스칼-월리스 검정을 사용했다. 연속형 변수는 평균과 표준 오차를 동반하여 보고되었으며, 범주형 변수는 TyG 지수 및 CKM 증후군 단계의 사분위수(Q1–Q4)를 기준으로 백분율로 제시되었다. 기술적 분석은 연속형 변수에 대해 가중치 일원 분산분석(ANOVA), 범주형 변수에 대해 가중치 카이제곱 검정을 사용하여 수행하였다. TyG 지수와 진행성 CKM 증후군 간의 연관성을 탐색하기 위해 다변량 로지스틱 회귀 분석을 수행하고 세 가지 다른 통계적 추론 모델을 구축하였다. 원시 모델은 미조정 모델이었으며, 모델 1은 연령, 성별, 인종에 대해 조정되었고, 모델 2는 모델 1을 기반으로 교육 수준, 결혼 상태, 체질량지수(BMI), 혈청 크레아티닌, 혈청 요산, 총 콜레스테롤, HDL-C, 당화혈색소, ACR, 수축기 혈압, 이완기 혈압, 흡연 상태, 일반 건강 상태, 신체 활동에 대해 추가로 조정되었다. TyG 지수와 진행성 CKM 증후군 발생 가능성 간의 잠재적 연관성을 탐색하기 위해 RCS 분석을 수행하였다. 본 연구에서 P값이 0.05 미만인 경우 통계적으로 유의한 것으로 간주하였다.
Results
Baseline characteristics of study participantsBaseline characteristics of study participants stratified by TyG index quartiles
Table 1 showed the baseline characteristics of the participants stratified by quartiles of the TyG index. The study enrolled a total of 7904 participants with a mean age of 47.67 ± 16.94 years, and 49.45% of them were male. The mean prevalence of advanced CKM syndrome was found to be 14.85%. Notably, the prevalence of advanced CKM syndrome was higher in participants with higher quartiles of the TyG index (Q1: 7.88%; Q2: 12.91%; Q3: 15.94%; Q4: 23.31%). Additionally, there was a higher mortality rate among participants in the highest quartile compared to the lowest quartile. Participants with higher TyG index were more likely to be older, male, of Hispanics or white ethnicity, less educated, former smokers or current smokers, and mildly physically active compared to participants in the lowest TyG index quartile. In terms of biochemical parameters, the highest TyG index group showed a statistically significant increase in several parameters, including serum creatinine, uric acid, total cholesterol, glycohemoglobin, and ACR, along with a significantly lower HDL-C level. Furthermore, physiological parameters such as systolic blood pressure (SBP), diastolic blood pressure (DBP), and BMI tended to increase in the highest TyG index group. Analyses revealed that the prevalence of chronic diseases, such as hypertension, diabetes mellitus, cardiovascular diseases, and renal failure, was significantly higher in the highest TyG index group compared to the lowest group.
결과
연구 참여자의 기저 특성TyG 지수 사분위별로 분류된 연구 참여자의 기저 특성
표 1은 TyG 지수 사분위별로 분류된 참여자의 기저 특성을 보여줍니다. 연구에는 총 7904명의 참여자가 등록되었으며, 평균 연령은 47.67±16.94세였고, 49.45%가 남성이었습니다. 진행성 CKM 증후군의 평균 유병률은 14.85%로 나타났다. 특히 TyG 지수가 높은 사분위군일수록 진행성 CKM 증후군 유병률이 높았다(Q1: 7.88%; Q2: 12.91%; Q3: 15.94%; Q4: 23.31%). 또한 최고 사분위군 참가자의 사망률이 최저 사분위군에 비해 높았다. TyG 지수가 높은 참가자는 최저 사분위군 참가자에 비해 고령, 남성, 히스패닉 또는 백인 인종, 낮은 교육 수준, 과거 흡연자 또는 현재 흡연자, 신체 활동이 낮은 경향이 더 컸다. 생화학적 지표 측면에서 최고 TyG 지수 그룹은 혈청 크레아티닌, 요산, 총 콜레스테롤, 당화혈색소, ACR 등 여러 지표에서 통계적으로 유의미한 증가를 보였으며, HDL-C 수치는 유의하게 낮았다. 또한 최고 TyG 지수 그룹에서는 수축기 혈압(SBP), 이완기 혈압(DBP), 체질량지수(BMI)와 같은 생리학적 지표가 증가하는 경향을 보였다. 분석 결과, 최고 TyG 지수 그룹은 최저 그룹에 비해 고혈압, 당뇨병, 심혈관 질환, 신부전과 같은 만성 질환의 유병률이 유의하게 높았다.
Table 1 Baseline characteristics according to the TyG index quartiles.
Baseline characteristics of study participants stratified by CKM syndrome stages
Table 2 showed the baseline characteristics of the participants stratified by stages of CKM syndrome. The mean TyG index observed in the study was 5.04 ± 0.41. Compared to participants in the low CKM stage, those in the late CKM syndrome stage tended to exhibit certain distinguishing characteristics. These characteristics included being older, male, having relatively lower education, and engaging in milder intensity of physical activity. Furthermore, participants in the late CKM syndrome stage showed significant changes in physiological parameters. Specifically, they had higher levels of serum creatinine, uric acid, glycohemoglobin, and ACR. They also tended to have higher levels of SBP and BMI, as well as higher values of TyG index and increased mortality rates (Fig. 1).
Fig. 1
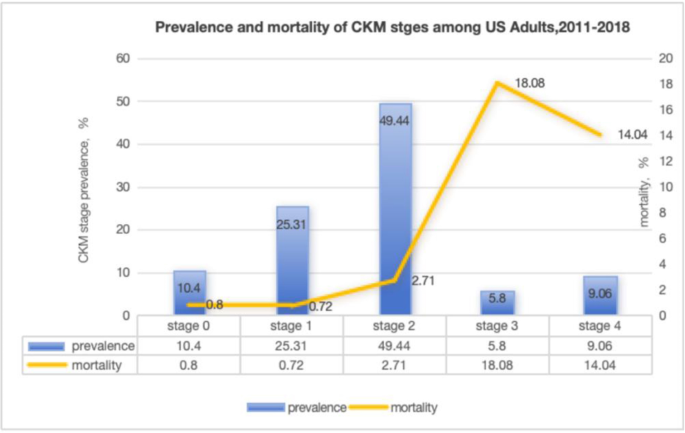
Prevalence and mortality of CKM syndrome stages among U.S. adults (2011–2018) .
Table 2 Baseline characteristics according to the cardiovascular-kidney-metabolic (CKM) syndrome stages.
Association of TyG index with advanced CKM syndrome risk
In our study, a potential association between the TyG index and the likelihood of advanced CKM syndrome was observed (Table 3). In the fully adjusted model (model 2), this positive association remained stable, with an odds ratio (OR) of 1.53 and a 95% confidence interval (CI) of 1.21–1.94 (p < 0.001). To verify the sensitivity of this result, we analyzed the TyG index by converting it from a continuous variable to a categorical variable. The multivariate-adjusted ORs and 95% CIs for the quartiles, from the lowest to the highest TyG index, were 1.00 (reference value), 1.25 (0.95, 1.63), 1.42 (1.06, 1.90), and 1.94 (1.37, 2.75), respectively. Furthermore, our study provided insight into the potential linear relationship between the TyG index and the risk of advanced CKM syndrome using RCS curves (Fig. 2). The results significantly revealed the existence of a linear association (P nonlinear = 0.476) in model 2.
Fig. 2
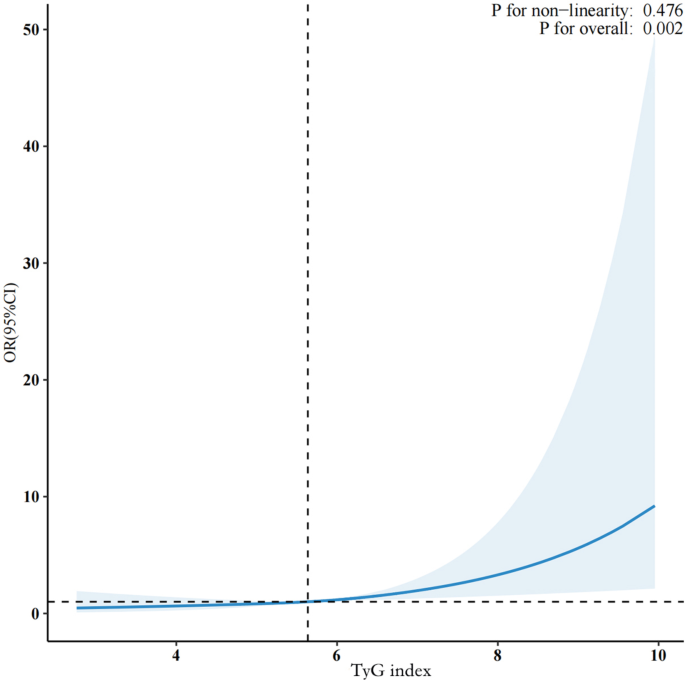
Restricted cubic spline analysis of the association between the TyG index and the risk of advanced CKM syndrome.
Table 3 Multivariate regression analysis of TyG index with advanced CKM syndrome.
Subgroup analysis
Subgroup analyses and interaction tests were performed to evaluate the robustness of the association between the TyG index and the risk of advanced CKM syndrome across various population subgroups (Figure S2). Results showed a positive association between the TyG index and advanced CKM syndrome in both men and women. Notably, the association was stronger in females (OR = 1.72, 95% CI 1.23–2.41, p = 0.002) than in males (OR = 1.37, 95% CI 1.01–1.87, p = 0.05). Additionally, participants aged ≥ 60 exhibited a more pronounced association (OR = 1.72, 95% CI 1.31–2.26, p < 0.001) compared to those under 60 (OR = 1.29, 95% CI 0.91–1.82, p = 0.15). Interaction analysis identified a significant interaction between sex and age (p for interaction < 0.005), while no significant interactions were found in other subgroups, suggesting that these factors may not substantially modify the association between the TyG index and advanced CKM syndrome.
Interactive protective role of HDL-C against TyG index in advanced CKM syndrome
The analysis demonstrated that HDL-C is significantly and independently associated with a lower likelihood of advanced CKM syndrome (coefficient = 0.0084, p < 0.001), with higher HDL-C levels being strongly associated with reduced risk. Additionally, there was a significant negative interaction between HDL-C and the TyG index (interaction coefficient = −0.001658, p < 0.001). Low HDL-C levels intensified the positive association between the TyG index and CKM risk, whereas high HDL-C levels corresponded with a weaker relationship, nearly reaching a plateau in risk reduction. Stratified analysis further confirmed that elevated HDL-C levels effectively buffer the adverse impact of an increased TyG index (Figure S3, Figure S4).
Discussion
Based on data from a cross-sectional study involving 7,904 adults, our research has uncovered an association between the progression stages of CKM syndrome and the TyG index. Specifically, we observed that as the stage of CKM syndrome advanced, both the TyG index exhibited corresponding upward trends. Further analysis revealed a significant and independent association between a higher TyG index and the likelihood of advanced CKM syndrome, with this association demonstrating notable linear characteristics. Additionally, subgroup analyses consistently showed associations between the TyG index and the probability of advanced CKM syndrome onset across various subgroups, including those categorized by hypertension status, diabetes status, smoking habits, and exercise status. Concurrently, we noted that differences in gender, age groups, and BMI influenced this association.
Current research has found that abnormal accumulation and dysfunction of adipose tissue, particularly visceral adipose tissue, serve as key drivers of excessive secretion of pro-inflammatory factors15. Additionally, insulin resistance and abnormal glucose tolerance in peripheral tissues induced by metabolism-related inflammation significantly exacerbate the damage caused by pro-inflammatory factors and oxidative stress products to the cardiovascular system and kidneys16. This inflammatory and oxidative stress response triggered by IR may provide a fundamental basis for explaining the potential association between the TyG index and CKM syndrome. During the pathological process of IR, it is observed that the inhibition of the insulin signaling pathway leads to a significant increase in the synthesis of monocyte chemoattractant protein-1 (MCP-1), which further promotes inflammatory responses in adipose tissue. When adipose tissue is stimulated by inflammation, macrophages are activated and produce key pro-inflammatory cytokines: tumor necrosis factor (TNF)-a and interleukin-6 (IL-6)17,18. Among them, TNF-a significantly promotes the production of MCP-119, thereby initiating a positive feedback loop that intensifies the inflammatory response. Furthermore, IL-6 stimulates the release of free fatty acids (FFA)20, and the accumulation of FFA, in turn, exacerbates the vicious cycle of IR and inflammation by activating signaling pathways such as NF-κB and JNK21. These intricate interactions underscore the complexity of the pathological processes underlying IR and highlight the need for targeted therapeutic interventions.Furthermore, the hyperglycemic state induced by insulin resistance impairs endothelial function, thereby increasing the risk of atherosclerosis and heart failure22,23. Endothelial dysfunction, a key factor in promoting lipid accumulation, also contributes to increased platelet aggregation and inflammatory responses, thereby accelerating the development of cardiovascular diseases24. Cardiovascular diseases often occur concomitantly with kidney diseases and metabolic disorders, including obesity and T2DM. The presence of T2DM or CKD also leads to worse cardiovascular outcomes for patients25,26. The exact mechanisms behind this relationship require further research.
In the field of assessing IR, although the hyperinsulinemic-normoglycemic clamp technique is recognized as the gold standard, researchers have been dedicated to finding simpler and more cost-effective surrogate markers due to its complex, time-consuming, and expensive nature. Multiple studies have confirmed the role of IR in the pathogenesis of T2DM, dyslipidemia, and obesity in the general population, as well as its close association with the development of cardiovascular diseases. As IR intensifies, the risk of clustering metabolic risk factors also gradually increases27,28, The TyG index, based on fasting triglyceride and glucose levels, is a surrogate marker of IR and is closely related to various metabolic diseases. Notably, TyG levels are strongly associated not only with IR but also with adverse lipid profiles and disrupted lipid metabolism29, further enhancing its relevance in metabolic health assessments. A meta-analysis of 15 cohort studies found a significant positive association between the TyG index and the risk of T2DM30. Wang et al. discovered that the TyG index is a valuable predictive indicator for assessing the severity of coronary heart disease, particularly in prediabetic patients31. In non-diabetic populations, participants with higher TyG index values exhibit an increased likelihood of impaired cardiovascular health32. Furthermore, the TyG index has been positively associated with the risk of cardiovascular diseases in several studies, including those focused on metabolic syndrome, hypertension, arterial stiffness, carotid atherosclerosis, coronary artery disease, and coronary artery calcification33,34,35,36,37,38,39. The TyG index is an effective predictor of metabolic syndrome components, such as obesity and hypertension, and its strong association with adverse lipid profiles makes it a valuable tool for assessing broader metabolic risks across diverse clinical settings40. Evidence from a meta-analysis involving 49,325 participants from 13 observational studies indicates that the pooled sensitivity and specificity of the TyG index for MetS screening are both above 80%41. Furthermore, a large-scale longitudinal study has demonstrated that the TyG index also possesses high predictive value in determining the risk of death from MetS in the US population 42. Research has also confirmed the value of the TyG index in the study of CKD. In a cross-sectional survey involving 18,078 American adults, the prevalence of CKD and proteinuria was significantly positively correlated with TyG index levels43,44. A Japanese cohort study found a link between higher TyG index levels and increased prevalence of CKD45, Similarly, an Austrian study reported a positive association between the TyG index and end-stage kidney disease (ESKD)46. Patients with CKM syndrome exhibit a complex metabolic profile that includes conditions such as obesity and diabetes. These comorbidities significantly elevate insulin resistance, which in turn increases the TyG index. This vicious cycle exacerbates the progression of CKM syndrome. Our study has identified a significant positive association between the risk of the TyG index and advanced CKM syndrome. This finding offers a novel perspective for disease management, highlighting the importance of managing TyG index levels as part of strategies aiming at reducing the likelihood of advanced CKM syndrome. In the early stages of CKM syndrome, an elevated TyG index can serve as an indicator of underlying metabolic abnormalities and increased insulin resistance, underscoring the importance of early identification and intervention. Timely management of the TyG index may help slow disease progression. In the advanced stages of CKM syndrome, the TyG index may serve as a marker of disease severity and potential irreversibility.
Our subgroup analyses observed a significant interaction effect between sex and age, suggesting a complex interplay of these variables in disease development. This finding underscores the importance of considering participants patient characteristics when assessing the risk of advanced CKM syndrome. In line with our results, a meta-analysis of 87 studies reported that women with metabolic syndrome are more prone to developing cardiovascular disease compared to men47. Furthermore, among participants with impaired glucose tolerance, women exhibit a heightened risk of coronary heart disease relative to men48. These findings partially elucidate the higher prevalence of cardiovascular risk factors among women, which aligns with our current observations49. With advancing age, human metabolic capabilities gradually decline, potentially leading to weight gain, accumulation of adipose tissue, and reduction in muscle mass. This process is associated with an increased risk of developing chronic diseases, thereby exacerbating the progression of CKM syndrome. This study suggests that HDL-C may play a pivotal role in modulating the relationship between the TyG index and CKM syndrome. Individuals with low HDL-C levels appear to face an elevated risk due to the TyG index’s impact on CKM progression, while higher HDL-C levels seem to buffer and stabilize this risk. This aligns with previous findings linking HDL dysfunction to risks of metabolic syndrome, cardiovascular disease, and diabetes, and recognizing HDL-C as an independent predictor of diabetes in those with metabolic syndrome50,51. HDL-C shows potential as a clinical target to reduce CKM risk, particularly for individuals with higher TyG indices. While interactions in other subgroups did not reach statistical significance, certain trends were observed. Given the limitations in sample size, further studies with larger cohorts are needed to clarify these potential associations on CKM syndrome.
This study is based on the NHANES database, utilizing a nationally representative sample of the US population. Rigorous multi-stage probability sampling methods were employed, significantly enhancing the reliability and generalizability of the research results. However, this study also has some limitations. Firstly, although adjustments have been made for multiple potential confounding covariates, the possibility of residual confounding still exists, which may impact the results. Secondly, this study is primarily based on participants from the United States, and geographical constraints may limit the universality and applicability of the research results due to factors such as living environment and dietary habits. Thirdly, only baseline values of the TyG index were collected in the NHANES study, and there is a lack of long-term data on participants’ TyG index status, which may underestimate the assessment of the association between the TyG index and advanced CKM syndrome risk. Additionally, Our CKM staging definitions were adapted from AHA guidelines; however, due to data availability constraints within NHANES, certain staging criteria were adjusted. This study relied on self-reported variables and available biomarkers in NHANES, lacking some subclinical cardiovascular indicators and related disease information, which may affect the consistency and accuracy of CKM staging. Future research should further explore the specific mechanisms linking the TyG index and the risk of advanced CKM syndrome.
Conclusion
In conclusion, there is a significant positive association between the risk of the TyG index and advanced CKM syndrome. Our findings suggest that the TyG index may serve as a practical tool for early risk identification, stratification, and management guidance for CKM syndrome, particularly in primary care settings.
Data availability
The data used in this study were obtained from the National Health and Nutrition Examination Survey (NHANES) conducted between 2011 and 2018. NHANES data is publicly available and can be accessed at the following URL: https://www.cdc.gov/nchs/nhanes/index.htm. The specific datasets used in this analysis include demographic, laboratory, and examination data files from the respective survey years.
References
Magliano, D. J., Boyko, E. J. & I.D.F D.A.t.e.s. committee, IDF Diabetes Atlas, In Idf diabetes atlas. International Diabetes Federation© International Diabetes Federation, 2021.: Brussels. (2021).
Ndumele, C. E. et al. Cardiovascular-kidney-metabolic health: a Presidential Advisory from the American Heart Association. Circulation 148 (20), 1606–1635 (2023).
Aggarwal, R., Ostrominski, J. W. & Vaduganathan, M. Prevalence of Cardiovascular-kidney-metabolic syndrome stages in US adults, 2011–2020. Jama 331 (21), 1858–1860 (2024).
Kadowaki, T. et al. Interconnection between cardiovascular, renal and metabolic disorders: a narrative review with a focus on Japan. Diabetes Obes. Metab. 24 (12), 2283–2296 (2022).
Minh, H. V. et al. Assessment of preferred methods to measure insulin resistance in Asian patients with hypertension. J. Clin. Hypertens. (Greenwich). 23 (3), 529–537 (2021).
Tao, L. C. et al. Triglyceride-glucose index as a marker in cardiovascular diseases: landscape and limitations. Cardiovasc. Diabetol. 21 (1), 68 (2022).
Simental-Mendía, L. E., Rodríguez-Morán, M. & Guerrero-Romero, F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab. Syndr. Relat. Disord. 6 (4), 299–304 (2008).