오랜만에 보는
근골격계 생체역학 논문!!
언젠가 써내야 하는 어깨통증 치료법 책을 위해!!
EFORT Open Rev
. 2020 Sep 10;5(8):508–518. doi: 10.1302/2058-5241.5.200006
Shoulder biomechanics in normal and selected pathological conditions
Patrick Goetti 1, Patrick J Denard 2, Philippe Collin 3, Mohamed Ibrahim 4, Pierre Hoffmeyer 5, Alexandre Lädermann 6,7,8,✉
- Author information
- Article notes
- Copyright and License information
PMCID: PMC7484714 PMID: 32953136
Abstract
The stability of the glenohumeral joint depends on soft tissue stabilizers, bone morphology and dynamic stabilizers such as the rotator cuff and long head of the biceps tendon. Shoulder stabilization techniques include anatomic procedures such as repair of the labrum or restoration of bone loss, but also non-anatomic options such as remplissage or tendon transfers.
Rotator cuff repair should restore the cuff anatomy, reattach the rotator cable and respect the coracoacromial arch whenever possible. Tendon transfer, superior capsular reconstruction or balloon implantation have been proposed for irreparable lesions.
Shoulder rehabilitation should focus on restoring balanced glenohumeral and scapular force couples in order to avoid an upward migration of the humeral head and secondary cuff impingement. The primary goal of cuff repair is to be as anatomic as possible and to create a biomechanically favourable environment for tendon healing.
초록
견관절의 안정성은
연부 조직 안정 장치, 골 형태 및 회전근개와 이두근 장두 건과 같은
동적 안정 장치에 달려 있습니다.
bone morphology and soft tissue stabilizers, dynamic stabilizers
어깨 안정화 기술에는
관절순 복원이나 골 손실 복원과 같은 해부학적 시술뿐만 아니라,
렘플리사주나 힘줄 이식과 같은 비해부학적 옵션도 포함됩니다.
회전근개 복원은
가능한 경우 회전근개 해부학을 복원하고,
회전근개를 재부착하며, 견봉쇄골궁을 존중해야 합니다.
복원이 불가능한 병변의 경우 힘줄 이식, 상부 관절낭 재건 또는 풍선 이식이 제안되어 왔습니다.
어깨 재활은
상완골두의 상방 이동 및 이차적 회전근개 충돌을 방지하기 위해
견관절과 견갑골의 균형 잡힌 힘의 쌍을 회복하는 데 중점을 두어야 한다.
회전근개 봉합술의 주요 목표는
가능한 한 해부학적이며 힘줄 치유에 생체역학적으로 유리한 환경을 조성하는 것이다.
Cite this article: EFORT Open Rev 2020;5:508-518. DOI: 10.1302/2058-5241.5.200006
Keywords: anatomy, glenohumeral instability, humerus, ligaments, rehabilitation, rotator cuff, scapula, therapeutic implications
Introduction
The biomechanics of the shoulder are highly complex.
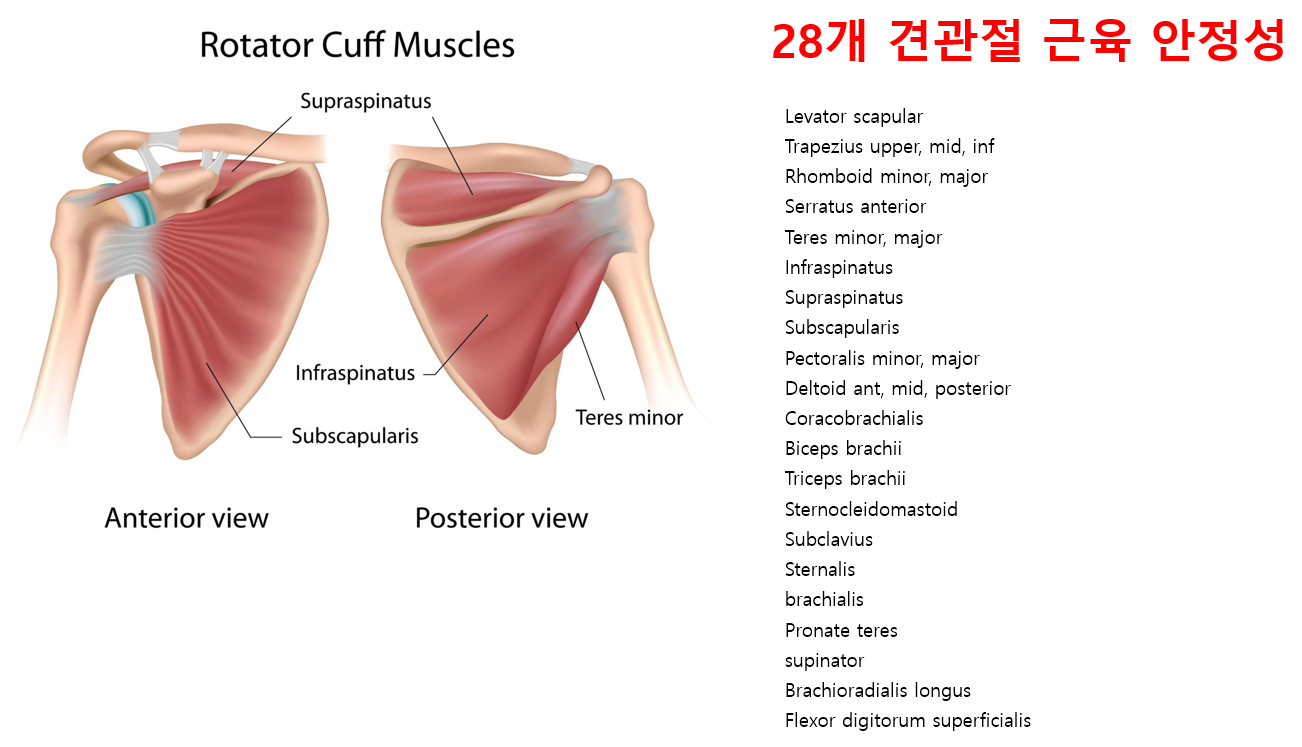
First, it is composed of four joints (glenohumeral, acromioclavicular, scapulothoracic, and sternoclavicular). The glenohumeral joint has six degrees of freedom and is the most mobile joint in the human body, allowing the hand to reach a wide range of positions. This mobility can be further enhanced by translation of the humeral head on the glenoid, but the consequence of this tremendous mobility is perhaps a predisposition to instability and impingements. Second, mobility is assumed by 18 muscles that act in synergy. Consequently, decoupling/isolating them is impossible, making precise kinematic analysis and clinical examination difficult. Third, the glenohumeral joint has the characteristics of an active non-weight-bearing joint, leading to major bony and muscular modifications and frequent tendon overuse.
When looking at the shoulder as a functional unit, it appears that several factors need consideration. To function normally, the shoulder needs all the anatomic structures to work in a chain. Form will allow function.1 First, the central nervous system provides a signal to the muscle-tendon unit. By contracting, the muscle transmits its tension to the tendon, which then acts as a lever arm on the joint. To be efficient, such a system requires a stable fulcrum. The necessary stability is provided by static and dynamic factors such as bony contours, ligaments, labrum, capsule, etc.
The specificity of biomechanically relevant parameters, such as, for example, joint reaction forces, is that they cannot be measured in vivo without invasive procedures.2 Our knowledge therefore mainly relies on experimental cadaveric studies3 or computational modelling.4 These simulations have become more sophisticated in recent years, allowing the inclusion of an increasing number of variables with the ability to adjust both pathology and patient-specific characteristics.5 This ongoing process will without doubt call into question prior assumptions and allow further insights into shoulder biomechanics.
It is crucial to understand the basic principles of shoulder biomechanics and their modifications in the most common pathologies encountered in daily practice. The goal of this article is to provide an overview of normal glenohumeral biomechanics as well as the most common non-prosthetic shoulder disorders including instability and rotator cuff tears.
서론
어깨의 생체역학은 매우 복잡하다.
첫째,
어깨는 네 개의 관절(견관절, 견봉쇄골관절, 견갑흉곽관절, 흉쇄관절)로 구성된다.
견관절은 6자유도를 가지며
인체에서 가장 가동성이 뛰어난 관절로,
손이 광범위한 위치에 도달할 수 있게 한다.
이 가동성은
상완골두가 관절와에서 전위됨으로써 더욱 증대될 수 있으나,
이러한 엄청난 가동성의 결과는 아마도 불안정성과 충돌 증후군에 대한 소인을 초래할 수 있다.
둘째,
18개의 근육이 시너지 작용을 통해 가동성을 담당한다.
따라서
이들 근육을 분리/고립시키는 것은 불가능하여
정밀한 운동학적 분석과 임상 검사가 어려워진다.
셋째,
견관절은 능동적 비체중부하 관절의 특성을 지녀
주요 골격 및 근육 구조 변화와 힘줄 과사용을 초래한다.
어깨를 기능적 단위로 볼 때 여러 요소를 고려해야 한다.
정상 기능을 위해 어깨는 모든 해부학적 구조가 연쇄적으로 작동해야 한다.
형태가 기능을 가능케 한다.1
첫째, 중추신경계가 근건 단위에 신호를 제공한다.
수축을 통해 근육은 긴장을 건으로 전달하며, 건은 관절에 대한 지렛대 역할을 한다.
효율적인 시스템 운영을 위해서는 안정된 지점이 필요하다.
필요한 안정성은 골 구조, 인대, 관절순, 관절낭 등 정적·동적 요소에 의해 제공된다.
관절 반응력 같은 생체역학적 매개변수의 특수성은 침습적 절차 없이는 생체 내에서 측정할 수 없다는 점이다. 2 따라서 우리의 지식은 주로 실험적 사체 연구3 또는 컴퓨터 모델링에 의존한다.4 이러한 시뮬레이션은 최근 몇 년간 더욱 정교해져 병리학적 특성 및 환자별 특성을 모두 조정할 수 있는 능력을 갖추고 점점 더 많은 변수를 포함할 수 있게 되었다.5 이 지속적인 과정은 의심할 여지없이 기존의 가정을 재검토하게 하고 어깨 생체역학에 대한 더 깊은 통찰을 가능하게 할 것이다.
일상 진료에서
가장 흔히 접하는 병리에서 어깨 생체역학의 기본 원리와 그 변형을 이해하는 것은
매우 중요하다.
본 논문의 목적은
정상적인 견관절 생체역학은
물론 불안정성과 회전근개 파열을 포함한
가장 흔한 비인공관절 어깨 질환에 대한 개요를 제공하는 것이다.
Instability
Static stabilizers
Static stability of the glenohumeral joint is provided by the capsulolabral structures as well as the bony anatomy of the glenoid. Historically, significant effort was placed on understanding the importance of the anterior capsulolabral structures, due to the fact that these structures are classically torn in the case of anterior shoulder instability.6 The glenohumeral ligaments are a thickening of the joint capsule and represent the primary static stabilizers. To allow a high degree of shoulder mobility they only become tight at the end-ranges of motion. The superior glenohumeral ligament is tight in adduction, the middle at 45 degrees of abduction and the inferior glenohumeral when the shoulder is brought to 90 degrees of abduction in external rotation.7 The inferior glenohumeral ligament is therefore considered the strongest and most important soft tissue stabilizer. Structurally it can be avulsed from the glenoid side resulting in an antero-inferior labral lesion, as well as from the humeral side resulting in the less-frequent humeral avulsion of the glenohumeral ligament (HAGL) lesion.8,9 The postero-inferior capsule and posterior inferior glenohumeral ligament are not as robust as their anterior counterparts,10 but it is often felt to be necessary to ‘balance’ both inferior ligaments during a soft tissue repair for instability. Laxity is a normal, physiologic and asymptomatic finding, that corresponds to translation of the humeral head in any direction to the glenoid.11 Hyperlaxity is constitutional, multidirectional, bilateral and asymptomatic. Hyperlaxity of the shoulder is probably best defined as external rotation with the elbow at the side equal to or greater than 85 degrees.12 This non-pathological finding is a risk factor for instability but does not by itself demand treatment unless there is clear pathological laxity. Pathological laxity of the inferior glenohumeral ligament is observed when passive abduction in neutral rotation in the glenohumeral joint is above 105 degrees, there is apprehension above 90 degrees of abduction, or if a difference of more than 20 degrees between the two shoulders is noted.13,14 Pathological laxity is often multidirectional and associated with a redundant capsule leading to an increased glenohumeral volume.15 Biomechanical studies have focused on evaluating the effectiveness of soft tissue procedures to reduce capsular volume. Cadaveric models created by stretching the capsule 10–30% beyond the maximal range of motion, revealed that 1 cm capsular shifts were effective to reduce capsular volume by an average 33.7% (range, 25.3% to 44.6%).16–18 Ponce et al further reported a linear relationship between the number of 1 cm stitches and capsular volume, each plication reducing the volume by approximately 10%.19 Lastly, while both capsular plication and rotator interval closure have been reported to be effective in restoring intact range of motion after capsular stretching, the addition of an interval closure has the benefit of better restoring humeral head translation at 60 degrees of abduction.18,20
The osseous glenoid is relatively flat, the biomechanical role of the glenoid cartilage and labrum is to double the depth of the glenoid socket and therefore enhance the contact area with the humeral head.21–23 This is further believed to stabilize the joint by helping to centre the humeral head when compressed against the glenoid by the rotator cuff muscles (concavity compression mechanism). A complete loss of the anterior labrum has been reported to decrease the contact area by 7% to 15%, and increase the mean contact pressure by 8% to 20%.24 A biomechanical study by Hara et al identified the antero-inferior labrum as being the weakest point, with a mean force necessary to cause a rupture of 3.84 ± 1.00 kg/5 mm.25 Finally, it was postulated that an intact labrum could help create a negative intra-articular pressure (vacuum effect); this effect is, however, thought to be marginal when the rotator cuff muscles are contracted.26–28 Despite these important stabilizing effects, Itoi et al revealed that soft tissues alone play only a minor role in glenohumeral stability in mid-range of motion.29
불안정성정적 안정화 장치
견관절의 정적 안정성은 관절낭-관절순 구조와 견갑골의 골성 해부학에 의해 유지됩니다. 역사적으로 전방 견관절 불안정증에서 전방 관절낭-관절순 구조가 전형적으로 파열된다는 사실로 인해, 이 구조들의 중요성을 이해하는 데 상당한 노력이 기울여졌습니다.6
견관절 인대는 관절낭의 두꺼워진 부분으로,
주요 정적 안정화 장치 역할을 합니다.
높은 수준의 어깨 가동성을 허용하기 위해
이 인대들은 운동 범위의 끝점에서만 긴장된다.
상부 견관절 인대는 내전 시,
중간 인대는 외전 45도 시,
하부 견관절 인대는 외회전 상태에서 외전 90도 시 긴장된다.7
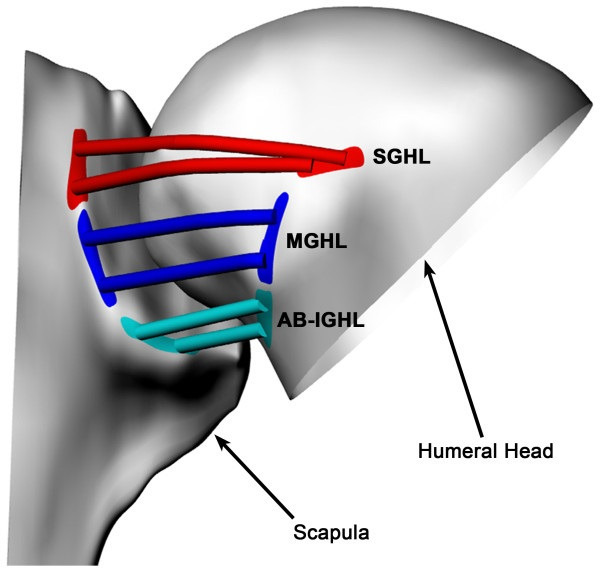
따라서
하부 견관절 인대는
가장 강력하고 중요한 연부 조직 안정기로 간주된다.
구조적으로 이 인대는
관절와 측에서 박리되어 전하방 관절순 손상을 초래할 수 있으며,
상완골 측에서 박리되어 덜 흔한 상완골 박리성 견관절 인대(HAGL) 손상을 유발할 수 있습니다.8, 9
후하방 관절낭과 후하방 견관절 인대는 전방 인대들만큼 견고하지는 않지만,10 불안정성 치료를 위한 연부 조직 수복 시 양측 하방 인대를 ‘균형’ 잡는 것이 종종 필요하다고 여겨진다. 관절 이완은 정상적이고 생리적이며 무증상 소견으로, 상완골두가 관절와에 대해 어느 방향으로든 이동할 수 있는 상태를 의미한다.11 과이완은 선천적이며 다방향성, 양측성이며 무증상이다. 어깨 과이완은 팔꿈치를 몸통에 붙인 상태에서 외회전이 85도 이상일 때 가장 잘 정의된다.12
이 비병리적 소견은 불안정성의 위험 요인이지만, 명백한 병리적 이완이 없는 한 그 자체로 치료를 요구하지는 않는다. 병리적 관절낭 이완은 견관절 중립 회전 상태에서 수동 외전 각도가 105도를 초과하거나, 90도 이상 외전 시 불안감이 느껴지거나, 양측 어깨 간 20도 이상의 차이가 관찰될 때 하부 견관절 인대의 병리적 이완으로 진단됩니다.13, 14 병리적 이완은 종종 다방향적이며 과다한 관절낭과 연관되어 견관절 부피 증가를 초래한다.15 생체역학적 연구는 관절낭 부피 감소를 위한 연부 조직 수술의 효과 평가에 초점을 두었다. 최대 가동 범위를 10~30% 초과하여 관절낭을 신장시킨 시체 모델 연구에서, 1cm의 관절낭 이동이 관절낭 부피를 평균 33.7%(범위 25.3%~44.6%) 감소시키는 데 효과적임이 밝혀졌다. 16–18 Ponce 등은 1cm 봉합 횟수와 관절낭 부피 사이에 선형 관계가 있으며, 각 주름 접힘이 부피를 약 10% 감소시킨다고 추가 보고하였다. 19 마지막으로, 관절낭 주름 잡기와 회전근개 간격 봉합술 모두 관절낭 신장 후 정상 가동 범위를 회복시키는 데 효과적이라고 보고되었으나, 간격 봉합술을 추가하면 외전 60도에서 상완골두의 이동을 더 잘 회복시키는 이점이 있다.18,20
골성 관절와(glenoid)는 상대적으로 평평하며, 관절와 연골과 관절순(labrum)의 생체역학적 역할은 관절와 소켓의 깊이를 두 배로 늘려 상완골두와의 접촉 면적을 증가시키는 것이다.21–23 이는 회전근개 근육에 의해 관절와에 압박될 때 상완골두를 중심에 위치시키는 데 도움을 줌으로써 관절을 안정화시키는 것으로 추가로 알려져 있다(오목부 압박 기전). 전방 관절순의 완전 손실은 접촉 면적을 7~15% 감소시키고 평균 접촉 압력을 8~20% 증가시키는 것으로 보고되었다. 24 Hara 등의 생체역학적 연구에서는 전하방 관절순이 가장 취약한 부위로 확인되었으며, 파열을 유발하는 데 필요한 평균 힘은 3.84 ± 1.00 kg/5 mm로 보고되었다.25 마지막으로, 온전한 관절순은 관절 내 음압(진공 효과)을 생성하는 데 도움이 될 수 있다고 가정되었으나, 그러나 회전근개 근육이 수축된 상태에서는 이 효과가 미미한 것으로 여겨진다.26–28 이러한 중요한 안정화 효과에도 불구하고, 이토이(Itoi) 등은 중간 가동 범위에서 관절의 안정성에 연부 조직만으로는 미미한 역할만 한다고 밝혔다.29
Glenoid bone defects and morphology
An important concept regarding glenohumeral joint stability is the concavity compression principle, which centres the humeral head on the glenoid. This centring mechanism is the result of the rotator cuff compressing the humeral head against the glenoid cavity, and is one reason why an anterior glenoid rim defect predisposes to recurrent anterior instability.30 While there is some controversy, 15% to 20% glenoid bone loss seems to be the cut-off value for soft tissue repair.31,32 Shin et al demonstrated that in case of an anterior defect ≥ 15%, a soft tissue procedure (Bankart) is unable to restore normal shoulder kinematics and even leads to postero-inferior translation of the humeral head in abduction and external rotation.32 On the other hand, bone grafting (glenoidplasty) can successfully reconstruct glenoid curvature and depth and therefore restore stability.30,33 Another key point is the reduced contact area and increased articular contact pressure induced by bony glenoid defects.24 While iliac bone graft (Eden-Hybinette), articular distal clavicle autografts and coracoid transfer (Latarjet or Bristow) can all restore normal values, the correct position and orientation of the bone graft is important.34,35 The Latarjet will, however, be limited by the amount of bone that can be harvested. Young et al reported mean values of 26.4 ± 2.9 mm and 9.3 ± 1.4 mm for length and thickness respectively.36 A graft placed in too lateral of a position will lead to an increased anterior-inferior peak contact pressure, whereas a recessed graft will lead to high edge loading. To avoid increased inferior contact pressure, the current evidence suggests orientating the coracoid bone graft in an inferior direction.37 The congruent-arc modification of the original Latarjet technique further allows the reconstruction of larger defects by matching the shape of the graft to that of the glenoid.38 The use of a distal tibial osteochondral allograft respects all these biomechanical principles and has been shown to be a valid alternative in the absence of reliable autograft.39
During posterior shoulder dislocation, reverse Bankart lesions are only present in isolation in 51% of cases.40 They are, however, sufficient to increase posterior translation and inferior translation of the humerus in the sulcus position by 86% and 31% respectively.41 Additionally, glenoid retroversion is more common in posterior instability and appears to predispose to posterior instability.42 Every five-degree increment of retroversion led to an additional posterior decentralization of the humeral head overall by (average ± standard deviation) 2.0 mm ± 0.3 in the intact and 2.0 mm ± 0.7 in the detached labrum condition. Bony alignment in terms of glenoid retroversion angle plays an important role in joint centration and posterior translation, especially in retroversion angles greater than 10 degrees.43 Labral injury from repetitive posterior loading or instability can range from a posterior labral tear to an incomplete, concealed avulsion of the postero-inferior labrum (also known as ‘Kim lesion’) to a reverse Bankart lesion. Glenoid retroversion beyond the average five degrees to 10 degrees has been shown to be a risk factor for developing subsequent posterior instability in a prospective study of healthy subjects. For every one degree increase in glenoid retroversion, the risk for posterior instability increase by 17%.44
관절와 결손 및 형태학
견관절 안정성에 관한 중요한 개념은 오목부 압축 원리로,
이는 상완골두를 관절와 중심에 위치시킨다.
concavity compression principle
이 중심화 메커니즘은
회전근개가 상완골두를 관절와강에 압박함으로써 발생하며,
관절와 전방 가장자리 결손이 재발성 전방 불안정성을 유발하는 이유 중 하나이다. 30
논란의 여지가 있지만,
15~20%의 관절와 골 손실이 연부 조직 수복의 기준값으로 보인다.31,32
신(Shin) 등은 전방 결손이 15% 이상인 경우 연부 조직 수술(Bankart)로는 정상적인 어깨 운동학을 회복할 수 없으며, 오히려 외전 및 외회전 시 상완골두의 후하방 이동을 유발할 수 있음을 입증했다. 32 반면, 골 이식술(관절와 성형술)은 관절와 곡률과 깊이를 성공적으로 재건하여 안정성을 회복시킬 수 있다.30,33 또 다른 핵심 요소는 골성 관절와 결손으로 인한 접촉 면적 감소와 관절 접촉 압력 증가이다.24 장골 골 이식(Eden-Hybinette), 관절면 원위부 쇄골 자가골 이식 및 견봉이식술(라타르제 또는 브리스토우)은 모두 정상 값을 회복시킬 수 있으나, 골 이식의 정확한 위치와 방향이 중요하다.34,35 그러나 라타르제술은 채취 가능한 골의 양에 의해 제한을 받는다. 영(Young) 등은 평균 길이와 두께가 각각 26.4 ± 2.9 mm 및 9.3 ± 1.4 mm라고 보고하였다.36 이식편이 너무 외측 위치에 배치되면 전하방 접촉 압력이 증가하는 반면, 함몰된 이식편은 높은 가장자리 하중을 초래한다. 하방 접촉 압력 증가를 피하기 위해, 현재 증거는 견봉골 이식편을 하방 방향으로 배향할 것을 제안한다. 37 원본 라타르제 기법의 일치 아크 수정법은 이식편의 형태를 관절와 모양에 맞추어 더 큰 결손 부위의 재건이 가능하게 한다.38 원위 경골 골연골 동종 이식편의 사용은 이러한 모든 생체역학적 원리를 준수하며, 신뢰할 수 있는 자가 이식편이 없을 때 유효한 대안으로 입증되었다.39
후방 어깨 탈구 시 역방크트 병변은 51%의 사례에서 단독으로 존재한다.40 그러나 이는 상완골이 홈 위치에 있을 때 후방 이동을 86%, 하방 이동을 31% 각각 증가시키기에 충분하다.41 또한, 관절와 후방 회전은 후방 불안정성에서 더 흔하며 후방 불안정성을 유발하는 요인으로 보인다. 42 후방 회전이 5도 증가할 때마다 상완골두의 후방 이탈은 전체적으로 (평균 ± 표준편차) 온전한 상태에서는 2.0mm ± 0.3, 분리된 상과순 상태에서는 2.0mm ± 0.7 추가로 발생하였다. 관절와 후방 회전각에 따른 골 정렬은 관절 중심화와 후방 이동에 중요한 역할을 하며, 특히 10도 이상의 후방 회전각에서 그러하다.43 반복적인 후방 하중 또는 불안정성에 의한 관절순 손상은 후방 관절순 파열부터 후하방 관절순의 불완전하고 은폐된 박리(‘김 병변’으로도 알려짐) 및 역방 뱅크아트 병변에 이르기까지 다양할 수 있다. 건강한 대상을 대상으로 한 전향적 연구에서, 평균 5도에서 10도를 초과하는 관절와 후방 회전은 후방 불안정성 발생의 위험 요인으로 밝혀졌습니다. 관절와 후방 회전이 1도 증가할 때마다 후방 불안정성 위험은 17% 증가합니다.44

Humeral bone defects
A Malgaigne lesion45 also called a Hill–Sachs lesion46 describes the grooved defect of the humeral head. This frequently unrecognized complication of anterior dislocation of the shoulder joint is the result of compression of the posterolateral head upon the anterior glenoid rim. The presence of humeral bone loss has been linked with recurrent instability after open or arthroscopic shoulder stabilization.47,48 Cadaveric studies have revealed that humeral bone defects as small as 12.5% of the humeral head diameter will affect joint stability, which can be restored with allograft reconstruction. However, an isolated 25% bone loss was not shown to be sufficient to explain recurrent instability on its own.49–51 In other words, glenoid bone loss is required as well. Clinically, the more common alternative to allograft reconstruction is the remplissage procedure, which insets the posterior capsule and infraspinatus tendon into the lesion. This procedure medializes the insertion of the posterior structures to prevent engagement and also decreases anterior translation of the humeral head. A recent review identified 10 biomechanical studies of which only one reported persistent engagement after a remplissage procedure in the presence of a 25% humeral head defect.52 The same study further compared the remplissage to the Latarjet and found that 84% of specimens (27 of 32 testing scenarios) stabilized after remplissage, and 94% of specimens (30 of 32 testing scenarios) stabilized after the Latarjet procedure. This was, however, not statistically significant and the authors concluded that both techniques are effective.53 Nevertheless, at maximum external rotation at 60 degrees of abduction, remplissage altered the kinematics of the glenohumeral joint by shifting posteriorly and inferiorly the apex of the humeral head.54 Moreover, while often described as an inset of the infraspinatus tendon, the procedure is in fact a capsulomyodesis of the infraspinatus and teres minor;55 this has not only been proven in anatomic investigation, but also follows normal form as the tendon does not extend very far medially from its normal insertion.
For posterior instability, the McLaughlin procedure56 using the detached subscapularis tendon has been described for locked posterior instability in presence of a reverse Malgaigne (Hill–Sachs) lesion. This technique has been subsequently modified as either a reverse remplissage57 or an osteotomy of the lesser tuberosity with the attached subscapularis (Hughes and Neer method) to allow additional bone support to articular cartilage with satisfactory outcome both in acute and chronic setting.58,59
상완골 결손
말게인 병변(Malgaigne lesion)45 또는 힐-삭스 병변(Hill–Sachs lesion)46은 상완골두의 홈 모양 결손을 의미한다. 이 병변은 어깨 관절 전방 탈구 시 흔히 간과되는 합병증으로, 상완골두 후측부가 관절와 전방 가장자리에 압박되어 발생한다. 상완골 골손실의 존재는 개방적 또는 관절경적 어깨 안정화 수술 후 재발성 불안정성과 연관되어 있다.47,48 시체 연구에 따르면 상완골두 직경의 12.5%에 불과한 작은 상완골 결손도 관절 안정성에 영향을 미치며, 이는 동종이식 재건술로 회복될 수 있다. 그러나 단독으로 25%의 골 손실만으로는 재발성 불안정성을 설명하기에 충분하지 않음이 밝혀졌다.49–51 즉, 관절와 골 손실 또한 동반되어야 한다. 임상적으로 동종 이식 재건술보다 더 흔한 대안은 후방 관절낭과 견갑하근 건을 결손 부위에 삽입하는 렘플리사주(replissage) 시술이다. 이 시술은 후방 구조물의 부착부를 내측으로 이동시켜 관절면 접촉을 방지하고 상완골두의 전방 이동을 감소시킨다. 최근 문헌 고찰에서 10건의 생체역학적 연구를 확인했으며, 그중 단 한 건만이 상완골두 결손 25%가 존재하는 상태에서 렘플리사주 시술 후 지속적인 접촉을 보고하였다.52 동일한 연구는 렘플리사주와 라타르제(Latarjet)를 추가로 비교하여, 렘플리사주 후 표본의 84%(32개 시험 시나리오 중 27개)가 안정화되었으며, 라타르제술 후에는 94%(32개 시험 시나리오 중 30개)의 표본이 안정화되었습니다. 그러나 이는 통계적으로 유의미하지 않았으며, 저자들은 두 기술 모두 효과적이라고 결론지었습니다.53 그럼에도 불구하고, 60도 외전 시 최대 외회전에서는 렘플리사주술이 상완골두 정점을 후방 및 하방으로 이동시켜 견관절 운동학을 변화시켰습니다. 54 또한, 흔히 견갑하근 힘줄의 내삽술로 설명되지만, 이 시술은 실제로 견갑하근과 소원근의 관절낭근접합술이다;55 이는 해부학적 연구에서 입증되었을 뿐만 아니라, 힘줄이 정상 부착부에서 내측으로 크게 확장되지 않는 정상 형태를 따르기 때문이다.
후방 불안정성의 경우, 역말가인(Hill–Sachs) 병변이 존재하는 고정된 후방 불안정성에 대해 분리된 견갑하근 힘줄을 사용하는 맥라플린(McLaughlin) 시술56이 기술되어 있습니다. 이 기법은 이후 역방향 렘플리사주(reverse remplissage)57 또는 부착된 견갑하근과 함께 소결절(lesser tuberosity)의 골절술(Hughes and Neer method)로 수정되어 관절 연골에 추가적인 골 지지대를 제공하며, 급성 및 만성 양상 모두에서 만족스러운 결과를 보였다.58,59
Bipolar defects
Neither glenoid nor humeral head bone loss can be viewed individually. Just as they occur together at the time of injury, they interact in the risk of recurrent instability. The concept of the glenoid track has emerged as a way to understand this relationship. The concept was first proposed by Yamamoto et al, who used three-dimensional computed tomography (CT) scans to reveal that the normal glenoid track is 84% ± 14% of the glenoid width.60 Subsequently this was validated in live subjects where the value was determined to be 83%. This concept is in fact the continuation of the work by Burkhart and De Beer on engaging vs. non-engaging Hill–Sachs lesions.61 Di Giacomo et al further refined this to the on-track and off-track concept, stating that glenoid bone loss will result in a reduction in the width of the glenoid track.62 In the setting of glenoid bone loss, the glenoid track decreases. The glenoid track in the bone loss situation is determined by subtracting the width of the defect from 83% of the original glenoid width, which is thought to be the width in the absence of a glenoid.63 Then, the width of the Hill–Sachs defect from the origin of the infraspinatus to the most medial extent of the defect is measured and compared to the glenoid track to determine whether it exceeds the glenoid track (‘off-track’) or is less than the glenoid track (‘on-track’).
양극성 결손
관절와와 상완골두의 골손실은 개별적으로 볼 수 없습니다. 손상 시점에 함께 발생하듯이, 재발성 불안정성 위험에서도 상호작용합니다. 이 관계를 이해하기 위한 방법으로 관절와 트랙 개념이 등장했다. 야마모토 등이 최초로 제안한 이 개념은 3차원 컴퓨터 단층촬영(CT)을 통해 정상 관절와 트랙이 관절와 너비의 84% ± 14%임을 밝혀냈다.60 이후 생체 대상 연구에서 이 값이 83%로 확인되었다. 이 개념은 사실 버크하트(Burkhart)와 드 비어(De Beer)가 연구한 ‘접촉성 대 비접촉성 힐-삭스 병변’ 연구의 연장선상에 있다.61 디 자코모(Di Giacomo) 등은 이를 ‘온트랙(on-track)'과 '오프트랙(off-track)’ 개념으로 정교화하며, 관절와 골 손실이 관절와 트랙 너비의 감소를 초래한다고 밝혔다.62 관절와 골 손실이 발생한 상황에서는 관절와 트랙이 감소한다. 골 손실 상황에서 관절와 트랙은 관절와 결손 폭을 원래 관절와 폭의 83%에서 빼서 결정하는데, 이는 관절와가 없는 상태에서의 폭으로 간주됩니다. 63 그런 다음, 하방근 기시부에서 결손부의 가장 내측 끝까지의 힐-삭스 결손부 너비를 측정하여 관절와 트랙과 비교함으로써, 결손부 너비가 관절와 트랙을 초과하는지(‘오프-트랙’) 또는 관절와 트랙보다 작은지(‘온-트랙’)를 판단합니다.
Dynamic stabilization (rotator cuff, conjoint tendon and long head of the biceps)
Dynamic stability of the glenohumeral joint is provided by the muscular structures during the mid-points of range of motion. As stated above, the rotator cuff is key to the concavity-compression concept in which it actively contributes to stability in opposition to the deltoid and pectoralis muscles (which tend to destabilize the joint superiorly and anteriorly).64,65 The cuff contributes to anterior (external rotators) and posterior (internal rotators) stability in cadaveric66,67 and electromyographic studies.68 While all rotator cuff muscles contribute to anterior joint stability, the subscapularis seems to be the least effective at end-range of motion in opposition to the long head of the biceps.69
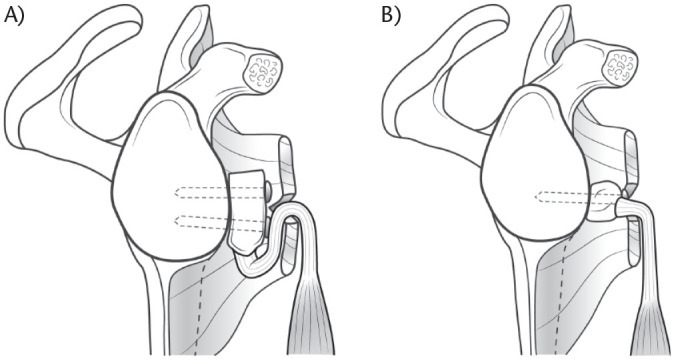
In addition to the previously mentioned bony augmentation, the Latarjet procedure and its variant the Bristow combine (1) the ligamentous effect by augmentation of the coracoacromial ligament by the inferior glenohumeral ligament, (2) a muscular effect (hammock effect) by lowering the inferior part of the subscapularis, which is mainly efficient in mid-range motion (Fig. 1A and Fig. 1B),70 as well as (3) a sling effect induced by the conjoint tendon forming an anterior rampart especially efficacious in end-range motion (Fig. 2). The two latter effects have often been confused in the literature.
동적 안정화 (회전근개, 공동건 및 이두근 장두)
견관절의 동적 안정성은
관절 가동 범위 중간 지점에서 근육 구조에 의해 제공된다.
앞서 언급한 바와 같이,
회전근개는 오목부 압박 개념의 핵심으로,
삼각근 및 대흉근(관절을 상방 및 전방으로 불안정하게 만드는 경향이 있음)에 대항하여
회전근개는 시체 연구66,67 및 근전도 연구68에서 전방(외회전근) 및 후방(내회전근) 안정성에 기여하는 것으로 나타났다. 모든 회전근개 근육이 관절 전방 안정성에 기여하지만, 견갑하근은 상완이두근 장두에 대항하여 관절 가동 범위 말단에서 가장 효과가 낮은 것으로 보인다.69
앞서 언급한 골성 보강술 외에도, 라타르제술과 그 변형인 브리스토우술은 (1) 하부 견관절 인대를 이용한 견봉쇄골 인대의 보강을 통한 인대적 효과, (2) 주로 중간 가동 범위에서 효과적인 견갑하근 하부 하강에 의한 근육 효과(해먹 효과)(그림 1A 및 그림 1B),70 그리고 (3) 특히 최종 가동 범위에서 효과적인 전방 방어벽을 형성하는 공동건에 의한 슬링 효과(그림 2)를 결합한다. 후자의 두 효과는 문헌에서 종종 혼동되어 왔다.
Fig. 1.
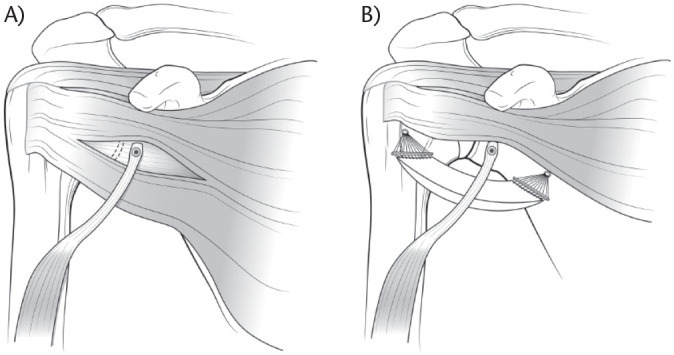
(a) Anterior view of a left shoulder after dynamic anterior stabilization. (b) Lowering the inferior part of the subscapularis muscle done by biceps tendon in low-range motion is called ‘hammock effect’. It represents a muscular effect.
(a) 동적 전방 안정화 후 좌측 어깨의 정면 관점. (b) 저범위 운동 시 이두근 건에 의해 수행되는 견갑하근 하부 하강은 '해먹 효과'라 불린다. 이는 근육적 효과를 나타낸다.
Fig. 2.
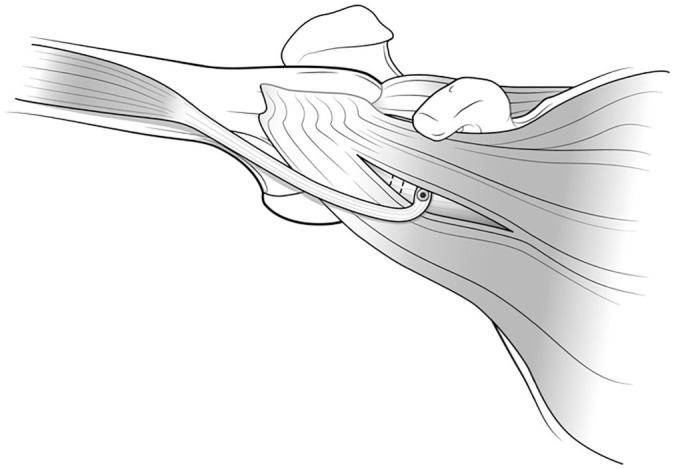
Anterior view of a left shoulder after dynamic anterior stabilization. At higher range of abduction, the biceps tendon is more horizontal and does not lower the inferior part of the subscapularis muscle anymore. It forms a veritable sling in front of the shoulder, called the sling effect.
According to a cadaveric study by Yamamoto et al, the hammock and sling effects appear to be the primary stabilizers and account for 51% to 62% of shoulder stability in mid-range of motion, and up to 76% to 77% at 90 degrees of abduction and maximal external rotation (end-range motion).71 The Latarjet technique further leads to an enhanced sling effect in comparison to the Bristow procedure due to the inferior graft position and subsequent conjoint tendon orientation and trajectory (Fig. 3).72
동적 전방 안정화 후 좌측 어깨의 정면 관점. 외전 범위가 높아질수록 이두근 건은 더 수평이 되어 견갑하근 하부를 더 이상 하강시키지 않습니다. 이는 어깨 전방에 진정한 슬링을 형성하며, 이를 슬링 효과라 합니다.
야마모토 등의 시체 연구에 따르면, 해먹 효과와 슬링 효과는 주요 안정화 장치로 작용하며 중간 가동 범위에서 어깨 안정성의 51~62%, 외전 90도 및 최대 외회전(최대 가동 범위) 시 최대 76~77%를 차지한다. 71 라타르제 기법은 하부 이식편 위치와 그에 따른 공동건의 방향 및 경로로 인해 브리스토우 수술에 비해 슬링 효과를 더욱 강화시킵니다(그림 3).72
Fig. 3.
Sagittal illustration of a right shoulder. Direction of the conjoint tendon in (a) the Latarjet and (b) Bristow procedure. Note that the conjoint tendon during Latarjet has to go around the inferior subscapularis (a). Contrarily, the conjoint tendon exits directly through the split during the Bristow procedure (b).
우측 어깨의 시상면 도식. (a) 라타르제 및 (b) 브리스토 수술에서 공동건의 방향. 라타르제 시술 시 공동건은 하부 견갑하근 주위를 돌아야 함(a). 반면 브리스토 시술에서는 공동건이 분할 부위를 통해 직접 빠져나옴(b).
These hammock and sling effects are also the central point of the recently developed dynamic anterior stabilization (DAS) procedure. In this technique the long head of the biceps, in place of the conjoint tendon, it transferred through a subscapularis split to the anterior glenoid margin.73 The DAS results in decreased anterior glenohumeral translation depending on the glenoid defect conditions. As compared with isolated Bankart repair, DAS shows significantly less relative anterior translation in 10% glenoid defects at translation forces of 20 N (0.3 ± 1.7 mm vs. 2.2 ± 1.8 mm, P = .005) and 30 N (2.6 ± 3.4 mm vs. 5.3 ± 4.2 mm, P = .044) and in 20% glenoid defects at all translation forces (20 N: –3.2 ± 4.7 mm vs. 0.8 ± 4.1 mm, P = .024; 30 N: –0.9 ± 5.3 mm vs. 4.0 ± 5.2 mm, P = .005; 40 N: 2.1 ± 6.6 mm vs. 6.0 ± 5.7 mm, P = .035).31 However, similar to previous biomechanical observations regarding isolated conjoint tendon transfer in 20% glenoid defects, DAS leads to a relevant posterior and inferior shift of the humeral head in the abduction external rotation (ABER) position and to a relevant increase in inferior glenohumeral translation and should consequently not be used for large bony defects.31,74 A recent comparative study on a subcritical bone model reported significantly improved peak resistance force to anterior displacement when augmenting labral repair with a transfer of the long head of the biceps compared to the conjoint tendon (54.1 ± 5.5 N vs. 46.5 ± 7.6 N; P = .039).75 The DAS does not appear to limit postoperative rotational range of motion.31
이러한 해먹 및 슬링 효과는 최근 개발된 동적 전방 안정화(DAS) 수술의 핵심이기도 하다. 이 기법에서는 공동건 대신 이두근 장두를 견갑하근 분열부를 통해 전방 관절와 가장자리로 이식한다.73 DAS는 관절와 결손 상태에 따라 전방 견관절 전위 감소 효과를 보인다. 단독 뱅크아트 봉합술과 비교 시, DAS는 20N(0.3 ± 1.7 mm vs. 2.2 ± 1.8 mm, P = .005) 및 30N(2.6 ± 3.4 mm vs. 5.3 ± 4.2 mm, P = .044) 및 모든 전위력에서 20% 관절와 결손 시(20 N: –3.2 ± 4.7 mm vs. 0.8 ± 4.1 mm, P = .024; 30 N: –0.9 ± 5.3 mm vs. 4.0 ± 5.2 mm, P = .005; 40 N: 2.1 ± 6.6 mm vs. 6.0 ± 5.7 mm, P = .035). 31 그러나 20% 관절와 결손에서 단독으로 시행한 공동건 이식에 관한 기존 생체역학적 관찰과 유사하게, DAS는 외전 외회전(ABER) 위치에서 상완골두의 후방 및 하방 이동을 유발하고 하방 견관절 이동을 현저히 증가시키므로, 큰 골 결손에는 사용해서는 안 된다.31, 74 최근 하위 임계 골 모델을 대상으로 한 비교 연구에서는 관절순 수복술에 공동건 이식보다 상완이두근 장두 이식을 병행할 경우 전방 변위에 대한 최대 저항력이 유의미하게 향상되었다고 보고하였다(54.1 ± 5.5 N vs. 46.5 ± 7.6 N; P = .039).75 DAS는 수술 후 회전 가동 범위를 제한하지 않는 것으로 보인다.31

Scapular morphology
Specific acromial morphology in the sagittal plane is significantly associated with the direction of glenohumeral instability. In shoulders with posterior instability, the acromion is situated higher and is oriented more horizontally than in shoulders with anterior instability. This acromial position may provide less osseous restraint against posterior humeral head translation. Posterior instability virtually never occurs with a steep ‘Swiss chalet roof-type’ acromion.76
견갑골 형태학
시상면에서의 특정한 견봉 형태는
견관절 불안정성의 방향과 유의미한 연관성을 보인다.
후방 불안정성이 있는 어깨에서는
전방 불안정성이 있는 어깨에 비해 견봉이 더 높게 위치하며 수평 방향으로 더 기울어져 있다.
이러한 견봉 위치는 후방 상완골두 전위에 대한 골성 제약력을 감소시킬 수 있다.
Swiss chalet roof-type’ acromion
후방 불안정은
가파른 ‘스위스 산장 지붕형’ 견봉에서는 사실상 발생하지 않는다.76
Restoration of stability
It is important to keep in mind that even if shoulder stabilization procedures are efficient to prevent recurrent macro-instability (defined as a recurrent shoulder dislocation), they seem inefficient in preventing micro-instability (defined as residual humeral head translation), which could be an explanation for persistent apprehension.77
Rehabilitation
From a biomechanical point of view, rehabilitation protocols after glenohumeral instability should avoid excessive pressure and over tensioning on the repaired structures. Regarding pressure, humeral cartilage and labral compression evaluated by motion simulation only occurred in the superior half of the glenoid during exercises.78 This indicates that postoperative exercises do not lead to important pressure changes on an inferior labral repair. Concerning soft tissue tension, rehabilitation should be performed in the scapular plane, which lies about 30 degrees anterior to the coronal plane of the body.79 This position allows for decreased stress on the anterior capsular structures, optimized glenohumeral congruence and enhanced functional activity of the posterior cuff compared to the body plane.79 As already mentioned, the rotator cuff acts as a key dynamic stabilizer, and if its force couples go unbalanced, the deltoid muscle will create an upward migration of the humeral head and secondary cuff impingement.80 The same principle applies to the scapula, where the serratus anterior and trapezius act as the primary force couple stabilizing the scapula in abduction in the scapular plane.81 Rehabilitation should therefore focus on strengthening and careful balancing of these force couples. Regarding soft tissues repair, protection is best achieved by avoiding constraints to the antero-inferior capsule-labral complex. At 0 degree of abduction, Black et al found that the low-tension zone was around 45 degrees of external rotation, in case of anterior capsular shortening of only 2 mm this zone was reduced by an additional 20 degrees.82 Penna et al confirmed these findings, further reporting that combination of passive abduction and external rotation was responsible for a maximum measured force of 17.7 N on a capsule-labral repair.83 While it seems reasonable to limit excessive stress on the capsule during early rehabilitation, residual capsular shortening on the other hand should be avoided as it alters physiologic glenohumeral head translation.84
안정성 회복
어깨 안정화 수술이 재발성 거대 불안정(재발성 어깨 탈구로 정의됨)을 예방하는 데 효과적일지라도, 잔여 상완골두 전위(잔여 불안정으로 정의됨)를 예방하는 데는 비효율적인 것으로 보이며, 이는 지속적인 불안감의 원인이 될 수 있다는 점을 명심해야 한다.77
재활
생체역학적 관점에서,
견관절 불안정성 수술 후 재활 프로토콜은
수복된 구조물에 대한 과도한 압력과 과도한 장력을 피해야 한다.
압력 측면에서,
운동 시뮬레이션을 통해 평가된 상완골 연골 및 관절순 압박은
운동 중 관절와 상부 반에서만 발생하였다.78
이는 수술 후 운동이 하부 관절순 수복에 중요한 압력 변화를 초래하지 않음을 시사한다.
연부 조직 장력 측면에서 재활은 체의 관상면보다 약 30도 전방에 위치한 견갑골 평면에서 수행되어야 한다.79 이 위치는 체 평면에 비해 전방 관절낭 구조물에 가해지는 스트레스를 감소시키고, 견관절 정합성을 최적화하며, 후방 회전근개 기능 활동을 향상시킨다.79 앞서 언급한 바와 같이, 회전근개는 핵심 동적 안정화 장치 역할을 하며, 그 힘의 쌍이 불균형해지면 삼각근이 상완골두의 상향 이동을 유발하고 이차적인 회전근개 충돌을 일으킵니다.80 동일한 원리가 견갑골에도 적용됩니다. 전거근과 승모근은 견갑골 평면에서 견갑골 외전 시 안정화를 담당하는 주요 힘의 쌍 역할을 합니다.81 따라서 재활은 이러한 힘의 쌍을 강화하고 신중하게 균형을 맞추는 데 초점을 맞춰야 합니다. 연부 조직 수복과 관련하여, 전하방 관절낭-관절순 복합체에 대한 제약을 피하는 것이 최선의 보호 방법이다. 외전 0도에서 Black 등은 전방 관절낭 단축이 2mm에 불과한 경우에도 외회전 45도 부근이 저장력 구역이며, 이 구역이 추가로 20도 감소함을 발견했다. 82 Penna 등은 이러한 결과를 확인했으며, 수동 외전과 외회전의 조합이 관절낭-관절순 수복부에 최대 17.7 N의 측정된 힘을 유발한다고 추가 보고하였다.83 초기 재활 중 관절낭에 가해지는 과도한 스트레스를 제한하는 것은 합리적으로 보이지만, 반면 잔여 관절낭 단축은 생리적 견관절두 이동을 변화시키므로 피해야 한다.84
Rotator cuff
The physiologic state
The role of the rotator cuff is to work in conjunction with the deltoid to balance the force couples around the glenohumeral joint. In the horizontal plane, the cross-sectional area and force couples between the anterior (subscapularis) and posterior (infraspinatus and teres minor) rotator cuff are balanced.85 The forces generated by the subscapularis, the supraspinatus, the infraspinatus and the teres minor are 53%, 14%, 22% and 10% respectively.85 The subscapularis seems to be a key muscle for anterior forward flexion,86 while the infraspinatus prevents superior and anterior translation of the humeral head.87
The rotator cable, first described by Burkhart88 as a thick bundle of fibres perpendicular to the supraspinatus, is of major biomechanical importance (Fig. 4).89 It is mandatory to have a good understanding of the anatomy surrounding the rotator cable as well as the close relationship between the insertion of the supraspinatus and infraspinatus tendons as well as the coracohumeral ligament. The rotator cable outlines the rotator crescent which is a relative avascular lateral portion of the supra and infraspinatus tendons. The anterior cable inserts in close relation to the coracohumeral ligament into the anterior greater tuberosity and upper lesser tuberosity, representing fibres of the anterior supraspinatus. The posterior cable insertion will be located at the junction between the infraspinatus and teres minor.89,90 Thus, a tear involving all of the infraspinatus disrupts the posterior cable while disruption of the anterior cable requires a tear involving the upper half of the subscapularis tendon. The function of the cable is frequently compared to that of a suspension bridge which transmits the forces of the cuff through the span to its pillars. This mechanism could explain why function is preserved in tears involving only the rotator crescent (Fig. 4) and why partial cuff repairs with restoration of the pillars can restore good function.89,91
회전근개
생리학적 상태
회전근개의 역할은
삼각근과 함께 어깨 관절 주변의 힘 쌍을 균형 잡는 것이다.
수평면에서는 전방 회전근개(하견갑근)와 후방 회전근개(견갑하근 및 소원근) 사이의 단면적과 힘 쌍이 균형을 이룬다.85 하견갑근, 상견갑근, 견갑하근 및 소원근이 생성하는 힘은 각각 53%, 14%, 22%, 10%를 차지한다.85 견갑하근은 전방 굴곡의 핵심 근육으로 보이며,86 견갑하근은 상완골두의 상방 및 전방 이동을 방지한다.87
회전근개는 버크하트(Burkhart)88에 의해 상근에 수직인 두꺼운 섬유 다발로 처음 기술되었으며, 생체역학적으로 매우 중요하다(그림 4).89 회전근개 주변 해부학 및 상근과 하근 건의 부착부, 그리고 견갑상완 인대 간의 밀접한 관계를 충분히 이해하는 것이 필수적이다. 회전근개는 상근과 하근 건의 상대적으로 혈관이 적은 외측 부분인 회전근개 초승달을 형성한다. 전방 케이블은 견갑상완 인대와 밀접한 관계로 전방 대결절과 상부 소결절에 부착되며, 이는 전방 상근 섬유를 나타낸다. 후부 케이블 부착부는 하견갑근과 소원근 사이의 접합부에 위치한다.89,90 따라서 하견갑근 전체를 포함한 파열은 후부 케이블을 손상시키며, 전부 케이블 손상은 견갑하근 힘줄 상반부의 파열을 필요로 한다. 케이블의 기능은 종종 현수교의 기능과 비교되는데, 이는 회전근개 힘을 스팬을 통해 기둥으로 전달하는 방식이다. 이러한 메커니즘은 회전근개 초승달 모양 구조(그림 4)만 손상된 경우 기능이 유지되는 이유와 기둥을 복원한 부분적 회전근개 수복술이 우수한 기능을 회복시킬 수 있는 이유를 설명해 줄 수 있다.89,91
그림 4.
Fig. 4.
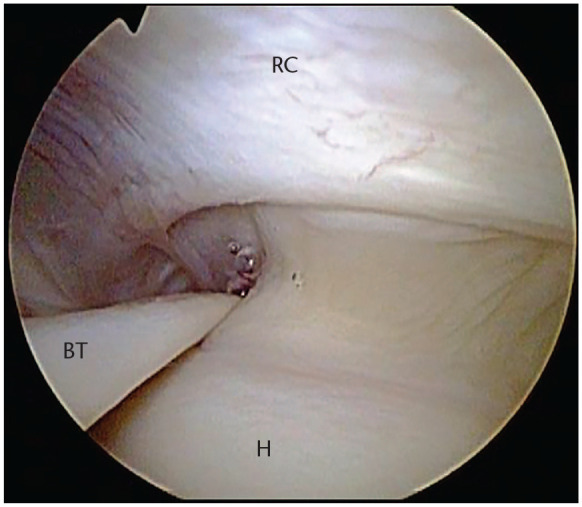
Right shoulder viewed through a posterior portal. Arthroscopic view of crescent configuration of the rotator cuff (RC). The cable surrounds the crescent.
후방 접근법을 통해 관찰한 우측 어깨. 관절경으로 본 회전근개(RC)의 초승달 모양 구조. 케이블이 초승달 모양 구조를 둘러싸고 있다.
참고. BT, 이두근 힘줄; H, 상완골두.
Note. BT, biceps tendon; H, humeral head.
Further, anatomical pseudoparalysis (defined as the inability to actively forward elevate the arm > 90 degrees with complete passive anterior forward elevation) was shown to be the consequence of the disruption of at least one rotator cable attachment, subsequently leading to insufficient equilibrium in the vertical plane and resulting in altered kinematics.92 Bouaicha et al recently introduced the concept of the shoulder abduction index (SAM), which is basically a ratio of the lever arm of the rotator cuff and deltoid as an anatomic predictor to the appearance of pseudoparalysis.93 According to their work, a SAM < 0.77 (odds ratio 11) in the presence of a massive rotator cuff tear is predictive of pseudoparalysis.
또한 해부학적 가성마비(능동적 전방상거 90도 이상 불가능, 완전한 수동적 전방상거 가능)는 최소 한 개의 회전근개 케이블 부착부 단절로 인해 발생하며, 이는 수직면에서의 불충분한 평형 상태를 초래하여 운동역학 변화를 유발하는 것으로 밝혀졌다. 92 Bouaicha 등은 최근 가성마비의 발생을 예측하는 해부학적 지표로 회전근개와 삼각근의 지레 팔 비율을 나타내는 어깨 외전 지수(SAM) 개념을 제시하였다.93 그들의 연구에 따르면, 대규모 회전근개 파열이 존재할 때 SAM < 0.77(오즈비 11)은 가성마비를 예측한다.
Rotator cuff tear repair
It appears preferable to restore the anatomy of the rotator cuff after a tear whenever possible to restore load transmission from tendon to bone. This can, however, be challenging when facing large and retracted tear patterns, particularly chronic tears. A medially non-anatomic reinsertion significantly reduces the compressive glenohumeral joint reaction forces, the glenohumeral stability and the supraspinatus moment arm, especially in abduction.94 Consequently, medialization of the supraspinatus should be limited to 10 mm as it does not seem to limit shoulder range of motion by internal impingement.95,96 Denard et al reported that subscapularis footprint medialization by up to 4 to 7 mm is also functionally acceptable.97
Articular-sided rotator cuff tears are thought to be the equivalent of superior capsular rupture and a physiological adaptation in the throwing athlete allowing enhanced external rotation and anterior humeral translation.98,99 However, biomechanical studies have shown that a partial-thickness tear will lead to altered strain patterns in the remaining cuff and therefore enhance the risk of tear propagation.100,101 A trans-tendon repair of articular-sided partial-thickness rotator cuff tears was shown to reduce glenohumeral contact pressure and contact area during internal impingement but also subacromial contact pressure.102 The latter assumes that the repair is done without overtensioning.
회전근개 파열 수복술
가능한 경우 파열 후 회전근개 해부학적 구조를 복원하여 힘줄에서 뼈로의 하중 전달을 회복하는 것이 바람직해 보인다. 그러나 특히 만성 파열과 같이 크고 후퇴된 파열 패턴을 마주할 때는 어려울 수 있다. 내측 비해부학적 재접합은 견관절 압박 반응력, 견관절 안정성 및 상근의 모멘트 암(특히 외전 시)을 현저히 감소시킨다.94 따라서, 상근의 내측 이동은 내부 충돌로 인한 어깨 가동 범위를 제한하지 않는 것으로 보이기 때문에 10mm로 제한해야 한다.95,96 Denard 등은 견갑하근의 발자국을 최대 4~7mm까지 내측으로 이동시키는 것도 기능적으로 허용 가능하다고 보고했다.97
관절측 회전근개 파열은 상부 관절낭 파열과 동등한 것으로 간주되며, 투구 운동선수의 생리적 적응으로 외부 회전 및 상완골 전방 이동을 향상시키는 것으로 여겨진다.98,99 그러나 생체역학적 연구에 따르면 부분 두께 파열은 잔여 회전근개에 변형된 변형 패턴을 초래하여 파열 진행 위험을 증가시킨다. 100,101 관절측 부분 두께 회전근개 파열에 대한 건을 가로지르는 봉합술은 내측 충돌 시 견관절 접촉 압력과 접촉 면적을 감소시킬 뿐만 아니라 견봉하 접촉 압력도 감소시키는 것으로 나타났다.102 후자의 경우 봉합 시 과도한 장력을 가하지 않았다는 전제 하에 성립한다.
The coracoacromial arch
Another important point is that contact between the rotator cuff and the coracoacromial arch is not per definition a pathologic state and can be seen under physiologic conditions.103 While acromion shape has been the source of extensive research, an increased critical shoulder angle (38 degrees) has been pointed out as a source of increased load to the supraspinatus tendon at lower degrees of abduction.104 This led to the suggestion to perform a lateral acromioplasty instead of anterior subacromial decompression as an adjunct to rotator cuff repair.105 This further has the advantage of preserving the acromial insertion of the coracoacromial ligament which, when resected, allows anterosuperior humeral head translation.106
견봉쇄골궁
또 다른 중요한 점은 회전근개와 견봉쇄골궁 사이의 접촉이 반드시 병리적 상태를 의미하지 않으며 생리적 조건에서도 관찰될 수 있다는 것이다.103 견봉 형태에 대한 광범위한 연구가 진행되어 왔지만, 증가된 임계 어깨 각도(38도)가 낮은 외전 각도에서 상근건에 가해지는 부하 증가의 원인으로 지적되었다. 104 이에 따라 회전근개 수복술 보조술로 전방 견봉하 감압술 대신 외측 견봉 성형술을 시행할 것을 제안하게 되었다.105 이는 견봉쇄골 인대의 견봉 부착부를 보존하는 추가적인 이점을 제공하는데, 이 인대가 절제될 경우 상완골두의 전상방 이동이 가능해진다.106

Surgical possibilities in case of irreparable rotator cuff lesions
When facing impaired shoulder function in the presence of an irreparable postero-superior cuff tear, several surgical options have been proposed. Tendon transfers, commonly using the latissimus dorsi and more recently the lower trapezius can both significantly enhance shoulder function. While the main goal of the tendon transfer is to restore external rotation, recent biomechanical data favours the use of lower trapezius tendon transfer to the infraspinatus insertion because of both stronger abduction and external rotation moment arms.107 The development of arthroscopic surgery led to an increased awareness and subsequently better understanding of the superior capsule, which is closely related to the undersurface of the supraspinatus and infraspinatus tendons and resists superior migration of the humeral head.108 Subsequent research showed that a double-layer repair with inherent approximation of the superior capsule leads to improved biomechanical properties of the construct.109 In the setting of an irreparable cuff, superior capsular reconstruction (SCR) using either an autograft (tensor fascia lata),110 a dermal allograft111 or the long head of the biceps112 recreates a passive restraint to superior and anteroinferior translation.113 Therefore, adding a static stabilization like the SCR to a dynamic stabilizer like a tendon transfer may ultimately enhance articular stability at the low to mid ranges of abduction.114 Finally, SCR is a promising procedure that remains, however, relatively new and is subject to further research regarding optimal graft choice and surgical technique to avoid excessive strain on the construct during activities of daily living.115,116
The last proposed solution trying to restore glenohumeral contact pressures is the implantation of a balloon spacer in the subacromial space. In a recent cadaveric study, this procedure was shown to efficiently lower the humeral head, increase deltoid load and normalize articular contact pressure at most abduction angles.117 While the use of a biodegradable balloon may be questionable regarding long-term outcomes in the setting of an irreparable tear, it could on the other hand be a suitable adjunct to rotator cuff repair by reducing peak pressure and wear on the repair, potentially avoiding a re-tear.118
An irreparable isolated subscapularis tear implies not solely a tendon failure, but also rupture of the underlying anterior capsule and ligaments, leading to subsequent altered shoulder kinematics. The biomechanical specificity being that both a dynamic and static stabilizing force is impaired, consequently increasing anterior and inferior humeral head translation.119 Treatment options include tendon transfer of the pectoralis major or latissimus dorsi tendon and/or anterior capsule reconstruction.120 An in vitro study by Konrad et al reported increased restoration of humeral head translation when the pectoralis tendon was transferred behind the conjoint tendon, allowing better restoration of the line of action of the subscapularis tendon.121 This led to further anatomic studies favouring an anterior transfer of the latissimus dorsi tendon.122 A variety of options have been proposed for anterior capsule reconstruction including autografts (tensor fascia lata, hamstrings), tendon allograft, or human dermal allograft.123 A recent cadaveric study by Komperda et al revealed that anterior capsular reconstruction was superior to pectoralis major tendon transfer to restore anterior and inferior humeral head translation.123 Further, the addition of an anterior latissimus dorsi tendon transfer to an anterior capsular reconstruction did not enhance antero-inferior humeral head stability.119
회전근개 손상이 수복 불가능한 경우의 수술적 가능성
수복 불가능한 후상부 회전근개 파열이 존재하는 상태에서 어깨 기능이 저하된 경우, 여러 수술적 옵션이 제안되어 왔다. 일반적으로 광배근을 사용하고 최근에는 하부 승모근을 사용하는 힘줄 이식은 모두 어깨 기능을 크게 향상시킬 수 있다. 건 이식의 주요 목표는 외회전 기능 회복이지만, 최근 생체역학적 연구 결과는 견갑하근 건을 견갑하근 부착부로 이식하는 방법이 외전 및 외회전 모멘트 암이 더 강력하다는 점에서 우월함을 보여준다.107 관절경 수술의 발전은 상부 관절낭에 대한 인식 제고와 이해 심화로 이어졌으며, 이는 상근과 하근 건의 하단면과 밀접하게 연관되어 있으며 상완골두의 상방 이동을 저항합니다.108 후속 연구에 따르면 상부 관절낭의 자연스러운 근접화를 동반한 이중층 수복술이 구조물의 생체역학적 특성을 개선하는 것으로 나타났습니다.109 수복 불가능한 회전근개 상황에서 자가이식편(대퇴근막장근), 110 피부 동종 이식편111 또는 이두근 장두112를 이용한 상부 관절낭 재건술(SCR)은 상방 및 전하방 이동에 대한 수동적 제한 기능을 재현한다.113 따라서 건 이식과 같은 동적 안정 장치에 SCR과 같은 정적 안정화 장치를 추가하면, 외전 운동의 하위에서 중간 범위에서 관절 안정성을 궁극적으로 향상시킬 수 있다.114 마지막으로, SCR은 유망한 시술이지만, 여전히 비교적 새로운 방법이며 일상생활 활동 중 구조물에 가해지는 과도한 긴장을 피하기 위한 최적의 이식편 선택과 수술 기법에 대한 추가 연구가 필요합니다.115,116
견관절 접촉 압력을 회복시키려는 마지막으로 제안된 해결책은 견봉하 공간에 풍선형 간극 유지 장치를 이식하는 것입니다. 최근 시체 연구에서, 이 시술은 대부분의 외전 각도에서 상완골두를 효과적으로 하강시키고, 삼각근 부하를 증가시키며, 관절 접촉 압력을 정상화시키는 것으로 나타났다.117 생분해성 풍선의 사용은 회복 불가능한 파열 상황에서 장기적 결과에 대해 의문이 제기될 수 있지만, 반면에 봉합 부위의 최대 압력과 마모를 감소시켜 재파열을 방지할 수 있다는 점에서 회전근개 봉합술에 적합한 보조 수단이 될 수 있다.118
수복 불가능한 단독 하부 견갑하근 파열은 단순히 건 손상뿐만 아니라 그 아래 전방 관절낭 및 인대의 파열을 의미하며, 이는 이후 어깨 운동역학 변화를 초래한다. 생체역학적 특이성은 동적 및 정적 안정화 힘이 모두 손상되어 결과적으로 상완골두의 전방 및 하방 이동이 증가한다는 점이다.119 치료 옵션에는 대흉근 또는 광배근 건 이식 및/또는 전방 관절낭 재건술이 포함된다. 120 Konrad 등의 체외 연구에 따르면, 대흉근 건을 공동건 뒤쪽으로 이식할 경우 견두하근 건의 작용선을 더 잘 복원할 수 있어 상완골두 전위 회복이 증가한다고 보고되었다.121 이로 인해 광배근 건의 전방 이식을 선호하는 추가 해부학적 연구가 진행되었다.122 전방 관절낭 재건에는 자가 이식편( (대퇴근막장근, 햄스트링), 동종건 이식편 또는 인간 피부 동종 이식편 등이 제안되었다.123 Komperda 등의 최근 시체 연구에 따르면, 상완골두의 전방 및 하방 이동을 회복시키는 데 있어 대흉근 건 이식보다 전방 관절낭 재건술이 더 우수했다.123 또한, 전방 관절낭 재건술에 광배근 전방 건 이식을 추가해도 상완골두의 전하방 안정성은 향상되지 않았다.119
Rehabilitation
The primary goal of cuff repair is to be as anatomic as possible and to create a biomechanically favourable environment for tendon healing. Rehabilitation protocols must logically be adapted to the strength of the repair and tissue quality. Basic science research has mainly focused on the effect of mechanical loading on tendon-to-bone repair during the acute phase of healing using rat models.124 While some authors reported improved tendon-to-bone healing with immobilization,124,125 others have found that limited early (during the first six weeks after a repair) tensile load is beneficial for viscoelastic tendon properties.126,127 However, uncontrolled tensile load (as seen with open chain exercises, eccentric muscle activation and motion beyond repair elasticity), leads to impaired tissue healing and can predispose to re-tear or repair tissue elongation.128–130 Excessive compressive loads, typically increased by postoperative scapular protraction,131 do further impair tissue healing.124,132 Lastly, Sonnabend et al, in a primate model, reported that while eight weeks after cuff repair the tissue appeared macroscopically healed, mature healing with Sharpey fibres started at 12 weeks, therefore supporting a 12–15 week rehabilitation programme.133 Further studies are needed to provide guidelines for rehabilitation based on tear size and type of repair.
재활
회전근개 봉합술의 주요 목표는 가능한 한 해부학적 구조를 유지하고 건 치유에 유리한 생체역학적 환경을 조성하는 것이다. 재활 프로토콜은 봉합 강도와 조직 품질에 논리적으로 맞춰 조정되어야 한다. 기초과학 연구는 주로 쥐 모델을 이용한 치유 급성기 동안 힘줄-뼈 접합에 대한 기계적 부하의 영향을 중점적으로 다루어 왔다.124 일부 저자들은 고정으로 힘줄-뼈 치유가 개선된다고 보고한 반면,124,125 다른 연구자들은 제한된 초기(수복 후 첫 6주 동안) 인장 부하가 점탄성 힘줄 특성에 유익하다는 것을 발견했다.126,127 그러나 통제되지 않은 인장 하중(개방 사슬 운동, 이심성 근육 활성화, 수복 탄성 한계를 초과하는 운동 등에서 관찰됨)은 조직 치유를 저해하고 재파열 또는 수복 조직 신장의 위험을 증가시킬 수 있다.128–130 과도한 압축 하중(일반적으로 수술 후 견갑골 전방 이동으로 증가함)131 역시 조직 치유를 더욱 저해한다.124,132 마지막으로, Sonnabend 등은 영장류 모델 연구에서 회전근개 수복술 8주 후 조직이 육안적으로 치유된 것처럼 보였으나, 샤피 섬유를 동반한 성숙한 치유는 12주부터 시작됨을 보고하여 12–15주 재활 프로그램의 필요성을 지지하였다.133 파열 크기 및 수복 유형에 기반한 재활 지침을 마련하기 위해서는 추가 연구가 필요하다.
Conclusions
The shoulder is a complex biomechanical entity with close relationships between anatomical structures and the biomechanical consequences of the different pathologies encountered. Soft tissue stabilizers, bone morphology and dynamic stabilizers such as the rotator cuff and long head of the biceps tendon all interact to ensure shoulder stability. Balanced glenohumeral and scapular force couples are mandatory to preserve or restore shoulder function. Further, a thorough knowledge of the anatomy and biomechanical properties of the rotator cuff, underlying joint capsule, rotator cable and coracoacromial arch is essential when performing a rotator cuff repair. The huge potential of the human body to cope and adapt to the different pathologies can make it sometimes challenging to differentiate between an anatomical or pathological variant. The wide range of pathologies encountered as well as the even higher number of proposed anatomic and non-anatomic surgical solutions make it a very interesting subject for further research. The understanding of the discussed biomechanical principles should therefore be of great help to the surgeon treating these pathologies.
결론
어깨는 해부학적 구조와 다양한 병리학적 상태의 생체역학적 결과 사이에 밀접한 관계가 있는 복잡한 생체역학적 실체이다. 회전근개와 이두근 장두 건과 같은 연부 조직 안정화 장치, 뼈 형태 및 동적 안정화 장치가 상호작용하여 어깨 안정성을 보장한다. 견관절과 견갑골의 균형 잡힌 힘 쌍은 어깨 기능을 보존하거나 회복하는 데 필수적이다. 또한 회전근개 수복술을 시행할 때는 회전근개, 그 아래 관절낭, 회전근개 인대, 견봉쇄골궁의 해부학적 구조와 생체역학적 특성에 대한 철저한 이해가 중요하다. 인체가 다양한 병리에 대처하고 적응하는 엄청난 잠재력 때문에 해부학적 변이와 병리학적 변이를 구분하기가 때로는 어려울 수 있다. 다양한 병리학적 사례와 그보다 더 많은 수의 해부학적 및 비해부학적 수술적 해결책 제안은 이 주제를 향후 연구에 매우 흥미로운 대상으로 만듭니다. 따라서 논의된 생체역학적 원리의 이해는 이러한 병리를 치료하는 외과의에게 큰 도움이 될 것입니다.
Footnotes
ICMJE Conflict of interest statement: PJD reports support for travel to meetings for the study or other purposes from Southern Oregon Orthopedics, related to the submitted work; and consultancy for, grants/grants pending, patents (planned, pending or issued) and royalties from Arthrex Inc., and payment for lectures including service on speakers’ bureaus from Pacira, all outside the submitted work.
PC reports consultant fees from Wright, Arthrex, Smith and Nephew and Conmed and receipt of royalties from Wright.
PH reports Board membership of the Foundation for Osreoarticular Research and employment by EFORT Open Reviews, outside the submitted work.
AL is a paid consultant for Wright, Arthrex and Medacta, and receives royalties from Wright.
The other authors declare no conflict of interest relevant to this work.
OA licence text: This article is distributed under the terms of the Creative Commons Attribution-Non Commercial 4.0 International (CC BY-NC 4.0) licence (https://creativecommons.org/licenses/by-nc/4.0/) which permits non-commercial use, reproduction and distribution of the work without further permission provided the original work is attributed.
Funding statement
The author or one or more of the authors have received or will receive benefits for personal or professional use from a commercial party related directly or indirectly to the subject of this article.
References
- 1. Burkhart SS, Lo IK. Arthroscopic rotator cuff repair. J Am Acad Orthop Surg 2006;14:333–346. [DOI] [PubMed] [Google Scholar]
- 2. Vidt ME, Santago AC, II, Marsh AP, et al. Modeling a rotator cuff tear: individualized shoulder muscle forces influence glenohumeral joint contact force predictions. Clin Biomech (Bristol, Avon) 2018;60:20–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Williamson P, Mohamadi A, Ramappa AJ, DeAngelis JP, Nazarian A. Shoulder biomechanics of RC repair and instability: a systematic review of cadaveric methodology. J Biomech 2019;82:280–290. [DOI] [PubMed] [Google Scholar]
- 4. Saul KR, Hu X, Goehler CM, et al. Benchmarking of dynamic simulation predictions in two software platforms using an upper limb musculoskeletal model. Comput Methods Biomech Biomed Engin 2015;18:1445–1458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Nikooyan AA, Veeger HE, Westerhoff P, Graichen F, Bergmann G, van der Helm FC. Validation of the Delft Shoulder and Elbow Model using in-vivo glenohumeral joint contact forces. J Biomech 2010;43:3007–3014. [DOI] [PubMed] [Google Scholar]
- 6. Broca A, Hartmann H. Contribution à l’étude des luxations de l’épaule (luxations anciennes et luxations récidivantes). Bull Soc Anat 1890;4:416–423. [Google Scholar]
- 7. Warner JJ, Deng XH, Warren RF, Torzilli PA. Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675–685. [DOI] [PubMed] [Google Scholar]
- 8. Pouliart N, Gagey O. Simulated humeral avulsion of the glenohumeral ligaments: a new instability model. J Shoulder Elbow Surg 2006;15:728–735. [DOI] [PubMed] [Google Scholar]
- 9. Bigliani LU, Pollock RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC. Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187–197. [DOI] [PubMed] [Google Scholar]
- 10. Bey MJ, Hunter SA, Kilambi N, Butler DL, Lindenfeld TN. Structural and mechanical properties of the glenohumeral joint posterior capsule. J Shoulder Elbow Surg 2005;14:201–206. [DOI] [PubMed] [Google Scholar]