구조석회화 발생 비율설명
| 극상근 힘줄 (Supraspinatus tendon) | 63% | 가장 흔한 위치. 단독 또는 다른 힘줄과 동반. |
| 견봉하 점액낭 (Subacromial bursa) | 7% (견갑하근과 동반) | 견갑하근 힘줄과 함께 발생한 경우로, 단독 비율은 명시되지 않음. |
| 견갑하근 힘줄 (Infraspinatus tendon) | 7% (견봉하 점액낭과 동반) | 견봉하 점액낭과 함께 발생한 경우로, 단독 비율은 명시되지 않음. |

Clin Shoulder Elb
. 2020 Nov 27;23(4):210–216. doi: 10.5397/cise.2020.00318
Diagnosis and treatment of calcific tendinitis of the shoulder
Min-Su Kim 1, In-Woo Kim 1, Sanghyeon Lee 1, Sang-Jin Shin 1,✉
- Author information
- Article notes
- Copyright and License information
PMCID: PMC7726362 PMID: 33330261
Abstract
Calcific tendinitis is the leading cause of shoulder pain. Among patients with calcific tendinitis, 2.7%–20% are asymptomatic, and 35%–45% of patients whose calcific deposits are inadvertently discovered develop shoulder pain. If symptoms are present, complications such as decreased range of motion of the shoulder joint should be minimized while managing pain. Patients with acute calcific tendinitis respond well to conservative treatment and rarely require surgery. In contrast, patients with chronic calcific tendinitis often do not respond to conservative treatment and do require surgery. Clinical improvement takes time, even after surgical treatment. This review article summarizes the processes related to the diagnosis and treatment of calcific tendinitis with the aim of helping clinicians choose appropriate treatment options for their patients.
초록
석회화 건염은
어깨 통증의 주요 원인이다.
석회화 건염 환자 중 2.7%–20%는 무증상이며,
우연히 발견된 석회화 침착이 있는 환자의 35%–45%에서 어깨 통증이 발생한다.
증상이 있는 경우,
통증 관리와 함께 어깨 관절 가동 범위 감소와 같은 합병증을 최소화해야 한다.
급성 석회화 건염 환자는
보존적 치료에 잘 반응하며 수술이 필요한 경우는 드물다.
반면 만성 석회화 건염 환자는
보존적 치료에 반응하지 않는 경우가 많으며 수술이 필요하다. 수
술 후에도 임상적 호전에는 시간이 소요된다.
본 총설은 임상가가 환자에게 적합한 치료 옵션을 선택하는 데 도움을 주기 위해
석회화 건염의 진단 및 치료와 관련된 과정을 요약한다.
Keywords: Calcification, Tendinitis, Shoulder joint, Conservative treatment, Surgical treatment
INTRODUCTION
Calcific tendinitis of the shoulder, classified as enthesopathy, is a self-limiting disease characterized by the deposition of calcium phosphate crystals in the rotator cuff tendons. It most commonly occurs between the ages of 30 and 50 and is rare in those older than 70 years. It is approximately twice as likely to occur in women as in men, is more common in the right shoulder than in the left, and involves both shoulders in 10% of patients [1]. The most common site of occurrence is 1.5–2 cm away from the supraspinatus tendon insertion site on the greater tuberosity. According to the literature, calcific tendinitis occurs more frequently in some tendons than in others, occurring most often in the supraspinatus tendon. A previous study reported that 63% of cases occur in the supraspinatus tendon, 20% in both the supraspinatus and subscapularis tendons, 7% in both the infraspinatus tendon and subacromial bursa, and 3% in the subscapularis tendon [2].
Diabetes and gout are considered to be risk factors for calcific tendinitis; however, that possibility has not been fully elucidated. Many patients with calcific tendinitis also have endocrine diseases, and conservative treatment is likely to fail in such cases. In addition, stiffness of the shoulder joint, such as frozen shoulder, can occur as a result of chronic shoulder pain. A rotator cuff tear is also present in approximately 25% of patients with calcific tendinitis, though such tears tend to be more associated with small calcific deposits than with large calcific deposits [3]. The management of calcific tendinitis varies, and whether a patient has pain is an important factor. Treatment options include conservative treatment and surgical intervention, and both options are effective when carried out in the appropriate conditions. This article is intended to help clinicians choose the appropriate treatment options for patients with calcific tendinitis.
서론
어깨 석회화 건염은
인대병증으로 분류되며,
회전근개 건에 인산칼슘 결정이 침착되는 것이 특징인 자가 제한성 질환이다.
주로 30~50세 사이에 발생하며
70세 이상에서는 드물다.
여성에서 남성보다 약 2배 더 흔하며,
왼쪽보다 오른쪽 어깨에서 더 자주 발생하고,
환자의 10%에서 양측 어깨에 동시에 발생한다[1].
가장 흔한 발생 부위는
상완골 대결절의 상완골두근 건 부착부에서 1.5~2cm 떨어진 곳이다.
문헌에 따르면,
석회화 건염은 특정 건에서 더 빈번하게 발생하며,
가장 흔히 상근건에서 나타난다.
이전 연구에 따르면,
63%의 사례가 극상근건에서,
20%는 상근건과 견갑하근 건 모두에서,
7%는 하근건과 견봉하낭 모두에서,
견갑하근 건에서 3%로 보고되었다 [2].
당뇨병과 통풍은 석회화 건염의 위험 요인으로 간주되나, 그 가능성은 완전히 규명되지 않았다. 석회화 건염 환자의 상당수는 내분비 질환을 동반하며, 이러한 경우 보존적 치료는 실패할 가능성이 높다. 또한 동결견과 같은 견관절 강직이 만성 어깨 통증의 결과로 발생할 수 있다. 회전근개 파열도 석회화 건염 환자의 약 25%에서 동반되나, 이러한 파열은 큰 석회 침착물보다는 작은 석회 침착물과 더 관련이 있는 경향이 있다[3]. 석회화 건염의 치료 방법은 다양하며, 환자에게 통증이 있는지 여부가 중요한 요소이다. 치료 옵션에는 보존적 치료와 수술적 개입이 포함되며, 적절한 조건에서 시행될 경우 두 옵션 모두 효과적입니다. 본 문서는 임상가가 석회화 건염 환자에게 적합한 치료 옵션을 선택하는 데 도움을 주기 위해 작성되었습니다.
ETIOLOGY
The etiology of calcific tendinitis of the shoulder remains controversial between two theories: degenerative calcification and reactive calcification. The theory of degenerative calcification was proposed by Codman and Akerson [4] in 1931. It posits that degenerative changes of the tendon accumulate with age, leading to decreased distribution of blood vessels and reduced local oxygenation of the tissue, which in turn produces hypoxia, thinning and tearing of the tendon, necrosis, and eventually calcification. However, that theory cannot explain why calcific tendinitis has a peak incidence in patients aged 50 years or why it is a self-limiting disease. In 1997, Uhthoff and Loehr [5] proposed the theory of reactive calcification, a series of processes that occur in precalcific, calcific, and postcalcific stages. Among them, the calcific stage consists of formative, resting, and resorptive phases. In the precalcific stage, tenocytes change into chondrocytes, a process called metaplasia, and fibrocartilaginous transformation occurs within the tendon. In the formative phase of the calcific stage, calcium deposits form and increase in size. Calcium deposition then stops at the resting phase of the calcific stage. During the resorptive phase of the calcific stage, calcific deposits are absorbed by cell-mediated phagocytosis, which is performed by cells such as macrophages and giant cells. Acute pain is mainly present in this phase. In the postcalcific stage, the spaces remaining in the tissue where calcium deposits were absorbed is replaced by granular tissue, and remodeling occurs. Calcific tendinitis eventually progresses to bursitis and inflammatory synovitis caused by chemical irritation due to the calcific deposits. Chemical furuncles are formed by swelling and increased local pressure in the tissue. Thickening of the bursa causes collisions in the subacromial space. All of these processes produce various forms of shoulder pain.
병인
어깨 석회화 건염의 병인은 퇴행성 석회화와 반응성 석회화라는 두 이론 사이에서 여전히 논란의 여지가 있습니다. 퇴행성 석회화 이론은 1931년 Codman과 Akerson[4]에 의해 제안되었다. 이 이론은 건의 퇴행성 변화가 연령과 함께 축적되어 혈관 분포 감소와 조직의 국소 산소 공급 저하를 초래하며, 이는 다시 저산소증, 건의 얇아짐과 파열, 괴사, 그리고 결국 석회화를 유발한다고 주장한다. 그러나 이 이론은 석회화 건염의 발생률이 50세 환자에서 최고조에 달하는 이유나 자가 제한성 질환인 이유를 설명하지 못한다. 1997년 Uhthoff와 Loehr[5]는 반응성 석회화 이론을 제안했는데, 이는 석회화 전 단계, 석회화 단계, 석회화 후 단계에서 발생하는 일련의 과정이다. 이 중 석회화 단계는 형성기, 휴지기, 흡수기로 구성됩니다. 석회화 전 단계에서는 건세포가 연골세포로 변하는 대체증식 과정이 일어나며, 건 내부에서 섬유연골 변형이 발생합니다. 석회화 단계의 형성기에는 칼슘 침착물이 형성되고 크기가 증가합니다. 이후 석회화 단계의 휴지기에서 칼슘 침착이 중단됩니다. 석회화 단계의 흡수 단계에서는 석회화 침착물이 대식세포 및 거대세포와 같은 세포에 의한 세포매개성 식작용을 통해 흡수된다. 급성 통증은 주로 이 단계에서 발생한다. 석회화 후 단계에서는 석회화 침착물이 흡수된 조직 내 잔여 공간이 과립 조직으로 대체되며 재형성이 일어난다. 석회화 건염은 결국 석회화 침착물에 의한 화학적 자극으로 인한 활액낭염 및 염증성 활막염으로 진행됩니다. 조직의 부종과 국소 압력 증가로 화학적 농양이 형성됩니다. 활액낭의 두꺼워짐은 견봉하 공간에서 충돌을 유발합니다. 이러한 모든 과정은 다양한 형태의 어깨 통증을 유발합니다.
CLASSIFICATIONS
Calcific tendinitis is classified as acute (within 2 weeks), subacute (3 to 8 weeks), and chronic (more than 3 weeks), according to the duration of clinical symptoms [1]. Depending on the degree of invasion, calcium deposits are classified as localized or diffused. The diffused form is usually more painful and persists for a longer time than the localized form. Idiopathic calcific tendinitis, type I, is not accompanied by endocrine disease, whereas secondary calcific tendinitis, type II, is accompanied by endocrine diseases such as diabetes. Patients with secondary calcific tendinitis often do not respond to conservative treatment, and they require surgical treatment more commonly than patients with idiopathic calcific tendinitis. Bosworth [6] classified calcific tendinitis based on the size of calcium deposits, with small deposits being less than 0.5 cm, medium deposits being 0.5–1.5 cm, and large deposits being >1.5 cm.
Neer [7] classified four types of calcific tendinitis based on pain and calcium deposits. Their first type is characterized by pain caused by chemical irritation as a result of the calcium deposits. The second type involves pain caused by increased local pressure within the tissue as it swells. The third type causes impingement-like pain through bursal thickening and irritation by prominent calcium deposits. The fourth type reflects pain caused by chronic stiffness of the glenohumeral joint, such as frozen shoulder.
Many classifications have been attempted based on the morphology of the calcific deposits as observed in simple radiography. In 1961, DePalma and Kruper [1] classified two types of calcium deposits on radiography. Type 1 has a fluffy shape with an ill-defined margin and mainly appears in the resorptive phase of the calcific stage, in which patients complain of acute pain. This disease state is acute calcific tendinitis. Type 2 has homogenously dense calcium deposits with a well-defined margin, and most patients with this type have little or no pain. These deposits appear in the formative or resting phase of the calcific stage, and they reflect subacute or chronic calcific tendinitis.
The French Arthroscopic Society classification divides calcific tendinitis into four types based on the morphology of calcium deposits on radiology [8]. Type A calcium deposits show dense, homogenous, and sharp contours; type B deposits show dense, segmented, and sharp contours; type C shows heterogeneous and soft contours; and type D shows dystrophic calcification at the insertion of the rotator cuff tendon. Loew et al. [9] classified three types of calcific tendinitis based on the pattern of calcium deposits observed on magnetic resonance imaging (MRI). Type A appears as a dense, uniform, and well-defined single deposit; type B is uniform and well-defined with two or more deposits; and type C appears as heterogeneous, widely spread, and ill-defined deposits.
분류
석회화 건염은 임상 증상 지속 기간에 따라 급성(2주 이내), 아급성(3~8주), 만성(3주 초과)으로 분류된다[1]. 침윤 정도에 따라 석회 침착은 국소형 또는 확산형으로 구분된다. 확산형은 국소형보다 통증이 더 심하고 지속 기간이 더 긴 경향이 있습니다. 제1형 특발성 석회화 건염은 내분비 질환을 동반하지 않는 반면, 제2형 이차성 석회화 건염은 당뇨병과 같은 내분비 질환을 동반합니다. 이차성 석회화 건염 환자는 보존적 치료에 반응하지 않는 경우가 많으며, 특발성 석회화 건염 환자보다 수술적 치료가 더 흔히 필요합니다. Bosworth [6]는 석회 침착물의 크기에 따라 석회화 건염을 분류했는데, 소형 침착물은 0.5cm 미만, 중형 침착물은 0.5–1.5cm, 대형 침착물은 1.5cm 이상이다.
Neer [7]는 통증과 석회 침착물을 기준으로 석회화 건염을 네 가지 유형으로 분류했다. 제1형은 석회 침착물로 인한 화학적 자극에 의한 통증이 특징이다. 두 번째 유형은 조직이 부어오르면서 발생하는 국소 압력 증가로 인한 통증을 포함한다. 세 번째 유형은 활액낭 비후와 두드러진 석회 침착물에 의한 자극을 통해 충돌 증후군과 유사한 통증을 유발한다. 네 번째 유형은 동결견과 같은 견관절의 만성적인 경직으로 인한 통증을 반영한다.
단순 방사선 촬영에서 관찰되는 석회화 침착물의 형태에 기반한 다양한 분류가 시도되어 왔다. 1961년 DePalma와 Kruper[1]는 방사선 사진상 석회 침착물을 두 가지 유형으로 분류했다. 제1형은 경계가 불분명한 푹신한 모양을 보이며 주로 환자가 급성 통증을 호소하는 석회화 단계의 흡수기에 나타난다. 이 병태는 급성 석회화 건염이다. 2형은 경계가 뚜렷한 균일하게 조밀한 석회 침착물을 보이며, 이 유형의 대부분의 환자는 통증이 거의 없거나 전혀 없습니다. 이러한 침착물은 석회화 단계의 형성기 또는 휴지기 형태로 나타나며, 아급성 또는 만성 석회화 건염을 반영합니다.
프랑스 관절경 학회 분류는 방사선학적 석회 침착물의 형태에 따라 석회화 건염을 네 가지 유형으로 구분합니다[8]. A형 석회 침착물은 고밀도, 균일성, 선명한 경계를 보이며, B형은 고밀도, 분절성, 선명한 경계를 나타낸다. C형은 이질적이고 부드러운 경계를 보이며, D형은 회전근개 힘줄 부착부에서 영양장애성 석회화를 보인다. Loew 등[9]은 자기공명영상(MRI)에서 관찰된 석회 침착 패턴에 따라 석회성 건염을 세 가지 유형으로 분류하였다. A형은 고밀도, 균일하고 경계가 뚜렷한 단일 침착물로 나타난다. B형은 균일하고 경계가 뚜렷한 두 개 이상의 침착물로 나타난다. C형은 이질적이고 광범위하게 퍼져 있으며 경계가 불분명한 침착물로 나타난다.
CLINICAL EVALUATION
Calcific tendinitis is diagnosed through patient history, physical examination, and imaging examination. Among patients with calcific tendinitis, 2.7%–20% are asymptomatic, and 35%–45% of patients whose calcific deposits are discovered inadvertently on simple radiographs develop symptoms [10,11]. The formative phase generally does not show clinical symptoms and is therefore often found by chance, although chronic intermittent pain is occasionally observed. Chronic pain occurs during shoulder forward flexion. In the resorptive phase, severe acute pain mainly occurs suddenly and worsens at night. Patients experience difficulties in lying on the affected side, and shoulder joint movement becomes limited. Patients consciously maintain a posture with internal rotation of the shoulder to relieve pain, and prior to diagnosis, most patients visit an emergency room due to the sudden onset of symptoms and pain. In addition, calcific tendinitis can be accompanied by local heat, redness, and oppressive pain. Therefore, it needs to be differentiated from septic arthritis, which presents with similar symptoms.
Simple radiographic images of the shoulder anteroposterior view, internal and external rotation views, supraspinatus outlet views, and axillary views should be acquired to determine the location of calcific deposits and predict the possibility of collision symptoms. If follow-up images are acquired, changes in the disease stage can be assessed. In general, the size of the calcific deposits does not change significantly over time, although a previous study reported that 18% of patients experienced an increase in the size of calcific deposits after follow-up for an average of 16 months [12]. According to the classification of Depalma and Kruper [1], radiological findings that show a type 1 pattern, with unclear margins and a fluffy or fleecy appearance, can be judged to be in the resorptive phase in which patients complain of acute pain. On the other hand, if a type 2 pattern with a clear margin and uniform density of calcific deposits is shown, most patients will report little or no pain because they are in the formative or resting phase.
In addition to simple radiographs, ultrasonography can be used to assess calcific deposits. It shows hyperechoic areas and an obvious posterior acoustic shadow in the formative or resting phase. In the resorptive phase, on the other hand, hyperechoic areas are relatively reduced, and the posterior acoustic shadow is also reduced or not observed. MRI is not a routine evaluation; however, it is helpful in identifying lesions in the shoulder joint, including the location of calcific deposits and the condition of the rotator cuff. In T1-weighted images, calcific deposits show a low signal intensity, whereas in T2-weighted images, the edema pattern surrounding the calcific deposits can show a high signal intensity.
Generally, calcific deposits appear to have a fluffy shape on radiography and a toothpaste-like appearance on arthroscopic findings in the resorptive phase of calcific tendinitis, whereas they appear homogeneously dense on radiography and have a chalk-like appearance on arthroscopic findings in the formative or resting phase of calcific tendinitis (Fig. 1).
임상 평가
석회화 건염은 환자 병력, 신체 검사 및 영상 검사를 통해 진단된다. 석회화 건염 환자 중 2.7%~20%는 무증상이며, 단순 방사선 촬영에서 우연히 석회화 침착이 발견된 환자의 35%~45%에서 증상이 발생한다[10,11]. 형성기에는 일반적으로 임상 증상이 나타나지 않아 우연히 발견되는 경우가 많으나, 만성 간헐적 통증이 가끔 관찰된다. 만성 통증은 어깨 전방 굴곡 시 발생한다. 흡수 단계에서는 주로 갑작스럽게 발생하는 심한 급성 통증이 밤에 악화된다. 환자는 환측으로 누워 있기 어렵고, 어깨 관절 운동이 제한된다. 환자는 통증 완화를 위해 의식적으로 어깨 내회전 자세를 유지하며, 진단 전 대부분의 환자는 갑작스러운 증상 발현과 통증으로 응급실을 방문한다. 또한 석회화 건염은 국소적 열감, 발적, 압박성 통증을 동반할 수 있다. 따라서 유사한 증상을 보이는 화농성 관절염과 감별 진단이 필요합니다.
견관절 정면 촬영, 내회전 및 외회전 촬영, 상근하구 촬영, 액와 촬영 등의 단순 방사선 영상을 통해 석회화 침착 부위를 확인하고 충돌 증상 가능성을 예측해야 합니다. 추적 촬영을 시행하면 병기별 변화를 평가할 수 있습니다. 일반적으로 석회화 침착물의 크기는 시간이 지나도 크게 변하지 않지만, 한 연구에서는 평균 16개월간 추적 관찰한 결과 18%의 환자에서 석회화 침착물 크기가 증가한 것으로 보고된 바 있다[12]. Depalma와 Kruper의 분류[1]에 따르면, 경계가 불분명하고 보송보송하거나 양털 같은 모양을 보이는 유형 1 패턴을 보이는 방사선학적 소견은 환자가 급성 통증을 호소하는 흡수 단계에 있다고 판단할 수 있습니다. 반면, 경계가 명확하고 석회화 침착물의 밀도가 균일한 2형 패턴이 관찰될 경우, 대부분의 환자는 형성기 또는 휴지기에 해당하므로 통증이 거의 없거나 전혀 없다고 보고합니다.
단순 방사선 촬영 외에도 초음파 검사를 통해 석회화 침착물을 평가할 수 있습니다. 형성기 또는 휴지기에는 고에코 영역과 뚜렷한 후방 음향 그림자가 관찰됩니다. 반면 흡수기에는 고에코 영역이 상대적으로 감소하고 후방 음향 그림자도 감소하거나 관찰되지 않습니다. MRI는 일상적인 검사는 아니지만, 석회화 침착물의 위치와 회전근개 상태를 포함한 어깨 관절 내 병변 확인에 유용하다. T1 가중 영상에서 석회화 침착물은 낮은 신호 강도를 보이며, T2 가중 영상에서는 석회화 침착물 주변의 부종 패턴이 높은 신호 강도를 나타낼 수 있다.
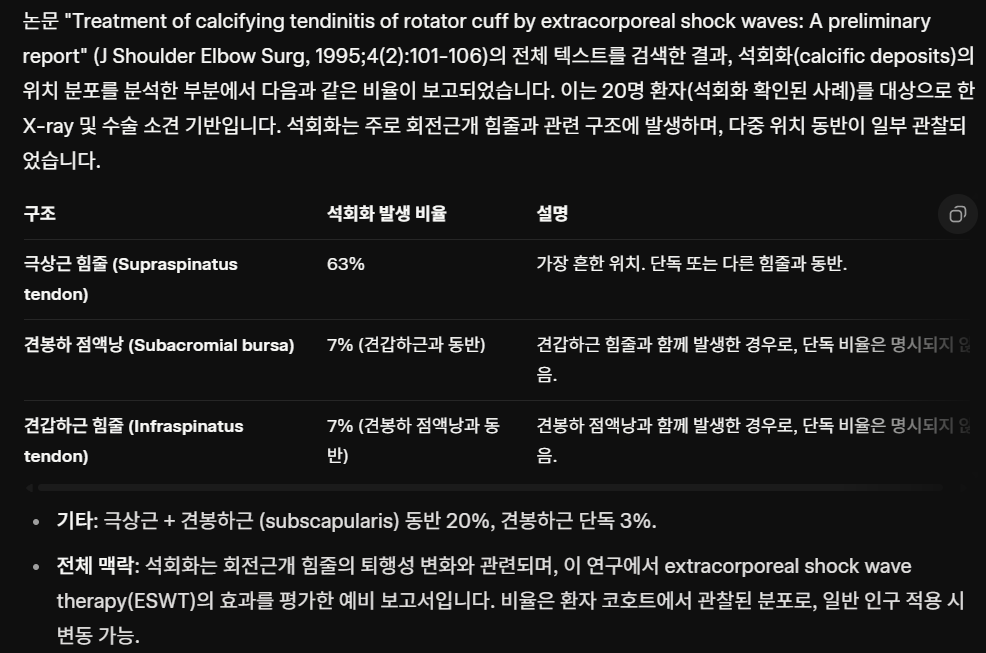
일반적으로 석회화 침착물은 석회화 건염의 흡수 단계에서는 방사선 사진상 푹신한 모양을, 관절경 소견상 치약 같은 모습을 보이는 반면, 석회화 건염의 형성기 또는 휴지기에 방사선 사진상 균일하게 조밀하게 나타나고 관절경 소견상 분필 같은 모습을 보인다(그림 1).
Fig. 1.
Radiographic and arthroscopic findings of resorptive and formative or resting phase of calcific tendinitis. (A) In the resorptive phase of calcific deposits (arrows) appear fluffy-like shape on shoulder anteroposterior (AP) view and (B) toothpaste-like appearance on macroscopic findings observed by arthroscopy. (C) In the formative or resting phase of calcific deposits (arrow) appear homogeneously dense on shoulder AP view and (D) chalk-like appearance on macroscopic findings observed by arthroscopy.
석회화 건염의 흡수기 및 형성기 또는 휴지기 단계의 방사선 및 관절경 소견. (A) 흡수기 단계의 석회화 침착물(화살표)은 어깨 정면(AP) 영상에서 푹신한 모양을 보이고, (B) 관절경으로 관찰된 거시적 소견에서는 치약 같은 모양을 보인다. (C) 형성기 또는 휴지기 단계의 석회 침착물(화살표)은 어깨 AP 영상에서 균일하게 고밀도로 나타나며, (D) 관절경으로 관찰된 거시적 소견에서는 분필 같은 모습을 보인다.
TREATMENTS
Conservative Treatment
The primary treatment for calcific tendinitis is conservative, and it has a success rate of 30% to 80%. Non-steroidal anti-inflammatory analgesics are used to relieve acute pain, and the affected shoulder joint needs to be rested using an arm sling. When there are signs of collision or the patient is in the resorptive phase, subacromial steroid injections are effective in alleviating pain. The ultrasound-guided barbotage technique can relieve pain with decompression effects by aspirating and washing out calcific deposits using an 18-gauge or 22-gauge needle. A 3–5-mL mixed solution of normal saline and lidocaine can be administered to locations with calcific deposits, and the aspiration can be repeated until the deposits are washed away. Afterward, an injection of an additional 1 mL of steroid and 2 mL of lidocaine into the bursa around the calcific deposits can enhance pain relief. A previous study reported that the ultrasound-guided barbotage technique achieved satisfactory results in 70% of patients [13]. It can also be performed under fluoroscopy. When performing the barbotage technique, anesthetics and steroids can be injected into the deposition sites and the subacromial space to enhance the effect of the technique.
A randomized controlled study found that ultrasound therapy improved quality of life and helped relieve pain [14]. The study was conducted at a 0.89 MHz frequency and 2.5 W/cm2 intensity for 15 minutes per session. The first 15 treatments were performed five times per week for a total of 3 weeks. The remaining nine treatments were performed three times per week for a total of 3 weeks. Furthermore, steroidal and nonsteroidal anti-inflammatory analgesic were not administered during the study. Ultrasound therapy show effects similar to those of surgery.
Extracorporeal shock wave therapy (ESWT) is also widely used and is one of the most effective treatments for pain relief. A prospective study showed that high-energy ESWT in chronic calcific tendinitis patients had a high treatment success rate and few side effects, however, 20% of the patients underwent surgical treatment due to treatment failure during 4 years [15].
In another study, surgical treatment was more effective than ESWT for homogeneous calcification; however, in heterogeneous calcification, ESWT and surgical treatment showed similar effects [11]. During the 1-year follow-up after ESWT in that study, calcific deposits were not observed in 47% of patients, were resorbed in 33% of patients, and showed no changes in 20% of patients [11]. Thus, ESWT is a treatment that can be performed before surgical treatment. Other studies have also reported ESWT as a successful treatment [16,17].
In sum, various conservative treatment options (ultrasound-guided barbotage and injection, ultrasound therapy, and ESWT) show effects similar to those with surgical treatment and are noninvasive. Therefore, conservative treatment is recommended before surgical treatment. Patients with acute pain should begin passive exercise of the shoulder joint to restore range of motion (ROM) after managing the pain with conservative therapy for 1 to 2 weeks and continue until they experience pain relief. In most patients with chronic pain, the ROM of the shoulder joint is close to the normal range. Thus, strengthening exercises need to be started within the range that is comfortable for the patient. If stiffness is observed in patients with chronic calcific tendinitis, adhesive capsulitis should be ruled out. Pain should be controlled first, followed by passive ROM exercises and pendulum exercises.
치료법보존적 치료
석회화 건염의 일차적 치료는 보존적이며, 성공률은 30~80%이다. 급성 통증 완화를 위해 비스테로이드성 항염증 진통제를 사용하며, 환측 어깨 관절은 팔 거치대를 사용하여 휴식시켜야 한다. 충돌 증상이 있거나 환자가 흡수기에 있을 경우, 견봉하 스테로이드 주사는 통증 완화에 효과적이다. 초음파 유도 바르보타주 기법은 18게이지 또는 22게이지 바늘을 사용하여 석회화 침착물을 흡인 및 세척함으로써 감압 효과를 통해 통증을 완화할 수 있다. 석회화 침착 부위에 생리식염수와 리도카인을 혼합한 3~5mL 용액을 주입하고, 침착물이 세척될 때까지 흡인 과정을 반복할 수 있습니다. 이후 석회화 침착물 주변 활액낭에 스테로이드 1mL와 리도카인 2mL를 추가 주사하면 통증 완화 효과가 증대됩니다. 선행 연구에 따르면 초음파 유도 바르보타주 기법은 환자의 70%에서 만족스러운 결과를 보였습니다[13]. 이 기법은 형광 투시법 하에서도 시행 가능합니다. 바르보타주 시술 시 침착 부위와 견봉하 공간에 마취제와 스테로이드를 주입하면 시술 효과를 증대시킬 수 있습니다.
무작위 대조 연구에서 초음파 치료가 삶의 질을 개선하고 통증 완화에 도움이 된다는 사실이 확인되었다[14]. 이 연구는 0.89MHz 주파수와 2.5W/cm2 강도로 세션당 15분 동안 시행되었다. 첫 15회 치료는 주당 5회, 총 3주간 진행되었다. 나머지 9회 치료는 주 3회, 총 3주간 시행되었습니다. 또한 연구 기간 동안 스테로이드 및 비스테로이드성 항염증 진통제는 투여되지 않았습니다. 초음파 치료는 수술과 유사한 효과를 보였습니다.
체외 충격파 치료(ESWT) 또한 널리 사용되며 통증 완화에 가장 효과적인 치료법 중 하나입니다. 전향적 연구에 따르면 만성 석회화 건염 환자에게 시행한 고에너지 ESWT는 높은 치료 성공률과 적은 부작용을 보였으나, 4년간 치료 실패로 인해 환자의 20%가 수술적 치료를 받았다[15].
다른 연구에서는 균질 석회화에 대해 수술적 치료가 ESWT보다 효과적이었으나, 이질 석회화에서는 ESWT와 수술적 치료가 유사한 효과를 보였다[11]. 해당 연구에서 ESWT 후 1년간 추적 관찰 결과, 환자의 47%에서 석회화 침착물이 관찰되지 않았고, 33%에서 흡수되었으며, 20%에서는 변화가 없었습니다[11]. 따라서 ESWT는 수술적 치료 전에 시행할 수 있는 치료법입니다. 다른 연구들에서도 ESWT가 성공적인 치료법으로 보고되었습니다[16,17].
요약하면, 다양한 보존적 치료 옵션(초음파 유도 바르보타주 및 주사, 초음파 치료, ESWT)은 수술적 치료와 유사한 효과를 보이며 비침습적이다. 따라서 수술적 치료 전에 보존적 치료를 권장한다. 급성 통증이 있는 환자는 보존적 치료로 통증을 관리한 후 1~2주 이내에 어깨 관절의 수동 운동을 시작하여 가동 범위(ROM)를 회복하고 통증 완화까지 지속해야 한다. 만성 통증 환자의 대부분에서 어깨 관절의 ROM은 정상 범위에 가깝습니다. 따라서 환자가 편안하게 느끼는 범위 내에서 강화 운동을 시작해야 합니다. 만성 석회화 건염 환자에게 경직이 관찰되면 유착성 관절낭염을 배제해야 합니다. 먼저 통증을 조절하고, 이후 수동적 ROM 운동과 진자 운동을 시행해야 합니다.
Surgical Treatment
When conservative treatment does not improve pain, shoulder function can decline, making daily activities difficult to perform. For patients who do not respond to conservative treatment after 6 months, surgery should be considered. One study reported that surgery was performed due to conservative treatment failure in approximately 10% of patients, and it showed the best effects in patients with chronic calcific tendinitis in whom the onset of symptoms was more than a year prior to surgery [18].
In general, acute calcific tendinitis responds well to conservative treatment. However, chronic calcific tendinitis often requires surgical treatment, which can take the form of open surgery or arthroscopic surgery. Both surgical methods remove calcific deposits and have shown satisfactory clinical outcomes. Between them, arthroscopic surgery has the advantages of a short rehabilitation period and cosmetic superiority, and it is a less invasive method that helps protect surrounding tissues and can be used to treat comorbidities such as frozen shoulder and rotator cuff tears. Previous studies have reported no significant differences in the clinical outcomes after complete and incomplete removal of calcific deposits [19]. Other studies reported that patients whose radiographic findings after surgery indicated a removal or reduction of calcific deposits showed better prognoses than those whose calcific deposits remained unchanged [20]. This suggests that it is essential to remove as many calcific deposits as possible while minimizing damage to the rotator cuff. If signs of collision are observed, an acromioplasty procedure is effective.
Whether rotator cuff repair after the removal of calcific deposits affects clinical outcomes remains controversial. In general, patients with rotator cuff repair do not show different clinical results from patients who do not receive such a repair, and further progression of a rotator cuff tear is rarely observed. However, several authors have suggested that rotator cuff repair can facilitate rehabilitation treatment in patients with a combined full-thickness rotator cuff tear [21]. In addition, one study reported that clinical outcomes were satisfactory when using both side-side sutures and suture anchors for rotator cuff tears [22].
수술적 치료
보존적 치료로 통증이 호전되지 않을 경우, 어깨 기능이 저하되어 일상생활 수행이 어려워질 수 있습니다. 6개월간 보존적 치료에 반응하지 않는 환자에게는 수술을 고려해야 합니다. 한 연구에 따르면, 보존적 치료 실패로 인해 약 10%의 환자에게 수술이 시행되었으며, 수술 전 증상 발현이 1년 이상 경과한 만성 석회화 건염 환자에서 가장 우수한 효과를 보였습니다 [18].
일반적으로 급성 석회화 건염은 보존적 치료에 잘 반응합니다. 그러나 만성 석회화 건염은 종종 개방 수술 또는 관절경 수술 형태의 수술적 치료가 필요합니다. 두 수술 방법 모두 석회화 침착물을 제거하며 만족스러운 임상 결과를 보였습니다. 이 중 관절경 수술은 재활 기간이 짧고 미용적 우월성이 있으며, 주변 조직 보호에 도움이 되는 덜 침습적인 방법으로 동결견이나 회전근개 파열과 같은 동반 질환 치료에도 활용될 수 있다. 기존 연구에서는 석회화 침착물의 완전 제거와 불완전 제거 후 임상 결과에 유의미한 차이가 없다고 보고되었다[19]. 다른 연구에서는 수술 후 방사선 소견상 석회화 침착물이 제거되거나 감소한 환자가 침착물이 변화 없는 환자보다 예후가 우수하다고 보고하였다[20]. 이는 회전근개 손상을 최소화하면서 가능한 한 많은 석회화 침착물을 제거하는 것이 중요함을 시사한다. 충돌 증상이 관찰될 경우 견봉 성형술이 효과적이다.
석회화 침착물 제거 후 회전근개 봉합술이 임상 결과에 영향을 미치는지는 여전히 논란의 여지가 있다. 일반적으로 회전근개 봉합술을 시행한 환자는 봉합술을 받지 않은 환자와 임상 결과가 다르지 않으며, 회전근개 파열의 추가 진행은 드물게 관찰된다. 그러나 여러 저자들은 완전층 회전근개 파열이 동반된 환자에서 회전근개 봉합술이 재활 치료를 용이하게 할 수 있다고 제안했다[21]. 또한 한 연구에서는 회전근개 파열에 측면-측면 봉합사와 봉합 앵커를 병용했을 때 임상 결과가 만족스러웠다고 보고하였다[22].
SURGICAL TECHNIQUES
Glenohumeral Joint
A posterior portal is made 2 cm inferior and 1 cm medial to the posterolateral corner of the acromion. After inserting the arthroscope into the joint, an anterior portal is made lateral to the coracoid process and anterior to the acromioclavicular joint. When frozen shoulder is present, arthroscopic capsular release should be performed. Expansion, swelling, or fibrillation of the articular side of a supraspinatus tendon that could have calcific deposits needs to be assessed in detail. If a suspicious area on the joint surface is observed, an 18-gauge spinal needle is passed through the supraspinatus tendon at the lesion site 1 cm outside the acromion and placed behind the long head of the bicep tendon. Polydioxanone (PDS) can then be passed through the needle to the supraspinatus tendon for marking, and the spinal needle can be removed while maintaining the PDS at its location. This helps locate calcific deposits in the subacromial space.
수술 기법
견관절
견봉의 후측외측 모서리에서 2cm 아래, 1cm 안쪽에 후방 포털을 생성한다. 관절경이 관절 내로 삽입된 후, 견봉돌기 외측 및 견쇄관절 전방에 전방 포털을 생성한다. 동결견이 동반된 경우 관절경적 관절낭 이완술을 시행해야 한다. 석회 침착 가능성이 있는 상근 건 관절면의 확장, 부종 또는 섬유화를 상세히 평가해야 한다. 관절면에 의심스러운 부위가 관찰되면, 견봉에서 1cm 바깥쪽 병변 부위의 상근 건을 통해 18게이지 척추 바늘을 통과시켜 이두근 건 장두 뒤쪽에 위치시킨다. 이후 폴리디오잔론(PDS)을 바늘을 통해 상완골두근 힘줄로 통과시켜 표지한 후, PDS를 해당 위치에 유지한 채 척추 바늘을 제거할 수 있다. 이는 견봉하 공간 내 석회화 침착물의 위치를 확인하는 데 도움이 된다.
Subacromial Space
After the appropriate glenohumeral joint exploration, an arthroscope moves into the subacromial space. Arthroscopic treatment of calcific tendinitis is mostly performed in the subacromial space. In general, moderate inflammatory changes, as well as hyperproliferation and thickening of the bursa, can be observed. Afterward, a lateral working portal is made at the anterolateral area of the acromion.
Bursectomy and Decompression
If PDS marking was performed to visualize a lesion in the articular joint, decompression is conducted by thoroughly removing the bursa using a shaver with a suction opening through the lateral working portal. The PDS should not be cut during the bursectomy. If no lesion is visible in the articular joint or if calcific deposits are located on the bursal side, comprehensive bursectomy is performed first. Adequate hemostasis using electrocautery is required to obtain a proper surgical field. Edema and swelling can be seen macroscopically in areas with calcific deposits, which helps to find them.
Calcific Deposit Removal
After identifying the location of calcium deposits, PDS and the needle used for marking are removed. In the acute or resorptive phases, calcific deposits have a toothpaste-like appearance. In the chronic or formative phases, they have a chalk-like appearance. The deposits can be visually identified using an arthroscope (a 16-gauge needle is most often used). When needling is performed in an area with calcific deposits, calcific deposits can be observed as creamy or snowy. If the deposits are large or if there are difficulties removing them, a small incision can be made in the long axis of the tendon using a scalpel. A probe can be used to remove residual calcific deposits in the tendons. It is unnecessary to completely remove the calcific deposits, which could damage the tendon, because the effect of decompression is more important than complete removal of the calcific deposits. After removing the calcific deposits in the tendon, debridement of the surrounding tissue and removal of floating residual calcific deposits is performed using a shaver.
견봉하 공간
적절한 견관절 관절 탐색 후 관절경이 견봉하 공간으로 이동한다. 석회화 건염의 관절경적 치료는 대부분 견봉하 공간에서 시행된다. 일반적으로 중등도의 염증 변화와 함께 활액낭의 과증식 및 비후를 관찰할 수 있다. 이후 견봉의 전외측 부위에 측면 작업 포털을 생성한다.
활액낭 절제 및 감압술
관절 내 병변을 시각화하기 위해 PDS 표지술을 시행한 경우, 측면 작업 포털을 통해 흡입구가 있는 쉐이버를 사용하여 활액낭을 완전히 제거함으로써 감압술을 시행한다. 활액낭 절제 시 PDS를 절단해서는 안 된다. 관절 내에 병변이 보이지 않거나 활액낭 측에 석회화 침착물이 위치한 경우, 먼저 포괄적 활액낭 절제를 시행한다. 적절한 수술 시야 확보를 위해 전기소작기를 이용한 충분한 지혈이 필요하다. 석회화 침착 부위에서는 육안적으로 부종과 팽창이 관찰되어 이를 찾는 데 도움이 된다.
석회화 침착물 제거
석회화 침착물 위치를 확인한 후 PDS와 표지용 바늘을 제거한다. 급성기 또는 흡수기에는 치약 같은 외관을 보이며, 만성기 또는 형성기에는 분필 같은 외관을 보인다. 관절경(대개 16게이지 바늘 사용)을 통해 침착물을 육안으로 확인할 수 있습니다. 석회화 침착 부위에 바늘을 삽입할 때 크림색 또는 눈처럼 하얀 침착물이 관찰됩니다. 침착물이 크거나 제거가 어려운 경우, 메스로 힘줄의 장축 방향에 작은 절개를 가할 수 있습니다. 건 내 잔여 석회화 침착물은 프로브를 이용해 제거할 수 있습니다. 석회화 침착물을 완전히 제거하는 것은 건 손상을 유발할 수 있으므로 불필요하며, 감압 효과는 석회화 침착물의 완전한 제거보다 더 중요합니다. 건 내 석회화 침착물 제거 후, 주변 조직의 데브리드먼트(청소)와 부유하는 잔여 석회화 침착물 제거를 위해 샤버를 사용합니다.
Rotator Cuff Tendon Repair and Acromioplasty
Whether the empty space in the tendon left by removing calcific deposits needs to be repaired is controversial. If the rotator cuff tear is small, repair is not needed. However, if the tear is 2 cm or larger and involves more than 70% of the thickness of the tendon, tendon repair is performed. Torn areas near the supraspinatus tendon insertion are generally repaired using suture anchors. If the tear is located within the musculotendinous junction, side-to-side suturing using PDS is performed with a suture lasso (Fig. 2). If the tear is large, rotator cuff repair using suture anchors is necessary (Fig. 3). However, repair should be performed carefully. Calcific tendinitis is a self-limiting disease, and thus repair can increase the pressure at the removal site. In a study by Lee and Shin [23], approximately 26.5% of patients required rotator cuff repair after arthroscopic removal of calcific deposits, and they found no clinical differences between patients who received rotator cuff repair and those who received simple decompression. Acromioplasty is not required in all patients with calcific tendinitis. In patients with impingement syndrome or obvious osteophytes in the acromion, acromioplasty is effective and widens the subacromial space to prevent collisions.
회전근개 힘줄 봉합술 및 견봉 성형술
석회화 침착물 제거로 인해 힘줄에 생긴 빈 공간을 봉합해야 하는지에 대해서는 논란이 있습니다. 회전근개 파열이 작을 경우 봉합이 필요하지 않습니다. 그러나 파열이 2cm 이상이고 힘줄 두께의 70% 이상을 차지할 경우 힘줄 봉합술을 시행합니다. 상근 건 부착부 근처의 파열 부위는 일반적으로 봉합 앵커를 사용하여 봉합한다. 파열이 근건 접합부 내에 위치할 경우, PDS를 이용한 측면-측면 봉합을 봉합 라소(그림 2)로 시행한다. 파열이 클 경우 봉합 앵커를 이용한 회전근개 봉합이 필요하다(그림 3). 그러나 봉합은 신중하게 시행해야 한다. 석회화 건염은 자연 치유되는 질환이므로, 봉합술은 제거 부위의 압력을 증가시킬 수 있다. Lee와 Shin의 연구[23]에 따르면, 관절경적 석회화 침착물 제거 후 약 26.5%의 환자에게 회전근개 봉합술이 필요했으며, 회전근개 봉합술을 받은 환자와 단순 감압술만 받은 환자 간 임상적 차이는 없었다. 모든 석회화 건염 환자에게 견봉 성형술이 필요한 것은 아닙니다. 견봉 압박 증후군이 있거나 견봉에 뚜렷한 골극이 있는 환자에게는 견봉 성형술이 효과적이며, 견봉하 공간을 넓혀 충돌을 방지합니다.
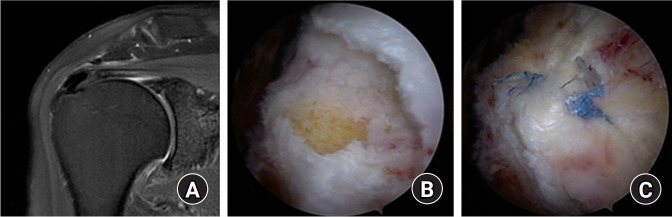
Fig. 2.
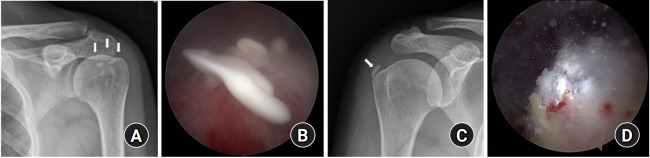
Arthroscopic decompression and rotator cuff repair using side-to-side sutures. (A) Preoperative fat suppressed T2-weighted magnetic resonance imaging coronal view shows calcific deposits on the supraspinatus tendon within musculotendinous junction. (B) Arthroscopic findings after removal and debridement of calcific deposits lesion and an approximately 1.0×1.0-cm-sized defect is seen. (C) Arthroscopic side-to-side suture is performed using polydioxanone .
Fig. 3.
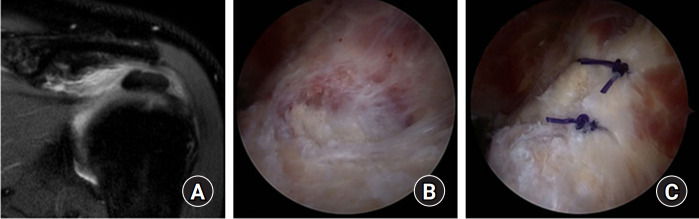
Arthroscopic decompression and rotator cuff repair using suture anchors. (A) Preoperative fat suppressed T2-weighted magnetic resonance imaging coronal view shows calcific deposits in the supraspinatus tendon insertion site. (B) Arthroscopic findings after removal and debridement of calcific deposits lesion and an approximately 2.5×1.5-cm-sized defect is seen. (C) Arthroscopic rotator cuff repair is performed using suture anchor.
측면-측면 봉합을 이용한 관절경적 감압술 및 회전근개 봉합술. (A) 수술 전 지방 억제 T2 가중 자기공명영상 관상면에서 상근건과 건근 접합부 내 석회화 침착물이 관찰됨. (B) 석회화 병변 제거 및 절제술 후 관절경 소견으로 약 1.0×1.0cm 크기의 결손이 확인됨. (C) 폴리디옥사논을 이용한 관절경적 측면-측면 봉합술 시행.
그림 3.
AUTHORS’ PREFERRED TREATMENTS
In some patients, it is difficult to identify the location of calcific deposits, even when the bursa has been sufficiently removed. In such patients, calcific deposits can be located by gently needling the rotator cuff tendon at suspicious areas with a 16-gauge spinal needle (after removing the stylet) and assessing the presence of calcific deposits on the needle tip. When the needle passes through calcific deposits, leaking of the calcific deposits into the subacromial space can be observed.
After removing calcific deposits, large partial or small full-thickness rotator cuff tears are not repaired. Rotator cuff repair is performed only for medium or large full-thickness rotator cuff tears. Side-to-side sutures are placed using PDS for tears at the musculotendinous junction. For other types of tears, rotator cuff repair is performed according to the shape of the tear using suture anchors.
봉합 앵커를 이용한 관절경적 감압술 및 회전근개 봉합술. (A) 수술 전 지방 억제 T2 가중 자기공명영상 관상면에서 상근 건 부착부에 석회화 침착물이 관찰됨. (B) 석회화 병변을 제거하고 정복한 후 관절경 소견에서 약 2.5×1.5cm 크기의 결손이 관찰됩니다. (C) 봉합 앵커를 이용한 관절경 회전근개 봉합술을 시행합니다.
POSTOPERATIVE REHABILITATION
Shoulder and elbow motion are allowed immediately after the operation as long as the pain is tolerable, and an arm sling is required for 3 weeks for protection in patients with calcific decompression. Passive and active shoulder ROM exercises should be started immediately, and muscle strengthening exercises should be started 6 to 12 weeks after the operation. Patients can immediately perform light office work, and moderate labor can be started from 6 to 12 weeks after the operation.
If the rotator cuff was repaired using a suture anchor at the tendon insertion site, a shoulder abduction brace needs to be used for 4 weeks, and gradual passive shoulder ROM exercises need to be started immediately after the operation. Muscle strengthening exercises can be started from 6 to 12 weeks after the operation, depending on the size of the tear.
저자들이 선호하는 치료법
일부 환자의 경우, 활액낭을 충분히 제거했음에도 석회화 침착물의 위치를 확인하기 어려운 경우가 있습니다. 이러한 환자에서는 16게이지 척추용 바늘(스타일렛 제거 후)로 회전근개 건의 의심 부위를 부드럽게 찔러 바늘 끝에 석회화 침착물이 있는지 확인함으로써 위치를 파악할 수 있다. 바늘이 석회화 침착물을 통과할 때 석회화 침착물이 견봉하 공간으로 유출되는 현상을 관찰할 수 있다.
석회화 침착물을 제거한 후, 큰 부분 파열 또는 작은 전층 회전근개 파열은 봉합하지 않습니다. 중등도 또는 큰 전층 회전근개 파열에 대해서만 회전근개 봉합술을 시행합니다. 근건 접합부 파열에는 PDS를 사용한 측면-측면 봉합을 시행합니다. 다른 유형의 파열에는 봉합 앵커를 사용하여 파열 형태에 따라 회전근개 봉합술을 시행합니다.
수술 후 재활
통증이 견딜 수 있는 범위 내에서 수술 직후부터 어깨와 팔꿈치 운동이 허용되며, 석회화 감압술을 시행한 환자의 경우 보호를 위해 3주간 팔 보호대 착용이 필요합니다. 수동적 및 능동적 어깨 가동 범위 운동은 즉시 시작해야 하며, 근력 강화 운동은 수술 후 6~12주 후에 시작해야 합니다. 환자는 즉시 가벼운 사무 작업을 수행할 수 있으며, 중등도 노동은 수술 후 6~12주부터 시작할 수 있습니다.
회전근개가 힘줄 부착부에서 봉합 앵커를 사용하여 봉합된 경우, 4주간 어깨 외전 보조기를 착용해야 하며, 수술 직후 점진적인 수동 어깨 ROM 운동을 시작해야 합니다. 근력 강화 운동은 파열 크기에 따라 수술 후 6~12주부터 시작할 수 있습니다.
CONCLUSION
The primary choice of treatment for calcific tendinitis is conservative, especially in patients with acute calcific tendinitis. However, conservative treatment often fails in chronic patients, so surgical treatment is required. Many patients regard operative treatment as a simple procedure and expect rapid recovery. However, the clinical symptoms of many patients do not improve immediately after surgery and require 6 months or more for complete recovery. Therefore, patients should be given sufficient prior explanation that recovery could be delayed and that intermittent pain could occur for 2 years or more after surgery. In addition, continual follow-up for pain control and recurrence of symptoms is necessary after surgery.
결론
석회화 건염의 일차적 치료 선택은 보존적 치료이며, 특히 급성 석회화 건염 환자에게 해당됩니다. 그러나 만성 환자에게는 보존적 치료가 종종 실패하므로 수술적 치료가 필요합니다. 많은 환자들이 수술적 치료를 간단한 시술로 여기고 빠른 회복을 기대합니다. 그러나 많은 환자의 임상 증상은 수술 직후 개선되지 않으며 완전한 회복까지 6개월 이상 소요됩니다. 따라서 환자에게 회복이 지연될 수 있으며 수술 후 2년 이상 간헐적 통증이 발생할 수 있다는 점을 사전에 충분히 설명해야 합니다. 또한 수술 후 통증 관리 및 증상 재발을 위한 지속적인 추적 관찰이 필요합니다.
Footnotes
Research Ethics
IRB approval: None.
Financial support
None.
Conflict of interest
None.
REFERENCES
- 1.Depalma AF, Kruper JS. Long-term study of shoulder joints afflicted with and treated for calcific tendinitis. Clin Orthop. 1961;20:61–72. [PubMed] [Google Scholar]
- 2.Loew M, Jurgowski W, Mau HC, Thomsen M. Treatment of calcifying tendinitis of rotator cuff by extracorporeal shock waves: a preliminary report. J Shoulder Elbow Surg. 1995;4:101–6. doi: 10.1016/s1058-2746(05)80062-x. [DOI] [PubMed] [Google Scholar]
- 3.Jim YF, Hsu HC, Chang CY, Wu JJ, Chang T. Coexistence of calcific tendinitis and rotator cuff tear: an arthrographic study. Skeletal Radiol. 1993;22:183–5. doi: 10.1007/BF00206150. [DOI] [PubMed] [Google Scholar]
- 4.Codman EA, Akerson IB. The pathology associated with rupture of the supraspinatus tendon. Ann Surg. 1931;93:348–59. doi: 10.1097/00000658-193101000-00043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Uhthoff HK, Loehr JW. Calcific tendinopathy of the rotator cuff: pathogenesis, diagnosis, and management. J Am Acad Orthop Surg. 1997;5:183–91. doi: 10.5435/00124635-199707000-00001. [DOI] [PubMed] [Google Scholar]
- 6.Bosworth DM. Diagnosis and treatment of lesions of the shoulder. R I Med J. 1953;36:512–5. [PubMed] [Google Scholar]
- 7.Neer CS II. Less frequent procedures. In: Neer CS II, editor. Shoulder reconstruction. Philadelphia, PA: WB Saunders; 1990. pp. 421–85. [Google Scholar]
- 8.Molé D, Kempf JF, Gleyze P, Rio B, Bonnomet F, Walch G. Results of endoscopic treatment of non-broken tendinopathies of the rotator cuff. 2. Calcifications of the rotator cuff. Rev Chir Orthop Reparatrice Appar Mot. 1993;79:532–41. [PubMed] [Google Scholar]
- 9.Loew M, Sabo D, Wehrle M, Mau H. Relationship between calcifying tendinitis and subacromial impingement: a prospective radiography and magnetic resonance imaging study. J Shoulder Elbow Surg. 1996;5:314–9. doi: 10.1016/s1058-2746(96)80059-0. [DOI] [PubMed] [Google Scholar]
- 10.Speed CA, Hazleman BL. Calcific tendinitis of the shoulder. N Engl J Med. 1999;340:1582–4. doi: 10.1056/NEJM199905203402011. [DOI] [PubMed] [Google Scholar]