Re:81 Rationale, Feasibility and Acceptability of Ketogenic Diet for Cancer Treatment - 2017년 review 한국논문
작성자문형철작성시간20.02.09조회수653 목록 댓글 0beyond reason
Rationale, Feasibility and Acceptability of Ketogenic Diet for Cancer Treatment
Hae-Yun Chung and Yoo Kyoung Park
Abstract
Ketogenic diet has been used for more than 80 years as a successful dietary regimen for epilepsy. Recently, dietary modulation by carbohydrate depletion via ketogenic diet has been suggested as an important therapeutic strategy to selectively kill cancer cells and as adjuvant therapy for cancer treatment. However, some researchers insist ketogenic diet to be highly undesirable as ketogenic diet may trigger and/or exacerbate cachexia development and usually result in significant weight loss.
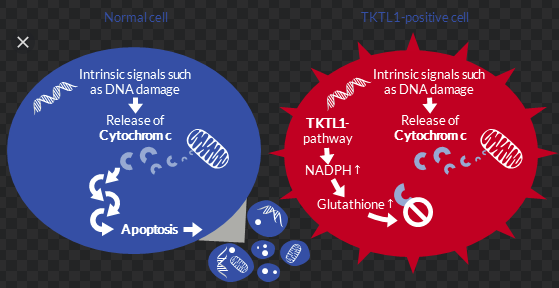
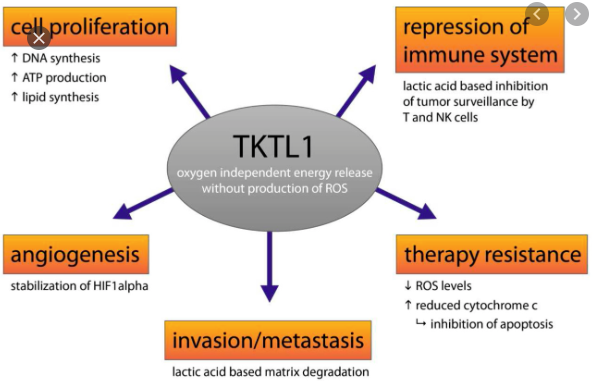
This review revisits the meaning of physiological ketosis in the light of this evidence and considers possibility of the use of ketogenic diet for oncology patients. Article search was performed from 1985 through 2017 and finally 10 articles were analyzed. The review focused on the results of human trials for cancer patients and checked the feasibility of using ketogenic diet for cancer patients as adjuvant therapy. The main outcomes showed improvement of body weight changes, anthropometric changes, serum blood profiles, and reduction in novel marker for tumor progression, TKTL1, and increase of ketone body. Lactate concentration was reduced, and no significant changes were reported in the measurements of quality of life.
Ketogenic diet may be efficacious in certain cancer subtypes whose outcomes appear to correlate with metabolic status, but the results are not yet supportive and inconsistent. Therefore, it warrants further studies.
INTRODUCTION
Diet and exercise interventions in cancer patients may be of benefit for ameliorating adverse events during cancer treatment and may increase overall survival.1–3 Metabolic processes in cancer are complex and highly regulated, and there is increasing evidence that dietary modulation can be efficacious in managing cancer, i.e., diet rich in fat and protein4 or calorie restriction.5,6Calorie restriction has been shown to reduce the pro-growth signaling, partially achieved by temporarily reducing glucose and circulating insulin-like growth factor 1, which is highly associated with aging and cancer.7 Also, manipulation of the molecular pathways using calorie restriction has been shown to render cancer cells susceptible to standard cytotoxic treatment with radiation and chemotherapy especially strong for breast cancer. However, considering the high drop-out rate (25%), this indicates that adherence to this low-calorie diet requires high commitment to the study participants.
Ketogenic diet is designed specifically to result in ketosis and is emerging as a metabolic therapy for treating cancer. The mechanism can be explained by inducing shortage of glucose and/or lactate for tumor cells to survive. Vander Heiden et al.8 observed that tumors take up enormous amounts of glucose compared to the surrounding tissue and eventually produces lactate through aerobic glycolytic pathway. Therefore, limitation of glucose availability in cancer cell may reduce energy production of cancer cells, and thereby decreasing tumor proliferation.9
The aim of this review is to assess the clinical evidence of ketogenic diet intervention in cancer patients by analyzing human trials.
STUDY SEARCH AND SELECTION
1. Literature search
The eligible literatures were retrieved by searching through databases (PubMed, MEDLINE, and Springer link) from 1985 until July, 2017. Searching keywords included “ketogenic diet” or “ketone”, “cancer” or “tumor”, and “oncology” with no language restriction and was limited to human clinical trials.
2. Inclusion and exclusion criteria
Articles were included under the following criteria: (1) randomized clinical trials with/without control, (2) prospective cohort study, (3) adult population, and (4) ketone diet composition mentioned. The exclusion criteria were as follows: (1) articles with incomplete data, (2) case studies, and (3) reviews. Letters or comments were irrespective.
3. Data extraction
After the completion of article screening, two investigators independently extracted the data from the eligible studies according to the predesigned protocol. The extracted information was summarized by the first author’s name, journal name, publication year, geographical area of study population, mean age of the participants, sample size of the intervention and control groups, detailed dietary regimen and the length of the study, adherence rate, outcome measures, and results of each article, and finally reported side effects.
ELIGIBLE STUDIES
The process of search strategy is presented in Figure 1. The original search yielded a total of 468 citations (limited to clinical trials, human studies, and years from 1985–2017). First, there were 63 articles after removing the duplicates. Then, 47 articles were excluded because of obvious irrelevance after screening the title and abstract. Six among the remained 16 articles were removed after full-text review: 2 for case studies; 4 without available data. Finally, 10 articles were included in this review. The recommendation of the Cochrane Effective Practice and Organization of Care Review systematic review and meta-analyses, randomized controlled studies, and non-randomized controlled studies were included.10

SUMMARY OF THE STUDY OUTCOMES OF ELIGIBLE ARTICLES
The detailed information of ketone diets from the selected articles are summarized in Table 1.11–20

A total of 214 subjects were included in the review. Most of the studies were intervention trials except for one prospective cohort study. The mean age of the studies was mostly from late fifties to early seventies. Eight out of ten articles were submitted from European countries (Germany and Italy) and only two were from USA. The duration of experimental intervention ranged from 5 days to 2 years and the outcome measures were mainly focused on the body weight and composition and blood profile. One article measured quality of life (QOL). The adherence rate in 5 studies were 100%, and the rest were from 31% to 85%. Reported side effects in the studies were relatively minor and included only few reported constipation, leg cramps, diarrhea, etc. Subjects maintained on ketogenic diet for a relatively short period (2 weeks in the study by Rossi-Fanelli et al.,12; 1 week in the study by Fearon et al.,11; 5 days in the study by Schroeder et al.16) did not show any significant changes of the markers, such as body weight or blood profile except for decrease in lactate concentration in the tumor tissues. Meanwhile, when subjects were maintained for a longer period, such as 8 weeks, ketogenic diet (normal meal + fat-enriched liquid diet) successfully showed increased energy intake and body weight of the subjects.13 Ketogenic diet in this study was used for only malnourished gastro-intestinal cancer patient with metastases, suggesting the possibility of application in specific cancer patients. Evaluation on anticancer biomarkers was not measured in most of the articles except for study by Jansen and Walach18 who found that TKTL1, a novel marker associated with tumor progression, was reduced by a 2-year ketogenic diet.
Notably, the results from Fine et al.,15 Rieger et al.,17 and Klement and Sweeney19 showed that ketone diet increased significant weight loss. These results showed that unlike the consistent ketogenic effects on epilepsy patients, ketogenic effects on cancer patients were not consistent in this review.
KETOGENIC DIET AS A CANCER THERAPEUTIC STRATEGY
Recently, ketogenic diet has been newly emerged as a cancer therapy in both animal models and humans. Some of the preclinical studies have shown the effect of ketogenic diet to reduce tumor growth and improve survival in animal models of malignant glioma,21–23 prostate cancer,24–26 colon cancer,27 and gastrointestinal cancer.28 Low calorie diet, such as fasting inducing a state of ketosis, has been shown to enhance the responsiveness of cancer cells to chemotherapy in pre-clinical cancer therapy models and to ameliorate some of chemotherapy-induced side effects in normal tissues.29
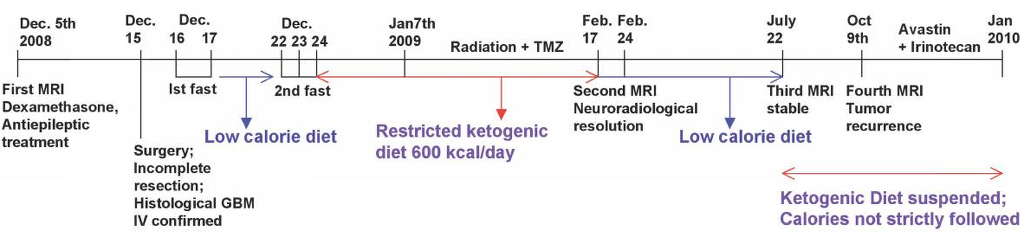
More recently, numerous case reports were reported. First report was derived from confirmed glioblastoma multiforme treated with standard therapy together with a restricted ketogenic diet, and the response observed in the case suggested the possibility of calorie-restricted ketogenic diet.30 - 토마스 사이프리드 교수 연구
Ketogenic diet has been studied intensively in the European country including Germany. In these studies, the physical condition was successfully improved and tumor shrinkage was observed by ketogenic diet.14 The studies here reviewed lack greatly in the homogeneity of type of cancer, location of cancer, the stages of cancer, and the treatment course of the cancer, and thus the results cannot be generalized. Because ketogenic diet normally results in an increased weight loss, there are continuous concerns to apply this diet for cancer patients. In this review, however, we found that ketogenic diet showed no significant adverse effects. It may be possibly because the subjects were adults, while in children long-term ketogenic diet induces renal damage such as kidney stones.31 Any adverse effects reported in this review were constipation, diarrhea, fatigue, etc. In healthy obese adults with low-carbohydrate ketogenic diet for 6 months, the only adverse effects reported were an increase in the level of low-density lipoprotein cholesterol and some shakiness and uneasiness.32
Studies described in this review assessed the effects of a ketogenic diet in cancer patients. Only ten studies were analyzed and the characteristics and study design, the ketogenic diet regimen, the length of study, cancer type and stage, and site were heterogeneous, thereby contributing to a poor conclusion.
As for ongoing clinical trials, there are currently 62 trials assessing low carbohydrate diets as a potential therapy for a variety of diseases of which 13 trials are assessing ketogenic diet as an adjuvant cancer therapy. Three of the studies are not initiated, but, one study with pancreatic cancer patients was terminated because of the low participation and adherence (Table 2).

CONCLUSION
Our main aim in this review was to assess the feasibility and acceptability of ketogenic diet and to assess the changes of outcome variables, such as body composition, biochemical blood profiles, and QOL. From this review, we found further evidence that ketogenic diet in cancer patients is safe and feasible as an adjuvant therapy. As described above, we could conclude that in order to see any significant progression or improvement by ketogenic diet, at least 3 to 4 weeks of ketogenic diet is required. Additionally, we suggest that not only body composition but also biomarker or measures for tumor size or tumor metabolism assessment is essential. We also conclude that the acceptability for ketone diet may be better in some cancer type (better in glioblastoma than gastric cancer).
In conclusion, ketogenic diet can be safely used to cancer patients if carefully monitored. Most importantly, we have to establish standardized treatment protocol which include the length and regimen for ketogenic diet.
ACKNOWLEDGMENTS
This work was supported by the Korea Institute of Planning and Evaluation for Technology in Food, Agriculture, Forestry and Fisheries (IPET) through the High Value-added Food Technology Development Program, funded by the Ministry of Agriculture, Food and Rural Affairs (MAFRA) (316055-3).
Footnotes
CONFLICTS OF INTEREST
No potential conflicts of interest were disclosed.