beyond reason
10만명당 5-20명
돌발성 난청의 흔한 원인
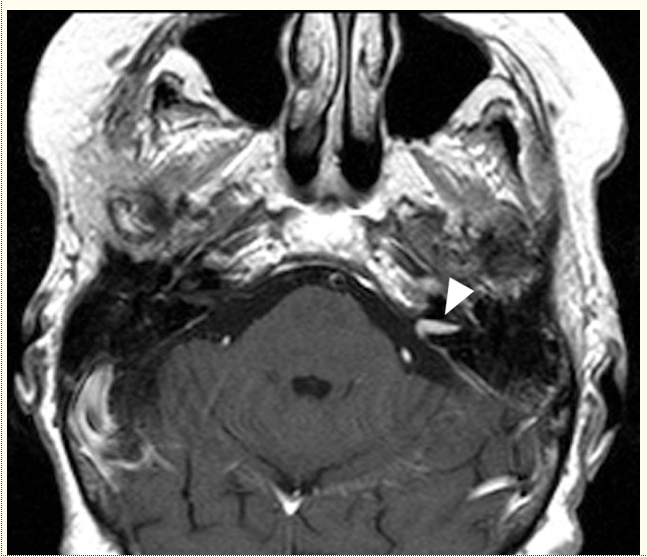
MRI of patient with SSNHL. This patient’s moderate flat SSNHL resolved completely following treatment with 1mg/kg prednisone and oral antiherpetic medications for 10 days followed by a short prednisone taper. Note small left intracanalicular enhancing mass consistent with vestibular schwannoma (arrowhead). MRI, magnetic resonance image; SSNHL, sudden sensorineural hearing loss.
Sudden Sensorineural Hearing Loss
 1
1Abstract
Sudden sensorineural hearing loss (SSNHL) is commonly encountered in audiologic and otolaryngologic practice. SSNHL is most commonly defined as sensorineural hearing loss of 30dB or greater over at least three contiguous audiometric frequencies occurring within a 72-hr period. Although the differential for SSNHL is vast, for the majority of patients an etiologic factor is not identified. Treatment for SSNHL of known etiology is directed toward that agent, with poor hearing outcomes characteristic for discoverable etiologies that cause inner ear hair cell loss. Steroid therapy is the current mainstay of treatment of idiopathic SSNHL in the United States. The prognosis for hearing recovery for idiopathic SSNHL is dependent on a number of factors including the severity of hearing loss, age, presence of vertigo, and shape of the audiogram.
Keywords: hearing loss, sudden sensorineural hearing loss, idiopathic sudden sensorineural hearing loss, evaluation, treatment
Sudden sensorineural hearing loss (SSNHL) is commonly encountered in audiologic and otolaryngologic practice. SSNHL is most commonly defined as sensorineural hearing loss of 30dB or greater over at least three contiguous audiometric frequencies occurring within a 72-hr period. Although the differential for SSNHL is vast, for the majority of patients an etiologic factor is not identified. Treatment for SSNHL of known etiology is directed toward that agent, with poor hearing outcomes characteristic for discoverable etiologies that cause inner ear hair cell loss. Steroid therapy is the current mainstay of treatment of idiopathic SSNHL in the United States. The prognosis for hearing recovery for idiopathic SSNHL is dependent on a number of factors including the severity of hearing loss, age, presence of vertigo, and shape of the audiogram.
Introduction
Sudden sensorineural hearing loss (SSNHL) is most often defined as sensorineural hearing loss of 30dB or greater over at least three contiguous audiometric frequencies occurring over 72 hr (Wilson, Byl, & Laird, 1980). SSNHL is a relatively common complaint in otologic and audiologic practices (1.5-1.7 per 100 new patients presenting in our practice). For 7% to 45% of patients, a defined cause can be identified and specific therapeutic regiment used for treatment (Byl, 1984; Chau, Lin, Atashband, Irvine, & Westerberg, 2010; Fetterman, Saunders, & Luxford, 1996; Huy & Sauvaget, 2005; Nosrati-Zarenoe, Arlinger, & Hultcrantz, 2007; Shaia & Sheehy, 1976). The majority of patients with sudden SNHL have no identifiable cause for hearing loss and are classified as “idiopathic” (Byl, 1984; Chau et al., 2010; Fetterman et al., 1996; Nosrati-Zarenoe et al., 2007; Shaia & Sheehy, 1976). Despite extensive research, controversy remains in the etiology and appropriate care of patients with idiopathic SSNHL Regardless of etiology, recovery of hearing thresholds following SSNHL may not occur, may be partial, or can be complete. Factors impacting hearing recovery include age at onset of hearing loss, hearing loss severity and frequencies affected, presence of vertigo, and time between onset of hearing loss and visit with the treating physician (Byl, 1984).
Over 1,200 articles on SSNHL are available on PubMed, and many more articles on the subject predate the PubMed era. For practitioners, the enormous number of articles on this topic can be overwhelming, particularly as recommendations vary greatly between publications. In this article, we summarize the available literature and suggest guidelines for evaluation and management of SSNHL.
Epidemiology
The incidence of SSNHL is 5-20 per 100,000 (Byl, 1984; Fetterman et al., 1996; Hughes, Freedman, Haberkamp, & Guay, 1996). The true incidence of SSNHL may be higher than these estimates because affected individuals who recover quickly do not present for medical care (Byl, 1984; Simmons, 1973). Although individuals of all ages can be affected, the peak incidence is between the fifth and sixth decade of life. SSNHL occurs with equal incidence in men and women (Byl, 1984; Fetterman et al., 1996; Nosrati-Zarenoe et al., 2007; Shaia & Sheehy, 1976). Nearly all cases are unilateral; less than 2% of patients have bilateral involvement and typically bilateral involvement is sequential (Byl, 1984; Fetterman et al., 1996; Huy & Sauvaget, 2005). Accompanying symptoms include tinnitus (41% to 90%) and dizziness (29% to 56%) (Byl, 1984; Fetterman et al., 1996; Huy & Sauvaget, 2005; Xenellis et al., 2006). Many patients report first noting their hearing loss on awakening (Chau et al., 2010).
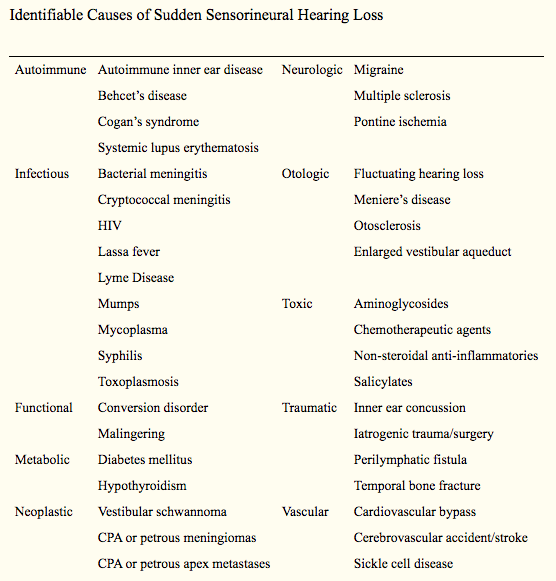
Identifiable Causes of SSNHL
Identifiable causes are found for 7% to 45% of patients with SSNHL (Byl, 1984; Chau et al., 2010; Fetterman et al., 1996; Huy & Sauvaget, 2005; Mattox & Simmons, 1977; Nosrati-Zarenoe et al., 2007; Shaia & Sheehy, 1976). The differential diagnosis for SSNHL includes more than a hundred potential etiologies (Chau et al., 2010; Fetterman et al., 1996; Mattox & Simmons, 1977). Cases with a potentially discoverable etiology fall into one of several broad categories including infectious, autoimmune, traumatic, vascular, neoplastic, metabolic, and neurologic (Table 1). In a meta-analysis of 23 studies of SSNHL, the most frequent causes identified were infectious (13%) followed by otologic (5%), traumatic (4%), vascular or hematologic (3%), neoplastic (2%), and other (2%) (Chau et al., 2010). Other causes, such as malingering, conversion disorder, and ototoxic drug administration, were not examined in this study, and should be added to the list of identifiable etiologies of SSNHL (Table 1). For many of these etiologic agents, hearing loss results from damage to hair cells or other cochlear structures and is irreversible. Further damage can occasionally be prevented if the underlying etiology is identified and treated promptly. More rarely, SSNHL resulting from known causes can be reversed. However, many of these identifiable causes of SSNHL have broader health implications for the patient. Thus, identification of conditions underlying SSNHL can be justified in terms of overall patient health rather than simply in terms of hearing outcomes.
Table 1.
Identifiable Causes of Sudden Sensorineural Hearing Loss
| Autoimmune | Autoimmune inner ear disease | Neurologic | Migraine |
| Behcet’s disease | Multiple sclerosis | ||
| Cogan’s syndrome | Pontine ischemia | ||
| Systemic lupus erythematosis | |||
| Infectious | Bacterial meningitis | Otologic | Fluctuating hearing loss |
| Cryptococcal meningitis | Meniere’s disease | ||
| HIV | Otosclerosis | ||
| Lassa fever | Enlarged vestibular aqueduct | ||
| Lyme Disease | |||
| Mumps | Toxic | Aminoglycosides | |
| Mycoplasma | Chemotherapeutic agents | ||
| Syphilis | Non-steroidal anti-inflammatories | ||
| Toxoplasmosis | Salicylates | ||
| Functional | Conversion disorder | Traumatic | Inner ear concussion |
| Malingering | Iatrogenic trauma/surgery | ||
| Metabolic | Diabetes mellitus | Perilymphatic fistula | |
| Hypothyroidism | Temporal bone fracture | ||
| Neoplastic | Vestibular schwannoma | Vascular | Cardiovascular bypass |
| CPA or petrous meningiomas | Cerebrovascular accident/stroke | ||
| CPA or petrous apex metastases | Sickle cell disease | ||
| CPA myeloma |
The two most common bacterial infections known to cause SSNHL in the United States are Lyme disease and syphilis. Lyme disease is endemic in North America. It is caused by infection with the spirochete Borrelia burgdorferi which is transmitted by the bite of deer ticks. The infected tick must be attached to a human host for 2-3 days to transfer the bacteria. One of the most characteristic early manifestations of this infection is an expanding erythematous rash (known as erythema migrans) which lasts 2-3 weeks without treatment. Chronic manifestations of Lyme disease can occur within the first year of infection and include systemic neurologic involvement including facial paralysis and asymmetric sensorineural hearing loss. Other sequelae include rheumatologic disorders such as arthritis, cardiac conditions such as arterioventricular block, neurologic disorders including chronic meningoencephalitis, and fibromyalgia (Wormser et al., 2006). Some studies examining rates of Lyme disease in SSNHL find up to a 20% rate of positive Lyme titers (Lorenzi et al., 2003; Walther, Hentschel, Oehme, Gudziol, & Beleites, 2003); however, some authors report a 0% incidence or very low incidence of Lyme titer positivity in their series (Heman-Ackah, Jabbour, & Huang, 2010; Walther et al., 2003). One of the higher incidence studies (Lorenzi et al., 2003) found that elevated Lyme titers were not typically associated with a history of erythema migrans (only 1 of 10 Lyme-positive patients had that history) and many (40%) were not associated with risk factors for Lyme disease (living in an endemic area, history of tick bite, history of pet with ticks). Hearing recovery was similar for Lyme-positive and Lyme-negative SSNHL patients, although there was a trend for worse hearing in the Lyme-positive group (Lorenzi et al., 2003).
Syphilis is a sexually transmitted disease that results from infection by the bacterium Treponema pallidum. Known as the great imitator, syphilis has a wide variety of clinical manifestations. Following infection, the patient can initially present with a painless skin lesion, called a chance, on the genitalia (primary infection). Even at this early stage, the infected patient is at risk for neurosyphilis, and one of the manifestations can be otosyphilis (Marra, 2009). Otosyphilis Otosyphilis can have a variety of presentations, including SSNHL, progressive hearing loss, fluctuating hearing loss, or a Meniere’s-like syndrome with episodic attacks of vertigo, increased tinnitus, and hearing loss (Chau et al., 2010; Fitzgerald & Mark, 1998; Garcia-Berrocal et al., 2006; Gleich, Linstrom, & Kimmelman, 1992; Pulec, 1997; Xenellis et al., 2006). Immunosuppressed patients, particularly those with HIV, are at greatest risk for developing neurosyphilis even after appropriate treatment of primary, secondary, or early latent disease and in the presence of decreased serum RPR and high CD4 counts (Marra, 2009; Mishra et al., 2008).
Other infectious agents have been associated with SSNHL. Toxoplasmosis is a treatable condition caused by the protozoan Toxoplasma gondii, commonly contracted due to contact with cats’ feces or ingestion of undercooked meat, that has been associated with some cases of SSNHL (Cadoni et al., 2005). Many viruses have been implicated in the etiology of SSNHL, including herpes simplex, varicella zoster, enteroviruses, and influenza (Chau et al., 2010). The one virus that has very clearly been shown to be a cause of SSNHL is mumps (Vuori, Lahikainen, & Peltonen, 1962; Westmore, Pickard, & Stern, 1979).
Up to 4.7% of patients who initially present with SSNHL will ultimately be diagnosed with some or other otologic disorder as their disease fully manifests over time (Chau et al., 2010). The leading final otologic diagnosis is Meniere’s disease; years after the initial hearing insult (and potential recovery), the patient can develop the more typical symptoms of this disorder (Figure 1). Other common otologic diseases that can present initially with SSNHL include fluctuating hearing loss, otosclerosis, and progressive sensorineural hearing loss (Byl, 1984; Chau et al., 2010). Additionally, trauma can cause SSNHL; often the history in these cases is obvious (Chau et al., 2010). However, in patients with enlarged vestibular aqueduct syndrome, patients can present with SSNHL following very minor trauma (such as diving into a swimming pool) (Okumura, Takahashi, Honjo, Takagi, & Mitamura, 1995).

Audiograms of a patient initially presenting with SSNHL ultimately found to have Meniere’s disease. Note near resolution of initial hearing loss following high-dose corticosteroid therapy. Initial audiogram following SSNHL (A); audiogram following 10-day course of 1mg/kg prednisone (B); and audiogram following onset of episodes of spinning vertigo lasting 30-60 min accompanied by left aural fullness and tinnitus. Circles represent right masked air levels; squares represent left masked air levels; right facing bracket represent right masked bone levels; squares represent left masked bone levels. SSNHL, sudden sensorineural hearing loss.
Many vascular and hematologic pathologies have been associated with SSNHL. These include emboli, transient ischemic attacks, sickle cell anemia, macroglobulinemia, and subdural hematoma, among many others (Chau et al., 2010; Lee, Lopez, Ishiyama, & Baloh, 2000; Ruben, Distenfeld, Berg, & Carr, 1969; Urban, 1973). These pathologies decrease the blood supply to the cochlea, thus reducing intracochlear oxygen levels. As cochlear structures are fairly susceptible to even brief episodes of hypoxia, this type of obstruction can lead to either a transient or permanent hearing loss in experimental models (Scheibe, Haupt, & Baumgartl, 1997; Schweinfurth & Cacace, 2000).
A variety of neoplasms can cause SSNHL, particularly vestibular schwannomas (acoustic neuromas). The incidence of vestibular schwannoma in series of patients with SSNHL ranges from none to 48%, although most studies find at least one or two within their groups of patients (Byl, 1984; Cadoni et al., 2005; Chau et al., 2010; Fitzgerald & Mark, 1998; Heman-Ackah et al., 2010; Nosrati-Zarenoe, Hansson, & Hultcrantz, 2010; Tucci, Farmer, Kitch, & Witsell, 2002; Xenellis et al., 2006). One review estimated the incidence of all neoplastic causes of SSNHL at 2.3%. This figure includes more rare metastatic and benign tumors as well as vestibular schwannomas (Chau et al., 2010). Return of hearing does not indicate that neoplasms are absent as SSNHL due to these causes can potentially recover spontaneously or after treatment with systemic steroids (Berg, Cohen, Hammerschlag, & Waltzman, 1986; Nageris & Popovtzer, 2003). Thus evaluation of patients with SSNHL for neoplasms cannot be omitted in patients with complete hearing recovery (Figure 2).

MRI of patient with SSNHL. This patient’s moderate flat SSNHL resolved completely following treatment with 1mg/kg prednisone and oral antiherpetic medications for 10 days followed by a short prednisone taper. Note small left intracanalicular enhancing mass consistent with vestibular schwannoma (arrowhead). MRI, magnetic resonance image; SSNHL, sudden sensorineural hearing loss.
SSNHL may be a manifestation of various systemic autoimmune disorders and thyroid disorders. A number of autoimmune diseases including Cogan’s syndrome, systemic lupus erythematosus, temporal arteritis, and Wegener’s granulomatosis have been associated with a sudden hearing loss (Garcia Berrocal, Vargas, Vaquero, Ramon y Cajal, & Ramirez-Camacho, 1999; Kempf, 1989; Paira, 1998; Rowe-Jones, 1990; Wolfovitz, Levy, & Brook, 1987). Thyroid dysfunction has been reported in 1% to 15% of patients presenting with SSNHL (Heman-Ackah et al., 2010; Narozny, Kuczkowski, & Mikaszewski, 2006). As hypo- and hyperthyroidism are treatable and potentially reversible causes of SSNHL, thyroid stimulating hormone (TSH) is often a component of the serologic evaluation of SSNHL.
Theories of the Etiology of Idiopathic SSNHL
The etiology remains unknown in the majority of patients who present with SSNHL and therefore their hearing loss is classified as idiopathic (Byl, 1984; Chau et al., 2010; Fetterman et al., 1996; Nosrati-Zarenoe et al., 2007; Shaia & Sheehy, 1976). Numerous hypotheses of the pathophysiology of idiopathic SSNHL have been proposed. The most widely accepted theories are vascular compromise (Fisch, Nagahara, & Pollak, 1984; Gussen, 1976; Morgenstein & Manace, 1969; Ruben et al., 1969), cochlear membrane rupture (Goodhill, 1971; Harris, 1984; Simmons, 1968), and viral infection (Saunders & Lippy, 1959; Schuknecht et al., 1962) (reviewed in Byl, 1984; Mattox & Simmons, 1977).
Some authors have suggested that idiopathic SSHL has a vascular etiology. The blood supply to the cochlea arises from two small terminal arteries. Due to the small diameter of the vessels within the arterial supply and lack of collateral blood supply, the cochlea is susceptible to injury through a variety of vascular insults. The clinical presentation of unilateral sudden SNHL is comparable to the clinical presentation of ischemic vascular diseases such as transient ischemic attacks and amaurosis fugax (Ballesteros et al., 2009). Some studies have found that risk factors for ischemic vascular disease, including cigarette smoking, hypertension, and hyperlipidemia, are risk factors for the development of idiopathic SSNHL (Capaccio et al., 2007; Chau et al., 2010), although others have found no association of these risk factors with idiopathic SSNHL (Ballesteros et al., 2009; Cadoni et al., 2005; Einer, Tengborn, Axelsson, & Edstrom, 1994). According to the vascular etiologic theories, the sudden loss of hearing could result from an acute vascular hemorrhage (Colclasure & Graham, 1981; Schuknecht, Igarashi, & Chasin, 1965), occlusion by emboli (Jaffe, 1970), vascular disease (Kirikae, Nomura, Shitara, & Kobayashi, 1962), vasospasm (Mattox & Simmons, 1977), or change in blood viscosity (Ruben et al., 1969; Urban, 1973). Using magnetically guided iron particles, Schweinfurth and colleagues embolized the cochlear vasculature of six New Zealand white rabbits yielding a 12-37 dB drop in distortion product otoacoustic emissions (DPOAEs; Schweinfurth & Cacace, 2000). Spontaneous recovery of hearing was noted in only 33% of animals within this study. The changes found in the animals’ DPOAEs parallel those reported in clinical studies of patients with idiopathic SSNHL (Schweinfurth, Cacace, & Parnes, 1997).
However, the clinical course and radiographic findings characteristic of most cases of idiopathic SSNHL are not consistent with a vascular etiology. In cases of sensorineural hearing loss resulting from a known intravascular insult, the loss is permanent, whereas, hearing loss in the majority of cases of idiopathic SSNHL is reversible (Byl, 1984; Mattox & Simmons, 1977; Merchant, Durand, & Adams, 2008; Stokroos & Albers, 1996). Potentially as a reflection of the amount of damage and permanence of the hearing loss following occlusion of the cochlear vasculature, cochlear fibrosis occurs over the subsequent weeks (Belal, 1979; Schuknecht & Donovan, 1986; Yoon, Paparella, Schachern, & Alleva, 1990), and this fibrosis can be seen in radiologic studies of patients with hearing loss following known vascular occlusion (Lee et al., 2000). In idiopathic SSNHL, cochlear fibrosis is not typically observed (Albers, Demuynck, & Casselman, 1994; Schuknecht et al., 1962; Schuknecht & Donovan, 1986). Thus, though a vascular etiology may explain a few cases of idiopathic SSNHL, it is not the cause of most cases of this disorder.
Cochlear trauma with tearing or rupture of delicate inner ear membranes has been proposed as a pathophysiologic factor in the development of idiopathic SSNHL. Simmons reported on several patients who presented with complaints of sudden onset of hearing loss accompanied by a “pop,” often occurring at a time of strenuous activity or increased intracranial pressure, and proposed Reissner’s membrane was the site of injury (Simmons, 1968). Postmortem histopathologic temporal bone evaluation of two patients with idiopathic SSNHL who later died due to unrelated causes revealed rupture of Reissner’s membrane supporting the membrane rupture theory as a potential pathophysiology of idiopathic SSNHL (Gussen, 1981; Simmons, 1968). However, most people with idiopathic SSNHL do not remember a significant Valsalva, trauma, or a “pop” immediately prior to onset of hearing loss; and many studies do not see inner membrane ruptures in temporal bone studies of patients who had idiopathic SSNHL (Merchant et al., 2008; Schuknecht & Donovan, 1986). Goodhill presented a case series of patients with SSHL, often following a popping sensation, and proposed that these patients had hearing loss due to perilymphatic fistulae (Goodhill, 1971). This engendered the practice of middle ear exploration and fistula repair in most cases of idiopathic SSNHL (Grundfast & Bluestone, 1978; Meyerhoff, 1979; Meyerhoff & Pollock, 1990; Singleton et al., 1987). Although the concept of perilymphatic fistula underlying most cases of idiopathic SSNHL has fallen out of favor, fistulae clearly underlie some cases of SSNHL in patients with a clear history of barotraumas, temporal bone fractures, or trauma after otologic surgery (Singleton et al., 1987).
The third main theory of the pathophysiology of idiopathic SSNHL is that viral infection or viral reactivation within the inner ear causes cochlear inflammation and/or damage to critical inner ear structures. There are data from clinical, in vitro animal studies, and human temporal bone studies to support this etiology. Significant levels of serum antiviral antibodies, including antibodies to cytomegalovirus, herpes zoster, herpes simplex type 1, influenza B, mumps, enterovirus, and rubeola have been isolated from the serum of patients suffering from idiopathic SSNHL (Mentel, Kaftan, Wegner, Reissmann, & Gurtler, 2004; Wilson, Veltri, Laird, & Sprinkle, 1983). Temporal bones from patients with idiopathic SSNHL show histological patterns similar to those seen in viral labyrinthitis including atrophy of the organ of Corti, tectorial membrane, stria vascularis, and vestibular end organ (Schuknecht & Donovan, 1986). Labyrinthine and cochlear enhancement on magnetic resonance imaging (MRI) is a potential sign of inner ear inflammation and is seen in 3.8% to 9% of patients with idiopathic SSNHL (Chon et al., 2003; Fitzgerald & Mark, 1998; Stokroos, Albers, Krikke, & Casselman, 1998). Following resolution of hearing loss in two of 12 patients with initial enhancement in the cochlea or labyrinth, the inner ear enhancement on MRI was lost (Mark et al., 1992). Animal experiments have given further support to a viral etiology for idiopathic SSNHL. For instance, application of herpes simplex type 1 virus to the round window induced sensorineural hearing loss in guinea pigs (Stokroos, Albers, & Schirm, 1998). However, many difficulties with this etiology exist, including the following: SSNHL in humans due to known viral causes and caused by viral agents in animal experiments typically is severe and not reversible, and in animal models viruses cause progressive hearing loss (Mattox & Simmons, 1977; Merchant et al., 2008; Stokroos et al., 1998). Thus similar to other potential etiologies of idiopathic SSNHL, viral infection of inner ear structures may underlie some but not all cases of this disorder.
Natural History
Many of the discoverable causes of SSNHL cause permanent hearing loss due to damage to hair cells or other inner ear structures. In contrast, most patients with idiopathic SSNHL will regain some degree of hearing (Figure 3). Natural history and placebo-controlled studies have shown hearing recovery rates of 32% to 65% (average 46.7%) without treatment, typically within 2 weeks of onset (Byl, 1984 ; Mattox & Simmons, 1977; Nosrati-Zarenoe et al., 2007; Wilson et al., 1980). One study found that 45% of patients with idiopathic SSNHL spontaneously regained hearing levels in the affected ear within 10dB of the contralateral ear (Byl, 1984). Longer durations of hearing loss are associated with a decreased probability of hearing recovery, with deficits lasting more than 2-3 months likely becoming permanent (Byl, 1984; Fetterman et al., 1996; Nosrati-Zarenoe et al., 2007; Shaia & Sheehy, 1976; Simmons, 1973; Xenellis et al., 2006; Zadeh, Storper, & Spitzer, 2003). Rates of hearing recovery for idiopathic hearing loss are additionally affected by hearing loss severity, duration, and age at presentation, as discussed below (Byl, 1984; Shaia & Sheehy, 1976; Wilson et al., 1980; Nosrati-Zarenoe et al., 2007).

Audiograms of two patients presenting with idiopathic SSNHL. Both patients were women in their mid-40s who presented with complaints of SSNHL within less than 1 week of onset. Both patients were treated with 1mg/kg prednisone and oral antiherpetic medications for 10 days. Initial audiogram following onset of SSNHL for Patient 1 (A); follow-up audiogram at 2 weeks (B); initial audiogram following onset of SSNHL for Patient 2 (C); follow-up audiogram at 3 weeks for Patient 2 (D). SSNHL, sudden sensorineural hearing loss.
Evaluation
Patients presenting with SSNHL should undergo a workup to establish their diagnosis, obtain appropriate therapy, predict their prognosis for hearing recovery, and most importantly, to rule out an identifiable underlying cause of hearing loss.
Standard pure tone audiometry not only provides the criteria for diagnosis of SSNHL; characteristics of the initial audiogram have prognostic value as discussed below. Patients undergo a series of audiograms to document recovery, monitor treatment, guide aural rehabilitation, screen for relapse, and to rule out hearing loss in the contralateral ear. The Stenger test should be performed if malingering is suspected (Durmaz, Karahatay, Satar, Birkent, & Hidir, 2009). Auditory brainstem response testing (ABR) can be used to rule out a cerebellopontine angle (CPA) or internal auditory canal (IAC) lesion as a cause of unilateral hearing loss. ABR is particularly useful when MRI is not available or is contraindicated. However, the sensitivity of traditional ABR in diagnosing tumors is far lower than MRI (88% vs. 99%), and is substantially lower for tumors smaller than 1 cm in diameter (79%; Cueva, 2004; Fortnum et al., 2009). Stacked ABR has improved the sensitivity to 95% and specificity to 88% for tumors less than 1 cm in size, making it a more practical replacement for MRI (Don, Kwong, Tanaka, Brackmann, & Nelson, 2005). From a practical standpoint, ABR cannot be used to exclude vestibular schwannomas from all patients with SSNHL, as sufficient residual hearing must be present for the ABR response to be observed (thresholds of at least 75-80 dB or less; Borg & Lofqvist, 1982; Fortnum et al., 2009). Some authors recommend electronystagmography (ENG) for patients with idiopathic SSNHL to provide additional prognostic information (Danino et al., 1984; Laird & Wilson, 1983; Xenellis et al., 2006). However, in some studies, ENG results are either not predictive or not independently predictive factors and so the costs of the studies may not be justified for this purpose (Ben-David, 2002; Fetterman et al., 1996; Mattox & Simmons, 1977; Wilson et al., 1980).
The diagnostic evaluation of SSNHL can potentially include a number of serologic tests and radiographic studies. As these tests can be extremely low yield, questions of cost effectiveness of using a standard testing battery for patients with SSNHL have been advanced by several authors (Carrier & Arriaga, 1997; Daniels, Shelton, & Harnsberger, 1998; Heman-Ackah et al., 2010; Murphy & Selesnick, 2002; Raber, Dort, Sevick, & Winkelaar, 1997; Robinette, Bauch, Olsen, & Cevette, 2000; Rupa, Job, George, & Rajshekhar, 2003; Wilson et al., 2010). However, as noted above, many of the known causes of SSNHL can have broader health consequences for patients. Therefore, certain tests should be performed especially for patients with risk factors for the underlying condition.
Laboratory tests commonly ordered for patients with SSNHL include nonspecific markers of inflammation as well as tests for specific infections. Abnormal serum cholesterol or coagulation panels may suggest a vascular etiology. Autoimmune studies are performed to identify potential collagen-vascular, granulomatous, or rheumatologic causes of SSNHL. Alterations in the patient’s metabolism can be evaluated with serum studies.
Per U.S. Centers for Disease Control (CDC) recommendations, the first step in testing for Lyme disease is by enzyme-linked immunosorbent assay (ELISA) for Lyme antibodies, either by a total titer or separate IgG and IgM levels. Lyme disease is then confirmed by Western blot (CDC, 2010). However, although patients still have the characteristic erythema migrans, antibody testing may be falsely negative because there has not been enough time for antibody titers to rise (Steere, McHugh, Damle, & Sikand, 2008). For patients with characteristics of Lyme disease but without positive ELISA results, patients should be treated presumptively and then retested for anti-Lyme antibodies 3-4 weeks later (Steere et al., 2008). Alternatively, in cases with neurologic involvement but an unclear diagnosis, cerebrospinal fluid (CSF) should be obtained for cell counts and Lyme antibody titers as well as tests for other infectious agents (Wormser et al., 2006). Serum screening tests for syphilis including rapid plasma reagin (RPR) and venereal disease research laboratory (VDRL) tests may not be positive in cases of otosyphilis. Additionally, serum fluorescent treponemal antibody absorption (FTA-ABS) may not be positive in this disease (Yimtae, Srirompotong, & Lertsukprasert, 2007). In cases of SSNHL in which otosyphilis is high on the differential, particularly in patients with HIV disease, cerebrospinal fluid VDRL testing (CSF-VDRL) reactivity may be required to determine whether or not otosyphilis is the causative agent (Marra, 2009; Yimtae et al., 2007).
Markers of inflammation and autoimmune disease are often tested during serologic evaluation of patients with SSNHL. Erythrocyte sedimentation rate (ESR) is a nonspecific marker of inflammation. From 1.5% to 77% of patients (average 45.7%) with SSNHL have elevated ESR (Chang, Ho, & Kuo, 2005; Heman-Ackah et al., 2010; Kreppel, 1979; Mattox & Simmons, 1977; Suslu, Yilmaz, & Gursel, 2009b). ESR levels >30 have been associated with a poorer prognosis for hearing in several studies (Fetterman et al., 1996; Mattox & Simmons, 1977); although this association is not found in all studies that have examined ESR levels in patients with SSNHL (Chang et al., 2005; Suslu et al., 2009b). Elevated levels of two nonspecific markers for autoimmune disease, antinuclear antibody (ANA), and rheumatoid factor (RF) have been reported in 3% to 23% of patients presenting with SSNHL (Heman-Ackah et al., 2010; Suslu et al., 2009b). However, in one study, elevated ANA and RF levels were only identified patients with a known autoimmune disorder (Sjogrens), thus suggesting that these tests are only worthwhile in the setting of clinical suspicion in patients who do not have a prior diagnosis of autoimmune disease (Heman-Ackah et al., 2010). Other studies of markers of autoimmune disorders thought to be linked to hearing loss specifically, including heat shock protein 70 (hsp70) and specific antiinner ear antibodies have not shown that presence or absence of these markers is associated with hearing outcomes in idiopathic SSNHL (Soliman, 1997; Suslu et al., 2009a).
Practitioners often include serologic testing for markers of cardiovascular risk (lipid analysis and serum glucose) in the evaluation of idiopathic SSNHL. Thirty-five to 40% of patients with idiopathic SSNHL will have hypercholesterolemia (Aimoni et al., 2010; Cadoni et al., 2005; Heman-Ackah et al., 2010). Similarly, elevated blood glucose has been reported in approximately 37% of patients presenting with idiopathic SSNHL (Cadoni et al., 2005; Heman-Ackah et al., 2010). These tests may have previously been performed by the patient’s primary care physician, and do not need to be reordered for the purpose of identification of hypercholesterolemia or diabetes unless they are older than 6 months-1 year. From a practical standpoint, however, complete blood chemistries must be ordered within a month prior to an MRI in many U.S. centers, so often these will need to be reordered.
Thyroid dysfunction can be found in patients presenting with SSNHL, with one report of a 15% rate of hypothyroidism (Heman-Ackah et al., 2010; Narozny et al., 2006). Typically, modern evaluation of thyroid function begins with total TSH level as a screen, because it has a high negative predictive value (Kaplan, 1999). If an abnormal TSH level is found, the patient is typically referred back to their primary care providers or to an endocrinologist for further evaluation and treatment. Evaluation of low TSH levels (suspected hyperthyroidism) often includes a total triiodothyronine (T3) and free thyroxine (T4 level); whereas evaluation of high TSH levels (suspected hypothyroidism) will typically include a free T4 level (Kaplan, 1999).
A major component of the evaluation of SSNHL is radiographic evaluation of the internal auditory canal and cerebellopontine angle for tumors, including vestibular schwannomas and meningiomas. The sensitivity and specificity of MRI with gadolinium in the diagnosis of vestibular schwannoma is nearly 100% for tumors over 3 mm in diameter (Cueva, 2004; Fortnum et al., 2009). A total of 1% to 6% of patients with SSNHL on average will have positive findings on MRI (Chaimoff, Nageris, Sulkes, Spitzer, & Kalmanowitz, 1999; Chau et al., 2010; Fetterman et al., 1996; Fitzgerald & Mark, 1998; Nosrati-Zarenoe et al., 2010; Tucci et al., 2002). Contraindications to use of gadolinium include glomerular filtration rate <30 mL/min and nephrogenic systemic fibrosis (Thomsen, 2009). If use of gadolinium is contraindicated, a high-resolution MRI of the brain and brainstem, including, a constructive interference in the steady state (CISS) sequence can be performed instead, with an estimated sensitivity nearly 100% tumors over 5 mm (Fortnum et al., 2009). If MRI is contraindicated due to presence of ferromagnetic-implanted foreign bodies (implanted pacemakers, AICDs), and ocular metallic foreign bodies (Fortnum et al., 2009), a computed tomography scan (CT) of the head and temporal bones with IV contrast can be performed with reasonable sensitivity for tumors >1.5 cm (Cueva, 2004). If contrast cannot be used with the CT due to allergy, renal failure (CR > 2.5 mg/dL), myasthenia gravis or myeloma, then a CT of the brain and temporal bones without contrast can be performed, which typically can only detect tumors > 1.5 cm in diameter. Alternatively, in the presence of hearing thresholds <75dB, a stacked ABR could be performed (Don et al., 2005).
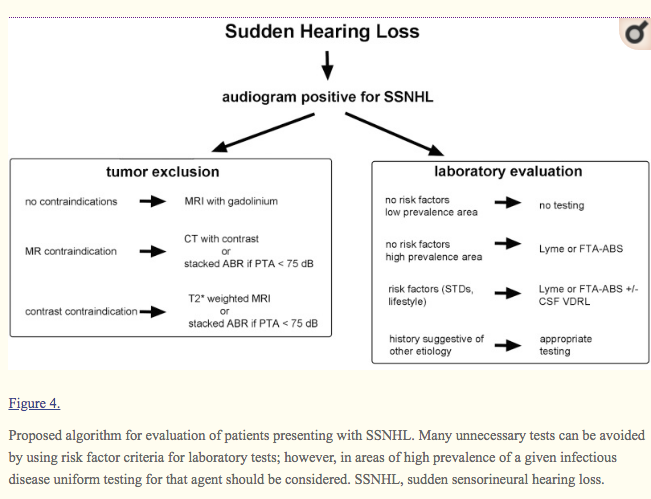
The number and type of tests ordered for the evaluation of SSNHL varies significantly between individual physicians and geographic location. A recent study of practice patterns in Sweden found that all of the 400 patients with SSNHL in the study had standard audiography, but only 65% and 40% underwent laboratory testing or MRI imaging, respectively, even when treated by otolaryngologists (Nosrati-Zarenoe et al., 2010). In comparison, a recent review of the diagnostic evaluation of 128 patients presenting with SSNHL presenting to a major U.S. medical center revealed the average number of diagnostic tests they received was six. Eighty-five percent of these patients underwent MRI with gadolinium (Heman-Ackah et al., 2010). For many tests, the likelihood of a positive result is extremely low, leading to a high cost per positive test finding (Heman-Ackah et al., 2010). Despite these results, ruling out treatable causes of SSNHL remains a critical part of the clinician’s evaluation. As a guideline for clinicians we have generated an algorithm for the evaluation of SSNHL (Figure 4). At the minimum, evaluation of patients with SSNHL should include a study to rule out vestibular schwannoma or other retrocochlear pathology as well as a laboratory evaluation for discernable causes of SSNHL directed by patient history and risk factors.

Proposed algorithm for evaluation of patients presenting with SSNHL. Many unnecessary tests can be avoided by using risk factor criteria for laboratory tests; however, in areas of high prevalence of a given infectious disease uniform testing for that agent should be considered. SSNHL, sudden sensorineural hearing loss.
Treatment
In cases in which a cause of SSNHL is discerned, the appropriate treatment for that condition is administered. A few reports have shown that hearing can potentially recover following therapy for a few conditions, including vestibular schwannoma, mumps, and secondary syphilis (Berg et al., 1986; Jeans, Wilkins, & Bonington, 2008; Vuori et al., 1962). Unfortunately, disease-specific therapy treatment does not improve hearing to preonset levels in the majority of SSNHL cases of identifiable etiology (Garcia Berrocal et al., 1999; Lorenzi et al., 2003; Nosrati-Zarenoe et al., 2010; Yimtae et al., 2007).
Controversy remains surrounding the necessity and options for treating idiopathic SSNHL. One of the bases of this ongoing debate is the fact that idiopathic SSNHL spontaneously resolves in 45% to 65% of patients (Byl, 1984; Mattox & Simmons, 1977). Numerous agents have been investigated for the treatment of idiopathic SSNHL including antiinflammatory agents, antimicrobials, calcium antagonists, vitamins, essential minerals, vasodilators, volume expanders, defibrinogenators, diuretics, hyperbaric oxygen, and bedrest (Conlin & Parnes, 2007). The number and variety of treatments results from the ongoing debate over the etiology of idiopathic SSNHL, the relative rarity of the condition, and the lack of a clearly superior therapy (Mattox & Simmons, 1977). Frequently, initially promising results are found in case series and small trials, but larger studies are either nonconclusive or show no significant improvement in hearing outcomes resulting from that therapy (Conlin & Parnes, 2007; Mattox & Simmons, 1977). Often the studies are nonrandomized and retrospective. Many do not clearly define clinical endpoints. Most studies are underpowered. For instance, estimating a spontaneous hearing recovery rate of 50% and an increased response rate for an effective therapy of 80% (alpha = .05), a study would require a total of 186 patients (93 cases and 93 controls) to complete therapy to have an 80% power. Despite these issues, in a survey of U.S. physicians, 100% of the otolaryngologists reported treating idiopathic SSNHL, whereas 97% of generalists either referred to an otolaryngologist for further treatment (71%) or treated the hearing loss themselves (26%; Shemirani, Schmidt, & Friedland, 2009). Similarly, 61% of 300 patients in Sweden with idiopathic SSNHL received treatment (Nosrati-Zarenoe et al., 2010).
When surveyed, 98% of U.S. otolaryngologists reported treating idiopathic SSNHL with oral steroids; additionally, 8% of otolaryngologists reported the use of intratympanic steroids (Shemirani et al., 2009). Corticosteroids are thought to improve idiopathic SSNHL by reducing inflammation and edema in the inner ear (Merchant et al., 2008; Wei, Mubiru, & O’Leary, 2006). An initial study combined the data from two separately administered double-blinded randomized controlled trials of a total of 67 patients using different corticosteroid regimens, finding an improved hearing recovery in patients receiving steroids (78%) compared to placebo (38%; Wilson et al., 1980). Subsequent attempts to replicate this study reveal inconsistent findings with regard to the benefit of corticosteroids in idiopathic SSNHL, and there are issues in terms of methodology with many of these trials (Cinamon, Bendet, & Kronenberg, 2001; Conlin & Parnes, 2007; Wei et al., 2006).
Intratympanic (IT) corticosteroids are being increasingly used frequently used in the management of idiopathic SSNHL. IT-steroid application leads to higher perilymph levels of steroids than systemic administration, at least in guinea pigs; however, IT steroids are not absorbed into the systemic circulation (Chandrasekhar et al., 2000). Initially, they were utilized mainly in the context of patients with contraindications to systemic steroid therapy and patients who have failed systemic steroid administration (Dallan et al., 2010; Ho, Lin, Shu, Yang, & Tsai, 2004; Hong, Park, & Lee, 2009; Plontke et al., 2009; She et al., 2010; Slattery, Fisher, Iqbal, Friedman, & Liu, 2005). Rausch and colleagues have recently shown that IT application of corticosteroids is not inferior to systemic steroids for idiopathic SSNHL with thresholds less than 70 dB HL (Rauch, Reda, & Halpin, 2010).
In a survey of 104 practicing otolaryngologists, 50% of respondents reported using antiherpetic therapy (acyclovir, famciclovir, etc.) in combination with corticosteroids for the treatment of idiopathic SSNHL despite lack of evidence of efficacy (Conlin & Parnes, 2007; Shemirani et al., 2009). Other therapeutic modalities, including “shotgun” approaches incorporating multiple modalities of treatment, are also frequently performed without good clinical evidence of their utility for idiopathic SSNHL.
Prognosis
Prognosis of SSNHL due to a discernable etiology depends heavily on that disease process, its duration, specific impact on cochlear structures, and treatment options (Berg et al., 1986; Byl, 1984; Jaffe, 1970; Jeans et al., 2008; Meyerhoff & Pollock, 1990; Narozny et al., 2006; Vuori et al., 1962; Westmore et al., 1979). In many such cases, hearing will not improve following appropriate therapy for the underlying pathologic process (Garcia Berrocal et al., 1999; Lorenzi et al., 2003; Nosrati-Zarenoe et al., 2010; Yimtae et al., 2007).
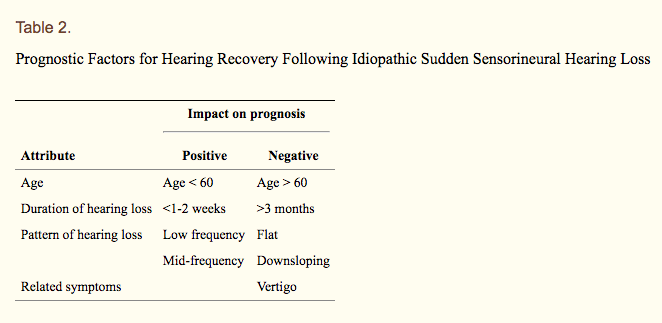
For idiopathic SSNHL, 45% to 65% of patients will regain their preloss hearing thresholds even without therapy, with average gains of 35 dB (Byl, 1984; Mattox & Simmons, 1977). The prognosis of idiopathic SSNHL depends on a variety of risk factors including demographics, duration of hearing loss, associated symptoms, and audiogram characteristics (Table 2). Of all demographic factors studied, advanced age (>60 years in most studies) has been universally correlated with decreased rates of hearing recovery and lower absolute threshold gains (Byl, 1984; Fetterman et al., 1996; Huy & Sauvaget, 2005; Laird & Wilson, 1983; Mattox & Lyles, 1989; Nosrati-Zarenoe et al., 2007; Shaia & Sheehy, 1976; Wilson et al., 1980; Xenellis et al., 2006; Zadeh et al., 2003). Byl (1984) additionally reported a poor prognosis in patients less than 15 years of age at presentation, although it is unclear how many patients in that study fall into that age group (Byl, 1984).
Table 2.
Prognostic Factors for Hearing Recovery Following Idiopathic Sudden Sensorineural Hearing Loss
| Impact on prognosis | ||
|---|---|---|
| Attribute | Positive | Negative |
| Age | Age < 60 | Age > 60 |
| Duration of hearing loss | <1-2 weeks | >3 months |
| Pattern of hearing loss | Low frequency | Flat |
| Mid-frequency | Downsloping | |
| Related symptoms | Vertigo | |
Generally patients with higher hearing thresholds on initial audiogram after SSNHL onset have a decreased rate of hearing recovery as compared to patients with mild losses (Byl, 1984; Laird & Wilson, 1983; Xenellis et al., 2006). Audiogram shape has been shown in many studies to impact hearing recovery, with higher rates of recovery found for low-frequency (63% to 88%) or mid-frequency (36% to 71%) hearing losses compared with flat (40% to 56%) or downsloping hearing loss (19% to 38%) (Chang et al., 2005; Huy & Sauvaget, 2005; Mattox & Simmons, 1977; Nosrati-Zarenoe et al., 2007; Shaia & Sheehy, 1976; Xenellis et al., 2006; Zadeh et al., 2003) (Figure 5).

Pure-tone audiogram configurations associated with different hearing outcomes following idiopathic SSNHL. Upsloping (A), flat (B), downsloping (C), and profound (D) configurations are shown with corresponding hearing recovery rates. SSNHL, sudden sensorineural hearing loss.
Presentation to a physician less than a week after onset of SSNHL also correlates with improved odds of hearing recovery, with chances of complete hearing recovery decreasing after that time. Rates of hearing recovery following audiogram within the first few days of onset is 87%, with a week, 87%, 2 weeks 52%, and 10% or less after 3 months (Byl, 1984; Fetterman et al., 1996; Nosrati-Zarenoe et al., 2007; Shaia & Sheehy, 1976; Simmons, 1973; Xenellis et al., 2006; Zadeh et al., 2003). Some authors have implied that this effect of longer duration between SSNHL onset and presentation to a physician indicates that earlier treatment leads to improved hearing outcomes; however, this effect is seen for a wide variety of types of treatments and in natural history studies. Thus, the negative prognosis associated with longer time between onset of SSNHL and presentation may be a reflection of the natural history of SSNHL. Sensorineural hearing loss of shorter duration is more likely to recover regardless of modality or timing of treatment (Mattox & Simmons, 1977).
Comorbid symptoms and signs have also been investigated as prognostic indicators for SSNHL. In some studies, patient complaints of imbalance or vertigo have been associated with a poorer prognosis for hearing recovery following SSNHL (Ben-David, Luntz, Podoshin, Sabo, & Fradis, 2002; Byl, 1984; Chang et al., 2005; Danino et al., 1984; Huy & Sauvaget, 2005; Laird & Wilson, 1983; Shaia & Sheehy, 1976), although this association was found to be insignificant in other studies (Fetterman et al., 1996; Nosrati-Zarenoe et al., 2007; Xenellis et al., 2006; Zadeh et al., 2003). Similarly, abnormalities on electronystagmography (ENG) have been associated with poorer hearing recovery in many (Danino et al., 1984; Laird & Wilson, 1983; Wilson et al., 1980; Xenellis et al., 2006) but not all studies in which they have been examined (Fetterman et al., 1996). In some studies, ENG effects on prognosis were only seen for patients with unfavorable audiograms (Ben-David et al., 2002; Mattox & Simmons, 1977); whereas in another, ENG abnormalities were not independently associated with hearing prognosis when other factors (age, degree of hearing loss) were included in the analysis (Wilson et al., 1980). Tinnitus on presentation with SSNHL has been identified as a negative prognostic indicator (Ben-David et al., 2002), a positive prognostic indicator (Danino et al., 1984), and as having no influence on outcomes in other studies (Chang et al., 2005; Nosrati-Zarenoe et al., 2007; Xenellis et al., 2006; Zadeh et al., 2003). Overall, vertigo, tinnitus, and ENG abnormalities appear to be less predictive of hearing outcomes than the other prognostic indicators listed above.
Some authors have attempted to develop algorithms combining multiple prognostic factors to yield a percentage likelihood of hearing recovery or an odds ratio for recovery for patients with different combinations of risk factors (Byl, 1984; Laird & Wilson, 1983; Mattox & Simmons, 1977). Although discernment of these numbers can be helpful in counseling patients regarding hearing recovery, effort must be taken to ensure that individual patients understand the meaning of numbers generated with respect to their own hearing prognosis. Thus a 90% chance of hearing recovery does not necessarily mean that individual patient will recover 90% of their hearing.
For patients with idiopathic SSNHL, the issue of the development of bilateral SSNHL is of great concern. In multiple studies, the prevalence of bilateral SSNHL is 2%, and this number includes patients with simultaneous bilateral onset (Byl, 1984; Fetterman et al., 1996; Huy & Sauvaget, 2005; Xenellis et al., 2006). Therefore patients can be reassured that the risk of sequential involvement of the contralateral ear is very low.
Conclusion
SSNHL is a common complaint in audiologic and otolaryngologic practice. Although most cases of SSNHL are idiopathic, a number of treatable conditions can underlie SSNHL. Efforts to discern these conditions should be part of the diagnostic evaluation. Prognosis for hearing recovery is based on several factors, including duration and degree of deafness, age, and vertigo. Although SSNHL will often spontaneously improve without treatment, directed therapy against discernable causes of SSNHL and corticosteroid therapy for idiopathic SSNHL are mainstays of the care of these patients.
Footnotes
Declaration of Conflicting Interests: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
References
- Aimoni C., Bianchini C., Borin M., Ciorba A., Fellin R., Martini A., . . . Volpato S. (2010). Diabetes, cardiovascular risk factors and idiopathic sudden sensorineural hearing loss: A case-control study. Audiology and Neurotology, 15(2), 111-115 [PubMed] [Google Scholar]
- Albers F. W., Demuynck K. M., Casselman J. W. (1994). Three-dimensional magnetic resonance imaging of the inner ear in idiopathic sudden sensorineural hearing loss. ORL; Journal of Oto-rhino-laryngology and its Related Specialities, 56(1), 1-4 [PubMed] [Google Scholar]
- Ballesteros F., Alobid I., Tassies D., Reverter J. C., Scharf R. E., Guilemany J. M., Bernal-Sprekelsen M. (2009). Is there an overlap between sudden neurosensorial hearing loss and cardiovascular risk factors? Audiology and Neurotology, 14(3), 139-145 [PubMed] [Google Scholar]
- Belal A., Jr. (1979). The effects of vascular occlusion on the human inner ear. Journal of Laryngology & Otology, 93, 955-968 [PubMed] [Google Scholar]
- Ben-David J., Luntz M., Podoshin L., Sabo E., Fradis M. (2002). Vertigo as a prognostic sign in sudden sensorineural hearing loss. International Tinnitus Journal, 8(2), 127-128 [PubMed] [Google Scholar]
- Berg H. M., Cohen N. L., Hammerschlag P. E., Waltzman S. B. (1986). Acoustic neuroma presenting as sudden hearing loss with recovery. Otolaryngology–Head and Neck Surgery, 94(1), 15-22 [PubMed][Google Scholar]
- Borg E., Lofqvist L. (1982). A lower audiometric limit for auditory brainstem response (ABR). Scandivanian Audiology, 11, 277-278 [PubMed] [Google Scholar]
- Byl F. M., Jr. (1984). Sudden hearing loss: Eeight years’ experience and suggested prognostic table. Laryngoscope, 94(5 Pt 1), 647-661 [PubMed] [Google Scholar]
- Cadoni G., Agostino S., Scipione S., Ippolito S., Caselli A., Marchese R., Paludetti G. (2005). Sudden sensorineural hearing loss: Our experience in diagnosis, treatment, and outcome. Journal of Otolaryngology, 34, 395-401 [PubMed] [Google Scholar]
- Capaccio P., Ottaviani F., Cuccarini V., Bottero A., Schindler A., Cesana B. M., . . . Pignataro L. (2007). Genetic and acquired prothrombotic risk factors and sudden hearing loss. Laryngoscope, 117, 547-551 [PubMed][Google Scholar]
- Carrier D. A., Arriaga M. A. (1997). Cost-effective evaluation of asymmetric sensorineural hearing loss with focused magnetic resonance imaging. Otolaryngology–Head and Neck Surgery, 116, 567-574 [PubMed][Google Scholar]
- Chaimoff M., Nageris B. I., Sulkes J., Spitzer T., Kalmanowitz M. (1999). Sudden hearing loss as a presenting symptom of acoustic neuroma. American Journal of Otolaryngology, 20, 157-160 [PubMed][Google Scholar]
- Chandrasekhar S. S., Rubinstein R. Y., Kwartler J. A., Gatz M., Connelly P. E., Huang E., Baredes S. (2000). Dexamethasone pharmacokinetics in the inner ear: Comparison of route of administration and use of facilitating agents. Otolaryngology–Head and Neck Surgery, 122, 521-528 [PubMed] [Google Scholar]
- Chang N. C., Ho K. Y., Kuo W. R. (2005). Audiometric patterns and prognosis in sudden sensorineural hearing loss in Southern Taiwan. Otolaryngology–Head and Neck Surgery, 133, 916-922 [PubMed][Google Scholar]
- Chau J. K., Lin J. R., Atashband S., Irvine R. A., Westerberg B. D. (2010). Systematic review of the evidence for the etiology of adult sudden sensorineural hearing loss. Laryngoscope, 120, 1011-1021 [PubMed][Google Scholar]
- Chon K. M., Goh E. K., Lee W. I., Lee B. J., Roh H. J., Wang S. G. (2003). Magnetic resonance imaging and sudden deafness. International Tinnitus Journal, 9(2), 119-123 [PubMed] [Google Scholar]
- Cinamon U., Bendet E., Kronenberg J. (2001). Steroids, carbogen or placebo for sudden hearing loss: A prospective double-blind study. European Archives of Oto-Rhino-Laryngology, 258, 477-480 [PubMed][Google Scholar]
- Colclasure J. B., Graham S. S. (1981). Intracranial aneurysm occurring as sensorineural hearing loss. Otolaryngology–Head and Neck Surgery, 89, 283-287 [PubMed] [Google Scholar]
- Conlin A. E., Parnes L. S. (2007). Treatment of sudden sensorineural hearing loss: I. A systematic review. Archives of Otolaryngology–Head & Neck Surgery, 133, 573-581 [PubMed] [Google Scholar]
- Cueva R. A. (2004). Auditory brainstem response versus magnetic resonance imaging for the evaluation of asymmetric sensorineural hearing loss. Laryngoscope, 114, 1686-1692 [PubMed] [Google Scholar]
- Dallan I., De Vito A., Fattori B., Casani A. P., Panicucci E., Berrettini S., . . . Nacci A. (2010). Intratympanic methylprednisolone in refractory sudden hearing loss: A 27-patient case series with univariate and multivariate analysis. Otology & Neurotology, 31(1), 25-30 [PubMed] [Google Scholar]
- Daniels R. L., Shelton C., Harnsberger H. R. (1998). Ultra high resolution nonenhanced fast spin echo magnetic resonance imaging: Cost-effective screening for acoustic neuroma in patients with sudden sensorineural hearing loss. Otolaryngology–Head and Neck Surgery, 119, 364-369 [PubMed] [Google Scholar]
- Danino J., Joachims H. Z., Eliachar I., Podoshin L., Ben-David Y., Fradis M. (1984). Tinnitus as a prognostic factor in sudden deafness. American Journal of Otolaryngology, 5, 394-396 [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention (Division of Vector Borne Infectious Diseases). (2010). Lyme disease diagnosis. Retrieved from http://www.cdc.gov/ncidod/dvbid/lyme/ld_humandisease_diagnosis.htm
- Don M., Kwong B., Tanaka C., Brackmann D., Nelson R. (2005). The stacked ABR: A sensitive and specific screening tool for detecting small acoustic tumors. Audiology and Neurotology, 10, 274-290 [PubMed][Google Scholar]
- Durmaz A., Karahatay S., Satar B., Birkent H., Hidir Y. (2009). Efficiency of Stenger test in confirming profound, unilateral pseudohypacusis. Journal of Laryngology & Otology, 123, 840-844 [PubMed][Google Scholar]
- Einer H., Tengborn L., Axelsson A., Edstrom S. (1994). Sudden sensorineural hearing loss and hemostatic mechanisms. Archives of Otolaryngology–Head & Neck Surgery, 120, 536-540 [PubMed] [Google Scholar]
- Fetterman B. L., Saunders J. E., Luxford W. M. (1996). Prognosis and treatment of sudden sensorineural hearing loss. American Journal of Otology, 17, 529-536 [PubMed] [Google Scholar]
- Fisch U., Nagahara K., Pollak A. (1984). Sudden hearing loss: Circulatory. American Journal of Otology, 5, 488-491 [PubMed] [Google Scholar]
- Fitzgerald D. C., Mark A. S. (1998). MRI in sudden sensorineural hearing loss. Otolaryngology–Head and Neck Surgery, 118, 737-738 [PubMed] [Google Scholar]
- Fortnum H., O’Neill C., Taylor R., Lenthall R., Nikolopoulos T., Lightfoot G., . . . Mulvaney C. (2009). The role of magnetic resonance imaging in the identification of suspected acoustic neuroma: A systematic review of clinical and cost effectiveness and natural history. Health Technology Assessment, 13(18), iii-iv, ix,-xi, 1-154 [PubMed] [Google Scholar]
- Garcia-Berrocal J. R., Gorriz C., Ramirez-Camacho R., Trinidad A., Ibanez A., Rodriguez Valiente A., Gonzalez J. A. (2006). Otosyphilis mimics immune disorders of the inner ear. Acta Oto-Laryngologica, 126, 679-684 [PubMed] [Google Scholar]