
beyond reason
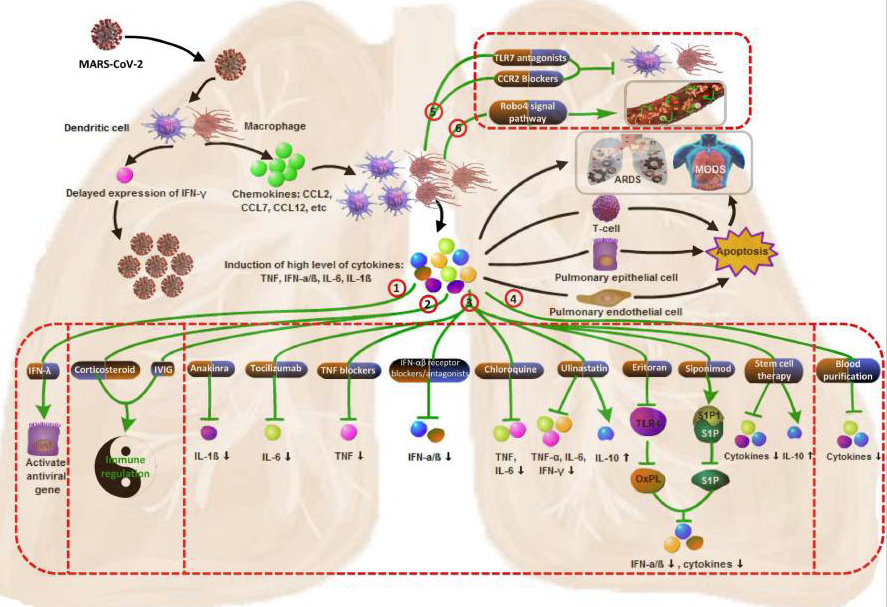
Mechanism of cytokine storm in COVID-19 and potential therapy.
① Supplement with IFN-λ to activate the innate immunity;
② Using immunomodulator to restore immune balance;
③ Inhibiting the production of cytokines;
④ Scavenging cytokines;
⑤ Inhibiting mononuclear macrophage recruitment and function;
⑥ Strengthening the vascular barrier by activating of the endothelial Slit-Robo4 signal pathway.
The pathogenesis and treatment of the `Cytokine Storm' in COVID-19
Summary
Cytokine storm is a general term applied to maladaptive cytokine release in response to infection and other stimuli. The pathogenesis is complex but includes loss of regulatory control of proinflammatory cytokine production, both at local and systemic levels. The disease progresses rapidly, and the mortality is high. Some evidence shows that, during the coronavirus disease 2019 (COVID-19) epidemic, severe deterioration in some patients has been closely associated with dysregulated and excessive cytokine release. This article reviews what we know of the mechanism and treatment strategies of the COVID-19 virus-induced inflammatory storm in an attempt to provide some background to inform future guidance for clinical treatment.
Keywords: Coronavirus, 2019-nCoV, SARS-CoV-2, Cytokine storm, Immunomodulation
Cytokine storm is a general term applied to maladaptive cytokine release in response to infection and other stimuli. The pathogenesis is complex but includes loss of regulatory control of proinflammatory cytokine production, both at local and systemic levels. The disease progresses rapidly, and the mortality is high. Some evidence shows that, during the coronavirus disease 2019 (COVID-19) epidemic, severe deterioration in some patients has been closely associated with dysregulated and excessive cytokine release. This article reviews what we know of the mechanism and treatment strategies of the COVID-19 virus-induced inflammatory storm in an attempt to provide some background to inform future guidance for clinical treatment.
Introduction
Severe acute respiratory syndrome corona virus 2 (SARS-CoV-2) emerged for the first time in Wuhan, China, in December 2019. It is a type of highly pathogenic human coronavirus (HCoV) that causes zoonotic diseases and poses a major threat to public health. The vast majority of patients with the coronavirus disease 2019 (COVID-19) have had a good prognosis, but there were still some critical individuals and even deaths.1
Most of these critically ill and dead patients did not develop severe clinical manifestations in the early stages of the disease. Some of the patients only showed mild fever, cough, or muscle soreness. The conditions of these patients deteriorated suddenly in the later stages of the disease or in the process of recovery. Acute respiratory distress syndrome (ARDS) and multiple-organ failure occurred rapidly, resulting in death within a short time.2 Cytokine storm is considered to be one of the major causes of ARDS and multiple-organ failure.3 It plays an important role in the process of disease aggravation.4Clinical studies have detected a cytokine storm in critical patients with COVID-19. Therefore, effectively suppressing the cytokine storm is an important way to prevent the deterioration of patients with COVID-19 infection and save the patients' lives.5 This article reviews the mechanisms by which HCoV infection induces cytokine storm and the options to inhibit the cytokine storm, in order to provide a reference for the clinical diagnosis and treatment of COVID-19.
HCoVs
Coronaviruses (CoVs) are single-stranded, positive-strand RNA viruses belonging to the Coronaviridae family, Nidovirales order. The International Committee on Taxonomy of Viruses (ICTV) classifies the CoVs into four categories: α, β, γ, and δ. Under the electron microscope, the virus particles display a rough spherical or multi-faceted crystal shape. The surface of the viruses has prominent club-shaped projections composed of its spike protein. Inside the virus particle is the viral genome wrapped in a nucleocapsid. The viral genome contains approximately 26,000 to 32,000 bases. CoVs are the largest known RNA viruses. The positive-strand viral RNA consists of a cap structure at the 5′ end and multiple poly(A) tails at the 3′ end. It serves as messenger RNA (mRNA), allowing the translation of replicase/transcriptase and viral structural proteins. The replicase/transcriptase genes account for approximately 2/3 of the 5′-end RNA sequence and are composed of two overlapping open reading frames (ORFs): ORF1a and ORF1b. The ORFs encode 16 non-structural proteins. The remaining 1/3 of the RNA sequence encodes four classical viral structural proteins, namely, spike (S) protein, envelope (E) protein, membrane (M) protein, and nucleocapsid (N) protein. In addition, genes encoding some viral accessory proteins are interspersed in the coding regions of the viral structural proteins. The coding sites and number of these accessory protein genes are an important basis for CoV classification. CoVs can infect a variety of host species, including birds, humans and some other vertebrates. These viruses mainly cause respiratory and intestinal infections and induce a variety of clinical manifestations.6 , 7
Coronaviruses have long been recognized as important pathogens that infect the respiratory tracts of domestic and companion animals and are the causes of mild and severe respiratory diseases in humans.7 , 8So far, seven HCoVs that can invade humans have been identified, including the α-type HCoV-229E and HCoV-NL63; the β-type HCoV-HKU1, SARS-CoV, MERS-CoV, and HCoV-OC43; and 2019-nCoV, causing the present epidemic. According to their pathogenicity, HCoVs are divided into mildly pathogenic HCoVs (including HCoV-229E, HCoV-OC43, HCoV-NL63, and HCoV-HKU) and highly pathogenic CoVs (including severe acute respiratory syndrome CoV (SARS-CoV),9 Middle East respiratory syndrome coronavirus (MERS-CoV) 10 , 11 and SARS-CoV-2). The mildly pathogenic HCoVs infect the upper respiratory tract and cause seasonal, mild to moderate cold-like respiratory diseases in healthy individuals. In contrast, the highly pathogenic HCoVs (hereinafter referred to as pathogenic HCoVs or HCoVs) infect the lower respiratory tract and cause severe pneumonia, sometimes leading to fatal acute lung injury (ALI) and ARDS. The pathogenic HCoVs have high morbidity and mortality and pose a major threat to public health.12, 13, 14
Mechanism of cytokine storm by pathogenic HCoV infection
It has long been believed that cytokines play an important role in immunopathology during viral infection. A rapid and well-coordinated innate immune response is the first line of defense against viral infection. However, dysregulated and excessive immune responses may cause immune damage to the human body.15, 16, 17 The relevant evidences from severely ill patients with HCoVs suggest that proinflammatory responses play a role in the pathogenesis of HCoVs. In vitro cell experiments show that delayed release of cytokines and chemokines occurs in respiratory epithelial cells, dendritic cells (DCs), and macrophages at the early stage of SARS-CoV infection. Later, the cells secrete low levels of the antiviral factors interferons (IFNs) and high levels of proinflammatory cytokines (interleukin (IL)-1β, IL-6, and tumor necrosis factor (TNF)) and chemokines (C-C motif chemokine ligand (CCL)-2, CCL-3, and CCL-5).18, 19, 20 Like SARS, MERS-CoV infects human airway epithelial cells, THP-1 cells (a monocyte cell line), human peripheral blood monocyte-derived macrophages and DCs, and induces delayed but elevated levels of proinflammatory cytokines and chemokines.21 , 22 After MERS-CoV infection, plasmacytoid dendritic cells, but not mononuclear macrophages and DCs,23 are induced to produce a large amount of IFNs.
Serum cytokine and chemokine levels are significantly higher in patients with severe MERS than patients with mild to moderate MERS.24 , 25 The elevated serum cytokine and chemokine levels in MERS patients are related to the high number of neutrophils and monocytes in the patients’ lung tissues and peripheral blood, suggesting that these cells may play a role in lung pathology.24, 25, 26 Similar phenomena have been observed in patients with SARS-CoV infection.27, 28, 29, 30, 31, 32, 33, 34 The production of IFN-I or IFN-α/β is the key natural immune defense response against viral infections, and IFN-I is the key molecule that plays an antiviral role in the early stages of viral infection.35 , 36 Delayed release of IFNs in the early stages of SARS-CoV and MERS-CoV infection hinders the body's antiviral response.36 Afterward, the rapidly increased cytokines and chemokines attract many inflammatory cells, such as neutrophils and monocytes, resulting in excessive infiltration of the inflammatory cells into lung tissue and thus lung injury. It appears from these studies that dysregulated and/or exaggerated cytokine and chemokine responses by SARS-CoV-infected or MERS-CoV-infected cells could play an important role in pathogenesis of SARS or MERS.
Animal models can well elucidate the role of cytokines and chemokines in mediating pulmonary immunopathology after HCoV infection. Despite of similar virus titers in the respiratory tract, SARS-CoV-infected old nonhuman primates are more likely to develop immune dysregulation than the infected young primates, leading to more severe disease manifestations.37 It seems that the excessive inflammatory response rather than the virus titer is more relevant to the death of the old nonhuman primates.37 Similarly, in BALB/c mice infected with SARS-CoV, disease severity in old mice is related to the early and disproportionately strong upregulation of the ARDS-related inflammatory gene signals.38 The rapid replication of SARS-CoV in BALB/c mice induces the delayed release of IFN-α/β, which is accompanied by the influx of many pathogenic inflammatory mononuclear macrophages.15 The accumulated mononuclear macrophages receive activating signals through the IFN-α/β receptors on their surface and produce more monocyte chemoattractants (such as CCL2, CCL7, and CCL12), resulting in the further accumulation of mononuclear macrophages. These mononuclear macrophages produce elevated levels of proinflammatory cytokines (TNF, IL-6, IL1-β, and inducible nitric oxide synthase), thereby increasing the severity of the disease. Depleting inflammatory monocyte-macrophages or neutralizing the inflammatory cytokine TNF protected mice from the fatal SARS-CoV infection. In addition, IFN-α/β or mononuclear macrophage-derived proinflammatory cytokines induce the apoptosis of T cells, which further hinders viral clearance.15 Another consequence of rapid viral replication and vigorous proinflammatory cytokine/chemokine response is the induction of apoptosis in lung epithelial and endothelial cells. IFN-αβ and IFN-γ induce inflammatory cell infiltration through mechanisms involving Fas–Fas ligand (FasL) or TRAIL–death receptor 5 (DR5) and cause the apoptosis of airway and alveolar epithelial cells.39, 40, 41Apoptosis of endothelial cells and epithelial cells damages the pulmonary microvascular and alveolar epithelial cell barriers and causes vascular leakage and alveolar edema, eventually leading to hypoxia in the body. Therefore, inflammatory mediators play a key role in the pathogenesis of ARDS.
ARDS is the leading cause of death in patients infected with SARS-CoV or MERS-CoV.42 , 43 It is now known that several proinflammatory cytokines (IL-6, IL-8, IL-1β, granulocyte-macrophage colony-stimulating factor, and reactive oxygen species) and chemokines (such as CCL2, CCL-5, IFNγ-induced protein 10 (IP-10), and CCL3) all contribute to the occurrence of ARDS.44, 45, 46 These results support such points of view that, following SARS-CoV infection, high virus titers and dysregulation of cytokine/chemokine response cause an inflammatory cytokine storm. The inflammatory cytokine storm is accompanied by immunopathological changes in the lungs.
The relationship between cytokine levels and disease progression in patients
High levels of expression of IL-1B, IFN-γ, IP-10, and monocyte chemoattractant protein 1 (MCP-1) have been detected in patients with COVID-19. These inflammatory cytokines may activate the T-helper type 1 (Th1) cell response.47 Th1 activation is a key event in the activation of specific immunity.48 However, unlike SARS patients, patients with COVID-19 also have elevated levels of Th2 cell-secreted cytokines (such as IL-4 and IL-10), which inhibit the inflammatory response. The serum levels of IL-2R and IL-6 in patients with COVID-19 are positively correlated with the severity of the disease (i.e., critically ill patients > severely ill patients > ordinary patients).49 Other studies have found that, compared with COVID-19 patients from general wards, patients in the intensive care unit (ICU) display increased serum levels of granulocyte colony-stimulating factor, IP-10, MCP-1, macrophage inflammatory protein-1A, and TNF-α. The above studies suggest that the cytokine storm is positively correlated with disease severity.47
A report on the severe new-type coronavirus-infected pneumonia showed that 37 patients (71.2%) required mechanical ventilation, and 35 patients (67.3%) suffered ARDS. Moreover, the mortality of the elderly patients with ARDS was significantly elevated.50 The core pathological change in ARDS is the pulmonary and interstitial tissue damage caused by nonspecific inflammatory cell infiltration.51 Local excessive release of cytokines is the decisive factor that induces this pathological change and clinical manifestation.52 In COVID-19, the inflammatory cytokine storm is closely related to the development and progression of ARDS. The serum levels of cytokines are significantly increased in patients with ARDS, and the degree of increase is positively correlated with mortality rate.53 The cytokine storm is also a key factor in determining the clinical course of extrapulmonary multiple-organ failure.54 This partially explains the signs of extrapulmonary organ failure (such as elevated liver enzymes and creatinine) seen in some COVID-19 patients without respiratory failure, suggesting that the inflammatory cytokine storm is the cause of damage to extrapulmonary tissues and organs.
In summary, the new-type coronavirus infection causes an inflammatory cytokine storm in patients. The cytokine storm leads to ARDS or extrapulmonary multiple-organ failure and is an important factor that causes COVID-19 exacerbation or even death.
Theoretical treatment strategy with inflammatory cytokine storm
High virus titer and the subsequent strong inflammatory cytokine and chemokine responses are related to the high morbidity and mortality observed during the pathogenic HCoV infection. The experience from treating SARS and MERS shows that reducing viral load through interventions in the early stages of the disease and controlling inflammatory responses through immunomodulators are effective measures to improve the prognosis of HCoV infection.55, 56, 57, 58
IFN-λ
IFN-λ primarily activates epithelial cells and reduces the mononuclear macrophage-mediated proinflammatory activity of IFN-αβ.59 In addition, IFN-λ inhibits the recruitment of neutrophils to the sites of inflammation.60 SARS-CoV and MERS-CoV mainly infect alveolar epithelial cells (AEC). IFN-λ activates the antiviral genes in epithelial cells, thereby exerting antiviral effects without overstimulating the human immune system. Therefore, IFN-λ may be an ideal treatment. Some studies have applied pegylated and non-pegylated interferons for the treatment of HCoVs, but the efficacy varied significantly due to the application of different treatment regimens. Early administration of interferons has certain benefits in reducing viral load and improves the clinical symptoms of patients to a certain extent. However, it fails to reduce mortality rates.61, 62, 63 With the exception of early administration, the use of interferons at other time periods will not bring more benefits than placebo treatment.63
Corticosteroid therapies
Corticosteroids are a class of steroid hormones that have anti-inflammatory functions. Corticosteroids are commonly used to suppress inflammation. During the 2003 SARS epidemic, corticosteroids were the primary means of immunomodulation. Timely administration of corticosteroids often leads to early improvements such as reducing fever, relieving radiation infiltration of the lung, and improving oxygenation.64, 65, 66 A retrospective study of 401 patients with severe SARS revealed that proper administration of glucocorticoids in patients with severe SARS significantly reduced the mortality rate and shortened the hospital stay. Moreover, secondary infections and other complications rarely occurred in these glucocorticoid-treated patients.67 However, there are studies showing that administration of corticosteroid therapy during human SARS-CoV infection led to adverse consequences. Early treatment of SARS patients with corticosteroids increased plasma viral load in non-ICU patients, resulting in the aggravation of the disease.64
In treatment of patients with COVID-19, the use of glucocorticoids has again become a major conundrum for clinicians.68 The timing of administration and the dosage of glucocorticoids are very important to the outcome of the severely ill patients. A too early administration of glucocorticoids inhibits the initiation of the body's immune defense mechanism, thereby increasing the viral load and ultimately leading to adverse consequences. Therefore, glucocorticoids are mainly used in critically ill patients suffering inflammatory cytokine storm. Inhibition of excessive inflammation through timely administration of glucocorticoids in the early stage of inflammatory cytokine storm effectively prevents the occurrence of ARDS and protects the functions of the patients’ organs. For patients with progressive deterioration of oxygenation indicators, rapid imaging progress, and excessive inflammatory response, the use of glucocorticoid in the short term (3–5 days) is appropriate, and the recommended dose is no more than equivalent to methylprednisolone 1–2 mg/kg/day.69 It should be noted that large doses of glucocorticoid may delay the clearance of coronavirus due to immunosuppression.
Intravenous immunoglobulin (IVIG)
Chen et al. analyzed the treatment of 99 Wuhan patients with COVID-19 and found that 27% of these patients had received IVIG treatment.70 IVIG therapy has the dual effects of immune substitution and immunomodulation. Its practical application value in treatment of COVID-19 needs confirmation in future studies.
IL-1 family antagonists
During the cytokine storm, the three most important cytokines in the IL-1 family are IL-1β, IL-18, and IL-33.4 Studies that focus on the inhibition of IL-1β to reduce the cytokine storm have attracted most attention. Anakinra, an antagonist of IL-1β, can be used to treat the cytokine storm caused by infection. It significantly improved the 28-day survival rate of patients with severe sepsis.71 There is currently no clinical experience with applying specific IL-1 family blockers to treat COVID-19. Their effects need to be verified through in vivo animal experiments and clinical trials.
IL-6 antagonists
Tocilizumab is an IL-6 antagonist that suppresses the function of the immune system. Currently, tocilizumab is mainly applied in autoimmune diseases such as rheumatoid arthritis.72 Tocilizumab itself has a therapeutic effect on the infection-induced cytokine storm.73 Serum IL-6 level is significantly increased in severely ill patients with COVID-19. Clinical studies from China have shown that Tocilizumab is effective in treating severely ill patients with extensive bilateral lung lesions, who have elevated IL-6 levels. The first dose was 4–8 mg/kg. The recommended dosage was 400mg with 0.9% saline diluted to 100 ml. The infusion time was more than 1 h. For patients with poor efficacy of the first dose, an additional dose can be applied after 12 h (the dose is the same as before), with a maximum of two cumulative dose.
TNF blockers
TNFs are key inflammatory factors that trigger a cytokine storm. They are attractive targets for controlling the cytokine storm. A meta-analysis showed that anti-TNF therapy has significantly improved survival in patients with sepsis.74 Anti-TNF therapy has also achieved satisfactory outcomes in treatment of noninfectious diseases such as atherosclerosis.75 Studies in animal models have shown that TNFs contribute significantly to acute lung injury and impair the T cell response in SARS-CoV-challenged mice. In mice, neutralization of TNF activity or loss of TNF receptor provides protection against SARS-CoV-induced morbidity and mortality.15 , 76 However, it should be noted that, at least in the later stages of infection, TNF has not been detected in the serum of patients with SARS. At present, TNF blockers have not been suggested in the treatment of patients with COVID-19, but the efficacy of TNF blockers in treatment of patients with COVID-19 deserves further exploration.
IFN-αβ inhibitors
IFN-αβ limits viral replication by inducing IFN-stimulated gene. However, IFN-αβ also exacerbates diseases through enhancing the recruitment and function of mononuclear macrophages and other innate immune cells. Although an early interferon response has a protective effect on mice infected with SARS-CoV, delayed IFN-αβ signaling causes an imbalance of the anti-SARS-CoV immune responses in humans. This phenomenon indicates that the timing of IFN treatment is crucial to the outcome of diseases. Based on these results, IFN-αβ receptor blockers or antagonists should be administered in the later stages of severe disease to prevent excessive inflammatory responses.16
Chloroquine
Chloroquine inhibits the production and release of TNF and IL-6, which indicates that chloroquine may suppress the cytokine storm in patients infected with COVID-19.77 Chloroquine phosphate has been used in the treatment of adults aged 18 to 65 in China.78 The recommended dosage by diagnosis and treatment of new coronavirus pneumonia (trial version 7) from china is as follows: If the weight is more than 50 kg, 500 mg each time, 2 times a day, 7 days as a treatment course; If the weight is less than 50 kg, 500 mg each time on the first and second days, twice a day, 500 mg each time on the third to seventh days, once a day.
Ulinastatin
Ulinastatin is a natural anti-inflammatory substance in the body. It protects the vascular endothelium by inhibiting the production and release of inflammatory mediators. Ulinastatin is widely used in clinical practice to treat pancreatitis and acute circulatory failure. Ulinastatin reduces the levels of proinflammatory factors such as TNF-α, IL-6, and IFN-γ, and increases the level of anti-inflammatory factor IL-10.79 These activities of ulinastatin promote the balance between proinflammatory and anti-inflammatory responses in humans, thus interrupting the cytokine storm induced by the vicious cycle of inflammation. Animal studies show that the anti-inflammatory effect of high-dose ulinastatin is equivalent to that of hormones.80However, unlike glucocorticoids, ulinastatin does not inhibit immune functions and is unlikely to cause sequelae such as femoral head necrosis. Therefore, ulinastatin has great application prospects in the treatment of COVID-19.
The inhibitory effect of oxidized phospholipids (OxPL)
In a mouse model of influenza A virus (IAV) infection, OxPL increases the production of cytokines/chemokines in lung macrophages through the Toll-like receptor 4 (TLR4)–TIR-domain-containing adapter-inducing interferon-β signaling pathway, thereby promoting the occurrence of ALI.81Eritoran is a TLR4 antagonist. It does not have direct antiviral activity but has strong immunomodulatory functions. Eritoran effectively lowers the production of OxPL, inflammatory cytokines, and chemokines in IAV-infected mice, thereby reducing death.82 Pathogenic human coronaviruses also cause a high accumulation of OxPL in patients' lung tissues, resulting in ALI.81 Thus, it seems that eritoran and other OxPL inhibitors may also be able to alleviate HCoV-induced inflammatory responses.
Sphingosine-1-phosphate receptor 1 agonist therapy
Sphingosine-1-phosphate (S1P) is a signal lysophospholipid that promotes cytokine synthesis and secretion.83 The S1P receptor signaling pathways significantly inhibit the pathological damage induced by the host's innate and adaptive immune responses, thereby reducing the cytokine storm caused by influenza virus infection.84 , 85 In mouse models of IAV infection, sphingosine-1-phosphate receptor 1 (S1P1) signal transduction in respiratory endothelial cells modulates pathogenic inflammatory responses.85 Agonists targeting S1P1 inhibit excessive recruitment of inflammatory cells, inhibit proinflammatory cytokines and chemokines, and reduce the morbidity and mortality of IAV.85 , 86 SARS-CoV-2 also mainly infects human lung epithelial cells and endothelial cells. Therefore, S1P1 agonists may be potential therapeutic drugs for reducing cytokine and chemokine responses in those HCoV patients whose cells generated excessive immune responses. An S1P-receptor modulating drug, siponimod, was approved in 2019 to treat multiple sclerosis. However, clinical trials are needed to further verify whether siponimod is an ideal alternative for the treatment of cytokine storm.
Stem cell therapy
As an important member of the stem cell family, mesenchymal stem cells (MSC) not only have the potential of self-renewal and multidirectional differentiation, but also have strong anti-inflammatory and immune regulatory functions. MSC can inhibit the abnormal activation of T lymphocytes and macrophages, and induce their differentiation into regulatory T cell (Treg) subsets and anti-inflammatory macrophages, respectively. It can also inhibit the secretion of pro-inflammatory cytokines, such as, IL-1, TNF-α, IL-6, IL-12, and IFN-γ, thereby reducing the occurrence of cytokine storms.87 , 88 At the same time, MSC can secrete IL-10, hepatocyte growth factor, keratinocyte growth factor and VEGF to alleviate ARDS, regenerate and repair damaged lung tissues, and resist fibrosis.89 Therefore, many functions of MSC are expected to make it an effective method for the treatment of COVID-19.
Blood purification treatments
In addition, the blood purification treatments currently used in clinic practice can remove inflammatory factors to a certain extent. Blood purification system including plasma exchange, adsorption, perfusion, blood/plasma filtration, etc., can remove inflammatory factors, block the "cytokine storm", to reduce the damage of inflammatory response to the body. This therapy can be used for severe and critical patients in the early and middle stages of the disease. The artificial liver technology led by Academician Li Lanjuan can eliminate inflammatory factors on a large scale. This technology has also been used to resist the cytokine storm of H7N9, and its application on COVID-19 has also achieved certain efficacy.90 Early renal replacement therapy, which is similar to the treatment principle of artificial liver technology, seems to be an effective method to control cytokine storm.91
Inhibitors of mononuclear macrophage recruitment and function
An autopsy report of patients with COVID-19 revealed a large amount of inflammatory cell infiltration in the lungs of the deceased.92 One potentially effective treatment approach is to reduce the recruitment of mononuclear macrophages to the site of inflammation through small interfering RNA (siRNA)-mediated silencing of C-C chemokine receptor type 2 (CCR2), which has been demonstrated by animal experiments to improve the outcome of the disease.93 , 94 Toll-like receptor 7 (TLR7) agonists stimulate mononuclear macrophages to undergo a strong inflammatory response at the time of infection with single-stranded RNA (ssRNA) viruses such as HCoV. Therefore, TLR7 antagonists may be able to alleviate the storm of inflammatory factors caused by SARS-CoV-2 infection.
Strengthens the vascular barrier
Increased vascular permeability is also a hallmark change that occurs in the process of a cytokine storm. It was found in animal infection models of sepsis and H5N1 virus that activation of the endothelial Slit-Robo4 pathway with drugs improved vascular permeability, thereby reducing the occurrence of a cytokine storm during infection.95
Conclusion
Inflammation is an essential part of an effective immune response. It is difficult to eliminate infections successfully without inflammation. The inflammatory response begins with an initial recognition of pathogens. The pathogens then mediate the recruitment of immune cells, which eliminates the pathogens and ultimately leads to tissue repair and restoration of homeostasis. However, SARS-CoV-2 induces excessive and prolonged cytokine/chemokine responses in some infected individuals, known as the cytokine storm. Cytokine storm causes ARDS or multiple-organ dysfunction, which leads to physiological deterioration and death. Timely control of the cytokine storm in its early stage through such means as immunomodulators and cytokine antagonists, as well as the reduction of lung inflammatory cell infiltration, is the key to improving the treatment success rate and reducing the mortality rate of patients with COVID-19. Fig. 1

Mechanism of cytokine storm in COVID-19 and potential therapy.
① Supplement with IFN-λ to activate the innate immunity; ② Using immunomodulator to restore immune balance; ③ Inhibiting the production of cytokines; ④ Scavenging cytokines; ⑤ Inhibiting mononuclear macrophage recruitment and function; ⑥ Strengthening the vascular barrier by activating of the endothelial Slit-Robo4 signal pathway.
Declaration of Competing Interest
The authors declare that they have no competing financial interests.
Contributors
QY led the writing of the manuscript. JHM developed the initial concept and framework for the manuscript and oversaw the drafting of the manuscript. All authors contributed to the content, drafting, and critical review of the manuscript.
Funding
This study was supported by Zhejiang University special scientific research fund for COVID-19 prevention and control.