https://www.cell.com/trends/neurosciences/fulltext/S0166-2236(19)30175-4
Microglia in neurodegenerative diseases: mechanism and potential therapeutic targets
- Review Article
- Open access
- Published: 22 September 2023
Microglia in neurodegenerative diseases: mechanism and potential therapeutic targets
Signal Transduction and Targeted Therapy volume 8, Article number: 359 (2023) Cite this article
Abstract
Microglia activation is observed in various neurodegenerative diseases. Recent advances in single-cell technologies have revealed that these reactive microglia were with high spatial and temporal heterogeneity. Some identified microglia in specific states correlate with pathological hallmarks and are associated with specific functions. Microglia both exert protective function by phagocytosing and clearing pathological protein aggregates and play detrimental roles due to excessive uptake of protein aggregates, which would lead to microglial phagocytic ability impairment, neuroinflammation, and eventually neurodegeneration. In addition, peripheral immune cells infiltration shapes microglia into a pro-inflammatory phenotype and accelerates disease progression. Microglia also act as a mobile vehicle to propagate protein aggregates. Extracellular vesicles released from microglia and autophagy impairment in microglia all contribute to pathological progression and neurodegeneration. Thus, enhancing microglial phagocytosis, reducing microglial-mediated neuroinflammation, inhibiting microglial exosome synthesis and secretion, and promoting microglial conversion into a protective phenotype are considered to be promising strategies for the therapy of neurodegenerative diseases. Here we comprehensively review the biology of microglia and the roles of microglia in neurodegenerative diseases, including Alzheimer’s disease, Parkinson’s disease, multiple system atrophy, amyotrophic lateral sclerosis, frontotemporal dementia, progressive supranuclear palsy, corticobasal degeneration, dementia with Lewy bodies and Huntington’s disease. We also summarize the possible microglia-targeted interventions and treatments against neurodegenerative diseases with preclinical and clinical evidence in cell experiments, animal studies, and clinical trials.
초록
다양한 신경퇴행성 질환에서
미세아교세포 활성화가 관찰된다.
최근 단일 세포 기술의 발전으로
이러한 반응성 미세아교세포가 높은 공간적·시간적 이질성을 지닌다는 사실이 밝혀졌다.
특정 상태의 일부 미세아교세포는
병리학적 특징과 연관되며 특정 기능과 관련이 있다.
미세아교세포는
병리적 단백질 응집체를 식균 및 제거함으로써 보호 기능을 발휘하는 동시에,
과도한 단백질 응집체 흡수로 인해
미세아교세포의 식균 능력 저하, 신경염증,
그리고 궁극적으로 신경퇴행을 초래하는 해로운 역할을 수행한다.
또한,
말초 면역 세포의 침윤은
미세아교세포를 친염증성 표현형으로 변화시키고
질병 진행을 가속화한다.
미세아교세포는
또한 단백질 응집체를 전파하는 이동 수단 역할을 한다.
미세아교세포에서 분비되는 세포외 소포와 미세아교세포의 자가포식 장애는
모두 병리적 진행과 신경퇴행에 기여한다.
따라서
미세아교세포의 식세포작용 강화,
미세아교세포 매개 신경염증 감소,
미세아교세포 엑소좀 합성 및 분비 억제,
미세아교세포의 보호형 표현형 전환 촉진은
신경퇴행성 질환 치료를 위한 유망한 전략으로 간주된다.
enhancing microglial phagocytosis,
reducing microglial-mediated neuroinflammation,
inhibiting microglial exosome synthesis and secretion, and
promoting microglial conversion into a protective phenotype
are considered to be promising strategies for the therapy of neurodegenerative diseases
본고에서는
미세아교세포의 생물학적 특성과 알츠하이머병,
파킨슨병,
다계통 위축증,
근위축성 측삭경화증,
전두측두엽 치매,
진행성 초핵성 마비,
피질기저부 퇴행,
루이체 치매,
헌팅턴병 등
신경퇴행성 질환에서의 역할을 포괄적으로 검토한다.
또한 세포 실험, 동물 연구 및 임상 시험에서 전임상 및 임상적 증거를 바탕으로 한
신경퇴행성 질환에 대한 미세아교세포 표적 개입 및 치료법 가능성을 요약한다.
Similar content being viewed by others

Microglia-driven inflammation induces progressive tauopathies and synucleinopathies
Article Open access01 May 2025

Article Open access27 July 2023
Article Open access29 October 2021
Introduction
Microglia, the resident macrophages of the central nervous system (CNS), utilize their specific receptor repertoire to monitor the microenvironment dynamically in the brain.1 Microglia phagocytose misfolded proteins, cellular debris, and dying cells to maintain homeostasis.2 Additionally, microglia could monitor and protect neuronal functions through microglia-neuron crosstalk.3
Microglia have long been considered homogenous cells that respond uniformly to their surroundings. Nevertheless, recent developments in single-cell technologies have revealed multiple microglial states in human and mouse brains related to specific developmental, aging, and disease processes.4 For example, single-cell RNA-seq (scRNA-seq) or single-nucleus RNA-seq (snRNA-seq) enabled the identification of microglia clusters by analyzing their transcriptional signatures. Using single-cell mass spectrometry (cytometry by time-of-flight [CyTOF]), more than 40 different surface markers can now be identified at the single-cell level, enabling the characterization of immune cell populations in humans and rodents.5,6,7 These findings indicate that microglia are highly heterogeneous cells that are more complex than previously believed. Both intrinsic factors (species, sex, genetic background, etc.) and extrinsic factors (pathogens, nutrition, microbiota, etc.) influence microglial states.8
The terminology “M1” and “M2” microglia is previously widely adopted in microglial research, in which microglia were artificially classified into two opposite types based on findings obtained using in vitro models: the M1 pro-inflammatory and neurotoxic microglia and the M2 anti-inflammatory and neuroprotective microglia.9,10 However, this simplistic classification fails to capture the complexity of microglial responses in the context of neurodegenerative disease. Reactive microglia that refer to microglia undergoing morphological, molecular, and functional remodeling in response to brain challenges (i.e., amyloid β [Aβ] or α-synuclein [α-syn] deposition, infected, damaged, or degenerating neurons) have been observed in various neurodegenerative diseases. Nevertheless, previous studies have relied solely on morphological observation or specific immunohistochemical staining markers to detect these reactive microglia, which were found to cluster in close proximity to pathological hallmarks such as amyloid plaques or α-syn deposits in various brain regions of mouse models and human postmortem cases.11,12 Recent advances in scRNA-seq and snRNA-seq technologies have identified high spatial and temporal heterogeneity levels and unique disease-related signatures of these reactive microglia without correspondence to the canonical M1/M2 classification in neurodegenerative diseases.13,14,15 For instance, scRNA-seq studies identified a specific microglial response state, called disease-associated microglia (DAMs), in mouse models and human patient specimens of AD.13,14,16 Notably, DAMs were localized near Aβ plaques and participated in the clearance of β-amyloid.13 Moreover, distinct Aβ and tau-associated microglia signatures have been discovered in AD patients.15 These findings suggest that microglia show plasticity when responding to various pathologies, highlighting the need to identify disease-specific microglial states and explore factors influencing them to treat AD and other neurodegenerative disorders effectively.
Overall, with the fast development of techniques, recent research on microglia has remarkably revealed their roles in neurodegenerative diseases. In this comprehensive review, we summarize the research history of microglia, the ontogeny and origin of microglia and their physical functions in the homeostatic brain, highlight the current knowledge of the roles of microglia in neurodegenerative diseases including Alzheimer’s disease (AD), Parkinson’s disease (PD), multiple system atrophy (MSA), amyotrophic lateral sclerosis (ALS), frontotemporal dementia (FTD), progressive supranuclear palsy (PSP), corticobasal degeneration (CBD), dementia with Lewy bodies (DLB), and Huntington’s disease (HD). We also summarize the possible microglia-targeted interventions and treatments against neurodegenerative diseases with preclinical and clinical evidence in cell experiments, animal studies, and clinical trials.
서론
중추신경계(CNS)의 상주 대식세포인 미세아교세포는
특이적인 수용체 레퍼토리를 활용하여
뇌 내 미세환경을 동적으로 모니터링한다.1
미세아교세포는
잘못 접힌 단백질, 세포 잔해물 및 사멸 세포를 식균하여 항상성을 유지한다.2
또한 미세아교세포는
미세아교세포-신경세포 간 교신을 통해
신경 기능을 모니터링하고 보호할 수 있다.3
미세아교세포는
오랫동안 주변 환경에 균일하게 반응하는 동질적인 세포로 여겨져 왔다.
그러나
최근 단일 세포 기술의 발전으로
인간과 생쥐 뇌에서 특정 발달, 노화 및 질병 과정과 관련된 여러 미세아교세포 상태가 밝혀졌다.4
예를 들어,
단일 세포 RNA-seq(scRNA-seq) 또는 단일 핵 RNA-seq(snRNA-seq)을 통해
전사 서명을 분석하여 미세아교세포 클러스터를 식별할 수 있게 되었다.
단일 세포 질량 분석법(비행시간형 세포계측법[CyTOF])을 사용하면
현재 40개 이상의 서로 다른 표면 마커를
단일 세포 수준에서 식별할 수 있어
인간과 설치류의 면역 세포 집단을 특성화할 수 있습니다.5,6,7
이러한 연구 결과는
미세아교세포가 이전에 생각했던 것보다
훨씬 더 복잡한 고도로 이질적인 세포임을 시사합니다.
미세아교세포 상태에는
내인성 요인(종, 성별, 유전적 배경 등)과 외인성 요인(병원체, 영양, 미생물군 등)이 모두 영향을 미칩니다.8
미세아교세포 연구에서는
이전에 “M1” 및 “M2” 미세아교세포라는 용어가 널리 채택되었으며,
이는 시험관 내 모델을 통해 얻은 결과를 바탕으로
미세아교세포를 인위적으로 두 가지 상반된 유형으로 분류한 것입니다:
M1형은 염증 촉진 및 신경독성 미세아교세포,
M2형은 항염증 및 신경보호성 미세아교세포로 구분되었다.9,10
그러나 이러한 단순한 분류는
신경퇴행성 질환 맥락에서
미세아교세포 반응의 복잡성을 포착하지 못한다.
반응성 미세아교세포는
뇌 내 도전 요인(예: 아밀로이드 베타[Aβ] 또는 알파-시누클레인[α-syn] 침착,
감염, 손상 또는 퇴행성 신경세포)에 반응하여
형태학적, 분자적, 기능적 재구성을 겪는 미세아교세포를 지칭하며,
다양한 신경퇴행성 질환에서 관찰되었다.
그럼에도 불구하고,
기존 연구들은 이러한 반응성 미세아교세포를 탐지하기 위해 형태학적 관찰이나
특정 면역조직화학 염색 마커에만 의존해 왔으며,
이 미세아교세포들은 마우스 모델 및 인간 사후 검체에서
다양한 뇌 영역의 아밀로이드 플라크나 α-syn 침착물과 같은
병리학적 특징 근처에 밀집해 있는 것으로 확인되었다.11, 12
최근 scRNA-seq 및 snRNA-seq 기술의 발전으로
신경퇴행성 질환에서 이러한 반응성 미세아교세포의 높은 공간적·시간적 이질성 수준과
고유한 질환 관련 서명이 확인되었으며,
이는 기존의 M1/M2 분류와 일치하지 않습니다.13,14,15
예를 들어,
scRNA-seq 연구를 통해 AD 마우스 모델 및 인간 환자 표본에서
질병 관련 미세아교세포(DAMs)라 불리는
특이적인 미세아교세포 반응 상태가 확인되었다.13,14, 16
특히 DAM은
β 플라크 근처에 국소화되어
베타 아밀로이드 제거에 관여하는 것으로 나타났다.13
또한 AD 환자에서 Aβ 및 타우 관련 미세아교세포의 뚜렷한 시그니처가 발견되었다.15 이러한 결과는 미세아교세포가 다양한 병리학적 변화에 반응할 때 가소성을 보임을 시사하며, AD 및 기타 신경퇴행성 질환을 효과적으로 치료하기 위해 질환 특이적 미세아교세포 상태를 규명하고 이를 영향을 미치는 요인을 탐구할 필요성을 강조한다.
기술의 급속한 발전과 함께,
최근 미세아교세포 연구는
신경퇴행성 질환에서의 역할을 놀랍게 밝혀냈다.
본 포괄적 리뷰에서는
미세아교세포의 연구 역사, 발생학적 기원과 기원,
그리고 정상 뇌에서의 물리적 기능을 요약하고,
알츠하이머병(AD), 파킨슨병(PD), 다계통 위축증(MSA), 근위축성 측삭경화증(ALS),
전두측두엽 치매(FTD), 진행성 초핵성 마비(PSP), 피질기저부 퇴행증(CBD),
루이체 치매(DLB), 헌팅턴병(HD) 등 신경퇴행성 질환에서의
미세아교세포 역할에 대한 최신 지식을 강조합니다.
또한 세포 실험, 동물 연구 및 임상 시험에서 전임상 및 임상적 증거를 바탕으로 한
신경퇴행성 질환에 대한 미세아교세포 표적 개입 및 치료 가능성을 요약한다.
Research history of microglia
It has been more than 100 years since microglia were first discovered in 1919. In 2019, Sierra et al. wrote a review to mark the 100th anniversary of the discovery of microglia and recounted the milestones in a century of microglia research.17 In 1919, Spanish researcher Pı´o del Rı´o-Hortega discovered a new type of glial cell based on his invention of a novel method to stain the brain.18 As the tiny size of its soma, so he named it “microglia”. He also found that microglia could phagocytose dendritic spines and cell debris and interact with other cells in the brain parenchyma. Microglia could also proliferate and undergo morphological activation in pathological conditions.18,19,20,21,22 In 1939, John Kershman from the Montreal Neurological Institute first analyzed the origin of microglia in the human brain and found that microglia infiltrate from some sites, such as the choroid plexus, during embryonic human development.23 In 1968, Georg Kreutzberg’s group discovered the role of microglia in synaptic stripping in pathology.24 In 1974, Ibrahim et al. developed a novel method to observe microglia based on histochemical labeling ATPases, which are highly expressed by microglial cells.25 In 1986, Dana Giulian and Timothy Baker established the first microglia culture system, which was an important step in manipulating and studying microglial function.26 Thereafter, it was found that microglia were involved in pathogenesis by releasing chemokines and cytokines.27,28 In 1990, the electrophysiology technique was applied to examine ionic currents in isolated microglia.29 In 1992, a BV-2 cell line was established to study microglia in vitro. Although in vitro and ex vivo microglia differ in many functional aspects, the BV-2 cell line is still in use today.30 In 1997, by developing microglial-preferring ligands, such as PK11195, “activated” microglia could be directly detected in vivo by positron emission tomography (PET) imaging.31 Nonetheless, this method of labeling microglia is not specific. The rationale and limitations of this method will be discussed later in the section “Microglial activation in AD brains”. In 1998, with the development of ionized calcium-binding adaptor molecule 1 (Iba1) antibodies, microglia could be reliably identified in tissue.32 Iba1-label has become one of the gold standards for identifying microglia, although it can also be used to label macrophages. In 2005, a heterozygous Cx3cl1GFP/+ mouse line was established. Cx3cl1 is selectively expressed in microglia in the brain. Thus, by utilizing this mouse line in conjunction with in vivo imaging techniques, it is possible to directly observe the response of microglia to their surrounding environment.33,34
In the past 20 years, microglia research has undergone rapid exponential growth. The advance in technology has contributed significantly to our in-depth understanding of microglia. Here, the progress of our knowledge of microglia identity will be shown as an example. It was in the mid-1970s that the microglia were divided into “resting microglia” and “activated microglia”. The consensus at that time was that microglia remain static under physiological conditions or in the normal brain, showing a ramified phenotype, and these “resting microglia” transform to “activated” under pathological conditions or in the diseased brain, characterized by an ameboid morphological appearance. Nevertheless, in 2005, with the development of a two-photon in vivo imaging system and the establishment of a heterozygous Cx3cl1GFP/+ mouse line, researchers found that microglia are not static but rather extraordinarily dynamic and constantly survey the parenchyma with their highly motile processes, even in the absence of pathological challenge. Recently, based on single-cell sequencing and single-cell mass cytometry, studies have identified various microglial states in both normal and diseased brains. Now, microglia are no longer considered to simply switch from ‘resting’ to ‘activated’ in response to injury, disease, or other challenges. Instead, microglia are continuously active, adopt different states and perform different functions in response to the surrounding environment in the context of health or disease.8,17 Here are some of the key findings in the last decades: (1) microglial are dynamic and heterogenous; (2) microglia communicate with other cell types in the brain; (3) microglia play both protective and deleterious roles in neurodegenerative diseases; (4) microglia can be reprogramed; (5) peripheral immunity regulate microglial response such as via gut–microbiota–brain axis; and (6) microglia also age.17 It is beyond this article’s scope to thoroughly review all progress of microglial research in health and disease, which has been reviewed elsewhere.35,36,37,38,39,40,41 With the fast development of techniques such as live imaging, single-cell omics, and tools designed to manipulate microglia ex vivo and in vivo, the field is expected to advance rapidly in the coming years.17
미세아교세포 연구의 역사
미세아교세포가 1919년 처음 발견된 지 100년이 넘었습니다.
2019년 Sierra 등은
미세아교세포 발견 100주년을 기념하여 리뷰 논문을 발표하고,
한 세기 동안의 미세아교세포 연구의 주요 이정표를 되짚었습니다. 17
https://www.cell.com/trends/neurosciences/fulltext/S0166-2236(19)30175-4
1919년, 스페인 연구원 Pı´o del Rı´o-Hortega는
뇌를 염색하는 새로운 방법을 발명한 것을 바탕으로
새로운 유형의 신경교 세포를 발견했습니다.18
세포체의 크기가 매우 작았기 때문에
그는 이 세포를 “미세아교세포(microglia)”라고 명명했습니다.
그는 또한 미세아교세포가
수상돌기와 세포 잔해를 식균작용할 수 있으며
뇌 실질 내 다른 세포들과 상호작용할 수 있음을 발견했다.
미세아교세포는 병
리학적 조건에서 증식하고 형태학적 활성화를 겪을 수도 있었다.18,19,20,21, 22
1939년 몬트리올 신경학 연구소의 존 커쉬먼은
인간 뇌에서 미세아교세포의 기원을 최초로 분석하여,
인간 배아 발달 과정에서 맥락막과 같은 특정 부위에서
미세아교세포가 침투해 들어온다는 사실을 발견했다.23
1968년
게오르크 크로이츠베르크 연구팀은 병리학적 상황에서
미세아교세포가 시냅스 제거에 관여한다는 사실을 밝혀냈다. 24
1974년, Ibrahim 등은
미세아교세포에서 고도로 발현되는 ATP아제를 이용한
조직화학적 표지법을 바탕으로 미세아교세포를 관찰하는 새로운 방법을 개발하였다.25
1986년, Dana Giulian과 Timothy Baker는
최초의 미세아교세포 배양 시스템을 확립하였으며,
이는 미세아교세포 기능을 조작하고 연구하는 데 중요한 진전이었다. 26
이후 미세아교세포가
케모카인과 사이토카인을 분비하여 병리 발생에 관여한다는 사실이 밝혀졌다.27,28
1990년에는 전기생리학 기법을 적용하여
분리된 미세아교세포의 이온 전류를 조사하였다.29
1992년에는
체외에서 미세아교세포를 연구하기 위해 BV-2 세포주를 확립하였다.
비록 시험관 내 및 생체 외 미세아교세포가 여러 기능적 측면에서 차이가 있지만,
BV-2 세포주는 오늘날에도 여전히 사용되고 있다.30
1997년에는 PK11195와 같은
미세아교세포 선호성 리간드를 개발함으로써
양전자 방출 단층 촬영(PET) 영상으로 생체 내에서
“활성화된” 미세아교세포를 직접 검출할 수 있게 되었다.31
그럼에도 불구하고,
이러한 미세아교세포 표지 방법은 특이적이지 않다.
이 방법의 근거와 한계는
후술할 “알츠하이머병 뇌에서의 미세아교세포 활성화” 섹션에서 논의될 것이다.
1998년, 이온화 칼슘 결합 어댑터 분자 1(Iba1) 항체의 개발로
조직 내 미세아교세포를 신뢰성 있게 식별할 수 있게 되었다.32
Iba1 표지법은 대식세포 표지에도 사용될 수 있지만,
미세아교세포 식별을 위한 표준 방법 중 하나로 자리 잡았다.
2005년에는 이형접합 Cx3cl1GFP/+ 마우스 계통이 확립되었다. Cx3cl1은 뇌 내 미세아교세포에서 선택적으로 발현된다. 따라서 이 마우스 계통을 생체 내 영상 기법과 함께 활용함으로써 미세아교세포가 주변 환경에 반응하는 모습을 직접 관찰할 수 있다.33,34
지난 20년간 미세아교세포 연구는
기하급수적으로 급속히 성장했습니다.
기술 발전은 미세아교세포에 대한 심층적 이해에 크게 기여했습니다.
여기서는 미세아교세포 정체성에 대한 지식의 진전을 예시로 보여드리겠습니다. 1970년대 중반에 미세아교세포는 “휴지 상태 미세아교세포”와 “활성화된 미세아교세포”로 구분되었습니다.
당시 합의된 견해는
미세아교세포가 생리적 조건이나 정상 뇌에서는 정적 상태를 유지하며
가지 모양 형태를 보인다는 것이었고,
이러한 “휴지 상태 미세아교세포”는
병리적 조건이나 병든 뇌에서 “활성화” 상태로 전환되어
아메바 모양의 형태학적 특징을 보인다는 것이었다.
그러나 2005년,
2광자 생체 내 영상 시스템의 개발과 이형접합 Cx3cl1GFP/+ 마우스 계통의 확립을 통해
연구자들은 미세아교세포가 정적이지 않고
오히려 매우 역동적이며,
병리학적 자극이 없는 상태에서도 높은 운동성을 지닌 돌기들로
실질 조직을 지속적으로 탐색한다는 사실을 발견했습니다.
최근 단일 세포 시퀀싱 및 단일 세포 질량 세포계측법을 기반으로 한 연구를 통해
정상 및 병변 뇌 모두에서
다양한 미세아교세포 상태가 확인되었습니다.
이제 미세아교세포는
손상, 질병 또는 기타 자극에 반응하여
단순히 '휴지 상태'에서 '활성화 상태'로 전환되는 것으로 간주되지 않습니다.
대신 미세아교세포는
지속적으로 활동하며, 건강 또는 질병 상태에서 주변 환경에 반응하여
다양한 상태를 취하고 서로 다른 기능을 수행한다.8,17
지난 수십 년간의 주요 연구 결과는 다음과 같다:
(1) 미세아교세포는 역동적이고 이질적이다;
(2) 미세아교세포는 뇌 내 다른 세포 유형과 소통한다;
(3) 미세아교세포는 신경퇴행성 질환에서 보호적 역할과 해로운 역할을 동시에 수행한다;
(4) 미세아교세포는 재프로그래밍될 수 있다;
(5) 장-미생물군집-뇌 축 등을 통해 말초 면역이 미세아교세포 반응을 조절한다;
(6) 미세아교세포 역시 노화한다. 17
건강 및 질병 상태에서의 미세아교세포 연구 진전을 모두 철저히 검토하는 것은 본 논문의 범위를 벗어난다. 이는 다른 문헌에서 이미 검토된 바 있다.35,36,37,38,39,40,41 생체 내 영상, 단일 세포 오믹스, 생체 외 및 생체 내 미세아교세포 조작 도구 등 기술의 급속한 발전으로 향후 몇 년간 이 분야는 빠르게 진전될 것으로 예상된다.17
Ontogeny of microglia
Microglia were long thought to be of neuroectodermal origin like other glial cells and neurons. Nevertheless, microglia are a unique lineage of tissue macrophages, and it is now well-established that microglia are derived from yolk sac (YS) erythromyeloid precursors (EMPs). These EMPs give rise to YS macrophages, which serve as precursors that inhabit the embryonic brain.42,43
In rodents, haematopoiesis contains at least three waves.41 There is some overlap in timing and tissues involved in these waves, which could explain why it has always been difficult to determine the ontogeny of microglia and macrophages in the CNS.44 The first wave, that is the initial phase of hematopoiesis, termed “primitive” hematopoiesis, begins in the YS blood islands (posterior plate mesoderm) at approximately E7.0 (embryonic day 7.0). Between E7.0 and E8.0, this wave generates primary EMP cells. These primary EMPs in the YS generate YS macrophages, which differentiate into microglia or non-parenchymal macrophages in the CNS and tissue macrophages in the peripheral tissues.45 The primary EMPs express the macrophage colony-stimulating factor 1 receptor (CSF1R) and depend on it for survival and differentiation.42 The second “transient definitive” wave of hematopoiesis starts in the YS haemogenic endothelium at E8.25, This leads to the emergence of secondary EMPs. Unlike primary EMPs, secondary EMPs lack CSF1R expression but rely on c-myb for their development,46 suggesting that secondary EMPs possess distinct molecular properties and/or differentiation potential compared to primary EMPs. The third ‘definitive’ wave of haematopoiesis initiates in the embryo proper at E8.5. This wave generates immature hematopoietic stem cells (HSCs) from the haemogenic endothelium in the para-aortic splanchnopleura region. At E10.5, this region develops into the aorta, gonads, and mesonephros (AGM) region. Fetal HSCs migrate from this region to the liver, where they join the secondary EMPs in producing fetal liver (FL) monocytes.46,47 Thus, primary EMPs, secondary EMP-derived fetal liver monocytes, and HSC-derived fetal liver monocytes contribute to all tissue macrophages, with microglia arising solely from primary EMP.41
미세아교세포의 발생
미세아교세포는
오랫동안 다른 신경교세포 및 뉴런과 마찬가지로
신경외배엽 기원이라고 여겨져 왔다.
그러나 미세아교세포는
조직 대식세포의 독특한 계통이며,
현재는 난황낭(YS) 적혈구-골수계 전구세포(EMPs)에서 유래한다는 것이 확립되었다.
이러한 EMP는
배아 뇌에 서식하는 전구세포 역할을 하는
설치류에서 조혈은
최소 세 차례의 파동을 포함한다.41
이 파동들의 시기 및 관련 조직에는 일부 중복이 존재하며,
이는 중추신경계(CNS) 내 미세아교세포와 대식세포의 발생 과정을 규명하는 것이
항상 어려웠던 이유를 설명해 줄 수 있다. 44
첫 번째 단계인 “원시적” 조혈은 약 E7.0(배아 발생 7일차)에 난황낭 혈섬(후판 중배엽)에서 시작된다. E7.0부터 E8.0 사이에 이 단계는 1차 EMP 세포를 생성한다. YS 내의 이 1차 EMP는 YS 대식세포를 생성하며, 이는 중추신경계에서는 미세아교세포 또는 비실질성 대식세포로, 말초 조직에서는 조직 대식세포로 분화한다.45 1차 EMP는 대식세포 군집 자극 인자 1 수용체(CSF1R)를 발현하며, 생존과 분화에 이를 의존한다. 42
두 번째 “일시적 확정” 혈구 생성 파동은 E8.25에 YS 혈구 생성 내피에서 시작되어 이차 EMP의 출현으로 이어집니다. 일차 EMP와 달리 이차 EMP는 CSF1R 발현이 없지만 발달에 c-myb에 의존합니다.46 이는 이차 EMP가 일차 EMP와 비교하여 독특한 분자적 특성과/또는 분화 잠재력을 지닌다는 것을 시사합니다.
제3의 ‘확정적’ 조혈 파동은 배아 본체에서 E8.5에 시작된다. 이 파동은 대동맥 주위 내장흉막(para-aortic splanchnopleura) 영역의 조혈 내피세포로부터 미성숙 조혈줄기세포(HSCs)를 생성한다. E10.5에 이 영역은 대동맥, 생식선, 중신장(mesonephros) 영역(AGM)으로 발달한다. 태아 HSC는 이 영역에서 간으로 이동하여, 2차 EMP와 함께 태아 간(FL) 단핵구를 생성한다.46,47
따라서
1차 EMP, 2차 EMP 유래 태아 간 단핵구, HSC 유래 태아 간 단핵구는
모든 조직 대식세포의 기원이 되며,
미세아교세포는 오직 1차 EMP에서만 발생한다.41
Origin and development of brain microglia
Microglial cell colonization of the CNS is evolutionarily conserved across vertebrate species and occurs before the formation of the neuroectoderm-derived glial cell types such as oligodendrocytes and astrocytes.48,49 EMPs originate in the YS and differentiate into YS macrophages before migrating toward embryonic tissues, including the brain. At E9.5, microglia infiltrate the brain rudiment, entering the leptomeninges and the lateral ventricles to spread throughout the cortex at varying speeds depending on the region and developmental stage.42,50 Normal blood circulation is required for YS macrophage seeding of the CNS. Between E8.0 and E10.0, blood vessels form and remodel de novo in the mouse embryo, coinciding with the appearance of YS precursors in the embryo.51 Interestingly, sodium-calcium exchanger 1 (NCX1)-deficient mice, which exhibit a defective circulatory system, lack microglial progenitors in the embryonic brain despite with normal YS hematopoiesis. This observation supports the idea that the recruitment of YS progenitors into the brain is mediated by blood circulation.42 Yolk sac c-Kit+ EMPs developed into CD45+c-kitlo CX3CR1- immature (A1) cells and matured into CD45+c-kit- CX3CR1+(A2) macrophages.43 A2 macrophages enter the developing mouse brain via the pial surface at E9.5 and migrate along the abluminal surface through the vasculature to become microglia without a monocyte intermediate.43,52,53 Microglial precursors receive instructive signals from the CNS environment once inside the brain parenchyma, which aids in their differentiation.54 Amoeboid macrophages eventually become ramified morphology and cover more of the CNS between E14.5 and the first postnatal week.41
The microglia within the CNS are maintained by both circulating monocytes and repopulation from CNS-endogenous cells. Despite the decrease in proliferating microglia between E14.5 and E15.5, a significant increase in the total number of microglial cells was observed during this period. This finding indicates the possible existence of an additional source of microglial cells that contributes to the resident microglial population.54 Hoxb8 represents a gene of considerable significance in orchestrating the intricate development and functioning of microglia within the brain. At least two progenitor pools for microglia have been demonstrated: canonical non-Hoxb8 microglia and Hoxb8 microglia. Hoxb8 microglia progenitors appear to arise during the second wave of YS hematopoiesis and then enter the AGM region and fetal liver, where their number is greatly increased before they migrate into the developing brain at E12.5. It is estimated that non-Hoxb8 microglia account for 70% of all microglia in the adult brain, significantly outnumbering Hoxb8 microglia, but non-Hoxb8 microglia cannot compensate for the loss of Hoxb8 function in Hoxb8 microglia.55 It is of interest to identify the origin of Hoxb8 microglial progenitors, explore their development, migration, infiltration, and functional changes, and further explore their transcriptional profiles and turnover characteristics by proper fate-mapping system, such as tamoxifen-inducing Cre line, in combination with scRNA-seq and use of reporter cell lines, etc. Human amoeboid microglia infiltrate the developing cerebral cortex through multiple routes, including the pial surface, ventricles, and choroid plexus at 4.5 gestational weeks (gw). These microglia exhibit both radial and tangential migration, directing themselves toward the immature white matter, subplate layer, and cortical plate.48,56 At 12-13 gw, a second wave of microglial invasion via the vasculature is limited to the white matter.48 Evidence also showed repopulation of microglia from CNS-endogenous cells following global microglia depletion, which contributes to the dynamic regulation of the microglia population in the adult mouse brain.57,58 Studies have revealed that in mice, microglia undergo proliferating (Iba1+ BrdU+) at a rate of 0.69% after a single pulse of BrdU (per average of about 96 days), whereas in humans, this rate is ~2%.59 The turnover rate of microglia differs in various regions of the brain in mice, with the olfactory bulb, hippocampus, and cortex in mice undergoing complete renewal in 8, 15, and 41 months, respectively.60 Resident microglia in adults are known to maintain their cell density by balancing proliferation and apoptosis. In humans, the average lifespan of cortical microglia is ~4.2 years.61 Microglial self-renewal appears stochastic, with no regional hot spots, but this process switches to clonal proliferation during pathology.60
뇌 미세아교세포의 기원과 발달
중추신경계(CNS) 내 미세아교세포의 정착은
척추동물 종 전반에 걸쳐 진화적으로 보존되어 있으며,
신경외배엽 유래 글리아 세포 유형(예: 올리고도교세포 및 성상세포)의 형성 이전에 발생한다.48,49
EMP는 신경관(YS)에서 기원하여 YS 대식세포로 분화한 후 뇌를 포함한 배아 조직으로 이동한다. E9.5에 미세아교세포는 뇌 원시체에 침투하여 연막과 측뇌실로 진입한 후, 영역과 발달 단계에 따라 다양한 속도로 피질 전체로 확산된다.42,50
중추신경계로의 YS 대식세포 정착에는
정상적인 혈액 순환이 필요하다.
E8.0부터 E10.0 사이에 혈관이 형성되고 생쥐 배아에서 새로 재구성되며, 이는 배아에서 난황낭 전구세포의 출현과 일치한다.51 흥미롭게도, 순환계에 결함이 있는 나트륨-칼슘 교환기 1(NCX1) 결핍 생쥐는 정상적인 난황낭 조혈에도 불구하고 배아 뇌에서 미세아교세포 전구세포가 결핍된다. 이러한 관찰 결과는 난황낭 전구세포의 뇌 내 유입이 혈액 순환에 의해 매개된다는 가설을 뒷받침한다.42 난황낭 c-Kit+ EMPs는 CD45+c-kitlo CX3CR1- 미성숙 세포(A1)로 발달한 후 CD45+c-kit - CX3CR1+(A2) 대식세포로 성숙하였다.43 A2 대식세포는 E9.5에 뇌막 표면을 통해 발달 중인 생쥐 뇌로 진입하여 혈관 내막을 따라 이동하며 단핵구 중간 단계를 거치지 않고 미세아교세포로 분화한다.43,52, 53 미세아교세포 전구세포는 뇌 실질 내부에 진입한 후 중추신경계 환경으로부터 분화를 돕는 지시적 신호를 받는다.54 아메바형 대식세포는 결국 E14.5부터 출생 후 첫 주 사이에 가지형 형태로 변하며 중추신경계의 더 넓은 영역을 덮게 된다.41
중추신경계 내 미세아교세포는
순환 단핵구와 중추신경계 내재 세포의 재포화 작용에 의해 유지된다.
E14.5부터 E15.5 사이 증식성 미세아교세포 수는 감소하지만,
이 기간 동안 미세아교세포 총 개체수는 현저히 증가하는 것으로 관찰되었다.
이 결과는 상주 미세아교세포 집단에 기여하는 추가적인 미세아교세포 공급원이 존재할 가능성을 시사한다.54 Hoxb8 유전자는 뇌 내 미세아교세포의 복잡한 발달과 기능 조절에 상당한 중요성을 지닌 유전자이다. 미세아교세포를 위한 최소 두 가지 전구 세포 풀이 확인되었습니다: 표준 비-Hoxb8 미세아교세포와 Hoxb8 미세아교세포입니다. Hoxb8 미세아교세포 전구 세포는 YS 조혈의 두 번째 파동 동안 발생하여 AGM 영역과 태아 간으로 이동한 후, E12.5에 발달 중인 뇌로 이동하기 전에 그 수가 크게 증가하는 것으로 보입니다. 비-Hoxb8 미세아교세포는 성인 뇌 내 전체 미세아교세포의 70%를 차지하는 것으로 추정되며, 이는 Hoxb8 미세아교세포보다 훨씬 많은 수치입니다. 그러나 비-Hoxb8 미세아교세포는 Hoxb8 미세아교세포에서 Hoxb8 기능의 상실을 보상할 수 없습니다. 55 Hoxb8 미세아교세포 전구세포의 기원을 규명하고, 그들의 발달, 이동, 침윤 및 기능적 변화를 탐구하며, 타목시펜 유도형 Cre 계통과 같은 적절한 운명 매핑 시스템과 scRNA-seq 및 리포터 세포주 사용 등을 결합하여 그들의 전사 프로파일과 전환 특성을 추가로 탐구하는 것은 흥미로운 일입니다. 인간 아메보이드 미세아교세포는 임신 4.5주(gw)에 뇌막 표면, 뇌실, 맥락막을 포함한 여러 경로를 통해 발달 중인 대뇌 피질로 침투합니다. 이러한 미세아교세포는 방사상 및 접선 이동을 모두 나타내며, 미성숙 백질, 하부판층 및 피질판으로 향합니다.48,56 임신 12~13주에는 혈관을 통한 미세아교세포의 두 번째 침입이 백질로 제한됩니다. 48 또한, 전신 미세아교세포 고갈 후 중추신경계 내인성 세포로부터 미세아교세포가 재증식한다는 증거가 확인되었으며, 이는 성인 생쥐 뇌에서 미세아교세포 집단의 역동적 조절에 기여한다.57,58 연구에 따르면 생쥐에서 미세아교세포는 BrdU 단일 펄스 후 0.69%의 비율로 증식(Iba1+ BrdU+)한다 (평균 약 96일) 후 0.69%의 비율로 증식하는 반면, 인간에서는 이 비율이 약 2%임을 밝혀냈다.59 미세아교세포의 교체율은 쥐의 뇌 영역에 따라 다르며, 쥐의 후각구, 해마, 피질은 각각 8개월, 15개월, 41개월 만에 완전히 갱신된다.60 성체 상주 미세아교세포는 증식과 세포사멸의 균형을 통해 세포 밀도를 유지하는 것으로 알려져 있다. 인간에서 피질 미세아교세포의 평균 수명은 약 4.2년이다.61 미세아교세포의 자가 재생은 특정 부위에 집중되지 않은 확률적 양상을 보이나, 병리학적 상황에서는 클론 증식으로 전환된다.60
Microglia in the homeostatic brain
Factors for microglia development and maturation
Multiple factors regulate the development and maturation of microglia. PU.1, a member of the ETS family, and interferon regulatory factor (IRF8) both function as heterodimers in determining the phenotype of brain macrophages and are essential for the early development of YS microglia precursors.43,62,63 Runx1, expressed in a subset of microglia during early postnatal forebrain development, regulates myeloid cell proliferation and differentiation.64 Runx1 directly binds to the upstream regulatory region of the PU.1 gene, regulating its expression during embryonic and adult hematopoiesis.65 The colony-stimulating factor 1 receptor (CSF1R) is another key regulator for microglia development and maintenance.66 Mice lacking Csf1R exhibit impaired brain architecture and microglia-depleted embryos.67 IL-34, a tissue-restricted ligand of CSF1R, is also required for the development of microglia.68 Mature microglia also require CSF1R signaling, as demonstrated by the significant loss of microglia in adult mice treated with Csf-1R inhibitors.69 CSF1R ligands are major components in all protocols for generating induced pluripotent stem cell (iPSC)-derived microglia, underscoring that CSF1R signaling also plays a significant role in microglia fate specification.70 Transforming growth factor-β (TGF-β) has been proposed as a critical brain-derived signal for microglial specification. When primary microglia are cultured with CSF1 and TGFβ, a significant increase in the expression of microglial signature genes is observed compared to CSF1 alone.71
항상성 뇌의 미세아교세포미세아교세포 발달 및 성숙을 위한 인자
여러 인자가 미세아교세포의 발달과 성숙을 조절한다. ETS 가족의 일원인 PU.1과 인터페론 조절 인자(IRF8)는 모두 이종 이합체로 기능하여 뇌 대식세포의 표현형을 결정하며, YS 미세아교세포 전구세포의 초기 발달에 필수적이다.43,62, 63 출생 후 초기 전뇌 발달 과정에서 일부 미세아교세포에서 발현되는 Runx1은 골수계 세포의 증식과 분화를 조절한다.64 Runx1은 PU.1 유전자의 상류 조절 영역에 직접 결합하여 배아 및 성인 혈액 생성 과정에서의 발현을 조절한다.65 군집자극인자 1 수용체(CSF1R)는 미세아교세포 발달과 유지의 또 다른 핵심 조절인자이다. 66 Csf1R이 결핍된 마우스는 뇌 구조 장애와 미세아교세포가 고갈된 배아를 나타낸다.67 CSF1R의 조직 제한적 리간드인 IL-34 역시 미세아교세포 발달에 필수적이다.68 성숙한 미세아교세포도 CSF1R 신호전달을 필요로 하며, 이는 Csf -1R 억제제를 투여했을 때 미세아교세포가 현저히 감소한 것으로 입증된다.69 CSF1R 리간드는 유도만능줄기세포(iPSC) 유래 미세아교세포 생성 모든 프로토콜의 주요 구성 요소로, CSF1R 신호전달이 미세아교세포 운명 결정에도 중요한 역할을 함을 강조한다.70 변형성장인자-β(TGF-β)는 미세아교세포 특이화를 위한 중요한 뇌유래 신호로 제안되었다. 일차 미세아교세포를 CSF1과 TGFβ와 함께 배양할 때, CSF1 단독 배양 대비 미세아교세포 특이 유전자 발현이 현저히 증가하는 것이 관찰된다.71
Microglial expansion in CNS pathologies
Microgliosis refers to the reactive proliferation of microglial cells in response to pathological conditions. To recover from injury or damage, clones of microglia are reorganized by microglial cell migration and cell death. For example, in response to clinical recovery after facial nerve axotomy, certain microglia near the lesion in the facial nucleus underwent apoptosis or were eliminated through cell migration during the re-establishment of microglial steady state.60 scRNA-seq after facial nerve axotomy in mice revealed the genes that were related to immune response, neuronal cell death, and microglia migration were upregulated, whereas the genes associated with the homeostatic microglial signature, such as Cst3, demonstrate downregulation.72 Although the specific mechanisms underlying the migration and cell death of excess microglia due to clonal expansion remain unclear, these observations indicate that microglia tend to reorganize and restore their homeostasis during clinical recovery.
Recently, microglia and their blood-borne counterparts have been identified as crucial players in disease-associated brain microenvironments and have been implicated in neurodegenerative disease progression.73 The infiltration of monocyte-derived macrophages (MDMs), which have a higher phagocytic activity than microglia, promotes tissue repair and the resolution of inflammation.74 Various methods can be employed to distinguish resident microglia from infiltrated monocytes. In a study, researchers employed a CyTOF panel consisting of 57 markers to characterize the human CNS-resident microglia (huMG) in various brain regions, peripheral blood mononuclear cells (PBMCs), and immune cells from cerebrospinal fluid obtained postmortem from nine donors. Their analysis revealed a distinctive signature specific to huMG, enabling differentiation from mononuclear cells. Notably, CD44 expression was exclusively observed on infiltrating cells rather than resident myeloid cells. The study also detected three subpopulations of microglia that vary regionally and can be distinguished by different levels of specific markers. One subpopulation consisted of microglia increased expression of proteins associated with proliferation (cyclin, cyclin B, Ki-67) and was predominantly found in the subventricular zone (SVZ) and thalamus. The other two microglial clusters originated from the frontal and temporal lobes, respectively. Both clusters exhibited upregulated CD206 but they differed in the levels of CD64 and EMR1.7 Another approach involved using CD11b+CD45high and CD11b+CD45low as markers for peripheral monocytes/macrophages and microglia, respectively75 and found that during the early stages after focal transient ischemia, microglia exhibit a highly branched morphology and show a faint staining intensity (CD45low). In contrast, infiltrated leukocytes display a round-shaped morphology and exhibit a strong, well-contrasted staining (CD45high). These distinct characteristics allow for differentiation between microglia and infiltrated leukocytes.76 It is worthy to further explore different states and different functions of resident microglia and periphery-derived microglia-like cells in the CNS in neurodegenerative disease.
중추신경계 병리에서의 미세아교세포 증식
미세아교세포증(Microgliosis)은
병리적 상태에 대한 반응으로 미세아교세포가 증식하는 현상을 의미한다.
손상이나 손상으로부터 회복하기 위해,
미세아교세포 클론은 미세아교세포 이동과 세포 사멸을 통해 재조직된다.
예를 들어,
안면 신경 축삭 절단 후 임상적 회복에 반응하여,
미세아교세포 안정 상태 재구축 과정에서 안면 신경핵 병변 부근의 특정 미세아교세포는
세포 사멸을 겪거나 세포 이동을 통해 제거되었습니다.60
마우스 안면 신경 축삭 절단 후 수행된 단일세포 RNA 시퀀싱(scRNA-seq)은 면역 반응, 신경세포 사멸, 미세아교세포 이동과 관련된 유전자들은 상향 조절된 반면, Cst3과 같은 미세아교세포 항상성 시그니처 관련 유전자들은 하향 조절되는 것으로 나타났다.72 클론 확장에 따른 과잉 미세아교세포의 이동 및 세포 사멸 기전은 아직 명확하지 않으나, 이러한 관찰 결과는 임상적 회복 과정에서 미세아교세포가 재조직화되어 항상성을 회복하려는 경향이 있음을 시사한다.
최근 미세아교세포와 혈액 유래 대응 세포들은 질환 관련 뇌 미세환경의 핵심 요소로 확인되었으며, 신경퇴행성 질환 진행과 연관성이 제기되었다.73 미세아교세포보다 높은 식세포 활성을 지닌 단핵구 유래 대식세포(MDMs)의 침윤은 조직 회복과 염증 소실을 촉진한다.74 상주 미세아교세포와 침윤 단핵구를 구분하기 위해 다양한 방법이 활용될 수 있다. 한 연구에서 연구진은 57개 마커로 구성된 CyTOF 패널을 활용하여 다양한 뇌 영역의 인간 중추신경계 상주 미세아교세포(huMG), 말초혈 단핵구(PBMCs), 그리고 9명의 기증자로부터 사후에 채취한 뇌척수액의 면역 세포를 특성화하였다. 그들의 분석은 단핵구와 구별할 수 있는 huMG 특유의 독특한 시그니처를 밝혀냈다. 특히, CD44 발현은 상주 골수계 세포가 아닌 침윤 세포에서만 관찰되었다. 이 연구는 또한 특정 마커의 발현 수준 차이로 구별되는 세 가지 하위 집단의 미세아교세포를 검출했으며, 이들은 뇌 영역에 따라 다양하게 분포했다. 한 하위 집단은 증식과 연관된 단백질(사이클린, 사이클린 B, Ki-67) 발현이 증가된 미세아교세포로 구성되었으며, 주로 뇌실하대(SVZ)와 시상에서 발견되었다. 다른 두 미세아교세포 군집은 각각 전두엽과 측두엽에서 유래하였다. 두 군집 모두 CD206 발현이 증가했으나 CD64와 EMR1 수준에서는 차이가 있었다.7 또 다른 접근법에서는 CD11b+CD45high를 말초 단핵구/대식세포의 표지자로, CD11b+CD45low를 미세아교세포의 표지자로 사용했으며75, 국소적 일시적 허혈 후 초기 단계에서 미세아교세포는 고도로 분지된 형태를 보이며 CD45 저발현(CD45low) 상태에서 희미한 염색 강도를 나타냄을 발견했다. (CD45low). 반면, 침윤된 백혈구는 둥근 형태를 보이며 강하고 선명한 염색(CD45high)을 나타낸다. 이러한 뚜렷한 특성으로 미세아교세포와 침윤 백혈구를 구분할 수 있다.76 신경퇴행성 질환에서 중추신경계 내 상주 미세아교세포와 말초 유래 미세아교세포 유사 세포의 다양한 상태 및 기능을 추가로 탐구할 가치가 있다.
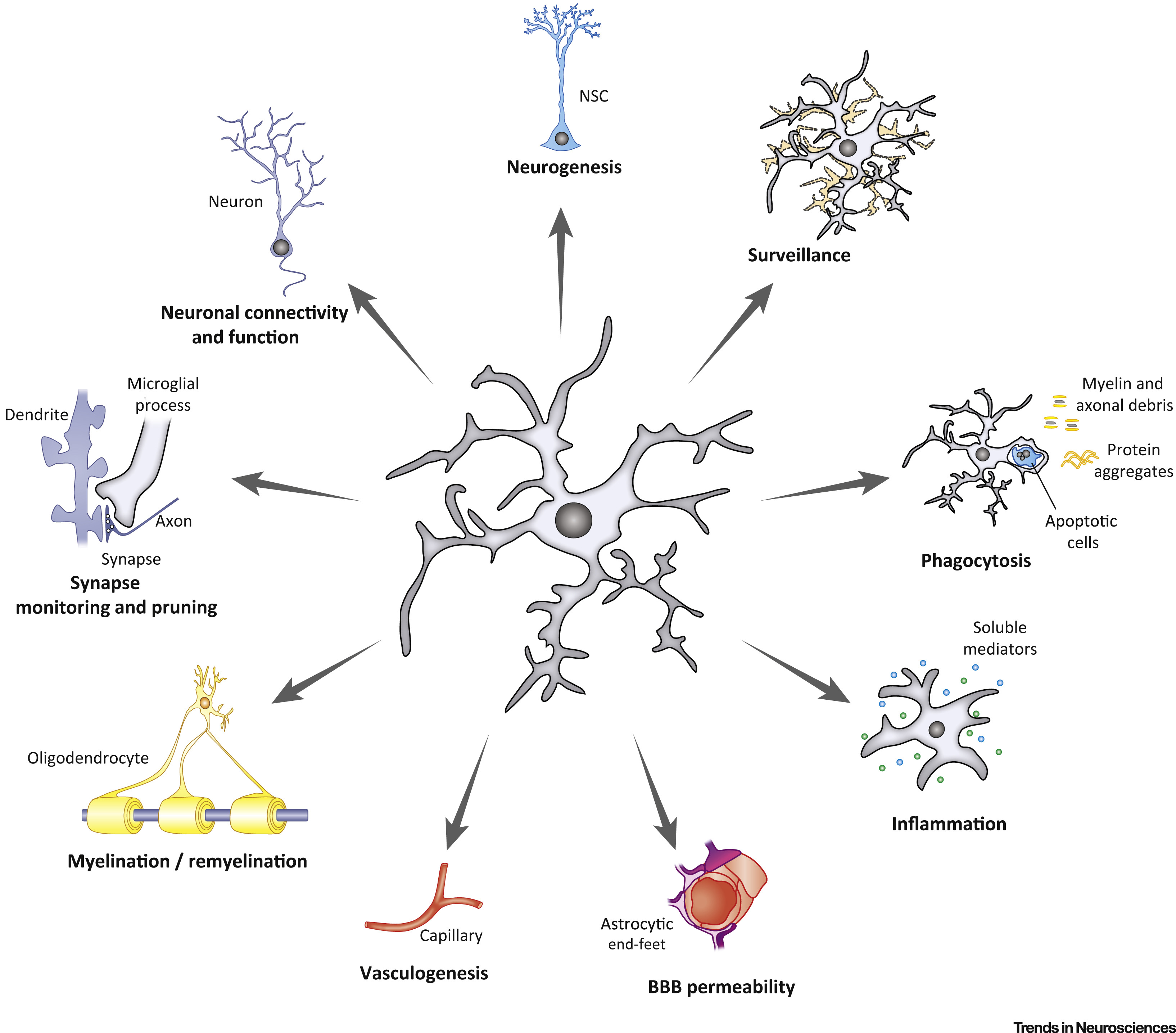
Functions of microglia during homeostasis
Microglia in a homeostatic state use their ramified processes to survey the microenvironment in real time for potential signals that warrant further action. Mature microglia in the postnatal brain use a wide range of surface molecules to respond quickly to their extracellular environment, including cytokines, chemokines, purines, hormones, and neurotransmitters.77 Similar to other macrophages residing in tissues, microglia express common markers such as the fractalkine receptor CX3CR1, CSF1R, the integrin CD11b, surface glycoproteins F4/80 and CD68, ionized calcium-binding adaptor molecule 1 (Iba1), and pan-hematopoietic CD45. However, the expression levels of these markers are generally lower than those observed in perivascular macrophages and blood monocytes at steady state.78 Microglial activation is tightly regulated through receptor-ligand interactions, such as CX3CR1-CX3CL1 and SIRPa-CD47.79 Additionally, in the adult brain, microglia display remarkable efficiency in clearing dead cells and excess cellular material, and microglial phagocytosis shapes adult hippocampal neurogenesis.80 TAM receptor tyrosine kinases Mer and Axl and their ligands Gas6 and protein S regulate the process of microglial phagocytosis. In adult mice, the absence of microglial expression of Axl and Mer leads to a marked accumulation of apoptotic cells, specifically in neurogenic regions of the CNS.81
A rising number of investigations have shown microglial roles in synapse formation, pruning and elimination, and regulation of synaptic function. Synapse elimination occurs during normal brain development, which involves the removal of unnecessary excitatory and inhibitory synaptic connections.82 This elimination process is vital for the formation of mature and efficient neuronal circuits during normal brain development.83 The traditional complement cascade proteins C1q and C3, broadly expressed in the developing brain, localize to specific subsets of immature synapses and mediate their elimination.84 Microglia can phagocytose complement-tagged synapses through the C3-C3 receptor(C3R) pathway, which is crucial for accurate synaptic connection. Importantly, interruption of this pruning mechanism causes long-lasting damage to brain circuitry and synaptic connections.84 Recent research suggests that microglia may respond to astrocyte-derived interleukin-33 (IL-33) to promote synaptic pruning in regions such as the hippocampus and the reticular thalamic nucleus. Knockout mice lacking IL-33 revealed impairments in synaptic elimination during development, suggesting the contribution of astrocytes in regulating microglial-mediated synaptic pruning.85 Microglia also play a crucial role in the modulation of synaptic plasticity. Microglia could enhance synaptic plasticity through the expression and release of brain-derived neurotrophic factor (BDNF) via the microglial phosphatidylinositol 3-kinase (PI3K)/BDNF signaling pathway. BDNF, as a downstream effector of microglial PI3K, increases the plasticity of dendritic spines in the adult cortex.86,87 Microglia can also secrete other neurotrophic factors and cytokines to regulate synaptic plasticity, such as TNFα.88 Additionally, DAP12 signaling participates in the microglia-mediated regulation of synaptic plasticity. DAP12 is exclusively expressed in microglia in the murine brain, and DAP12 deficiency results in a marked impairment of synaptic plasticity.89
Dysregulation of synaptic elimination is involved in the pathogenesis of neurodegenerative diseases.90 Synaptic loss precedes neuronal loss and is considered a more accurate indicator of cognitive decline in AD.91 In neurodegenerative diseases, reactive microglia found near protein aggregates such as Aβ plaques are involved in synapse loss and neuronal damage. Eliminating microglia or attenuating microglial activation in neurodegenerative diseases restored spine number and synaptic integrity and improved functional outcomes.92 In AD brains, microglia mediate aberrant synapse loss via complement mediators (especially C1q and C3),93,94 as well as through the triggering receptor expressed on myeloid cells 2 (TREM2) signaling.95 Additionally, microglia phagocytosis of synapses is also affected by astrocytes. Selective removal of astrocytic APOE4 decreased microglial phagocytosis of synaptic elements in the tau transgenic mouse model.96 Thus, microglia play an indispensable role in regulating the formation, plasticity, and elimination of synapses throughout development and adulthood. Importantly, microglia dysfunction can be an active inducer of the initiation and progression of various neurodegenerative diseases.
항상성 상태에서의 미세아교세포 기능
항상성 상태의 미세아교세포는
분지된 돌기를 이용해 미세환경을 실시간으로 감시하며
추가 조치가 필요한 잠재적 신호를 탐지합니다.
출생 후 뇌의 성숙 미세아교세포는
사이토카인, 케모카인, 퓨린, 호르몬, 신경전달물질 등 세
포외 환경에 신속히 반응하기 위해 다양한 표면 분자를 활용한다.77
다른 조직 상주 대식세포와 유사하게,
미세아교세포는
프랙탈카인 수용체 CX3CR1, CSF1R, 인테그린 CD11b, 표면 당단백질 F4/80 및 CD68, 이온화 칼슘 결합 적응 분자 1(Iba1),
그리고 범혈액 생성 표지자 CD45를 발현한다.
그러나 이러한 표지자의 발현 수준은
일반적으로 정상 상태에서 혈관 주위 대식세포 및 혈액 단핵구에서 관찰되는 수준보다 낮습니다.78
미세아교세포 활성화는
CX3CR1-CX3CL1 및 SIRPa-CD47과 같은 수용체-리간드 상호작용을 통해 엄격하게 조절됩니다.79
또한 성인 뇌에서 미세아교세포는 사체 세포 및 과잉 세포 물질 제거에 탁월한 효율성을 보이며,
미세아교세포의 식작용은 성인 해마 신경생성을 형성한다.80
TAM 수용체 티로신 키나제 Mer 및 Axl과 그 리간드 Gas6 및 프로틴 S는
미세아교세포 식작용 과정을 조절한다.
성체 마우스에서 미세아교세포의 Axl 및 Mer 발현이 결여되면,
특히 중추신경계의 신경생성 영역에서 세포사멸 세포의 현저한 축적이 발생한다.81
점점 더 많은 연구에서
미세아교세포가
시냅스 형성, 정돈 및 제거, 시냅스 기능 조절에 관여함을 보여주고 있다.
시냅스 제거는
정상적인 뇌 발달 과정에서 불필요한 흥분성 및 억제성 시냅스 연결을 제거하는 과정이다.82
이 제거 과정은
정상적인 뇌 발달 중 성숙하고 효율적인 신경 회로 형성에 필수적이다. 83
발달 중인 뇌에 광범위하게 발현되는
전통적인 보체 캐스케이드 단백질인 C1q와 C3는
미성숙 시냅스의 특정 하위 집합에 국소화되어 이들의 제거를 매개한다.84
미세아교세포는
C3-C3 수용체(C3R) 경로를 통해 보체 표지된 시냅스를 식균할 수 있으며,
이는 정확한 시냅스 연결에 필수적이다.
중요한 것은, 이러한 가지치기 메커니즘이 중단되면 뇌 회로와 시냅스 연결에 지속적인 손상이 발생한다는 점이다.84 최근 연구에 따르면, 미세아교세포는 성상세포 유래 인터루킨-33(IL-33)에 반응하여 해마 및 망상 시상핵과 같은 영역에서 시냅스 가지치기를 촉진할 수 있다. IL-33이 결핍된 녹아웃 마우스는 발달 과정에서 시냅스 제거 장애를 보였는데, 이는 아스트로사이트가 미세아교세포 매개 시냅스 정리를 조절하는 데 기여함을 시사한다.85 미세아교세포는 또한 시냅스 가소성 조절에 중요한 역할을 한다. 미세아교세포는 미세아교세포 포스파티딜이노시톨 3-키나아제(PI3K)/BDNF 신호 전달 경로를 통해 뇌유래신경영양인자(BDNF)의 발현 및 분비를 통해 시냅스 가소성을 향상시킬 수 있다. BDNF는 미세아교세포 PI3K의 하류 효과자로서 성인 피질에서 수상돌기 가시의 가소성을 증가시킵니다.86,87 미세아교세포는 또한 TNFα와 같은 다른 신경 영양 인자와 사이토카인을 분비하여 시냅스 가소성을 조절할 수 있습니다.88 또한, DAP12 신호 전달은 미세아교세포 매개 시냅스 가소성 조절에 관여합니다. DAP12는 생쥐 뇌에서 미세아교세포에서만 발현되며, DAP12 결핍은 시냅스 가소성의 현저한 손상을 초래한다.89
시냅스 제거의 조절 이상은
신경퇴행성 질환의 병인에 관여한다.90
시냅스 손실은
신경세포 손실보다 먼저 발생하며,
알츠하이머병(AD)에서 인지 기능 저하의 더 정확한 지표로 간주된다.91
신경퇴행성 질환에서,
Aβ 플라크와 같은 단백질 응집체 근처에서 발견되는 반응성 미세아교세포는
시냅스 손실과 신경세포 손상에 관여한다.
신경 퇴행성 질환에서
미세 아교세포를 제거하거나
미세 아교세포 활성화를 약화시키면,
스파인 수와 시냅스 무결성이 회복되고 기능적 결과가 개선되었습니다. 92
AD 뇌에서 미세아교세포는
보체 매개체(특히 C1q 및 C3)93,94 및 골수세포에 발현되는 트리거링 수용체 2(TREM2) 신호전달을 통해
비정상적인 시냅스 손실을 매개한다.95
또한, 미세아교세포의 시냅스 식균작용은
성상세포의 영향도 받는다.
타우 트랜스제닉 마우스 모델에서 아스트로사이트 APOE4의 선택적 제거는
시냅스 요소에 대한 미세아교세포의 식작용을 감소시켰다.96
따라서
미세아교세포는 발달 및 성인기 전반에 걸쳐
시냅스의 형성, 가소성 및 제거를 조절하는 데 필수적인 역할을 한다.
중요한 것은, 미세아교세포 기능 장애가
다양한 신경퇴행성 질환의 발병 및 진행을 능동적으로 유발할 수 있다는 점이다.
Microglia-neuron crosstalk
Microglia communicate with nearly all cell types in the brain to facilitate developmental process, maintain homeostasis, assist in tissue repair, and contribute to the pathogenesis of diseases.53,97 Reactive microglia undergo proliferation and accumulate in regions with high densities of apoptotic neurons as phagocytes to promote neuronal turnover during developmental cell death and mediate the regulation of synaptic function.98
Microglia maintain neuronal survival and regulate neurogenesis throughout both the prenatal and postnatal stages of development. Microglia limit the production of cortical neurons by phagocytosing neural precursor cells99; at the same time, microglia also promote neurogenesis, as microglia depletion in mice reduces basal progenitors into the cerebral cortex.100 Microglia-derived insulin-like growth factor-1 (IGF1) maintained neuronal survival.101 Microglia can also prevent neuronal hyperexcitability as genetically inhibition of Gi in microglia increases hypersynchrony upon physiologically evoked neuronal activity.102 Microglia-derived IL-1β enhances presynaptic glutamate release by promoting the NMDAR-dependent synthesis of arachidonic acid and prostaglandins.103 Neuronal CD200 interacts with CD200 receptor (CD200R) expressed on microglia and modulates microglial activation.104 Meanwhile, the CD200/CD200R signaling pathway also contributes to the regulation of synaptic plasticity.105 Neuron also induces microglial process extension, and the mechanism involves the neuronal NMDA receptors activation which causes neuronal ATP release, and P2Y12 receptors mediated microglial response.106,107
미세아교세포-신경세포 간 교신
미세아교세포는
발달 과정 촉진, 항상성 유지, 조직 복구 지원, 질병 발병 기전에 기여하기 위해
반응성 미세아교세포는
발달기 세포사멸 동안 식세포로서 사멸 신경세포 고밀도 영역에 증식·축적되어
신경세포 교체를 촉진하고
시냅스 기능 조절을 매개한다.98
미세아교세포는
태내 및 출생 후 발달 단계 전반에 걸쳐
신경세포 생존을 유지하고 신경생성을 조절한다.
미세아교세포는 신경전구세포를 식균작용함으로써
피질 신경세포 생성을 제한한다99;
동시에 미세아교세포는
신경생성을 촉진하기도 하는데,
생쥐에서 미세아교세포를 제거하면 대뇌 피질로의 기초 전구세포 이동이 감소한다.100
미세아교세포 유래 인슐린 유사 성장 인자-1(IGF1)은
신경세포 생존을 유지했다.101
미세아교세포는 또한 신경세포 과흥분을 방지할 수 있는데,
미세아교세포 내 Gi 유전자를 억제하면 생리적으로 유발된
신경세포 활동 시 과동조화가 증가한다. 102
미세아교세포 유래 IL-1β는
아라키돈산과 프로스타글란딘의 NMDAR 의존적 합성을 촉진하여
시냅스 전 글루타메이트 방출을 증가시킵니다.103
신경세포 CD200은
미세아교세포에 발현된 CD200 수용체(CD200R)와 상호작용하여
미세아교세포 활성화를 조절합니다.104
한편, CD200/CD200R 신호전달 경로는
시냅스 가소성 조절에도 기여한다.105
뉴런은 또한 미세아교세포 돌기 확장을 유도하며,
이 메커니즘은 뉴런의 NMDA 수용체 활성화로 인한
뉴런 ATP 방출과 P2Y12 수용체 매개 미세아교세포 반응을 포함한다.106,107
Microglia-astrocyte crosstalk
The interaction between reactive microglia and astrocytes is critical in the development of neuroinflammation. Although the canonical M1/M2 (microglia) and A1/A2 (astrocyte) classifications are not accurate in describing the states of microglia and astrocytes, this classification is helpful to elucidate the interaction of microglia and astrocytes and will be adopted here. Microglia and astrocytes exhibit two polarization states: pro-inflammatory (M1 and A1) and anti-inflammatory (M2 and A2). Microglia are more susceptible to pathogens or damage such as LPS or stroke. Activation of pattern recognition receptors (PRRs) via pathogen-associated molecular patterns (PAMPs) or damage-associated molecular patterns (DAMPs) triggers microglia M1 phenotype.108 Microglia display a diverse set of toll-like receptors (TLRs), whereas astrocytes primarily express TLR3, with minimal expression of TLR1, TLR4, TLR5, and TLR9 and no expression of TLR2, TLR6, TLR7, TLR8, and TLR10.109 The relatively low expression of TLRs in astrocytes suggests they may have limited ability to respond directly to various pathogens. Instead, they rely on microglia to detect pathogens and communicate with astrocytes to induce their activation. Specifically, in the case of TLR4 activation triggered by LPS, microglia are directly involved in initiating or facilitating astrocytic responses by releasing mediators. This highlights the crucial role of microglia-astrocyte crosstalk in the CNS’s response to insults, injuries, or inflammatory stimuli.110 Microglia have the potential to enhance the inflammatory activation of astrocytes by increasing the expression level of cytokines and chemokines, specifically through the activation of nuclear factor-κB (NF-κB) signaling.111 Reactive microglia produce IL-1α, TNFα, and C1q, which induce the neurotoxic A1 astrocytes phenotype conversion.112 Once A1 astrocytes are induced, they lose their essential functions such as supporting neuronal survival, and they also promote neuroinflammation, which contributes to the progression of neurodegenerative diseases.113 Reactive M2-like microglia produce the anti-inflammatory cytokine IL-10, which binds to the IL-10 receptor (IL-10R) mainly expressed in A2 astrocytes. This interaction enables astrocytes to release TGF-β, reducing microglial activation.114 Communication via extracellular vesicles (EVs) has recently been identified as a critical pathway for CNS cells because EVs may be released and taken up by various cell types. EVs are essential mediators of microglia-astrocyte interaction. Astrocyte-derived ATP induces the formation and the shedding of EVs and IL-1β release in nearby microglia, triggering a neuroinflammatory response.115
미세아교세포-성상세포 간 교신
반응성 미세아교세포와 성상세포 간의 상호작용은 신경염증 발생에 핵심적 역할을 한다. 비록 정형화된 M1/M2(미세아교세포) 및 A1/A2(성상세포) 분류가 미세아교세포와 성상세포의 상태를 정확히 설명하지는 못하지만, 이 분류는 미세아교세포와 성상세포의 상호작용을 규명하는 데 유용하므로 본 논문에서도 채택한다. 미세아교세포와 성상세포는 두 가지 분극 상태를 나타낸다: 친염증성(M1 및 A1)과 항염증성(M2 및 A2). 미세아교세포는 LPS나 뇌졸중과 같은 병원체나 손상에 더 민감하다. 병원체 관련 분자 패턴(PAMPs) 또는 손상 관련 분자 패턴(DAMPs)을 통한 패턴 인식 수용체(PRRs)의 활성화는 미세아교세포의 M1 표현형을 유발한다.108 미세아교세포는 다양한 톨 유사 수용체(TLRs)를 발현하는 반면, 성상세포는 주로 TLR3을 발현하며, TLR1, TLR4, TLR5, TLR9의 발현은 최소한이며, TLR2, TLR6, TLR7, TLR8, TLR10은 발현하지 않습니다.109 아스트로사이트에서 상대적으로 낮은 TLR 발현은 다양한 병원체에 직접 반응하는 능력이 제한적일 수 있음을 시사합니다. 대신, 아스트로사이트는 병원체 감지를 미세아교세포에 의존하며, 미세아교세포는 아스트로사이트와 소통하여 그 활성화를 유도합니다. 특히, LPS에 의해 유발된 TLR4 활성화의 경우, 미세아교세포는 매개체를 방출함으로써 아교세포 반응을 시작하거나 촉진하는 데 직접 관여합니다. 이는 중추신경계(CNS)가 손상, 외상 또는 염증 자극에 반응하는 과정에서 미세아교세포-아스트로사이트 간 상호작용이 핵심적 역할을 함을 강조한다.110 미세아교세포는 특히 핵인자-κB(NF-κB) 신호전달 경로의 활성화를 통해 사이토카인과 케모카인의 발현 수준을 증가시켜 아스트로사이트의 염증 활성화를 증강시킬 잠재력을 지닌다.111 반응성 미세아교세포는 IL-1α, TNFα, C1q를 생성하며, 이는 신경독성 A1 아스트로사이트 표현형 전환을 유도한다.112 A1 아스트로사이트가 유도되면, 신경세포 생존 지원과 같은 필수 기능을 상실할 뿐만 아니라 신경염증을 촉진하여 신경퇴행성 질환의 진행에 기여한다.113 반응성 M2형 미세아교세포는 항염증성 사이토카인 IL-10을 생성하며, 이는 주로 A2 아스트로사이트에 발현되는 IL-10 수용체 (IL-10R)에 결합한다. 이 상호작용은 아스트로사이트가 TGF-β를 방출하여 미세아교세포 활성화를 감소시키는 것을 가능하게 한다.114 세포외 소포(EVs)를 통한 통신은 최근 중추신경계 세포의 중요한 경로로 확인되었는데, 이는 EVs가 다양한 세포 유형에 의해 방출 및 흡수될 수 있기 때문이다. EVs는 미세아교세포-아스트로사이트 상호작용의 필수 매개체이다. 아스트로사이트 유래 ATP는 근처 미세아교세포에서 엑소좀의 형성 및 분비와 IL-1β 방출을 유도하여 신경염증 반응을 촉발한다.115
Microglia-oligodendrocyte crosstalk
Oligodendrocyte precursor cells (OPCs), highly proliferative cells that mature in separate waves, give rise to myelinating oligodendrocytes. Microglia play an essential role in the proper development and homeostasis of OPCs and oligodendrocytes.116 Reactive microglia of the SVZ release TNFα, IL-1β, IL-6, and IFN-γ, promoting oligodendrocyte development. In contrast, a reduction in the levels of these cytokines impairs oligodendrogenesis.117 A CD11c+ microglial subset was identified in the developing brain that predominates in the primary myelinating areas. These CD11c+ microglia express genes for neuronal and glial survival, migration, and differentiation. These CD11c+ microglia, characterized by their amoebic shapes along white matter pathways such as the corpus callosum and cerebellum, serve as a primary source of IGF1 and other factors involved in neurogenesis and myelinogenesis, which exert their effects on oligodendrocytes in the newborn brain.118 Thus, the interaction between early postnatal microglia and OPCs/oligodendrocytes in the white matter at a specific developmental stage is critical in supporting proper myelin synthesis. Besides, fractalkine-dependent microglial pruning of OPCs is indispensable for proper myelination. Mice lacking fractalkine receptor show a reduction in microglial phagocytosis of OPCs, and increased numbers of oligodendrocytes but reduced myelin thickness.119 Additionally, in the microglia-oligodendrocyte cocultures system, microglia stimulate oligodendrocytes to synthesize sulfatide, a myelin-specific galactolipid, along with myelin proteins myelin basic protein (MBP) and proteolipid protein (PLP).120
미세아교세포-올리고도교세포 간 교신
올리고도교세포 전구세포(OPCs)는 고도로 증식하는 세포로, 별개의 파동으로 성숙하여 수초 형성 올리고도교세포를 생성한다. 미세아교세포는 OPC 및 올리고도교세포의 적절한 발달과 항상성 유지에 필수적인 역할을 한다.116 측뇌실주변대(SVZ)의 반응성 미세아교세포는 TNFα, IL-1β, IL-6 및 IFN-γ를 방출하여 올리고도교세포 발달을 촉진한다. 반면, 이러한 사이토카인 수치의 감소는 올리고도교세포 생성을 저해한다.117 발달 중인 뇌에서 주요 수초 형성 영역에 주로 존재하는 CD11c+ 미세아교세포 하위 집합이 확인되었다. 이러한 CD11c+ 미세아교세포는 신경세포 및 아교세포의 생존, 이동, 분화 관련 유전자를 발현합니다. 뇌량 및 소뇌와 같은 백질 경로를 따라 아메바 모양을 띠는 특징을 가진 이 CD11c+ 미세아교세포는 신생아 뇌에서 올리고도교세포에 영향을 미치는 신경발생 및 수초형성에 관여하는 IGF1 및 기타 인자의 주요 공급원 역할을 합니다.118 따라서 특정 발달 단계에서 백질 내 출생 후 초기 미세아교세포와 OPC/올리고도교세포 간의 상호작용은 적절한 미엘린 합성을 지원하는 데 매우 중요하다. 또한 프랙탈킨 의존적 미세아교세포에 의한 OPC의 제거는 정상적인 미엘린 형성에 필수적이다. 프랙탈카인 수용체가 결핍된 생쥐는 미세아교세포의 OPC 식작용이 감소하고, 올리고도교세포 수는 증가하지만 수초 두께는 감소하는 것으로 나타난다.119 또한, 미세아교세포-올리고도교세포 공배양 시스템에서 미세아교세포는 올리고도교세포가 수지상 단백질(MBP) 및 지단백질(PLP)과 함께 수초 특이적 갈락토지질인 설파타이드를 합성하도록 자극한다.120
Microglial dysfunction in neurodegenerative diseases
In the CNS, microglia, as the first line of immune defense, constantly survey their environment and interact with neurons, astrocytes, oligodendrocytes, and infiltrating immune cells. In the homeostatic brain, microglia exert roles in synapse pruning, injury repair, homeostasis maintenance, phagocytosis, support of other glial cells, and communication with other cells. Microglia respond to CNS injuries and diseases with complex reactions, commonly called “activation.” Microglia activation was observed in various neurodegenerative diseases. In the early years of microglial research, microglial activation was detected by morphological observation as they transformed from their ramified phenotype in the normal brain to ameboid morphological appearance in the diseased brain. However, microglia activation is more varied and dynamic than ever anticipated, both in -omics features and functional consequences, indicating that microglia respond differently in different diseases. In the last section, we reviewed microglial functions in the homeostatic brain to provide context for microglial changes in neurodegenerative diseases. In this section, we present the diversity of microglia states responding to pathological conditions and highlight the current knowledge of the roles of microglia in neurodegenerative diseases. Meanwhile, we also summarize some therapeutic approaches for neurodegenerative diseases that target microglia.
신경퇴행성 질환에서의 미세아교세포 기능 장애
중추신경계(CNS)에서 미세아교세포는 면역 방어의 최전선으로서 지속적으로 주변 환경을 감시하며 뉴런, 성상세포, 올리고도교세포 및 침윤 면역세포와 상호작용한다. 정상적인 뇌에서는 미세아교세포가 시냅스 정돈, 손상 복구, 항상성 유지, 식작용, 다른 신경교세포 지원 및 타 세포와의 소통에 역할을 수행한다. 미세아교세포는 중추신경계 손상 및 질환에 대해 일반적으로 “활성화”라고 불리는 복잡한 반응으로 대응한다. 다양한 신경퇴행성 질환에서 미세아교세포 활성화가 관찰되었다. 초기 미세아교세포 연구에서는 정상 뇌에서의 가지 모양 표현형에서 병변 뇌에서의 아메바형 형태학적 모습으로 전환되는 형태학적 관찰을 통해 미세아교세포 활성화를 확인했다. 그러나 미세아교세포 활성화는 -omics 특징과 기능적 결과 측면에서 예상보다 훨씬 다양하고 역동적이며, 이는 미세아교세포가 질환별로 상이하게 반응함을 시사한다. 마지막 섹션에서는 신경퇴행성 질환에서의 미세아교세포 변화를 이해하기 위한 맥락으로, 항상성 뇌에서의 미세아교세포 기능을 검토하였다. 본 절에서는 병리적 조건에 반응하는 미세아교세포 상태의 다양성을 제시하고, 신경퇴행성 질환에서 미세아교세포의 역할에 대한 현재의 지식을 강조한다. 동시에 미세아교세포를 표적으로 하는 신경퇴행성 질환 치료 접근법 일부를 요약한다.
Alzheimer’s disease
Alzheimer’s disease (AD) is the most common neurodegenerative cause of senile dementia, accounting for 60–70% of dementia cases. In 2019, there were more than 55 million dementia patients worldwide, and the number is expected to rise to 139 million by 2050, according to the World Alzheimer Report 2022.121 The primary pathological features of AD are extraneuronal amyloid plaques formed by the deposition of Aβ peptide in the brain and intracellular neurofibrillary tangles (NFTs) caused by abnormal aggregation of tau protein.122 Mechanismly, various factors, including genetics, amyloid protein, tau, ApoE, and neuroimmune activation, are involved in the pathogenesis of AD.123 Recently, genome-wide association studies (GWAS) have demonstrated that most AD risk genes are highly or exclusively in microglia,124 suggesting that microglia play an essential role in AD development.
알츠하이머병
알츠하이머병(AD)은 노인성 치매의 가장 흔한 신경퇴행성 원인이며, 치매 사례의 60~70%를 차지한다. 2019년 기준 전 세계 치매 환자는 5,500만 명 이상이었으며, 2022년 세계 알츠하이머 보고서에 따르면 2050년까지 1억 3,900만 명으로 증가할 것으로 예상됩니다.121 AD의 주요 병리학적 특징은 뇌 내 Aβ 펩타이드 침착으로 형성된 신경세포 외 아밀로이드 플라크와 타우 단백질의 비정상적 응집으로 인한 세포 내 신경섬유 엉킴( (NFTs)이다.122 기전적으로 유전학, 아밀로이드 단백질, 타우, ApoE, 신경면역 활성화 등 다양한 요인이 AD 발병에 관여한다.123 최근 전장유전체연관분석(GWAS)을 통해 대부분의 AD 위험 유전자가 미세아교세포에서 매우 높거나 독점적으로 발현된다는 사실이 밝혀졌다.124 이는 미세아교세포가 AD 발병에 핵심적인 역할을 함을 시사한다.
Microglial activation in AD brains
Several studies conducted on autopsy tissues of AD patients and controls showed that microglial activation was observed in AD brains,125,126 and microglial activation was significantly higher within Aβ plaques compared with plaque-free cortical areas.125,127 Microglial activation has been detected in vivo by PET imaging. Transporter protein (TSPO) is an 18 kDa translocator protein, expressed at low levels on the outer membrane of mitochondria in the glial cells under physiological conditions. However, during neuroinflammation, the expression level of TSPO is significantly upregulated in these reactive glial cells, especially in microglia. Therefore, numerous studies have utilized radiotracers that specifically bind to TSPO to visualize the reactive microglia directly.128,11[C](R)-PK11195 (PK), as the first-generation TSPO PET tracer, has been extensively used to study microglial activation. However, several factors have limited its widespread use. The first challenge is related to the low signal-to-noise ratio, which makes it difficult to detect subtle changes in neuroinflammation. Several sites in the blood, including plasma proteins, monocytes, and platelets, bind to 11[C](R)-PK11195, resulting in a low brain permeability and, therefore, a low signal-to-noise ratio.129 Secondly, TSPO is also expressed by other cell types, such as astrocytes and vascular endothelial cells in the brain, indicating its non-specificity. Cellular sources and subcellular localization of TSPO expression in healthy and diseased brain has been reviewed in previous studies.130,131 Thirdly, the relatively short half-life of carbon-11 also limits the clinical usefulness of11[C](R)-PK11195.132 Over the past few years, second and third-generation TSPO tracers have been developed to address these limitations. Unfortunately, these new radioligands have not been without their problems. The first factor concerning the rs6971 polymorphism of human TSPO polymorphisms affects the binding affinities of radiotracer.133 Furthermore, the problem of non-specific binding remains. Importantly, TSPO is more suitable as a biomarker of neuroinflammation than a marker of microglial activation.131 However, many studies have used TSPO-PET imaging to detect microglial activation in a diverse range of neurodegenerative diseases.132 Consistent evidence using PET imaging indicated microglial activation in the brains of AD patients. Using [11C](R)-PK11195, [11C]-PBR28, or some other TSPO-specific radiotracers, AD patients all showed significantly increased regional TSPO ligand binding in the cortices compared to controls.134,135,136 In addition, microglial activation was found in the white matter.137 Microglial activation has also been detected by PET in patients with mild cognitive impairment (MCI).138,139,140 In MCI, microglial activation was positively correlated with amyloid load.141,142
AD 뇌에서의 미세아교세포 활성화
AD 환자와 대조군의 부검 조직을 대상으로 수행된 여러 연구에서 AD 뇌에서 미세아교세포 활성화가 관찰되었으며,125,126 Aβ 플라크 내 미세아교세포 활성화는 플라크가 없는 피질 영역에 비해 현저히 높았다.125,127 PET 영상으로 생체 내 미세아교세포 활성화가 검출되었다. 수송체 단백질(TSPO)은 18kDa의 전좌 단백질로, 생리적 조건에서 신경교세포의 미토콘드리아 외막에 낮은 수준으로 발현된다. 그러나 신경염증 동안, TSPO의 발현 수준은 이러한 반응성 신경교세포, 특히 미세아교세포에서 현저히 상향 조절된다. 따라서 수많은 연구에서 TSPO에 특이적으로 결합하는 방사성 추적자를 활용하여 반응성 미세아교세포를 직접 시각화해 왔다.128,11[C](R)-PK11195(PK)는 1세대 TSPO PET 추적자로, 미세아교세포 활성 연구에 광범위하게 사용되어 왔다. 그러나 여러 요인으로 인해 그 광범위한 사용이 제한되어 왔다. 첫 번째 문제는 낮은 신호 대 잡음비와 관련되어 있어 신경 염증의 미세한 변화를 감지하기 어렵습니다. 혈장 단백질, 단핵구, 혈소판 등 혈액 내 여러 부위가 11[C](R)-PK11195에 결합하여 뇌 투과성이 낮아지고, 결과적으로 신호 대 잡음비가 낮아집니다.129 둘째, TSPO는 뇌의 성상 세포 및 혈관 내피 세포와 같은 다른 세포 유형에서도 발현되어 비특이성을 나타냅니다. 건강한 뇌와 병변 뇌에서의 TSPO 발현 세포 기원 및 세포 내 국소화는 기존 연구에서 검토된 바 있다.130,131 셋째, 탄소-11의 상대적으로 짧은 반감기도11[C](R)-PK11195의 임상적 유용성을 제한한다.132 지난 몇 년간 이러한 한계를 극복하기 위해 2세대 및 3세대 TSPO 추적자가 개발되었다. 안타깝게도 이러한 새로운 방사성 리간드 역시 문제점이 없지는 않았다. 첫 번째 요인은 인간 TSPO 다형성의 rs6971 다형성이 방사성 추적자의 결합 친화력에 영향을 미친다는 점이다.133 또한 비특이적 결합 문제 역시 여전히 남아 있다. 중요한 점은 TSPO가 미세아교세포 활성화 지표보다는 신경염증의 생체표지자로 더 적합하다는 것이다.131 그러나 다양한 신경퇴행성 질환에서 미세아교세포 활성화를 탐지하기 위해 TSPO-PET 영상이 다수 연구에 활용되었다.132 PET 영상 연구에서 일관되게 관찰된 증거는 알츠하이머병(AD) 환자 뇌에서 미세아교세포 활성화가 존재함을 시사한다. [11C](R)-PK11195, [11C]-PBR28 또는 기타 TSPO 특이적 방사성 추적자를 사용한 연구에서, AD 환자들은 대조군에 비해 피질에서 지역적 TSPO 리간드 결합이 유의하게 증가한 것으로 나타났다.134,135,136 또한, 백질에서도 미세아교세포 활성화가 발견되었다.137 경도인지장애(MCI) 환자에서도 PET를 통해 미세아교세포 활성화가 검출되었다.138,139,140 MCI에서 미세아교세포 활성화는 아밀로이드 부하와 양의 상관관계를 보였다.141,142
Microglia response to AD pathology
Previous studies detected reactive microglia by morphological observation and specific immunohistochemical staining markers. These reactive microglia were found to be clustered near Aβ plaques in various brain regions of AD mice and human postmortems.11,12 The in vivo imaging study also found that microglial activation correlated with tau and amyloid in AD.143 In recent years, with the development of scRNA-seq and snRNAseq technologies, microglia in various states were identified, significantly advancing our knowledge of microglia responses to pathological hallmarks in AD. In an AD mouse model (5×FAD transgenic mice which recapitulate major features of AD amyloid pathology), Keren-Shaul et al.13 first identified a subgroup of microglia in AD, termed disease-associated microglia (DAM), which participated in the clearance of Aβ. DAMs were localized near Aβ plaques, which has also been validated in AD postmortem brain samples. In AD patients, snRNA-seq of the occipital cortex and the occipitotemporal cortex from AD patients and controls identified three clusters: homeostatic microglia, AD1-microglia, and AD2-microglia. The occipital cortex contained Aβ pathology, with no or low-level tau pathology, while the occipitotemporal cortex contained both Aβ pathology and tau pathology. AD1-microglia were localized near Aβ plaques and were strongly correlated with the tissue Aβ load. Gene ontology analysis indicated that AD1-microglia showed similarities with DAM signatures in the 5×FAD mouse model. Both were associated with “phagocytosis”, “lipid localization”, and “cell migration. AD2-microglia possibly have neurotrophic functions.15 Besides, Nguyen et al. characterized microglia in various states in AD brains: homeostatic microglia, amyloid responsive microglia, dystrophic microglia, and motile microglia, among which the amyloid responsive microglia relied on triggering receptor expressed on myeloid cells-2 (TREM2) and APOE signaling.144 Another study used snRNA-seq to comprehensively characterize transcriptomes in microglia nuclei isolated from neuropathologically defined AD and control brains with a range of Aβ and phosphorylated (p)-Tau pathology. The study found that microglial transcripts were most highly positively associated with tissue Aβ and tissue pTau density.145 These results suggest that microglia respond to the pathology of AD. In the early stage of the disease, this response may be protective. The reactive microglia migrate to the vicinity of pathological deposits such as Aβ or tau and then engulf and eliminate them. However, when these growing pathological deposits chronically stimulate microglia, the protective microglia may convert to dysfunctional microglia, aggravating the disease progression of AD.
AD 병리에 대한 미세아교세포 반응
기존 연구에서는 형태학적 관찰과 특정 면역조직화학 염색 마커를 통해 반응성 미세아교세포를 검출했습니다. 이러한 반응성 미세아교세포는 AD 마우스 및 인간 사후 검체에서 다양한 뇌 영역의 Aβ 플라크 근처에 군집되어 있는 것으로 확인되었습니다.11, 12 생체 내 영상 연구에서도 미세아교세포 활성화가 AD에서 타우 및 아밀로이드와 상관관계가 있음을 발견하였다.143 최근 단일세포 RNA-seq 및 snRNAseq 기술의 발전으로 다양한 상태의 미세아교세포가 확인되어, AD 병리학적 특징에 대한 미세아교세포 반응에 대한 이해가 크게 진전되었다. AD 마우스 모델(AD 아밀로이드 병리의 주요 특징을 재현하는 5×FAD 트랜스제닉 마우스)에서 Keren-Shaul 등13은 AD에서 Aβ 제거에 관여하는 '질병 관련 미세아교세포(DAM)'라는 하위 집단을 최초로 확인했다. DAM은 Aβ 플라크 근처에 국한되어 있었으며, 이는 AD 사후 뇌 샘플에서도 검증되었다. AD 환자에서 후두피질 및 후두측두피질의 snRNA-seq 분석을 통해 대조군과 비교하여 세 가지 클러스터(항상성 미세아교세포, AD1-미세아교세포, AD2-미세아교세포)가 확인되었습니다. 후두피질은 타우 병리가 없거나 낮은 수준인 반면 Aβ 병리를 포함했으며, 후두측두피질은 Aβ 병리와 타우 병리를 모두 포함했습니다. AD1-미세아교세포는 Aβ 플라크 근처에 국한되어 조직 내 Aβ 부하량과 강한 상관관계를 보였다. 유전자 온톨로지 분석 결과, AD1-미세아교세포는 5×FAD 마우스 모델의 DAM(amyloid-responsive) 서명과 유사성을 나타냈다. 양자 모두 “포식작용”, “지질 국소화”, “세포 이동”과 연관되었다. AD2-미세아교세포는 신경 영양 기능을 가질 가능성이 있습니다.15 또한 Nguyen 등은 AD 뇌에서 다양한 상태의 미세아교세포를 특성화했습니다: 항상성 미세아교세포, 아밀로이드 반응성 미세아교세포, 영양 장애성 미세아교세포, 운동성 미세아교세포 등, 그중 아밀로이드 반응성 미세아교세포는 골수세포에 발현되는 트리거링 수용체-2 (TREM2) 및 APOE 신호 전달에 의존했다.144 또 다른 연구에서는 snRNA-seq을 사용하여 신경병리학적으로 정의된 AD 및 대조군 뇌에서 분리된 미세아교세포 핵의 전사체를 포괄적으로 특성화했으며, 이 뇌들은 다양한 Aβ 및 인산화(p)-Tau 병리를 보였습니다. 이 연구는 미세아교세포 전사체가 조직 Aβ 및 조직 pTau 밀도와 가장 높은 양의 상관관계를 보인다는 것을 발견했습니다.145 이러한 결과는 미세아교세포가 AD 병리에 반응한다는 것을 시사합니다. 질병 초기 단계에서 이러한 반응은 보호적일 수 있습니다. 반응성 미세아교세포는 Aβ 또는 타우와 같은 병리학적 침착물 주변으로 이동한 후 이를 포식하고 제거합니다. 그러나 이러한 병리적 침착물이 지속적으로 미세아교세포를 자극하면, 보호적 역할을 하던 미세아교세포가 기능 장애 미세아교세포로 전환되어 AD의 질병 진행을 악화시킬 수 있다.
Microglial roles in the pathogenesis of AD
Effect of microglia on Aβ pathology
Considerable evidence has found that microglia promote the uptake and degradation of Aβ. For example, LC3-associated endocytosis (LANDO) in microglia facilitates Aβ receptor recycling, increasing Aβ surface receptors, thus promoting Aβ clearance, and in contrast, LANDO-deficient AD mice induced neurodegeneration and memory deficits.146 With aging, the Nogo receptor (NgR) expression on microglia increased, impairing microglial phagocytosis and clearance of Aβ. In contrast, NgR-deficient AD mice reduced amyloid burden and improved cognitive impairment.147 BACE-1 inhibition in microglia facilitated the microglia phenotype transition from homeostatic to stage 1 disease-associated microglia (DAM-1) signature148 and thus enhanced amyloid clearance and improved cognitive performance in AD mice.149 In addition, microglia interact with astrocytes to promote Aβ clearance. After recognizing Aβ deposits, microglia increased their expression of IL-3Rα, the specific receptor for IL-3. Astrocyte-derived IL-3 bound to the upregulated IL-3Rα in microglia, enhancing microglial migration toward Aβ deposits and the Aβ aggregates clearance.150 APOE isoforms also affect the phagocytosis of Aβ by microglia. Compared with APOE4, APOE3 lipoproteins induce faster microglial migration towards Aβ, facilitate Aβ uptake, and ameliorate cognition.151
Although the above studies have shown that microglia could phagocytize Aβ and reduce amyloid plaque deposition and neurodegeneration, some studies have also found that the phagocytosis of Aβ by microglia promoted plaque development.152 In AD mice, sustained microglial depletion with CSF1R inhibitor reduced plaque development.32 Besides, microglia facilitate Aβ spreading. Aβ activates the immune system and induces the formation and release of apoptosis-associated speck-like protein containing a caspase activation and recruitment domain (CARD) (ASC) specks. After being released from microglia, ASC specks bind to and promote the cross-seeding of Aβ, leading to amyloid seeding and spreading of amyloid pathology.153 To examine whether microglia contribute to Aβ propagation, d’Errico P et al. using transplantation of wild-type (WT) neurons, found that Aβ entered WT grafts accompanied by microglia infiltration and in vivo imaging revealed that microglia were carries of Aβ pathology in previously unaffected tissue154 (Fig. 1).
AD 병리에서 미세아교세포의 역할미세아교세포가 Aβ 병리에 미치는 영향
미세아교세포가 Aβ의 포획 및 분해를 촉진한다는 상당한 증거가 발견되었다. 예를 들어, 미세아교세포에서 LC3 관련 세포내수(LANDO)는 Aβ 수용체 재순환을 촉진하여 Aβ 표면 수용체를 증가시키고, 결과적으로 Aβ 제거를 촉진한다. 반대로, LANDO 결핍 AD 마우스는 신경퇴행과 기억력 결손을 유발했다.146 노화와 함께 미세아교세포의 Nogo 수용체(NgR) 발현이 증가하여 미세아교세포의 식작용과 Aβ 제거가 손상되었다. 반대로, NgR 결핍 AD 마우스는 아밀로이드 부하를 감소시키고 인지 장애를 개선했습니다.147 미세아교세포에서 BACE-1 억제는 미세아교세포 표현형을 항상성 상태에서 1단계 질병 관련 미세아교세포(DAM-1) 시그니처로 전환시키는 데 도움이 되었습니다.148 따라서 AD 마우스에서 아밀로이드 제거를 강화하고 인지 능력을 개선했습니다.149 또한, 미세아교세포는 성상 세포와 상호 작용하여 Aβ 제거를 촉진합니다. Aβ 침착물을 인식한 후, 미세아교세포는 IL-3의 특이적 수용체인 IL-3Rα의 발현을 증가시켰다. 성상세포 유래 IL-3는 미세아교세포에서 상향 조절된 IL-3Rα에 결합하여 Aβ 침착물 및 Aβ 응집체 제거를 향한 미세아교세포의 이동을 강화했다.150 APOE 이소형도 미세아교세포에 의한 Aβ의 식세포 작용에 영향을 미친다. APOE4에 비해 APOE3 지단백질은 Aβ를 향한 미세아교세포의 이동을 더 빠르게 유도하고, Aβ 흡수를 촉진하며, 인지 기능을 개선한다.151
위 연구들은 미세아교세포가 Aβ를 식균하여 아밀로이드 플라크 침착과 신경퇴행을 감소시킬 수 있음을 보여주었으나, 일부 연구에서는 미세아교세포의 Aβ 식균이 오히려 플라크 형성을 촉진한다는 결과도 보고되었다.152 AD 마우스에서 CSF1R 억제제로 지속적 미세아교세포 제거 시 플라크 형성이 감소하였다.32 또한 미세아교세포는 Aβ 확산을 촉진한다. Aβ는 면역 체계를 활성화하여 세포사멸 관련 스펙클 유사 단백질(ASC)의 형성과 방출을 유도한다. 미세아교세포에서 방출된 ASC 스펙클은 Aβ에 결합하여 교차 시딩을 촉진함으로써 아밀로이드 시딩과 병리 확산을 유발한다.153 미세아교세포가 Aβ 전파에 기여하는지 확인하기 위해, d’Errico P 등은 야생형(WT) 뉴런 이식을 통해 Aβ가 미세아교세포 침윤과 함께 WT 이식편으로 유입됨을 발견했으며, 생체 내 영상 분석을 통해 미세아교세포가 이전에 영향을 받지 않은 조직에서 Aβ 병리의 운반체 역할을 함을 확인했다154 (그림 1).
Fig. 1
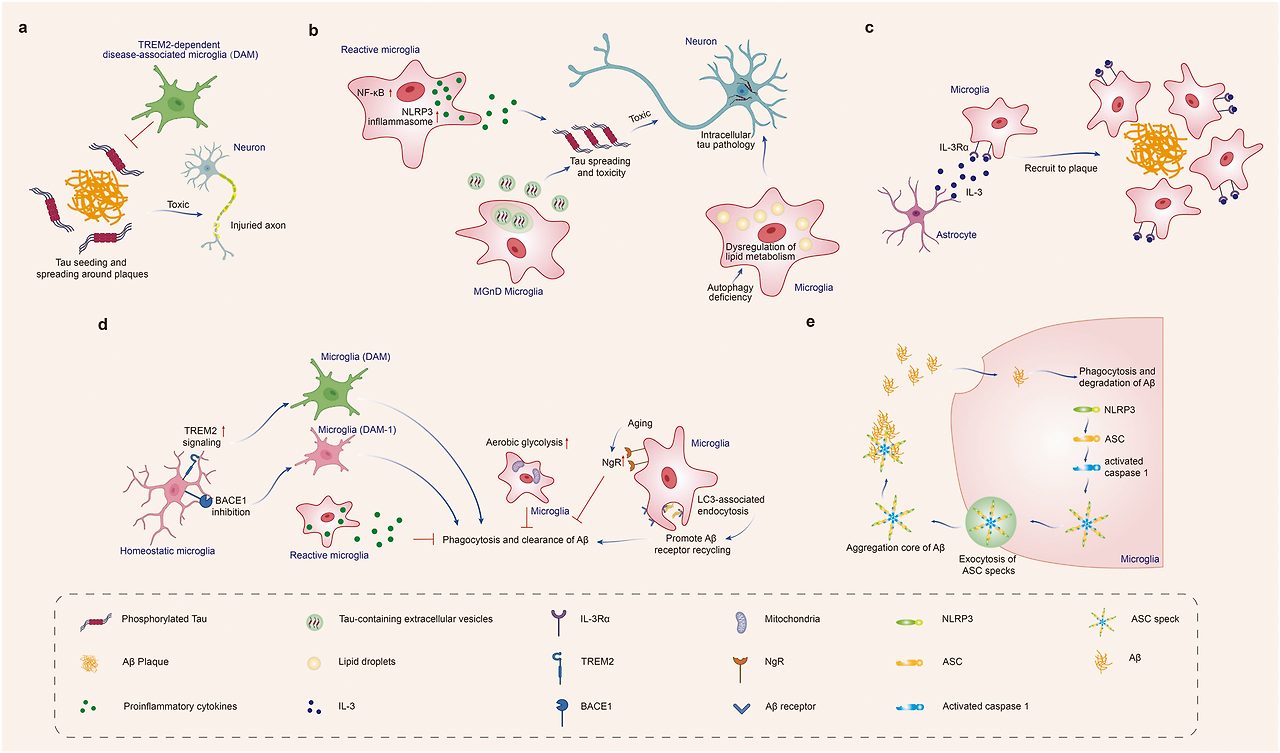
Effect of microglia on Aβ and tau pathology in Alzheimer’s disease. Microglia phagocytose Aβ and tau, limit propagation of Aβ and tau pathology. Under pathological conditions, microglia could also accelerate Aβ and tau spreading and lead to neurodegeneration. a TREM2-dependent DAM limits tau seeding and spreading around plaques. b Reactive microglia drive tau spreading and toxicity by promoting neuroinflammation, such as activating NLRP3 inflammasome or inducing NF-kB signaling. Microglial autophagy deficiency leads to dysregulation of lipid metabolism, thus increasing intraneuronal tau pathology and its spreading. MGnD microglia, which is common in neurodegeneration, hypersecrete EVs containing pTau, accelerates tau propagation. c Microglia increase their expression of IL-3Rα after recognition of Aβ deposits. Astrocyte-derived IL-3 binds to the upregulated IL-3Rα in microglia, enhancing microglial migration toward Aβ deposits, and the clearance of Aβ aggregates. d TREM2 promotes the conversion of microglia to the DAM phenotype, and BACE-1 inhibition in microglia facilitates the microglia phenotype transition from homeostatic to DAM-1 signature. DAM and DAM-1 phenotypes enhance amyloid clearance. LC3-associated endocytosis (LANDO) in microglia facilitates Aβ receptor recycling, increases Aβ surface receptors, and thus promotes Aβ clearance. In contrast, the microglia with enhanced aerobic glycolysis, and NgR expression on microglia increased with aging inhibit the phagocytosis and clearance of Aβ. e Microglia facilitate Aβ spreading. Aβ induces immune system activation and the formation and release of ASC specks. After being released from microglia, ASC specks bind to and promote the cross-seeding of Aβ, leading to amyloid seeding and spreading. Created with https://BioRender.com
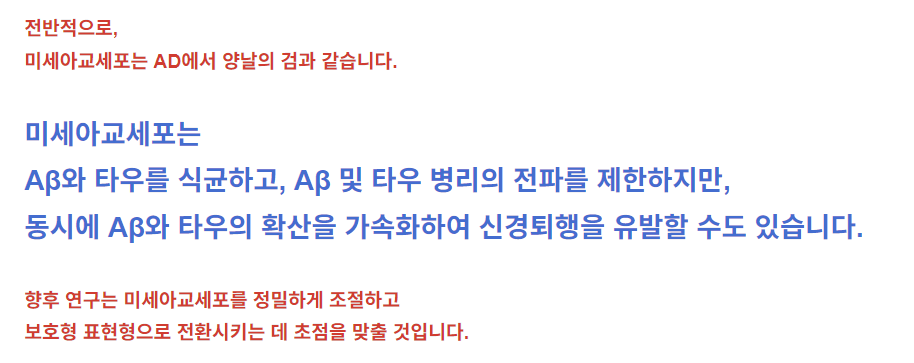
알츠하이머병에서 미세아교세포가 Aβ 및 타우 병리에 미치는 영향.
미세아교세포는 Aβ와 타우를 식균하여 Aβ 및 타우 병리의 전파를 제한한다. 병리학적 조건에서는 미세아교세포가 Aβ와 타우 확산을 가속화하여 신경퇴행을 유발할 수도 있다.
a TREM2 의존성 DAM은 플라크 주변 타우 시딩 및 확산을 제한한다.
b 반응성 미세아교세포는 NLRP3 인플라마좀 활성화 또는 NF-kB 신호전달 유도 등 신경염증을 촉진하여 타우 확산 및 독성을 유발한다. 미세아교세포의 자가포식 결핍은 지질 대사 조절 장애를 유발하여 신경세포 내 타우 병리 및 확산을 증가시킵니다. 신경퇴행성 질환에서 흔히 관찰되는 MGnD 미세아교세포는 pTau를 함유한 엑소좀(EVs)을 과다 분비하여 타우 확산을 가속화합니다.
c 미세아교세포는 Aβ 침착물 인식 후 IL-3Rα 발현을 증가시킵니다. 성상세포 유래 IL-3는 미세아교세포에서 상향 조절된 IL-3Rα에 결합하여 Aβ 침착물로의 미세아교세포 이동 및 Aβ 응집체 제거를 촉진한다.
d TREM2는 미세아교세포의 DAM 표현형 전환을 촉진하며, 미세아교세포 내 BACE-1 억제는 미세아교세포 표현형이 항상성 상태에서 DAM-1 시그니처로 전환되도록 돕는다. DAM 및 DAM-1 표현형은 아밀로이드 제거를 강화한다. 미세아교세포 내 LC3 관련 내포작용(LANDO)은 Aβ 수용체 재활용을 촉진하고, Aβ 표면 수용체를 증가시켜 Aβ 제거를 촉진한다. 반면, 노화에 따라 증가하는 미세아교세포의 강화된 호기성 당분해 및 NgR 발현은 Aβ의 식작용 및 제거를 억제한다.
e 미세아교세포는 Aβ 확산을 촉진한다. Aβ는 면역 체계 활성화와 ASC 스펙의 형성과 방출을 유도한다. 미세아교세포에서 방출된 ASC 스펙은 Aβ에 결합하여 교차 시딩을 촉진함으로써 아밀로이드 시딩 및 확산을 유발한다. https://BioRender.com로 생성됨
Effect of microglia on tau pathology
Microglia limit Aβ-associated tau seeding and spreading in AD mouse models. TREM2 has been reported to promote the conversion of microglia to the DAM phenotype, which is responsible for Aβ phagocytosis.13 Similarly, with the presence of Aβ, TREM2-dependent activation of the DAM phenotype can also limit tau pathology propagation. On the other hand, microglia could also drive tau spreading and toxicity by promoting neuroinflammation, such as activating NACHT-, LRR- and pyrin (PYD)-domain-containing protein 3 (NLRP3) inflammasome155 or inducing NF-kB signaling.156 In addition, autophagy is defective in AD microglia.157 Microglial autophagy deficiency can lead to dysregulation of lipid metabolism, induce microglia into a pro-inflammatory state, and as a result, enhance intraneuronal tau pathology and its spreading.158 The above evidence suggests that microglia-mediated neuroinflammation is detrimental in accelerating tau pathology. Besides, it has been suggested that EVs as potential carriers propagate misfolded proteins, such as tau and Aβ in AD and α-syn in PD.159 In a humanized APP mouse model, MGnD microglia, a class of disease-reactive microglia common in neurodegeneration, hypersecrete EVs containing phosphorylated tau (pTau), accelerating tau propagation.160 In contrast, inhibiting microglia secretion of tau-containing EVs alleviated tau pathology and cognitive impairment in P301S tau transgenic mice161 (Fig. 1).
미세아교세포가 타우 병리에 미치는 영향
미세아교세포는 AD 마우스 모델에서 Aβ 관련 타우 시딩 및 확산을 제한한다. TREM2는 미세아교세포를 Aβ 식세포작용을 담당하는 DAM 표현형으로 전환시키는 것으로 보고되었다.13 마찬가지로, Aβ 존재 시 TREM2 의존적 DAM 표현형 활성화는 타우 병리 전파를 제한할 수 있다. 반면 미세아교세포는 NACHT-, LRR- 및 pyrin (PYD)-도메인 함유 단백질 3 (NLRP3) 인플라마좀 활성화155 또는 NF-kB 신호전달 유도156과 같은 신경염증을 촉진함으로써 타우 확산 및 독성을 유발할 수도 있다. 또한 자식작용은 AD 미세아교세포에서 결함이 있다.157 미세아교세포 자식작용 결핍은 지질 대사 조절 장애를 초래하고, 미세아교세포를 염증 촉진 상태로 유도하며, 결과적으로 신경세포 내 타우 병리 및 그 확산을 증진시킬 수 있다.158 위 증거들은 미세아교세포 매개 신경염증이 타우 병리 가속화에 해롭다는 점을 시사한다. 또한, 엑소좀(EVs)이 잠재적 운반체로서 AD의 타우 및 Aβ, PD의 α-시누클레인(α-syn)과 같은 변형 단백질을 전파한다는 제안이 있다.159 인간화 APP 마우스 모델에서, 신경퇴행성 질환에서 흔히 관찰되는 질병 반응성 미세아교세포의 일종인 MGnD 미세아교세포는 인산화 타우(pTau)를 함유한 엑소좀을 과다 분비하여 타우 전파를 가속화한다.160 반면, 타우 함유 엑소좀의 미세아교세포 분비를 억제하면 P301S 타우 트랜스제닉 마우스에서 타우 병리와 인지 장애가 완화되었다161 (그림 1).
Impact of TREM2 on microglia responses to AD pathology
TREM2 is expressed highly and exclusively in microglia in the brain.162 GWAS showed that the R47H variant of TREM2 was associated with a 2- to 4-fold increased risk for the development of AD.163,164 Several other TREM2 variants that affect the expression of TREM2 also increased the risk of AD, including R62H, T66M, H157Y, and D87N.165,166,167,168 As a result of the genetic association of TREM2 variants with AD, how TREM2 impacts the microglial response to AD pathology has been studied.
TREM2-dependent microglial activation is critical to sustaining microglia defense against Aβ and tau pathology. Loss of TREM2 function impaired Aβ phagocytosis by microglia and increased amyloid seeding in AD mouse models.169,170 Conversely, enhancing TREM2 signaling by TREM2 agonist antibody, direct delivery of the TREM2 gene, or stimulating other pathways to increase TREM2 expression in the brains of AD mice enhanced Aβ phagocytosis and improved cognitive behaviors.171,172,173 As for the underlying mechanism, Aβ binds to microglial TREM2, which activates TREM2 signaling and lead to the enhanced phagocytosis of microglia.174 Additionally, sc-RNAseq revealed that TREM2 promoted the conversion of microglia to the DAM phenotype, which is responsible for Aβ phagocytosis.13 Although studies have found a protective role for TREM2 in response to amyloid pathology, the opposing roles for TREM2 have been reported in mouse models of tauopathies. The evidence supporting the protective role is that TREM2 knockout (KO) or TREM2 R47H variant dramatically enhanced tau seeding and spreading around plaques in AD mice.175,176,177 But other studies found that TREM2 deficiency significantly reduced brain atrophy and prevented microglial activation in tau transgenic mice.178,179 Notably, the impact of TREM2 on Aβ and tau pathology may vary at different disease stages. APP/PS1 mice treated with Trem2 knockdown antisense oligonucleotides (ASOs) through the ventricles at late stages exhibited a 50% reduction in plaque load. In contrast, administration of ASOs at early stages did not affect plaque load.180 Responding to tau pathology, in the early stages of AD, TREM2 may suppress tau seeding, but later in AD, it may aggravate tau propagation.178,179,181,182
TREM2, a single-pass transmembrane receptor, undergoes proteolytic processing and the soluble variant of TREM2 (sTREM2) is released from the cell via shedding by ADAM protease following proteolytic processing.183 sTREM2 can be detected in human plasma and CSF,184,185,186 and clinical evidence showed that sTREM2 is becoming a valuable marker of AD pathology and cognitive decline. High CSF sTREM2 was associated with slower rates of Aβ accumulation,187 and higher CSF sTREM2/p-Tau was associated with slower cognitive decline,188 which supports the hypothesis that microglia and sTREM2 play a protective role in AD. sTREM2 is thought to be protective by (i) stimulating microglial recruitment, activation, and phagocytosis of Aβ (ii) inhibiting secondary nucleation of Aβ fibrillization and preventing neurotoxicity, (iii) binding of sTREM2 to fibrils to enhance microglial uptake of fibrillar Aβ.189,190,191 However, in opposition to the protective role of sTREM2 in AD, the mutation p.H157Y located at the cleavage site of TREM2 extracellular domain significantly increased TREM2 shedding with elevated sTREM2 levels in the brain and serum but associated with increased AD risk.192,193 Additionally, experimental evidence revealed that sTREM2 directly bound to neurons in mouse models of AD194 and inhibited LTP induction.195 Together, these novel insights into the function of sTREM2 are important to deepen our understanding of the complex biology of TREM2 and microglia in AD.
Overall, microglia are a double-edged sword in AD. Microglia phagocytose Aβ and tau, limit propagation of Aβ and tau pathology, and can also accelerate Aβ and tau spreading and lead to neurodegeneration. Future research will focus on precisely regulating microglia and promoting their conversion into a protective phenotype.
TREM2가 AD 병리에 대한 미세아교세포 반응에 미치는 영향
TREM2는 뇌 내 미세아교세포에서만 고도로 발현된다.162 GWAS 연구에 따르면 TREM2의 R47H 변이체는 AD 발병 위험을 2~4배 증가시키는 것으로 나타났다.163,164 TREM2 발현에 영향을 미치는 다른 여러 TREM2 변이체들(R62H, T66M, H157Y, D87N 등이 포함된다.165,166,167,168 TREM2 변이체와 AD의 유전적 연관성 결과, TREM2가 AD 병리에 대한 미세아교세포 반응에 미치는 영향이 연구되었다.
TREM2 의존적 미세아교세포 활성화는 Aβ 및 타우 병리에 대한 미세아교세포 방어 유지에 중요하다. TREM2 기능 상실은 미세아교세포의 Aβ 식작용을 저해하고 AD 마우스 모델에서 아밀로이드 시딩을 증가시켰다.169,170 반대로, TREM2 작용제 항체, TREM2 유전자 직접 전달 또는 다른 경로 자극을 통한 TREM2 신호 전달 강화로 AD 마우스 뇌 내 TREM2 발현을 증가시키면 Aβ 식작용이 향상되고 인지 행동이 개선되었다. 171,172,173 기전 측면에서, Aβ는 미세아교세포의 TREM2에 결합하여 TREM2 신호전달을 활성화시키고, 이는 미세아교세포의 식작용을 강화시킵니다.174 또한, sc-RNAseq 분석 결과 TREM2가 미세아교세포를 Aβ 식작용을 담당하는 DAM(병리적 활성화 미세아교세포) 표현형으로 전환시키는 것으로 밝혀졌다.13 TREM2가 아밀로이드 병리 반응에서 보호적 역할을 한다는 연구 결과가 있는 반면, 타우병증 마우스 모델에서는 TREM2의 상반된 역할이 보고되었다. 보호적 역할을 뒷받침하는 증거로는 TREM2 녹아웃(KO) 또는 TREM2 R47H 변이체가 AD 마우스에서 플라크 주변의 타우 시딩 및 확산을 극적으로 증가시켰다는 점이 있다.175,176,177 그러나 다른 연구에서는 TREM2 결핍이 타우 트랜스제닉 마우스에서 뇌 위축을 현저히 감소시키고 미세아교세포 활성화를 방지한다는 사실을 발견했다.178,179 특히 주목할 점은, TREM2가 Aβ 및 타우 병리에 미치는 영향은 질병 단계에 따라 달라질 수 있다. 후기 단계에서 뇌실 내 Trem2 노크다운 안티센스 올리고뉴클레오티드(ASO)를 투여받은 APP/PS1 마우스는 플라크 부하가 50% 감소했다. 반면 초기 단계에서 ASO를 투여해도 플라크 부하에는 영향을 미치지 않았다.180 타우 병리에 대한 반응으로, 알츠하이머병 초기 단계에서 TREM2는 타우 시딩을 억제할 수 있으나, 후기 단계에서는 타우 전파를 악화시킬 수 있다.178,179,181,182
단일 통과 막 수용체인 TREM2는 단일 통과 막 관통 수용체인 TREM2는 단백질 분해 처리를 거치며, 이 과정에서 ADAM 프로테아제에 의한 분비 과정을 통해 세포 외부로 용해성 TREM2(sTREM2)가 방출된다.183 sTREM2는 인간 혈장 및 뇌척수액(CSF)에서 검출 가능하며,184,185,186 임상 증거에 따르면 sTREM2는 AD 병리 및 인지 기능 저하의 유용한 지표로 부상하고 있다. 높은 CSF sTREM2는 Aβ 축적 속도의 둔화와 관련이 있었으며,187 높은 CSF sTREM2/p-Tau는 인지 기능 저하의 둔화와 관련이 있었습니다.188 이는 미세 아교세포와 sTREM2가 AD에서 보호적인 역할을 한다는 가설을 뒷받침합니다. sTREM2는 (i) 미세아교세포의 모집, 활성화 및 Aβ의 식균 작용을 자극하고, (ii) Aβ 섬유화의 2차 핵형성을 억제하고 신경 독성을 방지하며, (iii) 섬유소 결합을 통한 미세아교세포의 섬유상 Aβ 흡수 촉진189,190,191. 그러나 AD에서의 sTREM2 보호 역할과 대조적으로, TREM2 세포외 도메인 절단 부위에 위치한 p.H157Y 돌연변이는 TREM2 분비를 현저히 증가시켜 뇌 및 혈청 내 sTREM2 수치를 상승시켰으나, 이는 AD 위험 증가와 연관되었다. 192,193 또한, 실험적 증거에 따르면 sTREM2는 AD 마우스 모델에서 뉴런에 직접 결합하여194 LTP 유도를 억제하는 것으로 밝혀졌습니다.195 종합하면, sTREM2의 기능에 대한 이러한 새로운 통찰력은 AD에서 TREM2와 미세아교세포의 복잡한 생물학적 특성에 대한 이해를 심화시키는 데 중요합니다.
전반적으로,
미세아교세포는 AD에서 양날의 검과 같습니다.
미세아교세포는
Aβ와 타우를 식균하고, Aβ 및 타우 병리의 전파를 제한하지만,
동시에 Aβ와 타우의 확산을 가속화하여 신경퇴행을 유발할 수도 있습니다.
향후 연구는 미세아교세포를 정밀하게 조절하고
보호형 표현형으로 전환시키는 데 초점을 맞출 것입니다.
Dysfunctional microglia impair neuronal activity
Microglia have surveillance functions that closely interact with neurons to regulate their activity. Disruption of this network can lead to neurodegeneration. The E4 allele of APOE increases the risk of developing late-onset AD.196 Microglia harboring an APOE4 allele showed altered cellular metabolism, increasing intracellular and extracellular lipid accumulation. The extracellular lipid droplets directly decreased neuronal activity by increasing inward K+ currents.197 Microglia could also lead to synaptic dysfunction in vivo and in vitro by releasing Aβ-containing EVs.198
Neuronal activity depends on the precise regulation of synapse formation and elimination. However, in AD brains, microglia dysregulation contributes to spine loss. Cerebrovascular damage is one of the key features of AD.199 Fibrinogen leaked from the site of cerebrovascular damage into the brain and subsequently bound to the receptor CD11b on the surface of microglia. The interaction of fibrinogen and CD11b mediated microglial activation led to spine loss and promoted cognitive deficits in the 5×FAD mice. Genetic elimination of the fibrinogen binding motif to CD11b ameliorated the above pathological processes and cognitive impairments.200 Microglia phagocytosis of synapses is also affected by astrocytes. Selective removal of astrocytic APOE4 decreased microglial phagocytosis of synaptic elements in the tau transgenic mouse model.96
In addition to eliminating neuronal synapses, the removal of perineuronal nets (PNNs) by microglia is also involved in the pathogenesis of AD. PNNs, components of the extracellular matrix (ECM) surrounding the soma and dendrites of various neuronal cell types in mammals, play important roles in controlling plasticity in the CNS. Removal of PNNs affects functional recovery after CNS injury.201 In the 5×FAD mouse model and human cortical tissue, extensive loss of PNNs has been observed, and the loss of PNNs was proportional to plaque burden. Chronically depleting microglia before and during plaque development in two AD transgenic mouse models significantly reduced PNN loss, indicating that microglia promote plaque-dependent PNN loss.202 The above studies indicated that dysfunctional microglia in AD promoted the clearance of synapses and PNNs and impaired neuronal plasticity and activity (Fig. 2).
기능 장애 미세아교세포는 신경 세포 활동을 손상시킵니다
미세아교세포는 신경 세포와 밀접하게 상호작용하며 그 활동을 조절하는 감시 기능을 수행합니다. 이 네트워크의 붕괴는 신경퇴행으로 이어질 수 있습니다. APOE의 E4 대립유전자는 후기 발병형 AD 발병 위험을 증가시킵니다.196 APOE4 대립유전자를 보유한 미세아교세포는 세포 대사가 변화하여 세포 내외 지질 축적이 증가했습니다. 세포외 지질 방울은 내향성 K+ 전류를 증가시켜 신경 세포 활동을 직접 감소시켰습니다.197 미세아교세포는 또한 Aβ를 함유한 엑소좀(EVs)을 방출함으로써 생체 내 및 시험관 내에서 시냅스 기능 장애를 유발할 수 있습니다.198
신경 세포 활동은 시냅스 형성과 소멸의 정밀한 조절에 의존한다. 그러나 AD 뇌에서는 미세아교세포의 조절 이상이 스파인 손실에 기여한다. 뇌혈관 손상은 AD의 주요 특징 중 하나이다.199 뇌혈관 손상 부위에서 유출된 피브리노겐이 뇌로 유입되어 미세아교세포 표면의 수용체 CD11b에 결합하였다. 피브리노겐과 CD11b의 상호작용에 의한 미세아교세포 활성화는 5×FAD 마우스에서 스파인 손실을 유발하고 인지 결손을 촉진했다. CD11b에 대한 피브리노겐 결합 모티프의 유전적 제거는 상기 병리학적 과정과 인지 장애를 완화시켰다.200 미세아교세포의 시냅스 식작용은 성상세포의 영향도 받는다. 타우 트랜스제닉 마우스 모델에서 아스트로사이트 APOE4의 선택적 제거는 시냅스 요소에 대한 미세아교세포의 식작용을 감소시켰다.96
신경 시냅스 제거 외에도, 미세아교세포에 의한 신경주위망(PNNs)의 제거 역시 알츠하이머병(AD)의 병인에 관여한다. PNN은 포유류의 다양한 신경 세포 유형의 세포체와 수상돌기를 둘러싸는 세포외 기질(ECM)의 구성 요소로, 중추신경계(CNS)의 가소성 조절에 중요한 역할을 합니다. PNN 제거는 CNS 손상 후 기능 회복에 영향을 미칩니다.201 5×FAD 마우스 모델과 인간 피질 조직에서 광범위한 PNN 손실이 관찰되었으며, PNN 손실은 플라크 부담과 비례했습니다. 두 알츠하이머병(AD) 트랜스제닉 마우스 모델에서 플라크 발생 전 및 발생 중 미세아교세포를 만성적으로 제거하면 PNN 손실이 현저히 감소하여, 미세아교세포가 플라크 의존적 PNN 손실을 촉진함을 시사한다.202 상기 연구들은 AD에서 기능 장애를 보이는 미세아교세포가 시냅스와 PNN의 제거를 촉진하고 신경 가소성 및 활성을 손상시킴을 나타냈다(그림 2
Fig. 2
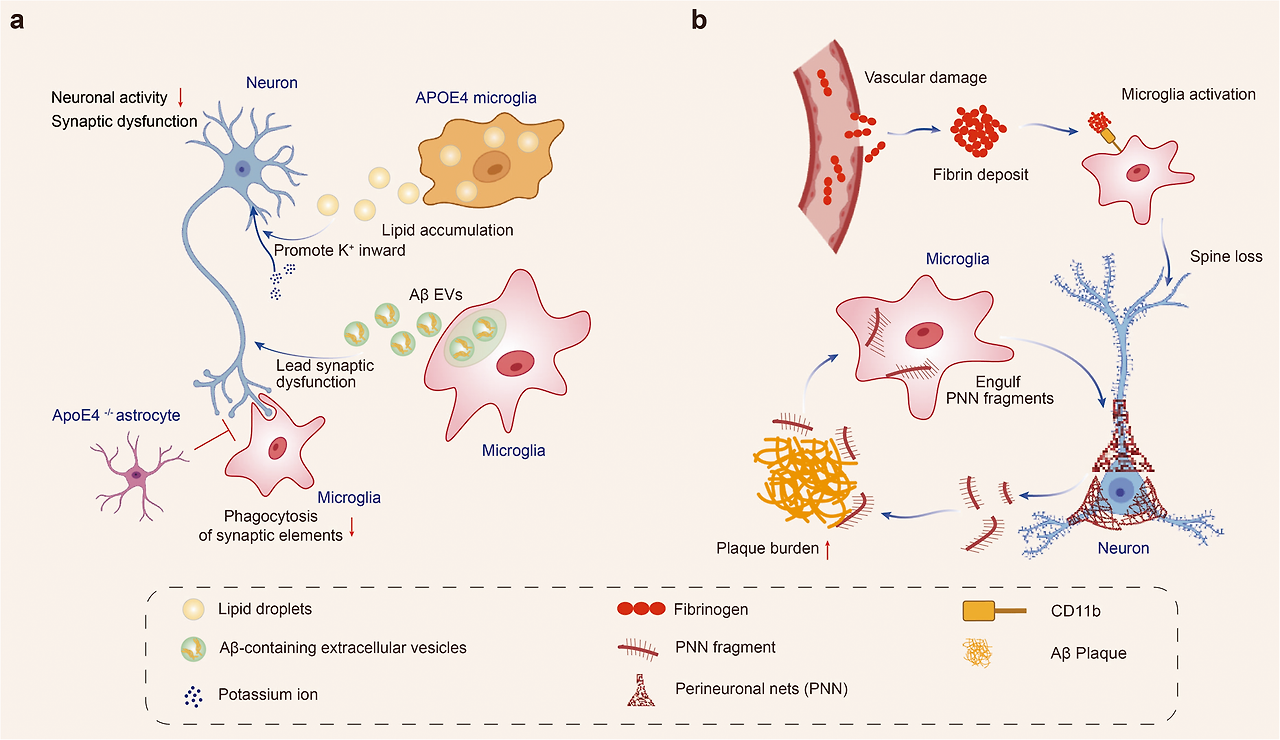
Dysfunctional microglia impair neuronal activity in Alzheimer’s disease. Dysfunctional microglia in AD promotes the clearance of synapses and PNNs and impairs neuronal plasticity and activity. a Microglia harboring an APOE4 allele shows altered cellular metabolism with increased intracellular and extracellular lipid accumulation. The extracellular lipid droplets directly decreased neuronal activity by increasing inward K+ currents. Microglia release Aβ-containing EVs and lead to synaptic dysfunction. Microglial phagocytosis of synapses is affected by astrocytes. Selective removal of astrocytic APOE4 decreases microglial phagocytosis of synaptic elements. b Fibrinogen leaks from the site of cerebrovascular damage into the brain and subsequently binds to the microglial surface receptor CD11b. The interaction of fibrinogen and CD11b mediates microglial activation and leads to spine loss. Microglia engulf perineuronal nets (PNN) and promote plaque-dependent PNN loss. Created with https://BioRender.com
알츠하이머병에서 기능 장애 미세아교세포는 신경 세포 활동을 손상시킵니다. AD에서 기능 장애 미세아교세포는 시냅스와 PNN의 제거를 촉진하고 신경 세포 가소성과 활동을 손상시킵니다. a APOE4 대립유전자를 보유한 미세아교세포는 세포 내 및 세포 외 지질 축적이 증가한 변형된 세포 대사를 보입니다. 세포 외 지질 방울은 내향성 K+ 전류를 증가시켜 신경 세포 활동을 직접 감소시켰습니다. 미세아교세포는 Aβ를 함유한 엑소좀(EVs)을 방출하여 시냅스 기능 장애를 유발한다. 미세아교세포의 시냅스 식균작용은 성상세포에 의해 영향을 받는다. 성상세포의 APOE4 선택적 제거는 미세아교세포의 시냅스 요소 식균작용을 감소시킨다. b 피브리노겐은 뇌혈관 손상 부위에서 뇌로 누출된 후 미세아교세포 표면 수용체 CD11b에 결합한다. 피브리노겐과 CD11b의 상호작용은 미세아교세포 활성화를 매개하여 스파인 손실을 유발한다. 미세아교세포는 신경주위망(PNN)을 포식하며 플라크 의존적 PNN 손실을 촉진한다. https://BioRender.com로 생성됨
Parkinson’s disease
Parkinson’s disease (PD) is the second most common neurodegenerative disease after AD, characterized by motor symptoms consisting of bradykinesia, resting tremor, rigidity, and postural instability and non-motor symptoms including hyposmia, constipation, sleep disorders, and depression. Prevalence and incidence rates of PD in Europe are estimated at 108–257/100,000 and 11–19/100,000, respectively.203 The number of patients with PD in China is estimated to be 3.62 million.204 Pathologically, PD is characterized by the loss of dopaminergic neurons in the substantia nigra pars compacta (SNpc) as well as the accumulation of misfolded α-syn in Lewy bodies. α-syn initially exists as a non-toxic and soluble monomer state. However, its aggregation results in a gain of toxic function.205 α-syn fibrils are the main form of α-syn in Lewy bodies. Several genetic and environmental factors regulate the conversion of α-syn monomers to α-syn fibrils, which involves various cellular and biochemical events.206 The cause of PD is unknown in most cases, but genetic mutations in the PARK genes and environmental factors such as pollutants, pesticides, heavy metals, and infections may increase the risk.207 Two types of PD models are currently used in research: neurotoxin-induced and transgenic. Neurotoxin-induced models use chemicals such as rotenone, 6-hydroxydopamine (6-OHDA), 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP), and paraquat to induce PD-like symptoms. Transgenic models involve genetic modification of PD-related genes such as SNCA, LRRK2, PINK1, PRKN, and DJ-1.208
파킨슨병
파킨슨병(PD)은 알츠하이머병(AD)에 이어 두 번째로 흔한 신경퇴행성 질환으로, 운동 증상(운동 둔화, 안정 시 떨림, 강직, 자세 불안정)과 비운동 증상(후각 저하, 변비, 수면 장애, 우울증)이 특징이다. 유럽의 PD 유병률과 발생률은 각각 10만 명당 108~257명, 11~19명으로 추정된다.203 중국의 PD 환자 수는 약 362만 명으로 추정된다.204 병리학적으로, 파킨슨병은 흑질 밀집부(SNpc)의 도파민 신경세포 소실과 루이체 내 변형된 α-시누클레인의 축적이 특징이다. α-시누클레인은 초기에는 비독성 용해성 단량체 상태로 존재한다. 그러나 응집을 통해 독성 기능을 획득하게 된다.205 α-시누클레인 섬유는 루이체 내 α-시누클레인의 주요 형태이다. 여러 유전적 및 환경적 요인이 다양한 세포 및 생화학적 과정을 통해 α-시누클레인 단량체에서 α-시누클레인 섬유로의 전환을 조절한다.206 대부분의 경우 파킨슨병의 원인은 알려지지 않았으나, PARK 유전자의 유전자 변이 및 오염물질, 농약, 중금속, 감염과 같은 환경적 요인이 위험을 증가시킬 수 있다.207 현재 연구에는 신경독소 유발 모델과 형질전환 모델, 두 가지 유형의 파킨슨병 모델이 사용된다. 신경독소 유도 모델은 로테논, 6-하이드록시도파민(6-OHDA), 1-메틸-4-페닐-1,2,3,6-테트라하이드로피리딘(MPTP), 파라콰트 등의 화학 물질을 사용하여 파킨슨병과 유사한 증상을 유도합니다. 유전자 변형 모델은 SNCA, LRRK2, PINK1, PRKN, DJ-1과 같은 파킨슨병 관련 유전자의 유전자 변형을 포함합니다.208
Microglia response to PD pathology
Microglial activation begins early and persists throughout the course of PD.209 In 1988, reactive microglia were first observed in the substantia nigra (SN) of postmortem brain tissue from PD patients.210 Other microglial activation markers, such as pro-inflammatory enzymes like iNOS and COX211,212 and phagocytosis-associated marker CD68,213 were also upregulated in PD patients. Additionally, PET scans of PD patients revealed widespread microglial activation.214 Notably, microglial activation was discovered not only in individuals with long-term illnesses but also in patients who were just diagnosed.214
Microglia in the SN of PD patients showed a higher proportion of amoeboid morphology, which is indicative of a reactive state.215 It was previously considered that microglia became reactive either towards the M1 pro-inflammatory and neurotoxic phenotype or the alternative M2 immunosuppressive and neuroprotective phenotype.216 However, researchers have called into doubt the M1 and M2 classifications.217 Through snRNA-seq analysis of frozen midbrain tissue from PD patients and controls, seven distinct microglia subpopulations were identified based on the expression of specific marker genes. Among these, the three largest subpopulations were defined by a high expression of P2RY12, HSP90AA1, and GPNMB. The microglial activation trajectory extends from P2RY12high cells to two activation branches, one with highly expressed HSP90AA1 or IL1B241 cells and the other containing GPNMBhigh cells.215 Using scRNA-seq and immunofluorescence analyses in a murine model, the researchers identified a distinct subset of microglia in the midbrain that displayed an intrinsic transcriptional immune alerted signature. Notably, some genes, including Casp4, Ccl4, Cd83, and H2-ab1, were exclusively overexpressed in the immune alerted subset. Interestingly, this subset was absent in other brain regions, such as the striatum. Furthermore, the study found that the microglia in the midbrain had a decreased complexity compared to those in the striatum, showing that midbrain microglia had a muted reaction to an inflammatory stimulus, displaying a tolerogenic rather than primed phenotype.218 In addition, a specific type of microglia, known as Cspg4-expressing microglia, has been identified as having the ability to proliferate triggered by pathological α-syn during neurodegeneration, particularly in PD.219 Overall, these findings provide valuable insights into the heterogeneity of microglia in the nigrostriatal pathway and their potential contributions to PD.
Microglia become reactive, migrate to the damaged sites, produce pro- and anti-inflammatory substances, and may phagocytose cellular debris. The microglial activation and recruitment (microgliosis) process is accompanied by increased cytokine levels.220 Elevated levels of cytokines (including IL1β, IL2, IL6, IFNγ, and TNFα) and CD4+ lymphocytes have been detected in both serum and CSF of PD patients.221,222 By analyzing snRNA-seq data from postmortem midbrain samples of PD patients and controls, the researchers observed an increased number in reactive microglia and a reduction in oligodendrocyte numbers in PD patients. The study also revealed that the reactive microglia states are enriched in cytokine secretion and the stress response to unfolded protein pathways.215 A higher level of NLRP3 inflammasome has been observed in microglial cells in the SN of PD patients, which has been linked to the secretion of pro-inflammatory cytokines associated with neurodegeneration.223,224
Peripheral inflammation can also affect the brain through the blood-brain barrier or the autonomic nervous system, triggering microglial activation and contributing to neurodegeneration.225 The exact contribution of peripheral immune activation versus recruitment and infiltration to this process remains unclear.226 Monocytes and macrophages have been found to infiltrate the inflamed brain. Increased expression of proteins associated with non-microglia myeloid cells, such as CD163, has been observed in the brains of PD patients.227 An increase in the macrophages, specifically CD163+ macrophages was also detected in the area of neurodegeneration in rodent PD models.228 The CCL2-CCR2 axis has been implicated in the infiltration of monocytes into the inflamed brain.229 Studies in PD mouse models and patients have shown upregulation and activation of CCR2, suggesting a detrimental role of infiltrating monocytes in PD. Additionally, differences in CCL2 levels in serum or CSF have been associated with different clinical subtypes of PD.230 Overall, CD163+ and CCR2+ monocytes appear to contribute to neurodegeneration in PD both through peripheral actions and infiltrating the brain. Compared to healthy controls, PD patients had increased frequencies of Th1 cells and higher levels of IL10 and IL17A in their serum. However, microglial activation in the brain of PD patients was not significantly associated with peripheral inflammation markers. These findings suggest that peripheral adaptive immunity might indirectly contribute to microglial activation during the neurodegenerative process in PD.231
파킨슨병 병리에 대한 미세아교세포 반응
미세아교세포 활성화는 초기부터 시작되어 파킨슨병의 전 과정에 걸쳐 지속됩니다.209 1988년, 사후 뇌 조직에서 반응성 미세아교세포가 파킨슨병 환자의 흑질(SN)에서 최초로 관찰되었습니다. 210 iNOS 및 COX와 같은 전염증성 효소211,212 및 식작용 관련 표지자 CD68213과 같은 다른 미세아교세포 활성화 표지자들도 파킨슨병 환자에서 상향 조절되었다. 또한 파킨슨병 환자의 PET 스캔은 광범위한 미세아교세포 활성화를 보여주었다.214 특히, 미세아교세포 활성화는 장기 질환자뿐만 아니라 새로 진단받은 환자에서도 발견되었다.214
파킨슨병 환자의 흑질(SN) 내 미세아교세포는 반응성 상태를 나타내는 아메바형 형태의 비율이 더 높았다.215 기존에는 미세아교세포가 M1형(염증 촉진 및 신경독성 표현형) 또는 대안적 M2형(면역억제 및 신경보호 표현형) 중 하나로 반응성을 보인다고 여겨졌다.216 그러나 연구자들은 M1 및 M2 분류에 의문을 제기했다.217 파킨슨병 환자와 대조군의 냉동 중뇌 조직에 대한 snRNA-seq 분석을 통해 특정 마커 유전자 발현을 기반으로 7개의 서로 다른 미세아교세포 하위 집단이 확인되었다. 이 중 가장 큰 세 하위 집단은 P2RY12, HSP90AA1 및 GPNMB의 높은 발현으로 정의되었다. 미세아교세포 활성화 경로는 P2RY12high 세포에서 두 가지 활성화 분기로 확장되며, 하나는 HSP90AA1 또는 IL1B241 세포가 고도로 발현된 세포이고 다른 하나는 GPNMBhigh 세포를 포함한다.215 생쥐 모델에서 scRNA-seq 및 면역형광 분석을 사용하여 연구진은 중뇌에서 고유한 전사적 면역 경보 서명을 나타내는 미세아교세포의 별개의 하위 집합을 확인했다. 특히, Casp4, Ccl4, Cd83 및 H2-ab1을 포함한 일부 유전자는 면역 경보 하위 집합에서만 과발현되었습니다. 흥미롭게도 이 하위 집합은 선조체와 같은 다른 뇌 영역에서는 발견되지 않았다. 또한, 이 연구는 중뇌의 미세아교세포가 선조체의 미세아교세포에 비해 복잡성이 감소되어 있음을 발견했으며, 이는 중뇌 미세아교세포가 염증 자극에 대해 억제된 반응을 보이며, 준비된 표현형보다는 관용성 표현형을 나타낸다는 것을 보여준다.218 또한, Cspg4 발현 미세아교세포로 알려진 특정 유형의 미세아교세포는 신경퇴행, 특히 파킨슨병(PD)에서 병리학적 α-시누클레오틴에 의해 유발된 증식 능력을 가진 것으로 확인되었다.219 전반적으로, 이러한 발견들은 흑질-선조체 경로 내 미세아교세포의 이질성과 파킨슨병(PD)에 대한 잠재적 기여에 대한 귀중한 통찰력을 제공한다.
미세아교세포는 반응성을 띠게 되어 손상 부위로 이동하며, 친염증성 및 항염증성 물질을 생성하고 세포 잔해를 식균할 수 있다. 미세아교세포 활성화 및 모집(미세아교세포증) 과정은 사이토카인 수치 증가를 동반한다.220 사이토카인(IL1β, IL2, IL6, IFNγ, TNFα) 및 CD4+ 림프구 증가가 PD 환자의 혈청과 뇌척수액 모두에서 검출되었다.221,222 사후 중뇌 샘플의 PD 환자와 대조군에 대한 snRNA-seq 데이터를 분석함으로써, 연구진은 PD 환자에서 반응성 미세아교세포 수가 증가하고 올리고도교세포 수가 감소하는 것을 관찰했다. 이 연구는 또한 반응성 미세아교세포 상태가 사이토카인 분비와 미접힘 단백질 경로에 대한 스트레스 반응이 풍부해짐을 밝혀냈다.215 파킨슨병 환자의 흑질(SN) 내 미세아교세포에서 NLRP3 인플라마좀 수치가 더 높게 관찰되었으며, 이는 신경퇴행과 연관된 전염증성 사이토카인 분비와 관련이 있는 것으로 알려져 있다.223,224
말초 염증은 혈뇌 장벽이나 자율신경계를 통해 뇌에 영향을 미쳐 미세아교세포 활성화를 유발하고 신경퇴화에 기여할 수 있습니다.225 이 과정에서 말초 면역 활성화와 모집 및 침윤의 정확한 기여도는 여전히 불분명합니다.226 단핵구와 대식세포가 염증성 뇌에 침윤하는 것으로 확인되었습니다. PD 환자의 뇌에서는 CD163과 같은 비미세아교세포 골수성 세포와 관련된 단백질의 발현 증가가 관찰되었습니다. 227 설치류 파킨슨병 모델에서 신경퇴행 부위에서도 대식세포, 특히 CD163+ 대식세포의 증가가 검출되었다.228 CCL2-CCR2 축은 염증성 뇌로의 단핵구 침윤과 연관되어 있다.229 파킨슨병 마우스 모델 및 환자 연구에서 CCR2의 상향 조절 및 활성화가 관찰되어, 침윤된 단핵구가 파킨슨병에서 해로운 역할을 함을 시사한다. 또한 혈청 또는 뇌척수액(CSF) 내 CCL2 수치 차이는 파킨슨병의 다양한 임상 하위 유형과 연관성이 확인되었다.230 종합적으로 CD163+ 및 CCR2+ 단핵구는 말초 작용과 뇌 침투를 통해 파킨슨병의 신경퇴화에 기여하는 것으로 보인다. 건강한 대조군에 비해 파킨슨병 환자는 혈청 내 Th1 세포 빈도가 증가하고 IL10 및 IL17A 수치가 높았다. 그러나 파킨슨병 환자의 뇌 내 미세아교세포 활성화는 말초 염증 표지자와 유의미한 연관성을 보이지 않았다. 이러한 결과는 말초 적응 면역이 파킨슨병의 신경퇴행성 과정 중 미세아교세포 활성화에 간접적으로 기여할 수 있음을 시사한다.231
Microglial activation induced by neurotoxins
The byproduct of synthetic heroin, MPTP, could be taken up by dopaminergic neurons and induces parkinsonism in humans, non-human primates, and mice. Astrocytes convert MPTP into MPP+. Dopamine receptors in neurons take up MPP+, which inhibits the mitochondrial complex 1 of the electron transport chain, resulting in ATP depletion and oxidative stress. Ultimately, this leads to the death of dopaminergic cells and the activation of pro-inflammatory microglia.232 Remarkably, reactive M1 microglia were found several years after MPTP exposure in humans and non-human primates exposed to MPTP, indicating a long-lasting reactive microgliosis.233 In rats, 6-OHDA injection also causes reactive microgliosis, which precedes astrogliosis and dopaminergic cell death.234 Additionally, LPS/IFN-γ induces microglial activation, increases exosome release,235 and microglia-derived exosomes facilitate the transmission of α-syn to neurons, accelerating neuronal death.236
신경독소에 의한 미세아교세포 활성화
합성 헤로인의 부산물인 MPTP는 도파민성 뉴런에 흡수되어 인간, 비인간 영장류 및 생쥐에서 파킨슨증후군을 유발할 수 있다. 아스트로사이트는 MPTP를 MPP+로 전환한다. 뉴런의 도파민 수용체는 MPP+를 흡수하며, 이는 전자 전달 사슬의 미토콘드리아 복합체 1을 억제하여 ATP 고갈과 산화 스트레스를 초래한다. 결국 이는 도파민성 세포의 사멸과 염증성 미세아교세포의 활성화를 초래한다.232 주목할 점은, MPTP에 노출된 인간과 비인간 영장류에서 MPTP 노출 수년 후에도 반응성 M1 미세아교세포가 발견되어 장기적인 반응성 미세아교세포증(microgliosis)을 시사한다는 것이다.233 쥐에서는 6-OHDA 주입 역시 반응성 미세아교세포증을 유발하며, 이는 성상세포증 및 도파민성 세포 사멸보다 선행한다.234 또한, LPS/IFN-γ는 미세아교세포 활성화를 유도하고 엑소좀 분비를 증가시키며,235 미세아교세포 유래 엑소좀은 α-시누클레오틴의 뉴런 전파를 촉진하여 뉴런 사멸을 가속화한다.236
Microglial activation and phagocytosis induced by α-syn
Microglia have pattern recognition receptors (PRRs) such as TLRs, nucleotide-binding oligomerization domain (NOD)-like receptors (NLRs), and scavenger receptors (SRs) that enable them to detect and respond to different stimuli, including extracellular α-syn. When α-syn accumulates outside of cells and is not properly cleared, it can activate microglia through PRRs, leading to the release of inflammatory cytokines. Chronic inflammation and neuronal damage contribute to the development of PD.9 Remarkably, neuroinflammation induced by α-syn may occur even before the loss of dopaminergic neurons in PD. Production of neuroinflammation may trigger α-syn oligomerization, leading to a harmful cycle of microglial activation.237
Subsequent investigations of postmortem brain tissue from PD patients revealed that reactive microglia, characterized by amoeboid-shaped morphology, were associated with α-syn pathology in the SN and hippocampus.220 α-syn is primarily located at presynaptic terminals and can be released by neurons through different mechanisms depending on its form. Monomers of α-syn are released passively through compromised cell membranes, while aggregated α-syn is released through non-classical exocytosis or multivesicular bodies. As CNS monitors, microglia take up and degrade α-syn, whose internalization can activate microglia and cause neuroinflammation.238,239 Different conformation states of α-syn can activate microglia in PD, leading to increased secretion of IL-6, IL-1β, and NO.240
Microglia have a high phagocytic capacity. The phagocytic ability of microglia is crucial for α-syn clearance and thus plays a role in the development of PD.241 In PD, α-syn is overexpressed and aggregates into oligomers or protofibrils, which can propagate between cells and disrupt the electrophysiological properties of synapses. These aggregates also act as chemoattractants, directing microglia toward damaged neurons. α-syn overexpression has been shown to drive microglia polarization towards a pro-inflammatory phenotype, resulting in increased production of inflammatory cytokines such as IL-1β, IL-6, and TNF-α, as well as enzymes such as COX-2 and iNOS, and the generation of free radicals.242,243 TLRs, TAM receptors (Tyro 3, Axl, and Mer), scavenger receptors CD14, and TREM-2 all play roles in microglial phagocytosis.81,244,245 TLRs, including TLR2 and TLR4, are receptors expressed on microglia, which were demonstrated to play a role in the uptake of α-syn and the subsequent activation of microglia, boosting α-syn clearance by microglia. Oligomeric α-syn directly engages TLR1/2 and TLR4 to induce a pro-inflammatory M1 phenotype.246,247 CD36 and P2X7 receptors are also involved in microglial activation induced by α-syn.248,249 α-syn-triggered phagocytic activity of microglia is critical for α-syn clearance and prevents accumulation of misfolded α-syn. Extracellular α-syn is taken up by microglia, perhaps via the autophagy receptor p62, and degraded by selective autophagy.239 Although glia can be beneficial in clearing misfolded aggregates in normal physiological conditions, this mechanism may have negative consequences in disease. The uptake and processing of non-toxic α-syn by glia could lead to the generation of toxic strains specific to the disease through autophagy and impaired lysosomal degradation250 (Fig. 3).
α-syn에 의해 유발된 미세아교세포 활성화 및 식작용
미세아교세포는 TLRs, 뉴클레오티드 결합 올리고머화 도메인(NOD)-유사 수용체(NLRs), 스캐빈저 수용체(SRs)와 같은 패턴 인식 수용체(PRRs)를 보유하고 있어 세포외 α-syn을 포함한 다양한 자극을 감지하고 반응할 수 있습니다. 세포 외부에서 α-syn이 축적되고 적절히 제거되지 않을 경우, PRR을 통해 미세아교세포를 활성화시켜 염증성 사이토카인의 분비를 유발할 수 있습니다. 만성 염증과 신경세포 손상은 파킨슨병(PD) 발병에 기여합니다.9 주목할 점은, α-syn에 의해 유발된 신경염증이 PD에서 도파민 신경세포 손실 이전에도 발생할 수 있다는 것입니다. 신경염증의 발생은 α-syn 올리고머화를 촉발하여 미세아교세포 활성화의 유해한 순환을 초래할 수 있다.237
이후 파킨슨병 환자의 사후 뇌 조직 연구에서 아메바 모양 형태를 특징으로 하는 반응성 미세아교세포가 흑질(SN)과 해마에서 α-syn 병리와 연관되어 있음이 밝혀졌다.220 α-syn은 주로 시냅스 전 말단에 위치하며, 그 형태에 따라 신경세포를 통해 다양한 기전으로 방출될 수 있다. α-syn 단량체는 손상된 세포막을 통해 수동적으로 방출되는 반면, 응집된 α-syn은 비고전적 세포외 분비 또는 다중 소포체를 통해 방출됩니다. 중추신경계 감시자로서 미세아교세포는 α-시누클레인을 포식 및 분해하며, 이 내부화는 미세아교세포를 활성화시켜 신경염증을 유발할 수 있다.238,239 α-시누클레인의 다양한 구조 상태는 파킨슨병에서 미세아교세포를 활성화시켜 IL-6, IL-1β 및 NO 분비를 증가시킬 수 있다.240
미세아교세포는 높은 식세포 능력을 지닌다. 미세아교세포의 식작용 능력은 α-시누클레인의 제거에 결정적이며, 따라서 파킨슨병 발병에 역할을 합니다.241 파킨슨병에서 α-시누클레인은 과발현되어 올리고머나 프로토피브리일로 응집되며, 이는 세포 간 전파되어 시냅스의 전기생리학적 특성을 교란시킵니다. 이러한 응집체는 또한 화학유인물질로 작용하여 미세아교세포를 손상된 뉴런 쪽으로 유도합니다. α-syn 과발현은 미세아교세포를 염증 유발형 표현형으로 분극화시켜 IL-1β, IL-6, TNF-α와 같은 염증성 사이토카인 및 COX-2, iNOS와 같은 효소의 생산 증가와 자유 라디칼 생성을 유발하는 것으로 밝혀졌다.242,243 TLRs(TLR2 및 TLR4 포함), TAM 수용체(Tyro 3, Axl, Mer), 스캐빈저 수용체 CD14, TREM-2는 모두 미세아교세포의 식작용에 관여한다.81,244,245 TLR2 및 TLR4를 포함한 TLRs는 미세아교세포에 발현되는 수용체로, α-syn의 포획 및 후속 미세아교세포 활성화에 관여하여 미세아교세포에 의한 α-syn 제거를 촉진하는 것으로 입증되었다. 올리고머화된 α-syn은 TLR1/2 및 TLR4를 직접 결합하여 염증성 M1 형질을 유도한다.246,247 CD36 및 P2X7 수용체도 α-syn에 의해 유발된 미세아교세포 활성화에 관여한다.248,249 α-syn에 의해 유발된 미세아교세포의 식작용 활성은 α-syn 제거에 중요하며, 잘못 접힌 α-syn의 축적을 방지한다. 세포외 α-syn은 아마도 자가포식 수용체 p62를 통해 미세아교세포에 흡수되어 선택적 자가포식에 의해 분해됩니다.239 정상적인 생리학적 조건에서는 신경교세포가 잘못 접힌 응집체를 제거하는 데 도움이 될 수 있지만, 이 메커니즘은 질병에서는 부정적인 결과를 초래할 수 있습니다. 글리아에 의한 비독성 α-syn의 흡수 및 처리는 자가포식과 리소좀 분해 장애를 통해 질병 특이적인 독성 변이체의 생성을 초래할 수 있습니다250 (그림 3).
Fig. 3
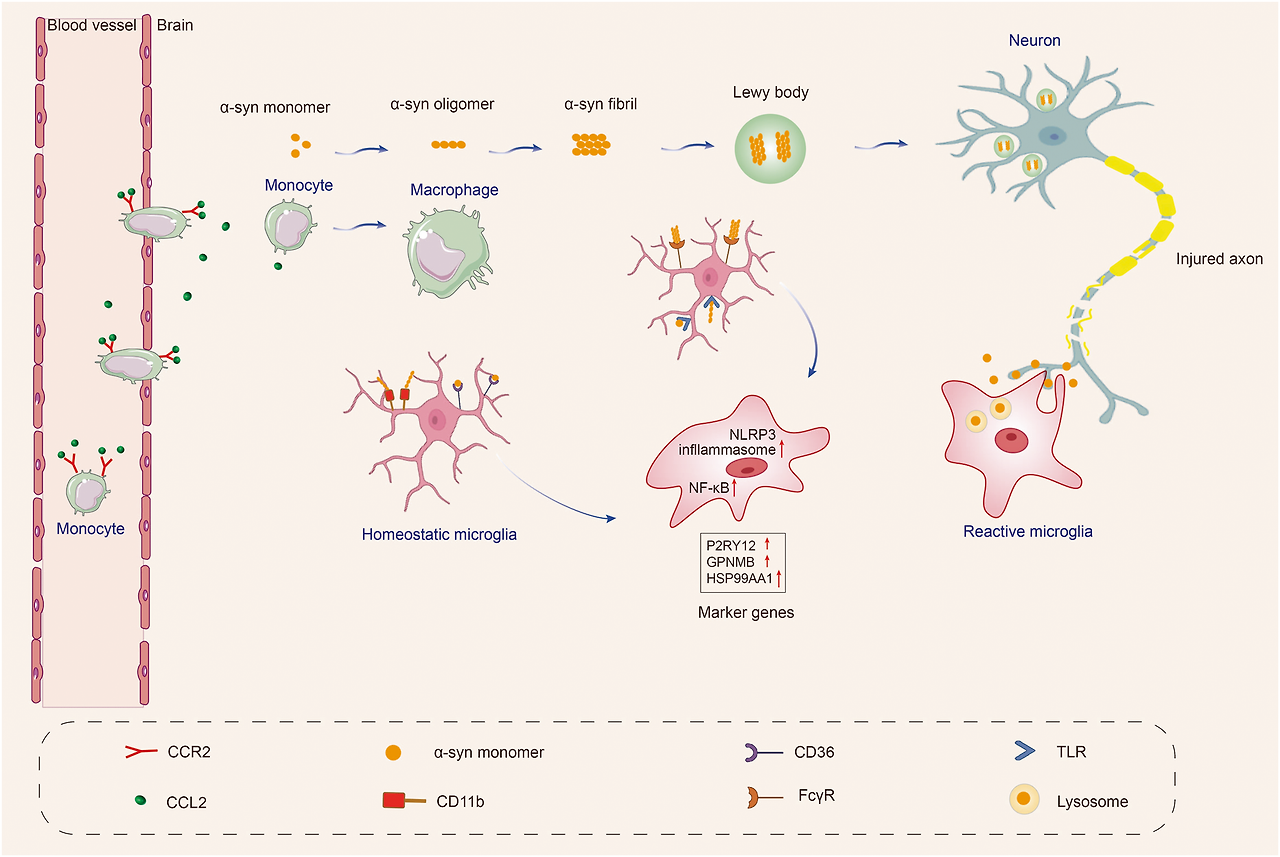
α-syn resulting in microglial response in Parkinson’s disease. Microglia are activated by α-syn, which can be encountered through phagocytosis of synapses or exocytosis from neighboring neurons. Different forms of α-syn, including monomeric, oligomeric, and fibrillar, can be encountered as the disease progresses. The recognition, uptake, and phagocytosis of α-syn by microglia are dependent on the type of α-syn encountered and the involved receptors and proteins. α-syn has been shown to initiate a pro-inflammatory response by interacting with membrane receptors that activate NF-κB through various mediators and assemble the NLRP3 inflammasome, leading to the production of inflammatory mediators and free radicals. The CCL2-CCR2 axis is involved in the infiltration of monocytes into the inflamed brain. Upregulation and activation of CCR2 have been observed in PD mouse models and patients, indicating a potentially harmful role in infiltrating monocytes in PD. Local cytokine and tissue signals can then induce the transformation of monocytes to macrophages. These cascades also result in the proliferation and migration of microglia. Created with https://BioRender.com
Crosstalk between microglia and neuron in PD
Several studies have revealed that the CX3CR1 receptor expressed on microglia is critical in neuron-microglia communication. This receptor specifically recognizes the protein CX3CL1.251 Studies have suggested that the CX3CL1-CX3CR1 signaling pathway is essential for maintaining a healthy balance in microglial activity, regulating chemoattraction and synaptic plasticity, and reducing microglia-mediated inflammation and neurotoxicity.252 Another protein that regulates microglial activation is CD200, which is expressed on the surface of neurons and interacts with microglial CD200R. Dysregulation of the CD200-CD200R pathway has been linked to increased microglial activation and degeneration of dopaminergic neurons.253 Besides, CB1 receptors are abundant in neurons, while CB2 receptors are primarily expressed in microglia in the brain. Several animal models of PD show that microglial CB2 receptor activation is neuroprotective and improves motor symptoms.254,255
Genetic mutations and microglial cell activity in PD
Among the genes linked to familial PD, some are involved in inflammatory processes. For example, mutations in SNCA have been proposed to cause aberrant conformation in α-syn, resulting in enhanced conversion of soluble α-syn into insoluble aggregates identified in PD.256 Extracellular α-syn exposure increases pro-inflammatory cytokine production in microglial cells.
LRRK2 (PARK8) gene mutations are the most common genetic cause of both familial and sporadic PD.257 Previous studies have shown that LRRK2 expression is particularly high in various immune cells, including microglia, macrophages, and monocytes. In contrast, its expression in T cells is relatively low.258,259 These findings suggest that LRRK2 may primarily modulate the innate immune system and inflammation in PD. Research on microglia has shown that TLR2 or TLR4 stimulation can increase the expression and phosphorylation of LRRK2.259,260 The researchers identified microglia-specific chromatin regions that regulated LRRK2 expression and showed that a specific regulatory DNA element containing the PD-associated genetic variant rs6581593 modulates LRRK2 expression in microglia. These findings highlight the importance of considering cell type when studying the impact of non-coding genetic variants on disease pathogenesis and provide mechanistic insight into the association between the 5’ region of LRRK2 and PD risk.261 Furthermore, inhibition of LRRK2 kinase activity can lead to the phosphorylation of NF-κB inhibitory subunit p50 at the protein kinase A (PKA) -specific phosphorylation site S337. This results in an abnormally higher proportion of nuclear P-p50, which may inhibit the function of NF-κB, preventing efficient DNA binding and gene transcription activation in response to inflammation.262
PARK7 encodes a tiny peptidase protein known as DJ-1. DJ-1 dysfunction is implicated in a small percentage (1–2%) of inherited forms of early-onset PD.256 In microglia, the knockdown of DJ-1 has been shown to enhance the production of inflammatory cytokines in response to LPS.263 Additionally, DJ-1 may function as a scaffold protein facilitating the interaction between signal-transducers and activators of transcription (STAT1) and its phosphatase, Src-homology 2-domain containing protein tyrosine phosphatase-1 (SHP-1) that negatively regulates inflammatory responses of microglia. In DJ-1 KO mice, microglia exhibited increased expression of phosphorylation levels of STAT1, as well as inflammatory mediators COX-2, iNOS, and TNF-α.264 In addition, microglia lacking DJ-1 showed increased mitochondrial activity, leading to elevated levels of ROS compared to normal microglia, and this effect was further increased by treatment with LPS.265
The investigation of genetic mutations associated with microglia significantly enhances our comprehension of the cellular pathways involved in PD. By unraveling these molecular mechanisms, we gain valuable insights into the underlying causes and potential therapeutic targets by modulating specific genes to restore or modify microglia function.
Multiple system atrophy
Multiple system atrophy (MSA) is a rare, progressive, and fatal neurodegenerative disease characterized by autonomic dysfunction, parkinsonism, and cerebellar ataxia.266 Incidence rates are estimated at 0.6–0.7 cases per 100,000 person-years.267 Depending on the predominant symptom, MSA is clinically classified into two subtypes: MSA with predominant cerebellar ataxia (MSA-C) and MSA with predominant parkinsonism (MSA-P), whereas olivopontocerebellar atrophy and striatonigral degeneration represent pathological variants, respectively.268 Many MSA patients, however, show a combination of both types.269 MSA is an adult-onset disorder; the onset age is 56 ± 9 years old.270 In MSA, most patients die within 6 to 10 years of diagnosis.266 The pathological hallmark of MSA is the abnormal accumulation of α-syn in the cytoplasm of oligodendrocytes, named glial cytoplasmic inclusions (GCIs).271,272,273,274,275 Mechanismly, various factors including the abnormal accumulation of α-syn, microglial activation and neuroinflammation,276 autophagic impairment,277,278,279 mitochondrial,280 and proteasomal dysfunction281,282 are involved in the pathogenesis of MSA.
Microglial activation in MSA brains
The exact pathogenesis of MSA remains a mystery, despite the suspicion of several players contributing to neurodegeneration. But according to pathological studies and PET imaging of MSA brains, microglial activation and neuroinflammation constitute important features of MSA.283,284,285,286,287 Histopathologically, microglial activation was found to be prominent in regions of motor-related structures, including cerebellar input, extrapyramidal and pyramidal motor structures, demonstrating that the mode of microglial activation was consistent with the known pattern of MSA-specific system degeneration,283 which suggests that microglial activation likely promotes neurodegeneration in MSA. In addition, the stereology method was used to estimate the number of neurons and glial cells (microglia, oligodendrocytes, astrocytes) in the neocortex of 11 MSA and 11 controls284 and white matter of 10 MSA and 11 controls.285 The results showed significant widespread microgliosis in both neocortex and white matter in MSA patients compared with controls.284,285
PET imaging also demonstrated microglial activation in the brains of patients with MSA. In a study utilizing [11C](R)-PK11195 PET imaging to localize microglial activation in 14 MSA patients and 10 controls, it was found that MSA-P patients had significantly higher binding potentials in the precentral gyrus, caudate nucleus, putamen, pallidum, orbitofrontal cortex, superior parietal gyrus and presubgenual anterior cingulate cortex than controls.286 Notably, the mean disease duration of these MSA-P patients was 2.9 years (range 2–5 years),286 suggesting widespread microglial activation occurs early in the clinical stage of MSA. Interestingly, a recent study using [11C] PBR28 PET imaging compared the pattern of microglial activation between 66 MSA (30 MSA-P and 36 MSA-C) and 24 PD patients and observed a conspicuous pattern of increased microglial activation in the cerebellar white matter and lentiform nucleus in MSA compared with PD.287 This pattern by visual reading achieved 100% specificity and 83% sensitivity in discriminating MSA from PD,287 suggesting that microglial activation has a specific pattern in MSA, although microglial activation has been considered a common immune response in neurodegenerative diseases.288
Microglial activation is associated with α-syn deposition
The neuropathological hallmark lesion of MSA is the presence of GCIs, located in oligodendrocytes.289 A significant constituent of GCI is insoluble α-syn. Evidence is still lacking concerning whether microglial activation precedes the emergence of GCIs. However, α-syn species are believed to activate microglial cells, accelerating neurodegeneration in MSA.290 Histopathological studies showed that microglial activation increased in regions with a high α-syn load in MSA patients.291 For example, microglial activation was evident in white matter where α-syn inclusions were abundantly observed.291 Transgenetic mouse models of MSA overexpressing α-syn in oligodendrocytes also presented early and significant microglial activation and related neuroinflammation accompanying the α-syn accumulation in oligodendrocytes.292,293 However, α-syn aggregation, microglial activation, and neuronal death usually coexist in the same brain regions, so does microglial activation secondary to α-syn aggregation or neuronal loss? Several studies exposed primary microglia to α-syn monomers or high-ordered oligomers. They found that high-ordered oligomers rather than monomers induced microglial activation identified by both morphological changes from bipolar to amoeboid and biochemical activation profiles manifested with increased pro-inflammatory cytokines secretion.294 The α-syn-induced microglial activation depends on TLRs 1/2 signaling294 and TLR4 signaling.246 The above evidence indicates that via a specific interaction with TLRs, the misfolded α-syn directly activates microglia and promotes the production and release of pro-inflammatory cytokines.
Microglial roles in the pathogenesis of MSAPhagocytosis impairment
TLR4-mediated microglial phagocytosis of α-syn in MSA. TLR4 gene ablation in a transgenic mouse model of MSA with oligodendroglial α-syn overexpression impaired the phagocytic ability of microglia to α-syn, leading to enhanced motor impairment and augmented loss of nigrostriatal dopaminergic neurons.295 In contrast, TLR stimulation with a TLR4 selective agonist (monophosphoryl lipid A) in the same MSA mouse model ameliorated motor deficits and rescued nigral neurodegeneration.245 In MSA brains, increased brain levels of α-syn were linked to disturbed TLR4-mediated microglial phagocytosis of α-syn.295 Evidence consistently showed that microglia could phagocytize α-syn, but excessive uptake of α-syn by microglia led to neurodegeneration. A study generated a mouse model by lentiviral-mediated selective α-syn accumulation in microglial cells in substantia nigra and found that these mice developed progressive degeneration of dopaminergic neurons. Mechanistic studies have found that α-syn aggregated in microglia led to a significant decrease in the phagocytic ability of microglia and triggered an inflammatory response, increasing the release of pro-inflammatory factors, ROS, and nitric oxide by microglia, which created a toxic environment eventually led to neurodegeneration295 (Fig. 4).
Fig. 4
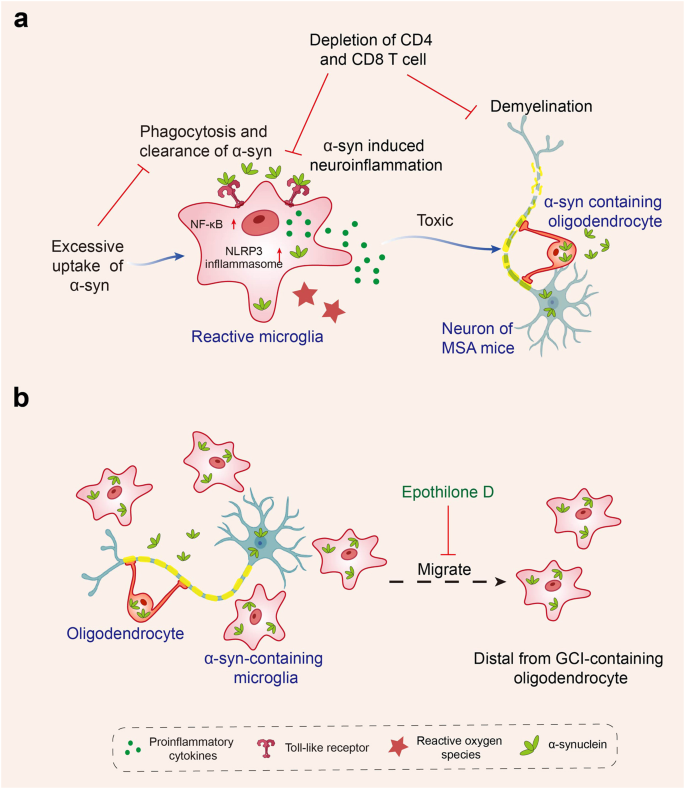
Microglial roles in the pathogenesis of multiple system atrophy. a α-syn can interact with microglial toll-like receptors (TLRs) and then was phagocytosed by microglia in an MSA mouse model. But excessive uptake of α-syn by microglia led to a significant decrease in the phagocytic ability of microglia, triggered an inflammatory response of microglia including NF-κB and NLRP3 inflammasome signaling activation, reactive oxygen species production, pro-inflammatory cytokines upregulation, and eventually induced neurodegeneration. Besides, CD4 and CD8 T cell depletion attenuated α-syn-induced inflammation and demyelination in MSA mice. b Microglia act as a mobile vehicle to propagate α-syn after phagocytosis of α-syn in MSA patients. An in vitro study showed the ability of microglia to transport α-syn distally was impaired when treated with Epothilone D, a natural product that can inhibit microtubule activity. Created with https://BioRender.com
Neuroinflammation
TLR4-mediated α-syn phagocytosis by microglia245,246,295 and induced NF-κB translocation, ROS production, and the release of pro-inflammatory cytokines such as TNF-α.246,296 Besides, the activation of microglia by α-syn was also dependent on TLR1/2 signaling,294 suggesting a modulatory role of TLRs on α-syn induced microglial pro-inflammatory responses and ROS release. Thus, misbalanced TLRs signaling may be crucial for MSA progression. Significantly increased levels of TLR-4 and TLR-1 were observed in multiple brain regions, such as substantia nigra and striatum, in MSA patients versus controls.297 Upregulated TLRs are a double-edged sword. It may have a protective effect by increasing the phagocytosis of α-syn by microglia, but as a result, it induces neuroinflammation and promotes neurodegeneration. Besides, NLRP3 inflammasome is probably involved in neuroinflammation in MSA. It triggers pyroptotic cell death in microglia and astrocytes by producing IL-1β and IL-18 pro-inflammatory cytokines.298 Immunohistochemical staining of postmortem brains found that the NLRP3 inflammasome was significantly upregulated compared with controls and was significantly correlated with the deposition of GCIs and neurodegeneration in the putamen of MSA299 (Fig. 4). The above evidence suggests that the NLRP3 inflammasome may be related to neurodegeneration in MSA. Whether and how the NLRP3 inflammasome participates in MSA pathogenesis needs further research.
Propagation of α-syn
A recent study observed the brain tissue sections of MSA patients by immunofluorescence and found that some α-syn-containing microglia were distal from GCI-containing oligodendrocytes,300 so it was speculated that these microglia acted as a mobile vehicle to propagate α-syn in MSA after uptaking of α-syn instead of degrading these misfolded proteins in place.300 In vitro experiments confirmed this hypothesis. In an in vitro culture system, α-syn was immobilized in the center of a glass coverslip and then treated either with microglia-like differentiated THP-1 cells or undifferentiated THP-1 cells. The proportion of α-syn-containing differentiated THP-1 cells was significantly increased in distant regions of α-syn compared with undifferentiated cells.300 The ability of microglia to transport α-syn distally was impaired when microtubule activity was inhibited with Epothilone D (EpoD)300(Fig. 4). Therefore, it is proposed that inhibiting microglial migration may be one of the therapeutic strategies to reduce the α-syn spreading.300 However, blocking the migration of microglia may also weaken microglial physiological function. Thus, specifically inhibiting the migration of α-syn transporting cells may offer a more effective and promising therapeutic approach in the future.
T cell involvement
T cell infiltration alongside the inflammatory microgliosis was observed both in postmortem brain tissues of MSA patients and in a virus-mediated mouse model of MSA.301 Meanwhile, in the same MSA mouse model, the proportion of Th1 T cells and the level of INF-γ cytokine in the striatal tissue were significantly increased.301 Moreover, MSA mice with Tcrb (CD4 and CD8 T cell knockout) or Cd4 (CD4 T cell knockout) genetic deletion showed reduced inflammation and demyelination after exposure to syn301 (Fig. 4). Therefore, a hypothesis is proposed: α-syn in oligodendrocytes induces microglial activation, and then the microglial signals trigger CD4 + T cell infiltration. After CD4+ T cells infiltrate the CNS, their T cell receptor binds to the upregulated MHCII on the surface of microglia, which promotes the differentiation of CD4 T cells into Th1 T cells and secretes INF-γ. All these pro-inflammatory cells, including microglia and CD4 T cells, cause oligodendrocyte dysfunction and striatal and corpus callosum demyelination. These results suggest that T cell infiltration into the CNS and their interaction with microglia are key mechanisms of disease pathogenesis in MSA.301
Amyotrophic lateral sclerosis and frontotemporal dementia
Amyotrophic Lateral Sclerosis (ALS) is characterized by the loss of motor neurons in the cortex, brainstem, and spinal anterior horn. The median survival time from the onset of symptoms for ALS is 30 months.302 Mutation in C9orf72 accounts for 40% of familial ALS and FTD cases.303,304 Mutations in the SOD1 gene (encoding superoxide dismutase 1) occur in ~20% of cases,305 while mutations in TARDBP (encoding TAR DNA- binding protein 43 [TDP43])306 and FUS (encoding the fused in sarcoma protein) have a lower frequency (<5%).307 Postmortem studies308,309,310 and in vivo PET studies311,312,313 revealed widespread cerebral microglial activation in patients with ALS,308,309,310,311,312 and even in pre-symptomatic ALS-related mutation carriers.309,313 Microglial activation in the corticospinal tract of ALS correlated with neuronal and axonal loss and more severe upper motor neuron symptoms.309 Microglial activation in middle frontal and superior or middle temporal gyrus regions was also highly found in vivo PET imaging studies in humans, indicating a pivotal role for microglia in ALS. However, whether the involvement of microglial activation is beneficial or detrimental remains unclear. Therefore, the researchers employed various transgenic mouse models to study the functional or pathological role of microglia in ALS pathogenesis.
Frontotemporal dementia (FTD) is the second most common form of dementia after AD in people among people under 65, and is characterized by progressive cognitive, behavioral, and language dysfunction. Pathological studies have shown the deposition of abnormal proteins in the brain tissues of FTD patients, including TDP-43 (50% of cases), tau (40% of cases), and FUS (5–10% of cases).314,315 Gene mutation is an important pathogenic factor for FTD. It is estimated that 60% of patients with FTD have autosomal dominant mutations in C9orf72, GRN, or MAPT genes.316 Additionally, mutations in TBK1 are associated with developing FTD,317,318 and variants in TREM2 increase an individual’s risk of developing FTD.319 In vivo PET studies320,321 and immunohistochemistry studies322,323,324 have found increased microglial activation in the frontal and temporal cortices of patients with FTD.
Introduction of commonly used animal models of ALS and FTD
Several experimental animal models have been established, given the pathogenic mutations found in ALS and FTD. The human SOD1 mutant mice (mSOD1) are widely used as ALS models because they exhibit progressive paralysis, pathological protein aggregation, motor neuron degeneration, and gliosis, which are hallmarks of ALS patients.325,326,327 However, neuron-specific expression of mSOD1 in transgenic mice failed to produce pathology or disease in these mice,328,329 suggesting a role of non-cell-autonomous factors, possibly from non-neuronal cells such as microglia, in ALS pathogenesis. Microglial activation was observed in SOD1 models, and microglial activation was detected before the onset of clinical disease in some studies.330,331 Several studies have demonstrated the role of microglia in ALS mSOD1 mouse models.
Ninety-seven percent of patients with ALS and 50% of patients with FTD have cytoplasmic TDP-43 aggregates within neurons,332 and mutations in TARDBP, the gene encoding TDP-43, have been identified in patients with ALS or FTD,306,333 indicating a mechanistic link between TDP-43 and ALS/FTD and also suggesting a common underlying mechanism, which prompts the use of TDP-43 mutant transgenic mice to study TDP-43-related neurodegeneration in ALS and FTD. In TDP-43 mouse models, pathogenesis is involved in a combination of loss of nuclear TDP43 function and TDP-43 cytoplasmic gain-of-toxic-function.334
C9orf72 intronic hexanucleotide repeat expansion (GGGGCC) was identified as the most common genetic cause of FTD and ALS.304,335 The mechanism by which these repeat expansions may cause disease is outlined in three hypotheses: first, downregulation of gene expression (haploinsufficiency) leads to a loss of C9orf72’s normal cellular function; second, the presence of sense and antisense RNA foci could sequester RNA-binding proteins, resulting in splicing defects in RNA metabolism; and third, the formation of repeat-associated non-ATG-translated dipeptide repeat proteins (DPRs) may cause neurodegeneration due to gain-of-function toxicity.336 Tansgenetic mouse models have been used to examine the role of C9orf72 and its hexanucleotide repeat expansion in the pathogenesis of FTD and ALS, and the results suggest that the microglia are involved in C9orf72-mediated ALS/FTD pathogenesis.
Heterozygous GRN mutations cause the deficiency in progranulin (PGRN), a lysosomal and secreted protein, and contribute to the development of FTD,337 while the homozygous GRN mutation leads to neuronal ceroid lipofuscinosis.338 PGRN is expressed in microglia and neurons and shows higher expression once microglia respond to the changes in their CNS environment. Grn loss of function causes microglial activation,339,340 cytosolic phosphorylated TDP-43 aggregation,339,340 myelin debris accumulation in white matter, and spatial learning and memory impairment in Grn -/- mice.340
Microglial roles in pathogenesis of ALS and FTDPhagocytosis of microglia
Microglia could phagocytize mobile TDP-43 deposits within degenerating motor neurons.341 There is also evidence that microglia actively facilitate the clearance of hTDP-43 in a transgenic TDP-43 mouse model.342 Nonsense or missense mutations in TREM2 have been identified in several families with FTD.343,344,345 One study comprising 609 patients with FTD and 1957 controls found that the TREM2 p.R47H variant is a risk factor for FTD (OR = 5.06; p-value = 0.001).346 Homozygous TREM2 p.T66M mutation has also been identified to cause FTD-like syndrome.344 Recently, Xie et al. found that TDP-43 interacted with microglial TREM2 and induced TREM2-dependent microglia with phagocytic ability that facilitated clearance of TDP-43.347 In mice lacking TREM2, microglia were locked in a homeostatic state, and TDP-43 clearance by microglia was reduced, leading to increased neuronal damage and motor impairments.347 This finding may partly explain the link between the TREM2 mutant and the FTD-like manifestation.
In the CNS, Grn loss of function profoundly impacts the microglial state and function, which plays a critical role in FTD pathogenesis. Deficiency of Grn caused synaptic loss by microglia-mediated synaptic pruning via complement involvement as deletion of the C1qa gene (which encodes complement C1q subcomponent subunit A) significantly reduced synaptic pruning by Grn-/-microglia, and ameliorated behavioral deficits, neuronal cell loss and increased survival in Grn-/- mice.348 Grn deficiency led to microglial lysosomal dysfunction and a reduced ability to degrade myelin debris, thus leading to the accumulation of myelin debris in microglial lysosomes and increased microgliosis and myelin debris accumulation in the white matter of Grn−/− mice and patients with GRN-associated FTD.349
Overall, microglia could phagocytize pathological protein deposits such as TDP-43, and the interaction of TDP-43 with microglial TREM2 promotes the phagocytosis and clearance of TDP-43 by microglia. In the disease state, microglial lysosomes undergo dysfunction, which reduces the clearance of deposited protein and myelin debris and accumulates myelin debris in the white matter. In addition, microglia increase synaptic pruning through interaction with complement, which exacerbates neuronal loss and behavioral abnormalities. The above dysfunctional modulation will promote the occurrence and development of the disease.
Neuroinflammation
TDP-43 protein could be secreted into the extracellular matrix via exosomes350 or cell death. Increased levels of TDP-43 in CSF have been detected in patients with ALS351,352 and FTD.352 In vitro studies found when WT or various forms of mutant TDP43 protein or TDP43 aggregates were added to primary microglial cultures, they were internalized, leading to microglial activation, NLRP3 inflammasome and pro-inflammatory markers upregulation, in which mutant TDP43 eliciting a more pronounced response.353 These TDP-43 proteins or aggregates-induced microglial activation and neuroinflammation have neurotoxic effects on co-cultured motor neurons.354 Notably, in the absence of microglia, added TDP-43 proteins were not toxic to cultured primary motor neurons,354 suggesting the involvement of non-cell autonomous pro-inflammatory effects mediated by microglia that enhance motor neuron injury. Therefore, in the context of the TDP-43 mouse model, microglia can phagocytize pathological TDP-43 to play a protective role and drive neuroinflammation, resulting in neuronal damage.
The anti-inflammatory cytokine IL-10 was upregulated in microglia at pre-symptomatic stages in SOD1 mice. In vitro studies found that upregulated IL-10 delayed the occurrence of the disease.355 Another study also found that microglia presented an anti-inflammatory phenotype in SOD1G93A mice at disease onset and were neuroprotective to motor neurons. In contrast, microglia presented a pro-inflammatory phenotype at end-stage disease and were neurotoxic to motor neurons.356 Reduced mutant levels in microglia did not have much effect on early disease progression, but substantially slowed it later on,306 emphasizing that microglia in the late stage accelerate disease progression. These findings suggest that modulating microglial phenotype to avoid its conversion to a pro-inflammatory state during disease progression will be helpful for the treatment of ALS.
Grn deficiency leads to NF-κB activation in microglia and elevation of TNFα, leading to hyperexcitability of medium spiny neurons and obsessive-compulsive disorder-like behavior.357 Recently, interleukin-18 receptor accessory protein (IL18RAP) 3′ untranslated region (3′UTR) variants were identified as protective factors which reduced the risk of developing ALS fivefold, delayed onset, and therefore the age of death in individuals with ALS. The 3′ untranslated region (3′UTR) variants of interleukin-18 receptor accessory protein (IL18RAP) has been identified as protective factors in ALS patients. They reduced the risk of developing ALS fivefold.358 These variants in the IL18RAP 3′UTR reduce mRNA stability and the binding of double-stranded RNA (dsRNA)-binding proteins. Mechanistically, IL18RAP is upstream of NF-κB; thus, the variants downregulate IL18RAP–NF-κB signaling in microglia. This study highlights the protective effect of alleviating microglia-mediated neurotoxicity in ALS.
Phenotype switching of microglia contributes to disease progression
Homeostatic microglia are protective against ALS. Antibiotic administration to SOD1 mice altered gut microbiota composition, weakened motor function, and caused death in the SOD1 mice. There was a downregulation of homeostatic genes and an increase in neurodegenerative genes in microglia after antibiotic treatment, and the microglia signature change preceded changes in motor function.359 Grn loss of function promoted the microglial transition from a homeostatic to a disease-specific state, aggravated TDP-43 pathology and neurodegeneration through the synergy of microglia and the complement system since deleting the genes for C1qa and C3 mitigated microglial toxicity and rescued TDP-43 proteinopathy and neurodegeneration.360
Microglia showed higher levels of C9orf72 expression than other cell types in the brain,361 and research suggests that C9orf72 is required for the normal immune function of myeloid cells. In the C9orf72–/– mice, progressive splenomegaly, lymphadenopathy, and upregulation of pro-inflammatory cytokines were observed at the periphery, while brain and spinal cord microglia showed an inflammatory state.361 C9orf72 is important for maintaining microglia homeostasis. Transcriptome and histologic analyses of postmortem tissue from patients with ALS carrying the C9orf72 expansion (C9-ALS) found that decreased C9orf72 expression in C9-ALS led to altered microglial function and increased microglial activation.309,361 In Lall et al.’s study, Cd11b+ isolated microglia from young (3 months) and aged (17 months) C9orf72+/+, C9orf72+/-, and C9orf72-/- mice were analyzed by RNA-seq. Results showed that loss of C9orf72 promoted microglial gene signature transition from homeostatic to an inflammatory state characterized by an enhanced type I IFN signature. Co-cultured C9orf72+/+ or C9orf72-/- microglia with WT cortical neurons found that loss of C9orf72 in microglial cells promoted microglial phagocytosis and neuronal synaptic loss. Thus, the authors argued that microglial impairment from decreased C9ORF72 expression directly contributed to neurodegeneration in C9-ALS.362 Although the loss of C9orf72 alone is insufficient to cause ALS motor deficits,363 the loss of function of C9ORF72 may lead to microglial dysfunction, which may accelerate disease progression in C9ALS/FTD patients.
Peripheral immune cells are involved in the regulation of microglia
In SOD1 mutant mice, reactive macrophages along peripheral axons of motor neurons were observed during disease progression. Replacing peripheral nerve macrophages at disease onset suppressed peripheral macrophage inflammation, reduced microglial pro-inflammatory responses, and prolonged survival in mice.364 NK cell infiltration into the spinal cord and cerebral motor cortex was observed in sporadic ALS patients and an ALS mouse model (SOD1G93A). NK cell depletion induced a protective microglial phenotype and increased survival in the ALS mouse models (hSOD1G93A and TDP43A315T). The above evidence suggests that peripheral immune cells shape microglia into a pro-inflammatory phenotype and accelerate disease progression in ALS365 (Fig. 5).
Fig. 5
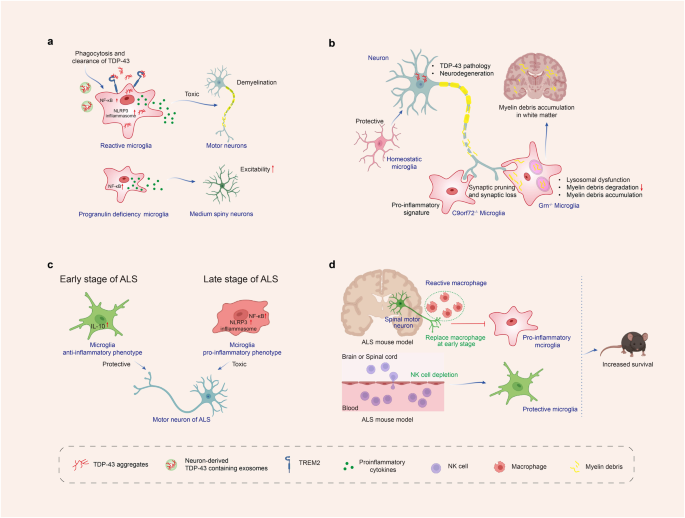
Microglial roles in the pathogenesis of amyotrophic lateral sclerosis and frontotemporal dementia. a TDP-43 could be released into the extracellular matrix via exosomes or cell death. TDP-43 interacted with microglial TREM2 and then increased their phagocytosis and clearance by microglia. Phagocytosis of TDP43 aggregates by microglia led to microglial activation, microglial NLRP3 inflammasome activation, and pro-inflammatory markers upregulation, which have neurotoxic effects on motor neurons. Besides, progranulin deficiency in microglia activated microglial NF-κB signaling and promoted the release of pro-inflammatory cytokines, leading to hyperexcitability of medium spiny neurons. b Homeostatic microglia are protective against ALS. Progranulin deficiency aggravated TDP-43 pathology, promoted synaptic pruning by microglia, and led to synaptic loss and neurodegeneration. Progranulin deficiency also led to microglial lysosomal dysfunction and reduced myelin debris degradation, leading to the accumulation of myelin debris in white matter. Besides, C9orf72 loss of function promoted microglial gene signature transition from a homeostatic to an inflammatory state and promoted synaptic pruning by microglia and synapse loss in neurons. c At the early stage of the ALS mouse model (SOD1 mice), the anti-inflammatory cytokine IL-10 was upregulated in microglia, and microglia presented with an anti-inflammatory phenotype, which was neuroprotective to motor neurons. But at the late stage, microglia presented with a pro-inflammatory phenotype, which was neurotoxic to motor neurons. d Peripheral nerve reactive macrophages along peripheral axons of motor neurons were activated in an ALS mouse model (SOD1 mutant mice). Replacing peripheral nerve macrophages at disease onset reduced microglial pro-inflammatory responses and prolonged survival in these mice. NK cell infiltration into the cerebral motor cortex and spinal cord was observed in an ALS mouse model (SOD1G93A). NK cell depletion induced a protective microglial phenotype and increased survival in these mice. Created with https://BioRender.com
Progressive supranuclear palsy
Progressive supranuclear palsy (PSP) encompasses a range of clinical phenotypes involving movement, behavioral abnormalities, and language impairments.366 PSP has a prevalence rate of around 0.9 per 100,000 person-years.367 The average age of onset of PSP is ~68 years, and the survival time after diagnosis is ~2.9 years.368 Neuropathologically, PSP is defined by the accumulation of pTau in both neurons and glial cells.369 Pathologically pTau leads to depolymerization of microtubules, neuronal damage, microgliosis, and astrogliosis, ultimately leading to irreversible neurodegeneration.370 There have been over 30 drugs that target tau aggregation, processing, and accumulation reaching the clinic over the past 15 years, but the results were disappointing.370 Recently, GWAS showed that most AD risk genes were highly or exclusively expressed in microglia in the brain such as TREM2 and MS4A4A.124 Notably, the expression level of TREM2 and MS4A4A gene were also upregulated in the substantia nigra of PSP patients versus controls. A positive correlation was found between TREM2 mRNA levels and hyperphosphorylated tau burden in the substantia nigra, specifically in neurons.371 The above evidence suggests that microglia participate in the disease process of PSP. Moreover, these findings suggest that tauopathies may share similar immune regulation mechanisms.
Microglial activation in PSP brains
Several studies have identified increased microglia number and activation in the substantia nigra pars compacta (SNpc),372 subthalamic nucleus,373 pyramidal, extrapyramidal motor system, and cerebellar output374 of brain tissues from PSP patients by immunochemical postmortem analysis. And in most of these regions, microglial activation was positively correlated with tau burden.374 Microglial activation in PSP brains was also detected by PET imaging. PSP patients showed significantly increased mean [11C](R)-PK11195 binding in the midbrain, basal ganglia, frontal lobe, cerebellum,375 thalamus, putamen, and globus pallidus376 compared to controls. Using another TSPO tracer 18F-GE-180, elevated TSPO uptake was also observed in subcortical brain regions, especially in the medial pallidus in PSP.377 Importantly, by using [11C]PK11195 and [18F]AV-1451 to measure microglial activation and tau pathology, respectively, studies found that microglial activation in cortical and subcortical regions was positively correlated with tau pathology.378 Additionally, subcortical tau pathology and microglial activation positively correlated with clinical severity376,378,379 and could predict disease progression in PSP.379 Taken together, the above pathological and neuroimaging evidence consistently showed that microglial activation was closely related to tau pathology and neurodegeneration, suggesting that microglia is likely to play a crucial role in the pathogenesis of PSP.
Tau serves as a main trigger of microglial activation
It has been hypothesized that tauopathy is the primary cause of microglial activation. Firstly, microglial activation colocalized and correlated with tau pathology in PSP patients374,378 and transgenic mice expressing mutant tau P301L.380 Secondly, to clarify the temporal sequence of microglial activation and tauopathy, a study used Thy1-hTau.P301S mice that expressed human tau with a P301S mutation, specifically in neurons. From 2 months onward, there was significant cortical pTau deposition, and several changes were observed in microglia following pTau accumulation, including morphological changes, an increase in microglial lysosomal volume, and a significant loss of homeostatic marker Tmem119.381 Thirdly, when applied in vitro, overexpression of full-length tau in cultured rat microglia caused their activation.382 Alternatively, tau oligomers and fibrils added into the culture of primary microglia directly caused microglial activation and secretion of pro-inflammatory cytokines.383 Together, these findings indicate that microglia adopt a pTau-induced phenotype. In vitro study also revealed that MAPK pathway mediated tau-induced microglial activation.384,385
Microglial roles in PSP pathogenesisPhagocytosis
Microglia could phagocytize different tau species,386,387 and this process was partly dependent on microglial fractalkine receptor (CX3CR1) receptor.388 The deficiency of the CX3CR1 enhanced tau phosphorylation and aggregation and memory impairment in a transgenic mouse model of tauopathy in which the WT human MAPT gene replaced the endogenous mouse Mapt gene (hTau mice).389 Furthermore, microglia could also phagocytize synapses that contain aggregated tau via synaptic tagging of C1q, leading to a decline in synapse density.390 A C1q-blocking antibody could inhibit microglial synapse removal and rescue synapse density in cultured neurons and Tau-P301S mice. Notably, microglia can even phagocytize live neurons containing tau inclusions in addition to free extracellular tau.391 Mechanically, microglia are activated when live neurons with tau aggregation expose phosphatidylserines as a “eat-me” signal. This is followed by opsonin milk-fat-globule EGF-factor-8 (MFGE8) and nitric oxide released from the microglia, resulting in the engulfment of the live neuron by the microglia.391 Together, microglia could phagocytize free extracellular tau, synapses of neurons containing pTau, and even live neurons containing Tau inclusion. It is currently unclear, however, if this process is detrimental or beneficial. Despite clearing tau aggregation, microglia also lead to the loss of synapses and stressed-but-viable neurons, which disrupt neuronal networks and may lead to cognitive impairments.392
Neuroinflammation
In parallel with the detection of microglial activation in the brains of PSP patients, upregulation of the expression levels of pro-inflammatory factors was also detected in the substantia nigra, such as IL- 1β.373 Microglial activation led to the release of pro-inflammatory factors and induced neuroinflammation, further accelerating the accumulation of hyperphosphorylated tau.393,394 Importantly, immunosuppression with FK506 significantly decreased tau pathology and increased lifespan in young P301S Tg mice, thereby demonstrating that microglial activation and neuroinflammation promoted the early progression of tauopathies.395 The further study discovered that Cx3cl1 expressed by neurons interacted with the microglial receptor Cx3cr1 and restricted microglia-mediated neuroinflammation. Genetic ablation of Cx3cl1396,397 or Cx3cr1389,398 in mouse models of tauopathy enhanced tau hyperphosphorylation, tau pathology, neuroinflammation, and cognitive deficits389,396,397,398 via IL-1/p38 MAPK pathway.389,397 Notably, merely transplanting purified microglia derived from hTauCx3cr1-/- mice into the brains of non-transgenic recipient mice could induce tau hyperphosphorylation within the recipient brain. But transplantation of inclusion of IL-1 receptor antagonist together into the recipient brain, microglia-induced tau pathology significantly reduced.398 The above evidence suggests that reactive microglia, released pro-inflammatory cytokines, and microglia-mediated neuroinflammation are sufficient to drive tau pathology. This also suggests that inhibition of microglial activation and related neuroinflammation could delay the progression of PSP and other tauopathies.
Besides, after microglial uptake and lysosomal sorting of tau fibrillization, aggregated tau-activated NLRP3-ASC-dependent inflammasomes. ASC deficiency in tau transgenic mice significantly inhibited exogenously seeded and non-exogenously seeded tau pathology. Alternatively, exogenously seededtau pathology was inhibited by chronic intracerebral administration of the NLRP3 inhibitor. These findings indicate that aggregated tau activates the ASC inflammasome via the NLRP3-ASC axis, which exacerbates exogenously seeded and non-exogenously seeded tau pathology in vivo.399 The mechanism of action of inflammasomes may be partly because inflammasome activation produces pro-inflammatory cytokines IL-1β and IL-18,298 which have been shown to increase the tau hyperphosphorylation and accumulation.400,401 The findings highlight that the NLRP3 inflammasome may be a therapeutic target in PSP and other tauopathies.
Tau propagation
Tau propagation was likely mediated through synaptic connections.402 As a result of injecting mice with adeno-associated virus (AAV) expressing human mutated tau under neuron-specific synapsin-1 promoters into their entorhinal cortex, it was observed that tau spread from the entorhinal cortex to the dentate gyrus 4 weeks after injection.402 Microglia may be critical in spreading tau protein since depleting microglia dramatically suppressed tau propagation in this mouse model.402 Moreover, microglia are pivotal in spreading tau by releasing tau-containing exosomes.402,403 Suppressing exosome synthesis and secretion from microglia may halt exosome-mediated tau propagation. Overall, microglia and their secreted exosomes contribute to tauopathy progression and the inhibition of exosome synthesis or secretion could be a therapeutic target.
Senescent glial cells
Cell senescence is involved in the occurrence or progression of neurodegenerative diseases.404 In Tau-P301S mice, senescent microglial cells and astrocytes were observed at six months of age. To investigate the role of senescent cells in the development of disease, two methods were used to clear senescent cells: first, by genetically engineering mice so that their senescent cells died after being fed a specific chemical, and second, by using senolytic, genetic approach decreased tau pathology and gliosis, prevented neuronal degeneration and thus improved cognitive function, while pharmacological intervention can also attenuate tau phosphorylation. These results show that senescent glial cells directly contribute to neuronal tau pathology and cognitive impairment. This finding also suggests that senescent glial cells may provide a therapeutic target.405
T cell involvement
T cell infiltration was observed in the cortex of patients with FTD with a P301L tau mutation and the hippocampus of THY-Tau22 tau transgenic mice. T cells were chronically depleted using specific antibodies to gain insight into the functional role of T cell infiltration in tauopathy pathogenesis. Prevention of hippocampal T cell infiltration in tau transgenic mice rescued spatial memory deficits, despite without modulation of tau pathology,406 suggesting that T cell infiltration is involved in the pathological mechanism of tauopathies, although the exact mechanism remains unclear.
Corticalbasal degeneration
Corticobasal Degeneration (CBD) is a rare, progressive neurodegenerative disease. In most cases, the disease begins between ages 60 and 70. CBD is manifested with parkinsonism, myoclonus, sensation loss on one side or difficulty identifying things by touch, alien limb, speech and language difficulties, and behavioral changes. As CBD symptoms overlap with other more common neurological diseases, corticobasal syndrome is more commonly used by neurologists than CBD.
Similar to PSP, increased microglial activation was also found in CBD brains compared with controls, and that microglial activation in most regions correlated with tau burden.374 Although both PSP and CBD brains showed microglial activation, a distinctive pattern of microglial activation and tau pathology was found in CBD and PSP, with CBD showing more pathology in supratentorial structures. In comparison, PSP showed more pathology in infratentorial structures.374 Another difference was that only CBD patients demonstrated increased TSPO uptake in additional motor and supplementary motor areas377 even though significantly increased mean [11C](R)PK11195 binding was observed in subcortical brain regions,377,407 especially in the medial pallidus377 in both CBD and PSP patients. Besides, the activation of microglia also showed asymmetry in CBD. For example, according to fluorodeoxyglucose (FDG) and [11C]PK 11195 PET imaging, a CBD patient with left-sided symptoms showed a marked right hemispheric hypometabolism as well as asymmetric microglial activation in corresponding areas of the right temporal and parietal cortex and basal ganglia.408 Although both CBD and PSP belong to tauopathies, the exact pathogenesis remains unclear as to why the regions of pathological tau deposition are different and microglial roles in different tauopathies are also unknown.
Dementia with lewy bodies
Dementia with Lewy bodies (DLB) is the second most common type of degenerative dementia following AD. DLB accounted for 3.2–7.1% of all dementia cases in the incidence studies.409 Clinical characteristics of DLB include cognitive fluctuations, parkinsonism-like motor symptoms, recurrent visual hallucinations, and rapid eye movement sleep behavior disorder (RBD).410 The defining pathological features of DLB are the presence of intracellular α-syn aggregates termed Lewy bodies.411 However, many DLB cases also exhibit Alzheimer-type pathology in the form of Aβ plaques and tangles of hyper-phosphorylated tau.412,413 This AD-type pathology in DLB was associated with global and regional atrophy rates.414,415
Microglial activation and neuroinflammation in DLB postmortem brains
Several studies have used immunostaining to detect microglial activation in the postmortem brain tissue of DLB patients, and the vast majority of these studies found that DLB patients and non-demented controls had similar microglial activation and neuroinflammation levels,416,417,418,419,420 except two studies that examined only 5 cases of DLB each.421,422 Among these studies, Amin et al.’s study was based on the largest postmortem cohort consisting of 30 postmortem confirmed DLB cases and 29 matched controls, which performed immunohistochemistry in the cerebral cortex to observe microglial phenotype with several markers including Iba1, HLA-DR, and CD68. Even though immunostaining showed increased neuropathology in DLB, there was no significant difference between groups in microglial activation.420 Also, transcriptomic and protein expression analyses of postmortem brain tissue in DLB did not reveal significant microglial activation.419,423 Although these studies of human postmortem brain tissue did not demonstrate microglial activation in DLB patients, they consistently showed increased cortical recruitment of T lymphocytes in DLB,420,424 suggesting that adaptive immunity may be involved in the pathogenesis of DLB.
Early microglial activation detected by in vivo PET imaging
In vivo brain imaging allows the investigation of inflammatory processes in the early stages of the disease and facilitates longitudinal monitoring of microglial activation during disease progression. Two studies found increased microglial activation in the early stage of DLB. One study included 6 DLB patients within a year from the onset (MMSE 24 ± 3.9) and found a significant increase in [11C]PK11195 binding in nearly all subcortical and cortical brain regions in DLB patients compared with 11 controls.425 To further clarify whether microglial activation is associated with severity of cognitive impairment, a larger study of 19 DLB cases (MMSE 21.9 ± 4.5) was divided into two subgroups by Addenbrooke’s Cognitive Examination Revised (ACE-R)score: nine ‘mild’ cases (ACE-R score>65) and 10 ‘moderate/severe’ cases (ACE-R score≤65), indicating their level of cognitive impairment at the time of their 11C-PK11195 PET scan. The mild DLB group showed increased 11C-PK11195 binding in the inferior and medial temporal gyri, putamen, cuneus, fusiform gyrus, and inferior frontal gyrus compared with controls.426 On the contrary, the moderate/severe DLB group demonstrated generally decreased binding compared with controls.426 This study suggests that microglial activation occurs in the early stages of the disease and that as the disease progresses, the microglia phenotype changes. This is consistent with another study using [3H]PK11195 and [3H]PBR28 PET to observe microglial activation and found that TSPO density in the SN of 5 late-stage DLB brains was significantly reduced compared to 8 controls. The authors of this study proposed that this distinctive pattern of TSPO density change in late stage DLB cases may indicate microglia dystrophy.427 This is similar to the results of a previous study, which observed the microglia morphology by immunohistochemistry and found that in the late stage of DLB, there was low microglia density and microglia showed dystrophic phenotype.418
Overall, whether using postmortem brain tissue immunostaining which reflects the advanced stage of the disease, or in vivo PET imaging of late-stage DLB or those DLB patients with more severe cognitive impairment, it is consistently found that in the late stage of DLB, microglia are not in an activated state, but instead appear to be dystrophic. In contrast, in the early stage, reactive microglia in an activated state were remarkable. This indicates that microglia show different phenotypes in different stages of DLB. To date, the following questions remain unclear, for example, whether early microglial activation in disease is protective or deleterious. Why does microglial activation diminish in the late stages of the disease? Cortical atrophy, neuropil degeneration, and microglial activation are less prominent in advanced DLB than in AD.420,428 Is this related to the fact that AD-like pathology (such as Aβ and tau deposition) in DLB is less significant than in AD? Are differences in the severity of neurodegeneration between AD and DLB related to differences in the degree of microglial activation? In the future, it is essential to conduct more longitudinal studies to observe the dynamic changes in microglial activation during disease progression. If possible, monitoring tau or Aβ or α-syn deposition alongside microglial activation may help elucidate the correlation of microglial activation in DLB with other neuropathology.
Huntington’s disease
Huntington’s disease (HD) is an inherited neurodegenerative disease that manifests with involuntary choreatic movements and cognitive and behavioral disturbances. HD is a monogenic autosomal dominant disorder caused by the expansion of CAG trinucleotide repeats in the HTT gene. The mutation leads to an abnormally long polyglutamine (polyQ) expansion in the huntingtin (HTT) protein, which confers the protein propensity to misfold.429 The length of the CAG repeat is critical for developing HD. Repeats up to 35 in length do not cause HD. People with 36–39 CAG repeats may or may not develop symptoms of HD. CAG repetition lengths over 40 are linked to a definite HD onset during a typical lifespan.430 Correlative studies have revealed an inverse relationship between the age of onset and CAG repeat length.431 The incidence of HD in the Western population is 4–10 per 100,000 people, and the average age of onset is 40 years.432 Pathogenic mutant huntingtin (mHTT) is expressed in various types of neurons in the brain.433 It causes selective loss of medium spiny neurons (MSNs) in the striatum, as well as caudate and putamen atrophy.434 R6/2 and N171-Q82 mouse models expressing truncated N-terminal segments of HTT are commonly used in research. R6/1 and R6/2 mice express exon 1 of the human HTT gene with approximately 116 CAG repeats and 144–150 CAG repeats, respectively, under the control of the human HTT promoter. Mice expressing truncated HTT (R6/2 and N171–82Q) demonstrate more severe behavioral and neurological abnormalities than transgenic mice that express full-length mutant HTT.435
Microglial activation in Huntington’s disease
Aggregated mHTT is typically observed as inclusion bodies in the cytoplasm or nucleus,436 and N-terminal htt fragments are widely believed to play a role in HD pathogenesis, with smaller N-terminal htt fragments showing greater neurotoxicity than large-sized fragments.437 Postmortem examination shows 95 percent of HD patients’ brains had bilateral striatal atrophy.438 Indeed, it has been demonstrated that neuron cell death in the cerebral cortex is diverse, explaining the various symptom profiles observed in HD.439,440 Reactive gliosis is routinely found in the striatum of HD patients, together with reactive fibrillary astrocytosis and reactive microglia.441 In vivo PET investigations have demonstrated significant microglial activation in affected areas of the HD brain, and this pathological phenomenon is more pronounced in severe cases of HD.442 11C(R)-PK11195 PET detected microglial activation in HD patients even before the onset of clinical symptoms.443 Expression of mHTT in neurons leads to microglial activation in cortico-striatal brain slice and primary neuronal culture models. These reactive microglia tend to cluster along aberrant neurites but do not directly contribute to neuronal degeneration.444 Using genome-wide approaches, one study revealed that microglia expressing mHTT exhibited an intrinsic pro-inflammatory gene expression profile even without pro-inflammatory stimuli. Moreover, ex vivo and in vivo studies showed that mHTT-expressing microglia are more toxic to neurons than WT microglia after pro-inflammatory stimuli.445
Major signaling pathways underlying the microglial activation
Several signaling pathways have been implicated in microglial activation in HD, including the NF-kB pathway, kynurenine pathway, and cannabinoid receptor pathway. By expressing TLRs, microglia can detect and respond to a wide range of external stimuli, including infections, tissue damage, and other sources of inflammation. Upon activation, TLRs trigger a series of signaling pathways that lead to the activation of immune responses. TLRs signaling can activate the downstream NF-kB signaling cascade by the intracellular adaptor protein MyD88, leading to an increase in the production of pro-inflammatory cytokines. It has been shown that soluble mHTT activate IκB Kinase (IKK), triggering the NF-kB signaling pathway,446 and leads to the increase in the gene expression of pro-inflammatory cytokines.447,448 Furthermore, the reduction of mHTT levels with siRNA improved NF-kB transcriptional dysregulation and reduced pro-inflammatory cytokine production in HD.449
Kynurenine pathway metabolic balance influences the function of microglia in HD. Kynurenine 3-monooxygenase (KMO) enzyme, which is predominantly expressed in microglia, catalyzes the conversion of L-kynurenine to 3-hydroxykynurenine (3-HK) in the kynurenine pathway.450 R6/2 HD mice treated with the KMO inhibitor JM6 showed a decrease in synaptic degeneration and a longer lifespan by reducing microglial activation.451
Altered activation of the cannabinoid system contributes to the development of HD. Genetic deletion of CB2 receptors in the R6/2 mouse model increased behavioral impairments, shortened life duration, and accelerated microglial activation.452 Furthermore, stimulation of CB1 and/or CB2 receptors in microglia was demonstrated to induce M2 polarization, while knocking out CB2 receptors in mice inhibited M2 polarization.453 As a result, pharmacological techniques targeting CB2 receptors in microglia may be beneficial in the treatment of HD.
Abnormal microglia in HD
Previous studies showed that the number and morphology of microglia changed with age in both WT and R6/2 mice, with more pronounced changes observed in the transgenic mice. Structural abnormalities in microglia were observed as early as 7 weeks in R6/2 brains.454 The findings suggest that changes in the dynamic states of microglia may contribute to an impairment of their neuro-supportive functions in HD. It is reported that increased immunostaining for ferritin in the striatum, cortex, and hippocampus in brains of R6/2 mice and HD patients. Ferritin-labeled microglia in R6/2 mice exhibited dystrophic, and some of these cells contained mHTT. Similarly, brains from HD patients displayed elevated numbers of ferritin-containing microglia that exhibited positive staining with Perl’s stain, indicating abnormally high iron levels.455 These findings provide new insights into the mechanisms underlying HD pathogenesis. Microglial elimination in R6/2 mice prevented the loss of PNNs and dramatically increased PNNs in the brains of naïve littermates. These findings suggest that microglia may play a new role in regulating the integrity and formation of PNNs.456
Preclinical and clinical evidence target on microglia in neurodegenerative diseases treatment
Alzheimer’s diseaseRegulation of neuroinflammation enhances phagocytosis of Aβ by microglia
AD patients and mouse models have elevated levels of inflammatory markers, and several AD risk genes associated with innate immune function have been identified, suggesting that neuroinflammation plays a critical role in AD pathogenesis.457 In AD, microglia exhibit a pro-inflammatory phenotype that impairs the phagocytic activity of microglia, promotes cerebral pathology, and exacerbates behavior defects. Therefore, some studies have improved AD by reducing microglia-mediated neuroinflammation. Min Hee Park et al. found N, N′-Diacetyl- p-phenylenediamine suppressed neuroinflammation, enhanced microglia phagocytosis, reduced Aβ burden, and improved cognitive function in AD transgenic mouse models by suppressing the expression of NLRP3 inflammasome-associated proteins.458 Inhibiting the NLRP3 inflammasome using NLRP3-specific inhibitor dapansutrile (OLT1177) could rescue cognitive impairment in a mouse model of AD.459 Besides, desloratadine, a selective antagonist of the 5HT2A receptor, and DW14006, a direct AMPKα1 activator, were applied in AD mouse models and found that they ameliorated innate immune response, enhanced microglial Aβ phagocytosis, reduced amyloid plaque deposition by polarizing microglia to an anti-inflammatory phenotype via selectively antagonizing the 5HT2A receptor and activating AMPKα1/PPARγ/CD36 signaling respectively.460,461 In addition, Chunmei Liang et al. found microRNA-146a lessened neuroinflammation and Aβ burden, prevented neuronal loss, and reduced cognitive deficits in APP/PS1 transgenic mice by switching microglial phenotype, decreasing pro-inflammatory cytokines, and enhancing phagocytosis.462 The above evidence suggests that modulating microglia-mediated neuroinflammation is a key therapeutic target in treating AD.
TREM2 activation modulates microglial phenotype and enhances Aβ phagocytosis
Emerging evidence has shown that TREM2 activation increased Aβ phagocytosis, relieved neuroinflammation, and improved cognitive behavior in AD mouse models. Thus, several approaches have been developed to enhance TREM2 signaling by TREM2 agonist antibody, direct delivery of the TREM2 gene, or stimulating other pathways to increase TREM2 expression. Currently available TREM2 antibodies are as follows: (1) 4D9, with a stalk region epitope close to TREM2 cleavage site, reducing TREM2 shedding, concomitantly activating TREM2 downstream phospho-SYK signaling171; (2) AL002c, agonist antibody that activate TREM2 signaling,172 and phase I clinical trials have demonstrated that a variant of AL002c is safe and well tolerate, and a phase 2 study to evaluate efficacy and safety of AL002 in participants with early AD are in progress (NCT04592874); (3) bispecific antibody, targeting TREM2 as a tetravalent TREM2 agonistic antibody that increases TREM2 activity by 100-fold, meanwhile targeting transferrin receptor, improved antibody brain entry by more than 10-fold.173 These antibodies have been evaluated in AD mouse models and found that they reduced Aβ and tau pathology, tempered microglial inflammatory response, and improved cognitive behaviors.171,172,173 In addition, Pengzhen Wang et al. developed microglia-targeted gene delivery systems-coated TREM2 plasmid to upregulate the TREM2 level in the brain, significantly regulated microglial polarization toward an anti-inflammatory phenotype, relieved neuroinflammation, enhanced Aβ clearance, and improved cognitive performance in APP/PS1 mice.463 Qiming Xu et al. utilized cGAMP to activate the cGAMP-STING-IRF3 pathway, leading to TREM2 upregulation, which decreased Aβ burden, neuron loss, and improved cognitive impairment in AD mice.464 Taken together, the above evidence suggests that activation of TREM2 in microglia is beneficial in treating AD.
Inhibition of microglial exosome synthesis and secretion reduces pathological Tau spreading
Microglia release tau-containing exosomes that contribute to the spread of tau.402,403 Thus, it may be possible to halt tau propagation by suppressing microglial exosome production and secretion. The P2X purinoceptor 7 (P2RX7), an ATP-evoked Na+/Ca2+ channel, is primarily expressed in microglia and triggers exosome release. Pharmacologic blockade of P2RX7 at an early stage in tau mice significantly impaired exosome secretion from microglia, decreased tau accumulation in the brain, and improved working and contextual memory.161 In addition, pharmacologic inhibition of exosome synthesis by targeting neutral sphingomyelinase-2 (nSMase2) could also reduce tau secretion from microglia.402
Altering microglial metabolism to decrease amyloid burden
Microglial phagocytosis requires a great deal of energy, and metabolic dysfunction has been implicated in the pathogenesis of AD.465,466 Stress can cause microglia to metabolic switch from oxidative phosphorylation (OXPHOS) to aerobic glycolysis,467 which may facilitate the immune function of microglia. However, persistent aerobic glycolysis impaired microglial function of Aβ engulfment.468 Some studies have found that regulating the microglial metabolism could enhance the phagocytosis of Aβ by microglia. Rui-Yuan Pan et al. found that sodium rutin (NaR) treatment shifted microglial metabolism from anaerobic glycolysis to mitochondrial OXPHOS, providing microglia with sufficient ATP for Aβ clearance. NaR administration could attenuate synaptic impairment, neuroinflammation, and Aβ burden in brains and rescue learning and memory defects in two mouse models of AD. Moreover, NaR promoted microglial Aβ clearance also by increasing the expression levels of phagocytosis-related receptors in microglia.469 This finding suggests that NaR is a potential therapeutic agent for AD. Rui-Yuan Pan et al. found that H4K12la levels were increased in microglia adjacent to Aβ plaque, facilitating the switch from OXPHOS toward glycolysis in microglia by enhancing glycolytic genes expression comprising PKM2. etc. When Pkm2 was specifically ablationed in microglia, cognitive deficits in AD mice were ameliorated.470 Besides, Baik et al. utilized IFN-γ to boost metabolic pathways through mTOR signaling and found that AD mice exhibited decreased amyloid pathology and improved memory deficits after IFN-γ administration.466 These findings suggest that modulation of microglial bioenergetic pathways and metabolic state might be promising strategies to treat AD.
Altering the microglial phenotype to enable microglia to play a protective role
The brain microenvironment regulates microglia phenotype conversion. For example, when organotypic brain slices from old APP/PS1 mice were co-cultured with young, neonatal WT mice, old microglia cells derived from old mice moved towards the amyloid plaques and cleared the plaque halo. Conditioning media derived from young microglia can also enhance old microglia’s proliferation and phagocytosis of amyloid plaques.471 This evidence suggests that microglia function can be restored through a microenvironment-driven therapeutic approach. Based on this rationale, Yifei Lu et al. developed a ROS-responsive polymeric micelle system. The micelles could accumulate in the diseased regions through an Aβ transportation-mimicked pathway. These micelles normalized oxidative and inflammatory microenvironments and reeducated microglia in early AD. In vivo studies established that this system decreased Aβ plaque burdens and improved cognitive functions.472
In AD brains, many proteins were highly expressed by microglial cells according to proteomics analysis, and some proteins mediated a critical checkpoint in the microglia phenotype transition. For example, RIPK1 was highly expressed by microglial cells in human AD brains, and RIPK1 decreased the microglial phagocytic capacity. Pharmacological or genetic inhibition of RIPK1 reduced neuroinflammation, decreased the cerebral Aβ load, and improved the behavioral deficits by enhancing the microglial degradation of Aβ.473 Similarly, genetic knockdown of REV-ERBs or pharmacological inhibition of REV-ERBs with the small molecule antagonist SR8278 promoted microglia polarization toward a phagocytic phenotype and enhanced microglial engulf of Aβ. Constitutive deletion of Rev-erbalpha altered microglia phenotype and decreased amyloid plaque number and size in an AD mouse model.474
Photobiomodulation has been proposed as a possible therapy for AD by nonthermal exposure of tissue to low-power light at the near-infrared end of the visible spectrum to trigger biological responses in cells and tissues. Li-Huei Tsai et al. found that using noninvasive exposure to 40-Hz light for 1 h transformed microglia into an engulfing state, increased amyloid/microglia colocalization, and reduced Aβ load by 40–50% in an AD mouse model at early pre-plaque stage.475 Similarly, Lechan Tao et al.476 found that treatment with 1070-nm light pulsed at 10 Hz induced the morphological change of microglia, increased the colocalization with Aβ, reduced Aβ burden, and ameliorated cognitive and memory impairment in AD mice. The above studies suggest that controlling microglia fate towards a beneficial phenotype is feasible and worth exploring to treat AD.
Parkinson’s diseaseTarget microglial activation and related neuroinflammation to treat PD
Microglial activation and the resulting inflammatory responses mediated are crucial factors in the development of PD. Understanding the intricacies and imbalances in microglial activation may provide insights into new therapeutic interventions for PD. Naloxone has been shown to safeguard dopaminergic neurons by impeding microglial activation and the production of pro-inflammatory cytokines.477 Similarly, celecoxib protects dopaminergic neurons from degeneration by suppressing microglial activation via inhibiting COX-2 in a rat model of PD.478 The regulation or modification of microglial receptors, such as TLRs and CB2 receptors, presents a promising pharmacological approach for the treatment of PD.479,480 A study in MPTP-induced PD mice found that endurance exercise was neuroprotective through modulating TLR2 and downstream signaling components, such as MyD88, TRAF6, and TAK1.481 The natural agonist of CB2 receptors, β-caryophyllene, and the selective CB2 receptor agonist JWH133 have both demonstrated neuroprotective effects in MPTP-induced PD mice by regulating microglial activation and suppressing expressions of pro-inflammatory cytokines.255,482 JWH133 also protects against BBB disruption and peripheral immune cell infiltration.255 These findings suggest that CB2 receptor agonists may serve as potential therapeutic targets for PD. Additionally, NLRP3 inhibitor MCC950 significantly inhibited inflammasome activation, accumulation of α-synuclein aggregates, and nigrostriatal dopaminergic degeneration, improving motor performance in PD mouse models.223 Several natural compounds, including ginsenoside Rg1,483 piperine,484 curcumin,485 rosmarinic acid,486 and astilbin,487 have been shown to inhibit microglial activation and reduce the production of pro-inflammatory cytokines in mouse models of PD. These compounds offer potential alternative therapeutic options for the treatment of PD.
Target microglial phenotype to treat PD
Vitamin D protects dopaminergic neurons from inflammation and oxidative stress by inhibiting microglial activation and promoting M2 polarization, with increased expression of M2 microglia markers, including CD163, CD204, and CD206.488 PPAR-γ agonists, such as rosiglitazone, have neuroprotective effects on dopaminergic neurons by regulating microglial polarization. Rosiglitazone reduces pro-inflammatory cytokines TNF-α and IL-1β and increases anti-inflammatory cytokines TGF-β and IL-10, induces M2 polarization, and alleviates dopaminergic neuron degeneration of SNc neurons.489
Microglia-targeted therapies in clinical trials for PD
The recruitment for the phase 1 trial of inzomelid, a promising NLRP3 inhibitor, was completed in 2020 (NCT04015076), but results have not yet been disclosed. Myeloperoxidase (MPO) is a key enzyme that produces ROS by phagocytic cells such as microglia and is a mediator of inflammatory processes in many diseases.490 Thus, inhibition of MPO represents an attractive target for reducing neuroinflammation in PD. AZD3241, a selective and irreversible MPO inhibitor, reduced microglial activation assessed by PET imaging in PD patients and was well tolerated.491 Glucagon-like peptide-1 (GLP-1) receptor agonists are commonly used to treat type 2 diabetes. GLP-1R agonist NLY01 directly prevents microglial-mediated astrocyte conversion to an A1 neurotoxic phenotype in the hA53T transgenic mice.113 GLP-1 analogs semaglutide and liraglutide reduced microglial activation, α-syn accumulation, the loss of dopaminergic neurons, and improved motor impairments in the chronic MPTP-induced mouse model of PD.492 Exenatide, one of the most extensively studied GLP-1 receptor agonists, provided both motor and cognitive benefits in PD patients and was well tolerated.493 Notably, the favorable effects lasted 12 months after treatment discontinuation.494
Multiple system atrophyTarget microglial activation and related neuroinflammation to treat MSA
The effect of microglial activation inhibitors has been examined in MSA mouse models and MSA patients. Myeloperoxidase (MPO) is a key enzyme that produces ROS by phagocytic cells such as microglia and is a mediator of inflammatory processes in many diseases.490 MPO expression level in reactive microglia was upregulated in the brains of MSA patients and a mouse model of MSA.495 Thus, inhibition of MPO represents an attractive target for reducing neuroinflammation in MSA. An MPO inhibitor, when applied in the MSA mouse model in the early stage of the disease, suppressed microglial activation and neuroinflammation, reduced intracellular aggregates of α-syn, and rescued neuronal loss and improved motor deficits.495 In the following study, MPO inhibitor therapy was initiated in the advanced stage of the disease after the onset of severe MSA-like neuropathology. It reduced microglial activation and decreased α-syn accumulation in degenerating brain areas. However, these effects failed to improve motor impairments and rescue neuronal loss,496 suggesting that the timing of treatment is important, and that inhibition of microglial activation should be implemented early in the disease. Verdiperstat (MPO inhibitor) has been clinically tested in Phase 1 and Phase 2 trials on approximately 250 healthy volunteers and patients. Results from a Phase 2 trial in MSA patients with the MPO inhibitor treatment for 12 weeks showed improved clinical scores and neuroinflammation reduction measured by PET imaging (NCT02388295). Therefore, a double-blind, randomized,placebo-controlled, phase III study is planned to evaluate the efficacy and safety of Verdiperstat (BHV-3241) treatment for 48 weeks in subjects with MSA, in which UMSARS score is used to assess the efficacy of verdiperstat (NCT03952806).
However, some interventions have failed in clinical trials in patients with MSA despite showing therapeutic effects in mouse models. Minocycline belongs to second‐generation tetracyclines, which can cross the blood‐brain barrier and inhibit microglial activation and pro‐inflammatory cytokines production.497,498,499 When applied in the transgenic MSA mouse model, minocycline suppressed microglial activation and prevented loss of dopaminergic substantia nigra pars compacta neurons and striatal dopaminergic terminals.276 Next, a multicenter, double-blind, randomized, placebo-controlled clinical trial was performed to examine the efficiency of minocycline on 63 patients with clinically probable MSA-P (NCT00146809). However, after a 12-month treatment with minocycline, microglial activation seemed to be decreased, as demonstrated by PET imaging, but symptom severity failed to show clinical benefits, as assessed by clinical motor function assessment.500 Besides, Fluoxetine, a selective serotonin reuptake inhibitor, significantly reduces LPS-induced pro-inflammatory cytokines production and oxidative stress in microglia and enhances microglia phagocytosis and autophagy.501 Fluoxetine ameliorated motor deficits and decreased neurodegenerative pathology in MSA mice.502 However, a phase II double-blind, placebo-controlled study on MSA patients found no difference in progression rates (NCT01146548).503
Amyotrophic lateral sclerosis and frontotemporal dementiaTargeting microglial neuroinflammation to treat ALS
Targeting microglial neuroinflammation has therapeutic effects in ALS mouse models. For example, the organoselenium compound diphenyl diselenide (DPDS) improved motor deficit, prolonged survival, and reduced motor neuronal loss in hSOD1G93A transgenic mouse through suppressing microglia activation by inhibiting NLRP3 inflammasome activation and IΚb/NF-κB pathway.504 Another study also demonstrated that inhibition of NF-κB activation by daily oral administration of A Nitroalkene Benzoic Acid Derivative (BANA) could reduce reactive microglia and prolong survival in SOD1G93A rats.505 In addition, LPS-treated mSOD1G93A microglia caused microglial activation and released nitric oxide, which induced co-cultured motor neuron injury. Pretreatment with L-NIL, an inhibitor of iNOS, increased co-cultured motor neuron survival.506 These studies indicate that inhibiting microglial activation and related iNOS production could treat ALS.
Additionally, pathological proteins of ALS can be secreted into the extracellular matrix, and these pathological proteins are sensed by microglia, causing microglial activation and pro-inflammatory effect that are harmful to co-cultured motor neurons. For example, in primary mouse microglia, SOD1G93A protein caused NLRP3 inflammasome activation and a significant increase in the release of pro-inflammatory factors such as TNF, IL-1β, superoxide, and iNOS.507 Nlrp3 knockout or pretreatment with a specific NLRP3 inhibitor blocked SOD1G93A protein’s ability to induce IL-1β secretion from microglia, indicating some specific pro-inflammatory factors production was NLRP3 dependent.508 Therefore, NLRP3 inhibition may also be used as a therapeutic strategy to prevent the progression of ALS by halting microglial neuroinflammation. These findings indicate that targeting reactive microglia and related neuroinflammation holds promise as therapeutic strategies for ALS.
Targeting progranulin insufficiency-caused microglial dysfunction may treat FTD-GRN
Heterozygous GRN mutations cause progranulin haploinsufficiency, resulting in patients with FTD (FTD-GRN). GRN encodes a secreted protein (progranulin) expressed in microglia and neurons in human brains. In the CNS, microglia express the highest progranulin levels and show higher expression in reactive states when responding to aging,360 or disease pathology.509 Progranulin reduction in microglia alone is sufficient to recapitulate inflammation, and lysosomal dysfunction, both of which are important pathogenic drivers in FTD-GRN.510 Therefore, it may be possible to treat or prevent FTD-GRN by targeting the dysfunction of microglia caused by insufficient progranulin. Telpoukhovskaia et al. screened a library of bioactive compounds using RNA-mediated oligonucleotide annealing, selection, and ligation with next-generation sequencing (RASL-seq) technique. They identified two compounds nor‑binaltorphimine dihydrochloride (nor‑BNI) and dibutyryl-cAMP, sodium salt (DB‑cAMP) that can reverse microglial defects in Grn‑deficient mice. Experimental evidence revealed that in progranulin‑deficient primary mouse microglia, these two compounds promoted microglial transcriptional profiles transition from the Grn KO signature toward the Grn WT state and could also partially rescue lysosomal dysfunction. As patients with FTD exhibited lysosomal dysfunction and neuroinflammation, and microglial signature is closely related to the regulation of neuroinflammation, thus this study proposed two compounds that may be beneficial for FTD therapy, meanwhile also highlighting the potential of a transcription‑based platform for drug screening.510
Progressive supranuclear palsyInhibition of microglia activation as a therapeutic target to treat PSP
5-lipoxygenase (5-LO), broadly expressed in the CNS, is a potent pro-inflammatory mediator regulating microglial activation.511 5-LO levels were significantly higher in the frontal cortex of the brains of PSP patients than in controls.512 By employing an AAV vector system to over-express 5-LO in the brain of the same transgenic model of human tauopathy, 5-LO increased tau phosphorylation and glial activation and enhanced behavioral impairments.513,514 In contrast, genetic deletion of 5-LO in P301S tau mice515 or pharmacologic inhibition of 5-LO with zileuton,512,516,517 both resulted in significant reduction of tau phosphorylation and glial cell activation and thus ameliorated cognitive deficits. It is worth mentioning that administration of 5-LO blocker at both early (age of 3 months)516 and late (age of 12 months)517 stages showed a beneficial effect in the transgenic tau mice, which suggests that the inhibition of 5-LO has a protective effect throughout the disease course. Collectively, the above evidence provides a rationale that 5-LO is a viable therapeutic target for treating and even preventing human tauopathy.
Benfotiamine (BFT) is a synthetic vitamin B1 (thiamine) derivative that reduces inflammation in LPS-stimulated BV-2 microglia.518 One previous study found that BFT reduced phosphorylated tau levels, ameliorated Aβ load, and improved cognitive function in an AD mouse model APP/PS1 mice.519 Another study treated P301S tau transgenic mice with chronically BMT dietary from the age of 1 to 10 months and found that BFT significantly decreased the expression of inflammatory mediators, including COX-2, TNF-α, IL-1β, NF-κB p65, and iNOS, attenuated oxidative damage, as well as ameliorated mitochondrial dysfunction and motor neuron loss, resulting in behavior improvement and lifespan increased.520 These findings demonstrate that BFT is a promising therapeutic agent for treating tau pathologies such as AD, PSP, and FTD.
Huntington’s diseaseInhibition of microglial activation as a therapeutic target to treat HD
There is no disease-modifying therapy for HD, so current treatment focuses on chorea and mental symptoms. Several medicines, including immunomodulators, and cytokine-neutralizing antibodies, have been explored in various research in the hunt for successful therapy. The expression of the CB2 cannabinoid receptor was increased in striatal microglia of HD patients and transgenic mouse models. Genetic ablation of CB2 receptors in R6/2 mice enhanced microglial activation, aggravated disease symptoms, and reduced lifespan. In contrast, activation of CB2 receptors with selective agonists reduced neuroinflammation, striatal neuronal loss, and motor symptoms in WT mice subjected to excitotoxicity.452 The selective CB2 receptor agonist, SR144528, could protect the striatum against mitochondrial toxin malonate toxicity via their effects on glial cells, especially reactive microglia.521 The above evidence suggests that CB2 receptors could be a potential therapeutic target for slowing neurodegeneration in HD. Galectin-3 (Gal3) is a lectin that was upregulated in the plasma and brain of patients and mice with HD, and their plasma Gal3 levels correlated with disease severity. Its upregulation in microglia occurred prior to the onset of motor impairment and contributed to inflammation through NF-κB- and NLRP3 inflammasome-dependent pathways. Knockdown of Gal3 suppressed neuroinflammation, reduced the aggregation of mHTT, alleviated motor dysfunction, and increased survival in HD mice.522 These findings suggest that Gal3 could be a novel target for therapeutic intervention in HD. Poly (ADP-ribose) polymerase-1 (PARP-1) is an enzyme involved in both DNA repair and transcriptional regulation. Inhibiting PARP-1 suppresses microglial activation likely via regulating NF-kB-dependent gene transcription.523 In a traumatic brain injury mouse model, administration of a PARP inhibitor for 12 days reduced inflammation, increased neuronal survival, and improved performance.524 Olaparib, a PARP-1 inhibitor commercially available as an anti-neoplastic drug, was found to have a neuroprotective effect in the R6/2 mouse model of HD. Administering Olaparib from the pre-symptomatic stage increased survival and improved clinical outcomes mainly by modulating the inflammasome activation.525 These results suggest that Olaparib could be a potentially useful therapy for HD. The researchers also discovered a compound (MIND4–17) that can selectively activate nuclear factor-erythroid 2 p45-derived factor 2 (NRF2) signaling by modifying a critical stress-sensor cysteine (C151) of an E3 ligase substrate adaptor protein Kelch-like ECH-associated protein 1 (KEAP1). Interestingly, the genetic correction of the disease-causing mutation restored a muted NRF2 activation response in HD neural stem cells. Conversely, selective activation of NRF2 signaling decreased the release of pro-inflammatory cytokines in primary microglia from HD mice.526 Semaphorin 4D (SEMA4D) is a transmembrane signaling molecule that modulates various processes central to neuroinflammation and neurodegeneration. Blocking SEMA4D significantly inhibits microglial activation and neuroinflammation in experimental autoimmune encephalomyelitis.527 In the YAC128 transgenic HD mouse model, treatment with an anti-SEMA4D monoclonal antibody reduced brain atrophy, improved cognition, and reduced anxiety-like behavior.528 These findings suggest that targeting microglia could be a promising direction in exploring treatments for HD.
Microglial activation in HD is caused by neuronal mHTT-mediated excitotoxicity or mHTT expression in microglia.529 Several therapeutic approaches are being investigated to reduce the expression of mutant huntingtin RNA (Htt RNA), which could potentially attenuate microglial activation, alleviate inflammatory processes, and provide neuroprotection. Two selective ASOs, WVE-120101 and WVE-120102, which target the most often occurring SNPs in HD patients, have been investigated in human studies (NCT04617847, NCT04617860). However, results showed no significant change in mHTT protein in CSF. The HTT-targeting ASO IONIS-HTTRx (also known as ISIS 443139 and RG6042), which is thought to act through the RNase H1 mechanism, has completed a Phase 1/2a clinical trial (NCT02519036, NCT03342053) and is currently undergoing a large multicenter worldwide efficacy study. This therapy has been deemed safe, with no significant side effects reported in the treatment group. Furthermore, dose-dependent reductions of mHTT concentrations in CSF have been observed, with a 40% decrease in mHTT at the two highest medication dosages,530 which holds promise for disease-modifying treatments for HD. Preclinical evidence in mouse models and clinical trials in patients with neurodegenerative disease has been provided in Table 1. The list of potential microglia-targeted interventions and treatments against neurodegenerative diseases is provided in Fig. 6.
Table 1 Preclinical evidence in mouse models and clinical trials in patients with neurodegenerative disease
Fig. 6
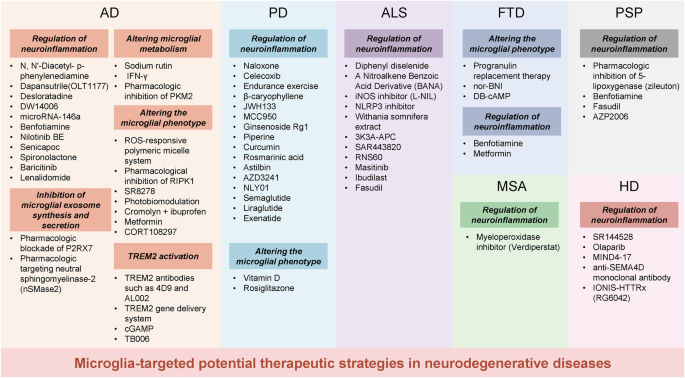
Possible microglia-targeted interventions and treatments against neurodegenerative diseases. Proof-of-principle therapeutic strategies used in cell experiments, animal studies, and clinical trials are shown together. Regulation of neuroinflammation, inhibition of microglial exosome synthesis and secretion, altering microglial metabolism, altering the microglial phenotype, and TREM2 activation are potential therapeutic strategies in treating neurodegenerative diseases. Among these, modulating neuroinflammation is the most widely used therapeutic target
Conclusion
Understanding of microglial roles in neurodegenerative diseases has increased exponentially in recent years. With the development of scRNA-seq and snRNAseq, microglial gene expression signatures are being defined at the single-cell level. It is demonstrated that some identified microglia in specific states correlated with pathological hallmarks and were associated with specific functions. Microglia participate in the progress of neurodegenerative diseases through multiple mechanisms. Dysregulation of microglia may cause impaired phagocytosis of pathological deposits, pathological deposits propagation, neuroinflammation, and microglial phenotype switching, and thus lead to pathology progression and neurodegeneration. Peripheral immune cells infiltration shapes microglia into a pro-inflammatory phenotype and accelerates disease progression. Dysfunctional microglia may also promote the clearance of synapses and perineuronal nets and impair neuronal plasticity and activity. Notably, microglia are a double-edged sword. Microglia can limit the propagation of Aβ and tau by phagocytosis of these proteins, but it can also contribute to neurodegeneration by accelerating their spreading. Future research will focus on precisely regulating microglia and promoting their conversion into a protective phenotype.
Recently, GWAS have demonstrated that most AD risk genes were highly or exclusively in microglia, suggesting that microglia play an important role in the development of AD. Thus, numerous studies have applied microglia-targeted therapeutic strategies in cell experiments, animal studies, and clinical trials in AD and other neurodegenerative diseases. Regulation of neuroinflammation, inhibition of microglial exosome synthesis and secretion, altering microglial metabolism, altering the microglial phenotype, and TREM2 activation are potential therapeutic strategies in treating neurodegenerative diseases. Among these, modulating neuroinflammation is the most widely used therapeutic strategy.
In spite of significant advances in the understanding of microglial functions in neurodegenerative diseases in recent years, microglial heterogeneity and dynamics during the progression of disease still need to be better clarified. The recent advent of high throughput omic data analyses help identify and determine the functional roles of microglia that are in specific states. Additionally, the advancement facilitated the discovery of dysregulated pathways and key molecules critical to pathogenesis, which will contribute to the development of new therapeutic strategies. In the next decade, research on microglia in neurodegenerative diseases should include (i) identify different microglia clusters and understand their functions (ii) identify regulatory factors of specific microglia phenotype and re-educate microglia into a protective state in the early phase of disease progress (iii) reveal microglial crosstalk with other cell types; and (iv) generate chimeric mice using xenotransplantation to recapitulate human microglial biology in vivo; (v) obtain primary microglia from fresh postmortem brain tissues of patients with various neurodegenerative diseases or reprogram human stem cells to develop into microglia-like cells to expand the studies from mouse models to human patients. These steps are essential for any successful effort to develop microglia-targeted therapeutic strategies for treating neurodegenerative disease.
References