beyond reason
우리몸의 대부분은 결합조직으로 구성되어 있다. 결합조직은 섬유아세포(fibroblast)가 만든다.
fibroblast growth factor(FAG)가 FAG수용체와 반응하여 결합조직 재생을 유도한다.
결합조직은 포도당 중합체(GAGs)와 콜라겐, 엘라스틴, 물, 세포 등으로 구성된다.
GAGs 반감기는 1주일, 콜라겐 반감기는 500여일이다.
결합조직이 손상되면 그 회복의 속도는 드라마틱하게 증가한다.
그 과정에 klotho protein이 역할을 한다.
클로토 효소 단백질이 제대로 발현하지 않으면 결합조직의 재생능력이 떨어지기 때문에 신장질환, 혈관의 동맥경화, 암세포증식, 관절강직 등의 문제가 발생한다.
비타민 D는 클로토 효소가 잘 발현되도록 기능을 한다.
아래 논문은 2018년 네이처 리뷰논문이다
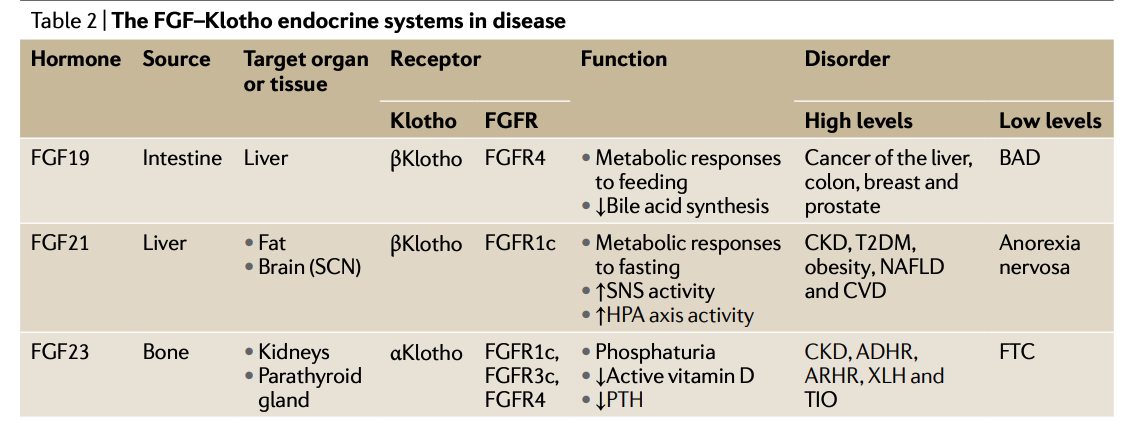
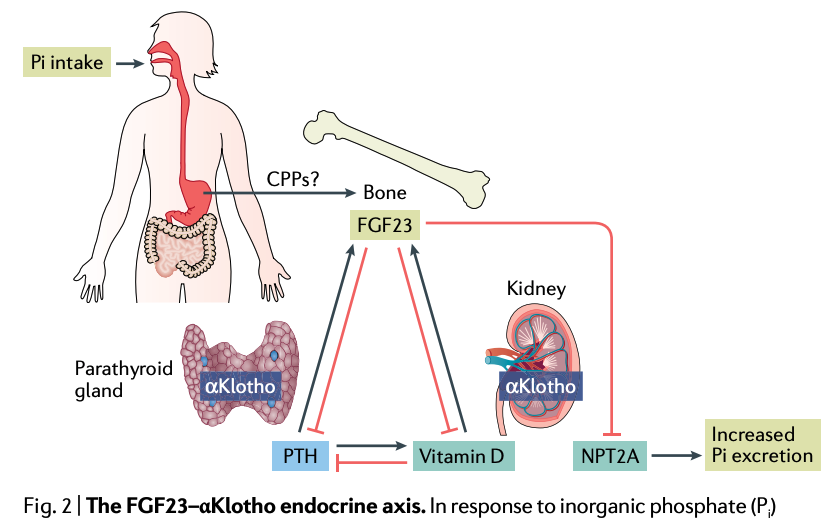
Fig. 2 | The FGF23–αKlotho endocrine axis. In response to inorganic phosphate (Pi ) intake, osteocytes secrete fibroblast growth factor 23 (FGF23). The mechanisms by which osteocytes detect Pi is unclear but might involve sensing of serum calciprotein particles (CPPs), which are nanoparticles that comprise solid-phase calcium phosphate and the serum protein fetuin A. Increased FGF23 levels result in increased urinary phosphate excretion by downregulating sodium-dependent phosphate co-transporter type 2a (NPT2A) levels in proximal tubules and by reducing calcium entry into the circulation (not shown) by lowering the serum level of parathyroid hormone (PTH) and active vitamin D. Increasing urinary phosphate excretion and suppressing calcium entry into the blood in response to phosphate intake enable the FGF23–αKlotho endocrine axis to maintain phosphate homeostasis and potentially prevent the formation of excess CPPs, which can cause tissue damage.
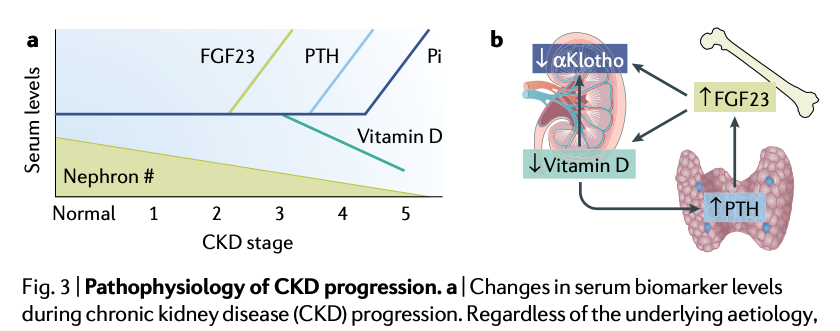
Fig. 3 | Pathophysiology of CKD progression. a | Changes in serum biomarker levels during chronic kidney disease (CKD) progression. Regardless of the underlying aetiology, CKD progression is characterized by a progressive decrease in the number of functional nephrons. To maintain phosphate balance, patients with CKD compensate for the decrease in the nephron number with a rise in fibroblast growth factor 23 (FGF23) levels, which increase phosphate excretion per nephron. The rise in FGF23 is followed by a decrease in active vitamin D and an increase in parathyroid hormone (PTH). All these changes, which are triggered by excess phosphate intake relative to residual nephron number, are characteristic of CKD–mineral and bone disorder. Serum inorganic phosphate (Pi ) levels are the last to increase (resulting in hyperphosphataemia) and indicate a disruption of phosphate homeostasis owing to insufficient functional nephrons to excrete the ingested phosphate. b | The spiral of deterioration in αKlotho expression. The increase in FGF23 levels in patients with renal dysfunction lowers active vitamin D levels, which then elevates PTH levels and further increases FGF23 levels. This positive feedback loop continues to promote an increase in FGF23 levels. Both the increase in FGF23 levels and the decrease in active vitamin D levels can suppress αKlotho expression, potentially resulting in FGF23 resistance and a loss of the renoprotective properties of αKlotho. Part a adapted with permission from ref.202: Kuro-o, M. Klotho and endocrine fibroblast growth factors: marker of chronic kidney disease progression and cardiovascular complications? Nephrol. Dial. Transplant. https://doi.org/10.1093/ndt/gfy126 (2018), by permission of Oxford University Press.
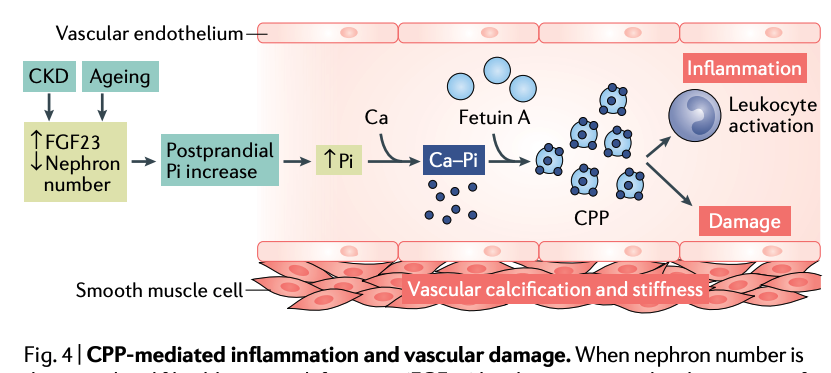
Fig. 4 | CPP-mediated inflammation and vascular damage. When nephron number is decreased and fibroblast growth factor 23 (FGF23) levels are increased in the context of chronic kidney disease (CKD) and ageing, the postprandial increase in serum inorganic phosphate (Pi ) levels is likely to be enhanced and prolonged. This rise in serum Pi can potentially lead to the formation of calciprotein particles (CPPs), which are colloids that comprise deposits of calcium and Pi (Ca–Pi ) adsorbed onto fetuin A. CPPs can induce immune cell activation and trigger an inflammatory response, as well as contribute to arteriosclerosis by inducing vascular damage. In the vasculature, endothelial cell death and dysfunction is accompanied by osteoblastic transformation and calcification of smooth muscle cells. Adapted with permission from ref.202: Kuro-o, M. Klotho and endocrine fibroblast growth factors: marker of chronic kidney disease progression and cardiovascular complications? Nephrol. Dial. Transplant. https://doi.org/10.1093/ndt/ gfy126 (2018), by permission of Oxford University Press.
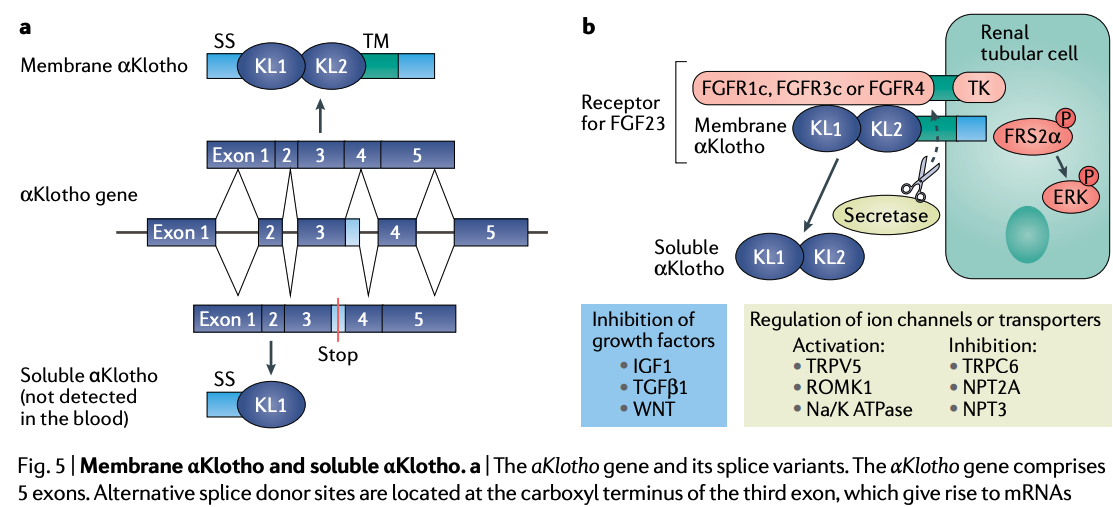
Fig. 5 | Membrane αKlotho and soluble αKlotho. a | The aKlotho gene and its splice variants. The αKlotho gene comprises 5 exons. Alternative splice donor sites are located at the carboxyl terminus of the third exon, which give rise to mRNAs that encode membrane αKlotho and putative secreted αKlotho. The extracellular domain of membrane αKlotho contains two domains, termed KL1 and KL2, which share sequence homology with family 1 glycosidases. The splice variant that encodes the secreted isoform contains a stop codon upstream of exons 4 and 5, which encode the transmembrane and cytoplasmic domains. However, this truncated protein isoform has thus far not been detected in blood. b | Membrane αKlotho functions as the obligate co-receptor for fibroblast growth factor 23 (FGF23) to activate the canonical FGF signalling pathway that is transduced through the tyrosine kinase (TK) domain of FGF receptor (FGFR) and leads to the phosphorylation of FGFR substrate 2α (FRS2α) and ERK1 and ERK2. In addition, membrane-bound αKlotho can also be cleaved by membrane-anchored secretases, which releases the extracellular domain of membrane αKlotho into the extracellular space by ectodomain shedding. This soluble αKlotho protein can regulate several ion channels and transporters and inhibit growth factors, including insulin-like growth factor 1 (IGF1), transforming growth factor β1 (TGFβ1) and WNT. The ion channels and transporters activated by soluble αKlotho include transient receptor potential cation channel subfamily V member 5 (TRPV5), renal outer medullary potassium channel 1 (ROMK1), and Na/K ATPase, whereas short transient receptor potential channel 6 (TRPC6), sodium-dependent phosphate transport protein 2A (NPT2A) and NPT3 are inhibited. SS, signal sequence; TM, transmembrane.
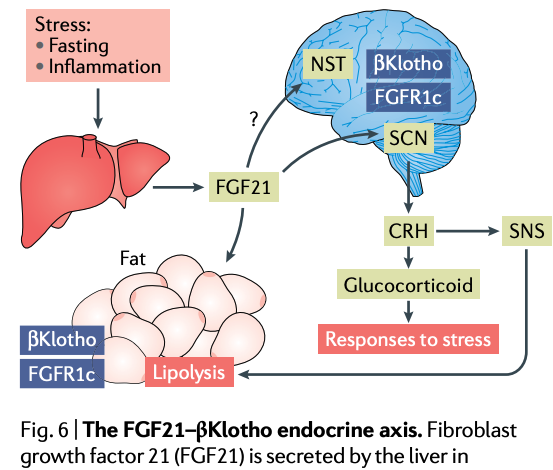
Fig. 6 | The FGF21–βKlotho endocrine axis. Fibroblast growth factor 21 (FGF21) is secreted by the liver in response to various types of stress, including fasting and inflammation. FGF21 acts on white adipose tissue, in which βKlotho and FGF receptor 1c (FGFR1c) are co-expressed, to induce lipolysis. Furthermore, FGF21 crosses the blood– brain barrier and acts on the suprachiasmatic nucleus (SCN) and perhaps on the nucleus of the solitary tract (NTS), in which βKlotho and FGFR1c are also co-expressed. FGF21 induces the expression of corticotropin-releasing hormone (CRH), resulting in an increase in serum glucocorticoid levels. CRH also activates the sympathetic nervous system (SNS) and this contributes to lipolysis. Thus, FGF21 induces responses to stress by activating the hypothalamic–pituitary–adrenal axis and the SNS.
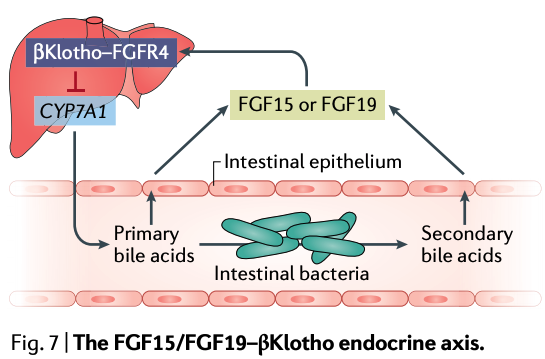
Fig. 7 | The FGF15/FGF19–βKlotho endocrine axis. Fibroblast growth factor 19 (FGF19; FGF15 in rodents) is secreted by intestinal epithelial cells in response to primary bile acids (that is, bile acids that are released from the liver) and secondary bile acids (that is, primary bile acid metabolites that are produced by intestinal bacteria). FGF19 binds to the βKlotho–FGF receptor 4 (FGFR4) complex that is present on hepatocytes to suppress the expression of CYP7A1, which encodes the rate-limiting enzyme of bile acid synthesis, cholesterol 7α-hydroxylase. Thus, the FGF19–βKlotho endocrine axis potentially affects the composition of the microbiome and vice versa.
- Review Article
- Published: 19 November 2018
The Klotho proteins in health and disease
- Makoto Kuro-o
Nature Reviews Nephrology volume 15, pages27–44(2019)Cite this article
- 7357 Accesses
- 78 Citations
- 127 Altmetric
- Metricsdetails
Abstract
The Klotho proteins, αKlotho and βKlotho, are essential components of endocrine fibroblast growth factor (FGF) receptor complexes, as they are required for the high-affinity binding of FGF19, FGF21 and FGF23 to their cognate FGF receptors (FGFRs). Collectively, these proteins form a unique endocrine system that governs multiple metabolic processes in mammals. FGF19 is a satiety hormone that is secreted from the intestine on ingestion of food and binds the βKlotho–FGFR4 complex in hepatocytes to promote metabolic responses to feeding.
By contrast, under fasting conditions, the liver secretes the starvation hormone FGF21, which induces metabolic responses to fasting and stress responses through the activation of the hypothalamus–pituitary–adrenal axis and the sympathetic nervous system following binding to the βKlotho–FGFR1c complex in adipocytes and the suprachiasmatic nucleus, respectively.
Finally, FGF23 is secreted by osteocytes in response to phosphate intake and binds to αKlotho–FGFR complexes, which are expressed most abundantly in renal tubules, to regulate mineral metabolism.
Growing evidence suggests that the FGF–Klotho endocrine system also has a crucial role in the pathophysiology of ageing-related disorders, including diabetes, cancer, arteriosclerosis and chronic kidney disease. Therefore, targeting the FGF–Klotho endocrine axes might have therapeutic benefit in multiple systems; investigation of the crystal structures of FGF–Klotho–FGFR complexes is paving the way for the development of drugs that can regulate these axes.
Key points
- The Klotho proteins αKlotho and βKlotho are essential components of endocrine fibroblast growth factor (FGF) receptor complexes, as they are required for the high-affinity binding of FGF19, FGF21 and FGF23 to their cognate FGF receptors.
- FGF21 is a starvation hormone that induces stress responses by activating the sympathetic nervous system and the hypothalamus–pituitary–adrenal axis.
- FGF19 is a satiety hormone that promotes metabolic responses to feeding.
- FGF23 is a phosphaturic hormone; increased FGF23 levels in patients with early-stage chronic kidney disease or elderly individuals is indicative of excess phosphate intake relative to the residual nephron number.
- Calciprotein particles are colloids of calcium phosphate adsorbed to fetuin A, which increase in concentration as renal function declines and that can induce innate immune responses and cell death, suggesting that they are mediators of phosphate-induced damage.
- Solving the crystal structure of αKlotho and βKlotho will facilitate the development of agonists and antagonists of endocrine FGFs, which will be potentially useful for the treatment of various disorders, including chronic kidney disease and other ageing-related disorders.