
과당과잉 섭취 문제의 3가지 큰틀
과일을 과다하게 먹으면(하루 50g)이상 먹으면
1. 과일 = 대개 과당 50% 포도당 50%로 구성되어 있어서 혈당 스파이크가 발생
고혈당은 염증성 사이토카인을 자극하여 만성염증 유발
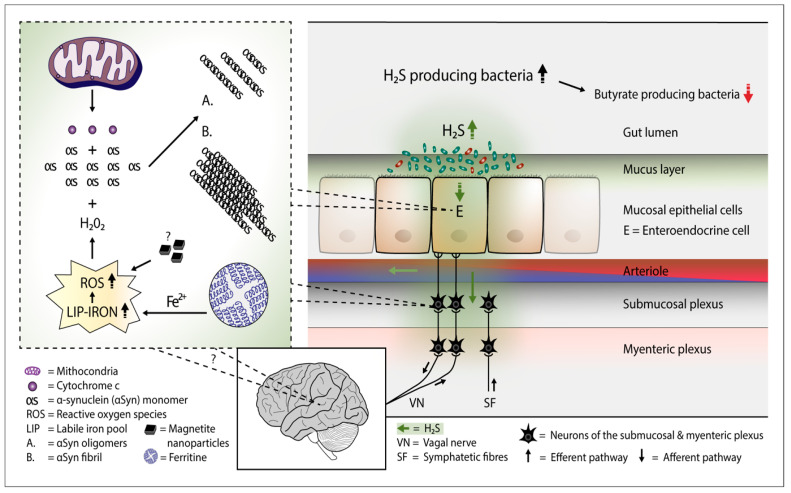
2. 흡수되지 않은 과당은 대장으로 내려가 발효되면서 IBS 발생
복통, 설사, 복부팽만, 방귀(가스) 생성
방귀 중 황화수소는 독성으로 작용하여 미토콘드리아에서 시토크롬 c 방출, 활성산소 증가 --> 파킨슨 병 유발
3. 소장에서 GLUT2, 5를 통해 수동적으로 흡수된 과당은 각종 질병을 일으킴
나트륨 흡수 증가, 고혈압
신장결석
비알콜성 지방간 등을 일으킴..
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6225702/


과당 과잉섭취 --> 요산염 대사 장애 --> 신장 결석...
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4195259/

참고로 어떤 환자는 5g만 먹어도 분리 과당(추출 과당)을 흡수하지 못해서 ibs를 일으킴
그렇다면 과일은?
Med Hypotheses. Author manuscript; available in PMC 2016 Sep 1.
Published in final edited form as:
Med Hypotheses. 2015 Sep; 85(3): 295–297.
Published online 2015 Jun 2. doi: 10.1016/j.mehy.2015.05.019
PMCID: PMC4729202
NIHMSID: NIHMS751451
PMID: 26059250
Is Fructose Malabsorption a Cause of Irritable Bowel Syndrome?
James J. DiNicolantonio, PharmD1 and Sean C. Lucan, MD, MPH, MS2
Author information Copyright and License information PMC Disclaimer
The publisher's final edited version of this article is available at Med Hypotheses
Abstract
Irritable Bowel Syndrome (IBS) is a condition that may be marked by abdominal pain, bloating, fullness, indigestion, belching, constipation and/or diarrhea. IBS symptoms can result from malabsorption of fructose. Fructose is a monosaccharide found naturally in small quantities in fruits and some vegetables, and in much larger quantities in industrially manufactured sweeteners and a dded sugars (e.g. sucrose and high fructose corn syrup). Fructose malabsorption leads to osmotic diarrhea as well as gas and bloating due to fermentation in the colon. A low-fructose diet has been found to improve IBS symptoms in some patients. This paper discusses the prevalence of fructose malabsorption and considers fructose ingestion as a possible cause of, and possible dietary treatment strategy for, IBS.
과민성 대장 증후군(IBS)은
복통, 복부 팽만감, 포만감, 소화 불량, 트림, 변비 및/또는 설사 등의
증상이 나타날 수 있는 질환입니다.
IBS 증상은
과당 흡수 장애로 인해 발생할 수 있습니다.
과당은
과일과 일부 채소에 자연적으로 소량 함유된 단당류이며,
산업적으로 제조된 감미료와 첨가당(예: 자당 및 고과당 옥수수 시럽)에는
훨씬 더 많은 양이 함유되어 있습니다.
과당 흡수 장애는
삼투성 설사뿐만 아니라
대장 내 발효로 인한 가스와 복부 팽만감을 유발합니다.
저과당 식단은
일부 환자에서 과민성 대장 증후군 증상을 개선하는 것으로 밝혀졌습니다.
이 백서에서는
과당 흡수 장애의 유병률에 대해 논의하고
과당 섭취가 과민성 대장 증후군의 가능한 원인 및
가능한 식이 치료 전략으로 고려됩니다.
Keywords: diarrhea, fructose, gastrointestinal, irritable bowel syndrome, sugar, high fructose corn syrup
Introduction
Irritable Bowel Syndrome (IBS) is a condition marked by abdominal pain, bloating, fullness, indigestion, belching, constipation and/or diarrhea. The cause of IBS is not definitively known although sensitivities to certain foods produce many symptoms consistent with the disorder. True food allergies are relatively uncommon in patients with IBS,(1) yet fructose malabsorption occurs frequently in IBS patients.(2) Poorly absorbed fructose can exacerbate and contribute to IBS symptoms and restricting fructose in the diet can lead to symptom improvement. This brief report explores some of the evidence for the link between fructose malabsorption and IBS.
과민성 대장 증후군(IBS)은
복통, 복부 팽만감, 포만감, 소화불량, 트림, 변비 및/또는 설사 등의
증상을 나타내는 질환입니다.
특정 음식에 민감하게 반응하면
과민성 대장 증후군과 일치하는 많은 증상이 나타나지만,
과민성 대장 증후군의 원인은 명확하게 밝혀지지 않았습니다.
실제 음식 알레르기는
IBS 환자에서 비교적 드물지만(1)
과당 흡수 장애는 IBS 환자에서 자주 발생합니다.(2)
과당이 제대로 흡수되지 않으면
IBS 증상이 악화될 수 있으며,
식단에서 과당을 제한하면 증상이 개선될 수 있습니다.
이 간략한 보고서에서는 과당 흡수 장애와 IBS 사이의 연관성에 대한 몇 가지 증거를 살펴봅니다.
Fructose Malabsorption May Cause Irritable Bowel Syndrome
From a physiologic standpoint, the human intestine lacks enzymes to digest and transport fructose.(1) The absorption of fructose occurs mainly via a non-specific glucose transporter (GLUT 2) and this transporter can be overwhelmed by small fructose loads.(1, 3-5) Some healthy individuals' capacity to absorb isolated fructose might be as little as 5 grams,(6) with fructose malabsorption (determined by hydrogen breath analysis) occurring at this level.(7) Bigger loads of fructose reduce the absorptive capacity in a dose-dependent way. In one experiment, ingestion of 5 or 10 grams of fructose lead to 10% of the study group being diagnosed as fructose malabsorbers, which increased to 40% when 20 grams of fructose was ingested.(3) Another study found malabsorption of fructose starting at higher doses (around 37.5 grams or higher).(8) In a randomized, double-blind, dose-response study, healthy individuals were able to tolerate 25 grams of fructose but when 50 grams of fructose was administered, 80% of patients exhibited malabsorption (based on breath tests measuring hydrogen and methane) with approximately 50% of subjects reporting mild to moderate belching, bloating or diarrhea.5 Another study showed that almost 40% of patients exhibited fructose malabsorption at an intake of 25 grams, and 66% of patients at an intake of 50 grams.(9)
Unabsorbed fructose may lead to an osmotic effect by increasing the liquidity of intestinal contents and increasing gastrointestinal motility.(1) Additionally, unabsorbed fructose can lead to the production of short chain fatty acids, hydrogen, carbon dioxide and trace gases from its fermentation by bacteria that reside in the colon. The increased production of gases can cause gastrointestinal side effects that mimic IBS.(1, 3, 4, 6, 10) Other possible mechanisms of fructose-induced gastrointestinal symptoms could include local ‘irritating’ effects of fructose upon contact with the intestinal tract. Yudkin indicated that after eating sugar, patient's intestine's become irritated and red.(11)
생리학적 관점에서 볼 때,
사람의 장에는 과당을 소화하고
운반하는 효소가 부족합니다.(1)
음식을 먹고 위장장애 : 33%~50%
일반인 생각 : 25% 음식 알러지가 있다고 인식, 실제 검사상으로는 성인 1~4%, 어린이 4~8% 음식 알러지
과당을 줄이고, 식이섬유를 늘리면 ibs 증상 개선 가능!!
과당의 흡수는
주로 비특이적 포도당 수송체(GLUT 2)를 통해 이루어지며
이 수송체는 소량의 과당 부하에도 압도당할 수 있습니다. (1, 3-5)
영향력지수 7점 논문
https://pubmed.ncbi.nlm.nih.gov/17217453/

전세계 과당 섭취량 11~54g
50%가 넘는 사람들이 한번에 25g의 과당을 흡수하지 못함.
20명 double blind 연구
10% 증상은 없지만 산소, 메탄검사에서 문제
55%가 50g 과당섭취에서 증상이 발생
일부 건강한 사람의 분리 과당 흡수 능력은
5g에 불과할 수 있으며(6)
이 수준에서 과당 흡수 장애(수소 호흡 분석으로 확인)가 발생합니다.(7)
과당을 더 많이 섭취하면
용량 의존적으로 흡수 능력이 감소합니다.
한 실험에서는
5g 또는 10g의 과당을 섭취하면
연구 그룹의 10%가 과당 흡수 장애로 진단되었으며,
20g의 과당을 섭취하면 40%로 증가했습니다.(3)
또 다른 연구에서는
과당 흡수 장애가
더 많은 양(약 37.5g 이상)에서 시작되는 것으로 나타났습니다. (8)
무작위, 이중맹검, 용량 반응 연구에서
건강한 사람은 25그램의 과당을 견딜 수 있었지만
50그램의 과당을 투여했을 때
80%의 환자가 흡수 장애를 보였으며(수소와 메탄을 측정하는 호흡 검사 기준),
약 50%의 피험자가
경증에서 중등도의 트림, 복부 팽만, 설사를 보고했습니다.5
또 다른 연구에 따르면
과당을 25그램 섭취한 환자의 약 40%,
50그램 섭취한 환자의 66%가
과당 흡수 장애를 보인 것으로 나타났습니다.(9)
흡수되지 않은 과당은
장 내용물의 유동성을 증가시키고
위장 운동성을 증가시켜 삼투압 효과를 유발할 수 있습니다.(1)
또한 흡수되지 않은 과당은
대장에 존재하는 박테리아에 의해 발효되어
단쇄 지방산, 수소, 이산화탄소 및 미량 가스를 생성할 수 있습니다.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8946538/
가스 생성 증가는
과민성 대장 증후군을 모방하는
위장 부작용을 일으킬 수 있습니다.(1, 3, 4, 6, 10)
과당으로 인한 위장 증상의 다른 가능한 메커니즘으로는
과당이 장과 접촉할 때
국소적인 '자극' 효과가 있을 수 있습니다.
유드킨은
설탕을 섭취한 후 환자의 장이 자극을 받아
붉어졌다고 지적했습니다.(11)
Acute feeding studies have shown that almost one-third of patients with IBS are unable to tolerate large amounts of fructose, whereas patients without IBS do not have this issue. (1),(12-15) In patients who have a positive hydrogen breath test (i.e. a rise in breath hydrogen or methane indicating fructose malabsorption/fermentation in the intestine), 75% have their principal symptoms at the time of breath test positivity.(5) Data are somewhat conflicting in regards to if patients with functional gastrointestinal disorders (i.e. IBS) have a greater likelihood of also being fructose malabsorbers (40-80% prevalence) as compared to healthy individuals (11-70%).5 An uncontrolled study showed that the prevalence of incomplete fructose absorption (at 25g) is higher in patients with functional bowel disorders (36-75%) versus healthy subjects (0-50%).(6) While it is not known for certain if gastrointestinal disorders can cause fructose malabsorption (although it is possible that if intestinal glucose transporters are injured this would then affect fructose absorption), it seems highly probable that fructose malabsorption can lead to gastrointestinal symptoms.
급성 food 연구에 따르면
과민성 대장 증후군 환자의 거의 1/3이
다량의 과당을 견디지 못하는 반면,
과민성 대장 증후군이 없는 환자는
이러한 문제가 없는 것으로 나타났습니다. (1),(12-15)
--> 과민성 장증후군 환자가 과당을 줄였더니 74%에서 ibs 증상이 개선됨.
수소 호흡 검사(즉, 장내 과당 흡수 장애/발효를 나타내는 호흡 수소 또는 메탄의 증가)에서
양성 반응을 보인 환자의 75%는
호흡 검사 양성 시점에 주요 증상이 나타납니다.(5)
기능성 위장 장애(즉, IBS)가 있는 환자가
건강한 사람(11-70%)에 비해
과당 흡수 장애(40-80% 유병률)가 있을 가능성이 큰지에 대해서는
데이터가 다소 상반된 것으로 나타나고 있습니다. 5
통제되지 않은 연구에 따르면
기능성 장 질환 환자(36-75%)는
건강한 사람(0-50%)에 비해
불완전 과당 흡수 유병률(25g 기준)이 더 높습니다.(6)
위장 장애가
과당 흡수 장애를 유발할 수 있는지 확실하지는 않지만(장내 포도당 수송체가 손상되면 과당 흡수에 영향을 미칠 수 있음),
과당 흡수 장애가 위장 증상을 유발할 가능성이 높은 것으로 보입니다.
The studies referenced above tested isolated fructose. Such studies may overestimate the prevalence of fructose malabsorption, as fructose is almost always consumed together with glucose in both naturally occurring and processed foods.(1) Indeed, when patients ingested 40 g of high fructose corn syrup (HFCS)-55, the prevalence of fructose intolerance (defined as having both an abnormal breath test and symptoms) was just 7%.(6) Yet, when pure fructose was consumed, the prevalence increased to a prevalence of 40% (p-value for the difference in prevalence between HFCS-55 and pure fructose = 0.062).(6) Despite a somewhat low prevalence of ‘fructose intolerance’ (when both gastrointestinal symptoms and a positive hydrogen breath test are used as the definition) 10% of healthy individuals and 47% of patients with IBS have 1 or more symptoms upon ingestion of HFCS-55 (providing 40 grams of fructose). Moreover, when ingesting 40 grams of fructose (provided as HFCS-55), 20% of healthy individuals and 30% of IBS patients were shown to have fructose malabsorption (based on an abnormal hydrogen breath test). Thus, randomized data indicate that around 1 in 2 patients with IBS have an exacerbation of gastrointestinal symptoms if they ingest 40 grams of fructose (when obtained from ingestion of HFCS-55). This level of fructose can be obtained by ingesting approximately two 12 oz. cans of regular soda. The prevalence of fructose malabsorption would presumably be higher if HFCS-90 (90% fructose; e.g., occurring in many agave products) were used as the sugar source instead as fructose malabsorption is both dose and concentration dependent.
위에 언급된 연구는
분리된 과당을 테스트한 것입니다.
과당은
자연 식품과 가공 식품 모두에서
거의 항상 포도당과 함께 섭취되기 때문에
이러한 연구는 과당 흡수 장애의 유병률을 과대평가할 수 있습니다.(1)
실제로
고과당 옥수수 시럽(HFCS)-55를
40g 섭취한 환자의 과당 불내성(호흡 검사 이상과 증상이 모두 있는 것으로 정의)의 유병률은
7%에 불과한 것으로 나타났습니다. (6)
그러나
순수 과당을 섭취한 경우
유병률이 40%로 증가했습니다(HFCS-55와
순수 과당의 유병률 차이에 대한 p-값 = 0.062). (6)
'과당 과민증'(위장 증상과 수소 호흡 검사 양성 반응을 모두 정의로 사용하는 경우)의 유병률은
다소 낮지만
건강한 사람의 10%와
과민성 대장 증후군 환자의 47%가
HFCS-55 섭취(과당 40g 제공) 시
1개 이상의 증상을 경험하는 것으로 나타났습니다.
또한
40g의 과당(HFCS-55로 제공)을 섭취했을 때
건강한 사람의 20%와
IBS 환자의 30%가 과당 흡수 장애(비정상적인 수소 호흡 테스트 기준)가 있는 것으로 나타났습니다.
따라서
무작위 데이터에 따르면
IBS 환자 2명 중 1명은
40g의 과당을 섭취할 경우 위장 증상이 악화되는 것으로 나타났습니다(HFCS-55 섭취로 얻은 경우).
이 수준의 과당은
일반 탄산음료 12온스 캔 약 2개를 섭취하면 얻을 수 있습니다.
12온스 = 360ml
6온스 = 180ml --> 작은 종이컵
과당 흡수 장애는
과당의 용량과 농도에 따라 달라지므로
HFCS-90(과당 90%, 예: 많은 아가베 제품에서 발생)을 당원으로 사용하는 경우
과당 흡수 장애의 유병률이 더 높을 것으로 추정됩니다.
Just as fructose loads may cause or exacerbate symptoms associated with IBS, dietary restriction of fructose may improve symptoms. In one study in patients with IBS and fructose malabsorption, 74% of individuals had improvements in all abdominal symptoms when avoiding fructose in the diet (e.g., fruits with a fructose concentration higher than glucose, certain dried fruits, fruit juice, high fructose corn syrup, sucrose, honey, etc.).(12) Additionally, overall positive response was significantly better in those adherent versus non-adherent to the diet (85% vs. 36%; P<0.01), including improvement in individual symptoms (P<0.01 for all symptoms). The authors concluded that, “fructose malabsorption dietary therapy achieves a high level of sustained adherence and good symptomatic response.” Other studies show similar symptoms improvement with fructose restriction.(10),(12, 16) Importantly, others(5, 7, 8, 17) suggest that fructose malabsorption is dose-dependent as well as concentration dependent.
과당 섭취가
과민성 대장 증후군과 관련된 증상을 유발하거나 악화시킬 수 있는 것처럼,
식단에서 과당을 제한하면 증상이 개선될 수 있습니다.
과당 흡수 장애가 있는 IBS 환자를 대상으로 한 연구에 따르면,
식단에서 과당을 피했을 때
74%의 환자가 모든 복부 증상이 개선되었다고 합니다(예, 포도당보다 과당 농도가 높은 과일, 특정 말린 과일, 과일 주스, 고과당 옥수수 시럽, 자당, 꿀 등).(12)
꿀 : 40% 과당, 30% 포도당, 17% 물
또한,
개별 증상 개선(모든 증상에 대해 P<0.01)을 포함하여
식단을 준수하는 사람들이
준수하지 않는 사람들보다
전반적인 긍정적인 반응이 유의하게 더 좋았습니다(85% 대 36%, P<0.01).
저자들은 "과당 흡수 장애 식이 요법은
높은 수준의 지속적인 순응도와 좋은 증상 반응을 달성한다"고 결론지었습니다.
다른 연구에서도
과당 제한으로 비슷한 증상 개선 효과를 보였습니다.(10),(12, 16)
중요한 것은
다른 연구(5, 7, 8, 17)에서는
과당 흡수 장애가
농도뿐만 아니라
용량에 따라 달라진다는 점을 시사한다는 점입니다.
Fructose is not consumed in isolation in the diets of free-living individuals though, and more general carbohydrate restriction has been shown to be beneficial for symptoms relief. Two-thirds of patients with abdominal bloating and gas-related symptoms (72.2% with sugar malabsorption—i.e. malabsorption of lactose, fructose plus sorbitol, or both [lactose and fructose + sorbitol), had clinical improvement out to 12 months (i.e. complete improvement in 50% and partial improvement in 16.7%) when educated about dietary restriction of these substances.(18) A randomized trial indicated that more than three-quarters of diarrhea-predominant IBS patients derived adequate relief of symptoms (stool frequency decreased, stool consistency improved from diarrheal to normal form, and pain scores and quality-of-life measures significantly improved) when placed on a very low carbohydrate diet.(19) In another trial, a marked improvement in symptoms in over 50% of patients (with either IBS or nonspecific functional bowel complaints) was shown upon restriction of either lactose, fructose, or sorbitol for 1 month.(20) The authors concluded that, “dietary restriction of the offending sugar(s) should be implemented before the institution of drug therapy.” This trial also showed that only 7% of IBS and 8% of patients with functional bowel complaints absorbed all three sugars normally (e.g. the frequency of sugar malabsorption among patients in both groups was 78% for lactose, 44% for fructose, and 73% for a mixture of fructose + sorbitol).
그러나
자유 생활을 하는 사람들의 식단에서
과당을 단독으로 섭취하는 것은 아니며,
일반적인 탄수화물 제한이
증상 완화에 도움이 되는 것으로 나타났습니다.
복부 팽만감 및 가스 관련 증상이 있는
환자의 3분의 2(당 흡수 장애, 즉 유당, 과당+소르비톨 또는 둘 다[유당과 과당+소르비톨] 흡수 장애가 있는 72.2%)가
이러한 물질의 식이 제한에 대한 교육을 받은 후
12개월까지 임상적으로 개선되었습니다(50%는 완전 개선, 16.7%는 부분 개선됨). (18)
무작위 시험에 따르면
설사를 주로 하는 과민성 대장 증후군 환자의 4분의 3 이상이
매우 낮은 탄수화물 식단을 섭취했을 때
적절한 증상 완화(배변 빈도 감소, 대변의 일관성이 설사에서 정상으로 개선, 통증 점수 및 삶의 질 측정이 유의하게 개선)를 경험한 것으로 나타났습니다. (19)
또 다른 시험에서는
유당, 과당 또는
소르비톨을 1개월 동안 제한했을 때
50% 이상의 환자(과민성 대장 증후군 또는 비특이적 기능성 장 질환)에서
증상이 현저하게 개선된 것으로 나타났습니다.(20)

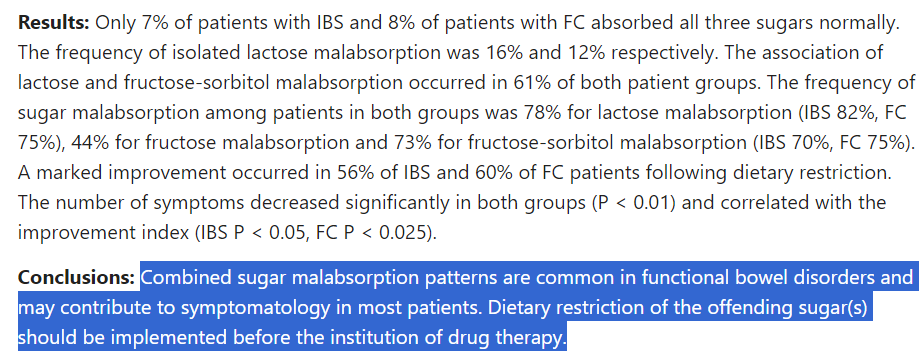
저자는 "약물 치료를 시행하기 전에
문제가 되는 당류의 식이 제한을 시행해야 한다"고 결론지었습니다.
이 실험에서는 또한
과민성 대장 증후군 환자의 7%와
기능성 장 질환 환자의 8%만이
세 가지 당을 모두 정상적으로 흡수하는 것으로 나타났습니다(예: 두 그룹 환자들의 당 흡수 장애 빈도는 유당 78%, 과당 44%, 과당+소르비톨 혼합물 73%).
The absorption of fructose is more efficient when combined with glucose.(21) Fructose loads from whole foods with mixed carbohydrates, like fruits and vegetables, might be expected to cause little problem with regard to malabsorption (except for perhaps fruits with a higher fructose concentration versus glucose, such as honeydew, star fruit, pear, pawpaw/papaya, mango, guava, watermelon, and apple to name a few). But refined products that are particularly high in fructose relative to glucose (such as HFCS-90 or agave, in which fructose has been found to make up 84.29% of the carbohydrate content(22)) may particularly pose problems for patients with IBS.
과당의 흡수는
포도당과 결합할 때 더 효율적입니다.(21)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4145298/
과일이나 채소와 같이
탄수화물이 혼합된 전체 식품에서
과당을 섭취하는 것은 흡수 장애와 관련하여
거의 문제를 일으키지 않을 것으로 예상됩니다
(단, 포도당에 비해 과당 농도가 높은 과일인
멜론, 스타 과일, 배, 포포/파파야, 망고, 구아바, 수박, 사과 등을 제외하면).
그러나
포도당에 비해 과당 함량이
특히 높은 정제 제품(예: 과당이 탄수화물 함량의 84.29%를 차지하는 것으로 밝혀진 HFCS-90 또는 아가베)은
특히 IBS 환자에게 문제를 일으킬 수 있습니다(22).
Implications
Encouraging patients to choose whole foods (e.g., vegetables, grains, nuts, and a selection of fruits as tolerated) and avoid highly-processed foods (e.g., sodas and industrially produced baked goods full of fructose-predominant added sugars), might lead to decided benefit and symptom control in patients with IBS.
환자에게 통식품(예: 채소, 곡물, 견과류, 내약성이 있는 일부 과일)을 선택하고
고도로 가공된 식품(
예: 과당이 주성분인 첨가당이 가득한
탄산음료 및 산업적으로 생산된 제빵 제품)을 피하도록 권장하면
IBS 환자의 증상 조절에 확실한 도움이 될 수 있습니다.
Acknowledgments
None
Abbreviations
| HFCS | high fructose corn syrup |
| IBS | irritable bowel syndrome |
Footnotes
Authors' contributions: Dr. DiNicolantonio conducted the primary literature review, conceived the paper , and drafted the arguments. Dr. Lucan substantively reframed, reshaped, and revised the manuscript.
Grants, conflicts of interest, disclosures, writing assistance, funding: Research by Dr. Lucan reported in this publication was supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under Award Number K23HD079606. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
1. Eswaran S, Tack J, Chey WD. Food: the forgotten factor in the irritable bowel syndrome. Gastroenterol Clin North Am. 2011;40:141–162. [PubMed] [Google Scholar]
2. Lee YJ, Park KS. Irritable bowel syndrome: emerging paradigm in pathophysiology. World J Gastroenterol. 2014;20:2456–2469. [PMC free article] [PubMed] [Google Scholar]
3. Rumessen JJ, Gudmand-Hoyer E. Functional bowel disease: malabsorption and abdominal distress after ingestion of fructose, sorbitol, and fructose-sorbitol mixtures. Gastroenterology. 1988;95:694–700. [PubMed] [Google Scholar]
4. Gibson PR, Newnham E, Barrett JS, Shepherd SJ, Muir JG. Review article: fructose malabsorption and the bigger picture. Aliment Pharmacol Ther. 2007;25:349–363. [PubMed] [Google Scholar]
5. Rao SS, Attaluri A, Anderson L, Stumbo P. Ability of the normal human small intestine to absorb fructose: evaluation by breath testing. Clin Gastroenterol Hepatol. 2007;5:959–963. [PMC free article] [PubMed] [Google Scholar]
6. Skoog SM, Bharucha AE, Zinsmeister AR. Comparison of breath testing with fructose and high fructose corn syrups in health and IBS. Neurogastroenterol Motil. 2008;20:505–511. [PMC free article] [PubMed] [Google Scholar]
7. Rumessen JJ, Gudmand-Hoyer E. Absorption capacity of fructose in healthy adults. Comparison with sucrose and its constituent monosaccharides. Gut. 1986;27:1161–1168. [PMC free article] [PubMed] [Google Scholar]
8. Ravich WJ, Bayless TM, Thomas M. Fructose: incomplete intestinal absorption in humans. Gastroenterology. 1983;84:26–29. [PubMed] [Google Scholar]
9. Choi YK, Johlin FC, Jr, Summers RW, Jackson M, Rao SS. Fructose intolerance: an under-recognized problem. Am J Gastroenterol. 2003;98:1348–1353. [PubMed] [Google Scholar]
10. Choi YK, Kraft N, Zimmerman B, Jackson M, Rao SS. Fructose intolerance in IBS and utility of fructose-restricted diet. J Clin Gastroenterol. 2008;42:233–238. [PubMed] [Google Scholar]
11. Pure JY. white and deadly. Penguin Books. 2012 [Google Scholar]
12. Shepherd SJ, Gibson PR. Fructose malabsorption and symptoms of irritable bowel syndrome: guidelines for effective dietary management. J Am Diet Assoc. 2006;106:1631–1639. [PubMed] [Google Scholar]
13. Nelis GF, Vermeeren MA, Jansen W. Role of fructose-sorbitol malabsorption in the irritable bowel syndrome. Gastroenterology. 1990;99:1016–1020. [PubMed] [Google Scholar]
14. Fernandez-Banares F, Esteve-Pardo M, de Leon R, et al. Sugar malabsorption in functional bowel disease: clinical implications. Am J Gastroenterol. 1993;88:2044–2050. [PubMed] [Google Scholar]
15. Symons P, Jones MP, Kellow JE. Symptom provocation in irritable bowel syndrome. Effects of differing doses of fructose-sorbitol. Scand J Gastroenterol. 1992;27:940–944. [PubMed] [Google Scholar]
16. Johlin FC, Jr, Panther M, Kraft N. Dietary fructose intolerance: diet modification can impact self-rated health and symptom control. Nutr Clin Care. 2004;7:92–97. [PubMed] [Google Scholar]
17. Truswell AS, Seach JM, Thorburn AW. Incomplete absorption of pure fructose in healthy subjects and the facilitating effect of glucose. Am J Clin Nutr. 1988;48:1424–1430. [PubMed] [Google Scholar]
18. Fernandez-Banares F, Rosinach M, Esteve M, Forne M, Espinos JC, Maria Viver J. Sugar malabsorption in functional abdominal bloating: a pilot study on the long-term effect of dietary treatment. Clin Nutr. 2006;25:824–831. [PubMed] [Google Scholar]
19. Austin GL, Dalton CB, Hu Y, et al. A very low-carbohydrate diet improves symptoms and quality of life in diarrhea-predominant irritable bowel syndrome. Clin Gastroenterol Hepatol. 2009;7:706–708. e701. [PMC free article] [PubMed] [Google Scholar]
20. Goldstein R, Braverman D, Stankiewicz H. Carbohydrate malabsorption and the effect of dietary restriction on symptoms of irritable bowel syndrome and functional bowel complaints. Isr Med Assoc J. 2000;2:583–587. [PubMed] [Google Scholar]
21. Laughlin MR. Normal roles for dietary fructose in carbohydrate metabolism. Nutrients. 2014;6:3117–3129. [PMC free article] [PubMed] [Google Scholar]
22. Willems JL, Low NH. Major carbohydrate, polyol, and oligosaccharide profiles of agave syrup. Application of this data to authenticity analysis. J Agric Food Chem. 2012;60:8745–8754. [PubMed] [Google Scholar]