https://pmc.ncbi.nlm.nih.gov/articles/PMC11148654/
염증성 장질환(IBD, 크론병·궤양성대장염)의
임상 증상이 나타나기 전(preclinical phase) 단계를
시간적·생물학적으로 세밀하게 구분한 최초의 체계적 리뷰.
IBD는
오랜 잠복기를 거쳐 발병한다는 점을 강조하며,
예방·조기개입의 새로운 전략을 제시.
1. At risk 단계 (유전적·조기 노출)
3. Preclinical phase: Disease Expansion (질환 확장 단계)
|
IBD의 Preclinical 단계 구분 (주요 기여)
- Phase 0 (Genetic Risk)
- 유전적 취약성만 존재 (예: NOD2, ATG16L1, IL23R 변이).
- 아직 어떠한 생물학적 변화도 없음.
- Phase 1 (Preclinical Inflammation)
- 장내 미생물 불균형(dysbiosis), 장벽 투과성 증가, 미세염증 시작.
- 혈청 바이오마커(anti-microbial antibodies, fecal calprotectin) 상승.
- Phase 2 (Subclinical Inflammation)
- 영상(내시경, MRI)이나 조직검사에서 경미한 염증 소견.
- 증상은 아직 없거나 매우 경미.
- Phase 3 (Clinical IBD)
- 전형적인 증상(설사, 복통, 혈변)과 내시경적 염증이 명확히 나타남.
주요 질문 6가지
|
주요 발견 및 함의
- Preclinical 단계에서 장내 미생물, 면역, 장벽 기능의 변화가 수년~수십 년 동안 진행됨.
- 예방 전략 가능성: 고위험군(가족력, 유전적 위험)에서 조기 스크리닝(fecal calprotectin, microbiome profiling)과 생활습관·식이·microbiome intervention을 통해 발병 지연 또는 예방 가능.
- IBD 발병은 단일 사건이 아니라 다단계 진행 과정이라는 새로운 패러다임 제시.
전체 구조 (시간축)
3. Cumulative IBD Risk (누적 위험)
|
의의
- IBD를 “예방 가능한 만성질환”으로 재정의.
- 향후 조기진단·예방의학 연구의 로드맵 역할.
- 임상적으로는 가족력 있는 사람들의 정기적 바이오마커 모니터링을 권고.
Nat Rev Gastroenterol Hepatol
. Author manuscript; available in PMC: 2024 Jun 4.
Published in final edited form as: Nat Rev Gastroenterol Hepatol. 2023 Nov 10;21(2):86–100. doi: 10.1038/s41575-023-00854-4
Deciphering the different phases of preclinical inflammatory bowel disease
Jonas J Rudbaek 1,2, Manasi Agrawal 1,4, Joana Torres 4,5,6,7, Saurabh Mehandru 4, Jean-Frederic Colombel 4, Tine Jess 1,3,†
- Author information
- Article notes
- Copyright and License information
PMCID: PMC11148654 NIHMSID: NIHMS1994548 PMID: 37950021
The publisher's version of this article is available at Nat Rev Gastroenterol Hepatol
Abstract
Inflammatory bowel diseases (IBD) are immune-mediated inflammatory diseases (IMIDs [G]) of the gastrointestinal tract and include two subtypes, Crohn’s disease and ulcerative colitis. It is well-recognized that IBD is associated with a complex multifactorial etiology that includes genetic predisposition and environmental exposures, with downstream dysregulation of systemic immune function and host-microbial interactions in the local environment in the gut. Evidence to support the notion of a multistage development of IBD is growing, as has been observed in other IMIDs such as rheumatoid arthritis and systemic lupus erythematosus. With the rising worldwide incidence of IBD, it is increasingly important to understand the complex interplay of pathological events during the different stages of disease development to enable IBD prediction and prevention strategies. In this article, we review comprehensively the current evidence pertaining to the pre-clinical phase of IBD, including at risk, initiation and expansion phases. We also discuss the framework of preclinical IBD, expanding on underlying pathways in IBD development, future research directions and IBD development in the context of other IMIDs.
염증성 장질환(Inflammatory Bowel Diseases, IBD)은
위장관의 면역매개 염증성 질환(IMIDs)으로,
크론병(Crohn’s disease)과 궤양성 대장염(ulcerative colitis)의 두 가지 아형을 포함합니다.
IBD는
유전적 소인(genetic predisposition)과 환경 노출(environmental exposures)이 복합적으로 작용하며,
전신 면역 기능의 조절 이상과
장 내 국소 환경에서의 숙주-미생물 상호작용의 이상이 발생하는
다인자성(multifactorial) 질환임이 잘 알려져 있습니다.
류마티스 관절염(rheumatoid arthritis)이나
전신홍반루푸스(systemic lupus erythematosus)와 같은
다른 IMIDs에서 관찰된 바와 같이,
IBD가 다단계(multistage)로 진행된다는 증거가 점차 늘어나고 있습니다.
전 세계적으로 IBD 발병률이 증가함에 따라,
질환 발달의 다양한 단계에서 일어나는 병리학적 사건들의
복잡한 상호작용을 이해하는 것이
IBD의 예측(prediction)과 예방(prevention) 전략을 수립하는 데 점점 더 중요해지고 있습니다.
본 논문에서는
위험(at risk) 단계,
발병 개시(initiation) 단계,
확장(expansion) 단계를 포함한 IBD의 pre-clinical phase(임상 전 단계)에 대한 현재의 증거를 포괄적으로 검토합니다.
또한
preclinical IBD의 프레임워크,
IBD 발달의 기저 경로(underlying pathways), 향후 연구 방향,
그리고 다른 IMIDs 맥락에서의 IBD 발달에 대해서도 논의합니다.
ToC Blurb
Inflammatory bowel disease (IBD) is an immune-mediated inflammatory disease (IMID). Here, the authors review evidence on the preclinical phase of IBD, outlining and describing the proposed at risk, initiation and expansion phases. Overlap with other IMIDs is discussed alongside the possible future directions for research into preclinical IBD.
염증성 장질환(IBD)은
면역매개 염증성 질환(IMID)입니다.
본 리뷰에서 저자들은
IBD의 preclinical phase(임상 전 단계)에 대한 증거를 검토하며,
제안된 위험(at risk) 단계, 발병 개시(initiation) 단계, 확장(expansion) 단계를 개요하고 설명합니다.
다른 IMID와의 중복(overlap)도 논의하며,
preclinical IBD 연구의 가능한 미래 방향을 제시합니다.
Introduction
Inflammatory bowel diseases (IBD) are chronic immune-mediated diseases (IMIDs) of the gastrointestinal tract. IBD takes two major forms, ulcerative colitis and Crohn’s disease, which differ in clinical presentation, disease location, and molecular pathology. Despite such differences, ulcerative colitis and Crohn’s disease share a complex etiology covering a multifaceted interplay of genetic susceptibility, environmental factors, dysregulated immune responses, and altered gut microbiota, which, in a yet unknown combination, lead to disease development1–4.
The increasing incidence of IBD worldwide5 makes research into ways of achieving secondary or primary prevention of IBD of great importance. To attain the goal of earlier diagnosis and prevention in IBD it is imperative that we understand the complex interplay of molecules and pathways that drives disease development in the pre-clinical phase, including pathological changes occurring in the early life period. It has been proposed that the clinical onset of IBD is preceded by a crucial pre-clinical phase, as observed for several other IMIDs, including rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE)6–8. One of the first studies to suggest the presence of a pre-clinical phase in IBD was a study published in 2005 by Israeli et al.9 after the observation of an association between anti-Saccharomyces cerevisiae (ASCA) positivity, an anti-microbial antibody commonly associated with Crohn’s disease, and later development of IBD in a cohort of 32 patients with Crohn’s disease, 8 patients with ulcerative colitis and 95 healthy individuals as controls. Since that study, new studies have brought evidence for a pre-clinical phase of IBD and a series of exciting observations have been made that might help shape our overall understanding of the length and form of the pre-clinical phase of IBD and guide future research in the field.
In this Review, we seek to compile the available evidence pertaining to the pre-clinical phase of IBD to better characterize the individual stages of the pre-clinical disease [G] period, using the nomenclature suggested in a 2021 European Crohn’s and Colitis Organization (ECCO) workshop10, and the importance of understanding the combination of factors that drive disease development in the different pre-clinical phases. We also discuss the overlap with other IMIDs and outline possible future directions of research within the field of pre-clinical IBD.
Introduction (서론)
염증성 장질환(Inflammatory bowel diseases, IBD)은
위장관의 만성 면역매개 질환(immune-mediated diseases, IMIDs)입니다.
IBD는
궤양성 대장염(ulcerative colitis)과 크론병(Crohn’s disease)의 두 가지 주요 형태를 가지며,
이들은 임상 양상, 질환 위치, 분자 병리학에서 차이를 보입니다.
이러한 차이에도 불구하고,
궤양성 대장염과 크론병은
유전적 취약성(genetic susceptibility),
환경 요인,
조절 이상된 면역 반응,
장내 미생물총 변화가 복잡하게 상호작용하는 다인자성(multifactorial) 병인을 공유하며,
아직 완전히 밝혀지지 않은 조합으로 질환이 발달합니다¹⁻⁴.
a multifaceted interplay of genetic susceptibility,
environmental factors,
dysregulated immune responses,
and altered gut microbiota
전 세계적으로 IBD 발병률이 증가하고 있는 가운데⁵,
IBD의 2차 또는 1차 예방 전략을 개발하는 연구가 매우 중요해졌습니다.
IBD의 조기 진단과 예방이라는 목표를 달성하기 위해서는,
pre-clinical phase(임상 전 단계)에서 질환 발달을 이끄는 분자와 경로들의 복잡한 상호작용,
특히 조기 생애 기간(early life period)에 발생하는 병리학적 변화를 이해하는 것이 필수적입니다.
여러 다른 IMID(류마티스 관절염(RA),
전신홍반루푸스(SLE) 등)에서 관찰된 바와 같이⁶⁻⁸,
IBD의 임상 발현도 중요한 pre-clinical phase에 선행된다는 제안이 있습니다.
IBD에서 pre-clinical phase의 존재를 처음 시사한 연구 중 하나는
2005년 Israeli et al.⁹이 발표한 연구로,
크론병 환자 32명, 궤양성 대장염 환자 8명, 건강 대조군 95명을 대상으로
크론병과 흔히 연관된 항균 항체인 anti-Saccharomyces cerevisiae (ASCA) 양성과
이후 IBD 발병 사이의 연관성을 관찰한 결과입니다.
그 이후 새로운 연구들이 IBD의 pre-clinical phase에 대한 증거를 제시했으며,
pre-clinical phase의 길이와 형태,
그리고 이 분야의 미래 연구를 안내할 수 있는 흥미로운 관찰들이 이어지고 있습니다.
본 리뷰에서는
IBD의 pre-clinical phase에 대한 이용 가능한 증거를 종합하여,
2021년 European Crohn’s and Colitis Organization (ECCO) 워크숍에서 제안된 용어를 사용하여¹⁰
pre-clinical disease 기간의 개별 단계를 더 잘 특징짓고,
서로 다른 pre-clinical 단계에서 질환 발달을 이끄는 요인들의 조합을 이해하는 중요성을 논의합니다.
또한
다른 IMID와의 중복(overlap)을 논의하고,
pre-clinical IBD 분야의 가능한 미래 연구 방향을 제시합니다.
Risk factors for IBD
A major focus within IBD research has been attempting to elucidate factors that increase the future risk of IBD development. Thus far, factors such as inherited genetic risk loci and exposures, both during early life and later in life, have been shown to increase risk of disease development11–14. These factors could have a synergistic role in both priming the intestinal immune system against commensal [G] and self-antigens [G], and making it more prone to dysregulation and therefore breaking down immune tolerance [G], culminating in disease initiation.
Risk factors for IBD (IBD의 위험 요인)
IBD 연구의 주요 초점 중 하나는
IBD 발달의 미래 위험을 증가시키는 요인을 밝히는 것이었습니다.
지금까지
유전적 위험 loci와 조기 생애 및 후기 생애 노출과 같은 요인들이
질환 발달 위험을 증가시키는 것으로 밝혀졌습니다¹¹⁻¹⁴.
이러한 요인들은
장내 면역계를 공생 미생물(commensal)과 자가 항원(self-antigens)에 대해 priming하고,
면역 조절 이상(dysregulation)을 일으키기 쉽게 만들어
면역 관용(immune tolerance)을 붕괴시키는 데 시너지 효과를 발휘할 수 있으며,
결국 질환 개시(disease initiation)로 이어질 수 있습니다.
Genetic predisposition
A genetic component in the development of IBD is well established. A concordance rate of 50% for Crohn’s disease and around 19% for ulcerative colitis was found for monozygotic twins15,16. Furthermore, first-degree relatives (FDRs) have a significantly higher risk of developing disease (Crohn’s disease, relative risk (RR), 10; 95 % CI, 2.73–25.60; ulcerative colitis, RR, 8; 95% CI, 5.86–10.67)17. These findings sparked an interest in identifying the genetic elements causing this higher familial prevalence of the disease. Since the introduction of genome-wide association studies (GWAS), the identification of genetic risk loci for IBD have been steadily increasing, and some of the identified loci include genes associated with immune function, including NOD2, OSMR, SMAD3, IL23R and the HLA locus12,18,19. So far as many as 240 IBD-associated risk loci have been identified 11,18. This development speaks to the possibility that with increasingly high-resolution studies, more relevant risk loci are likely to be uncovered. Present findings indicate that genetic risk explains disease development only to a relatively minor extent. A large trans-ancestry association study utilizing a cohort of 86,640 individuals of European decent and 9,846 individuals of East Asian, Indian or Iranian decent found that the identified loci explain only 13.1% and 8.2% of the variance in disease liability, for Crohn’s disease and ulcerative colitis, respectively18, with substantial differences in genetic risk determinants across European and Asian populations, indicating that most of the variance is either due to undiscovered loci or other factors such as environmental exposures. Furthermore, notably few of the identified loci have presently been mechanistically linked to the disease11,12,18. Overall, genetics only explain a subset of the identifiable IBD risk, thereby highlighting the role of the environment or other non-genetically mediated effects in disease development13. Relative contribution of genetic risk versus environmental risk is likely inter-individual with the rarer monogenic forms of IBD having the largest contribution from genetic factors, whereas in other cases environmental factors could play a more prominent part.
Genetic predisposition (유전적 소인)
IBD 발달에서
유전적 요소가 중요하다는 것은 잘 확립되어 있습니다.
일란성 쌍생아에서
크론병의 일치율(concordance rate)은 50%,
궤양성 대장염은 약 19%로 보고되었습니다¹⁵,¹⁶.
또한 1촌 친척(FDRs)은
IBD 발병 위험이 유의하게 높습니다
(크론병: 상대위험도(RR) 10, 95% CI 2.73–25.60; 궤양성 대장염: RR 8, 95% CI 5.86–10.67)¹⁷.
이러한 결과는
질환의 가족 내 유병률 증가를 설명하는 유전적 요소를 규명하려는 관심을 불러일으켰습니다.
전장유전체연관연구(Genome-wide association studies, GWAS)가 도입된 이후
IBD의 유전적 위험 loci 식별이 꾸준히 증가했으며,
그중 일부는 NOD2, OSMR, SMAD3, IL23R, HLA locus 등
면역 기능과 관련된 유전자입니다¹²,¹⁸,¹⁹.
현재까지
240개 이상의 IBD 관련 위험 loci가 확인되었습니다¹¹,¹⁸.
이는 고해상도 연구가 진행될수록
더 많은 관련 위험 loci가 밝혀질 가능성을 시사합니다.
그러나
현재까지의 결과는
유전적 위험이 질환 발달을 설명하는 비중은 상대적으로 작다는 점을 보여줍니다.
유럽계 86,640명과
동아시아·인도·이란계 9,846명을 포함한 대규모 다인종 연관연구에서 확인된 loci는
크론병 질환 liability 분산의 13.1%, 궤양성 대장염의 8.2%만 설명하며¹⁸,
유럽인과 아시아인 사이에 유전적 위험 결정인자에 상당한 차이가 있었습니다.
이는 대부분의 분산이 아직 발견되지 않은 loci나 환경 노출 같은 다른 요인에 기인한다는 것을 의미합니다.
또한 확인된 loci 중 기전적으로 질환과 명확히 연결된 것은 극히 적습니다¹¹,¹²,¹⁸.
전반적으로 유전학은
IBD 위험의 일부만 설명하며,
이는 환경 요인이나 기타 비유전적 요인이 질환 발달에서 중요한 역할을 한다는 점을 강조합니다.
유전적 위험과 환경적 위험의 상대적 기여도는 개인마다 다를 가능성이 높으며,
드문 단일유전자형(monogenic) IBD에서는 유전적 요인이 가장 큰 비중을 차지하지만,
다른 경우에는 환경 요인이 더 두드러질 수 있습니다.
Early life exposures
The early life period, considered conventionally to extend from prenatal life up to 5 years of age, represents a critical period towards immune maturation. Exposures during this period can modulate the risk of disease later in life20. The influence of early life exposures extends to IBD and other IMIDs13,21,22. In a systematic review and meta-analyses of 114 studies, restricted to exposures occurring during the first 5 years of age, Agrawal et al. have reported that infections, antibiotics, immigration from low to high incidence areas, passive smoking and breastfeeding modulate IBD risk 13. This finding is reminiscent of murine studies in which a ‘critical window of time’ in early life determines the immunological tone of the host and changes occurring within this timeframe associate with increased susceptibility to inflammatory pathologies later in life 23. Although breastfeeding seems to be protective against IBD 13, other exposures are detrimental. In subsequent epidemiological analysis, Agrawal, M. et al. have reported on increased ulcerative colitis risk with ≥3 courses of antibiotics during pregnancy and mebendazole, a broad-spectrum anthelminthic agent, exposure in early life24,25. Others have reported on the influence of greenspace and air pollutants on IBD risk, with increased greenspace conferring decreased risk and air pollutants conferring increased risk 26,27. Parental Crohn’s disease diagnosis at the time of birth, but not later in life, is associated with risk of Crohn’s disease in the offspring28. Last, in a case–control pilot analysis of deciduous teeth of 28 individuals with (n = 12) and without IBD (n =16), higher levels of heavy metals were positively associated with IBD diagnosis29.
Although these data provide important insights into the influence of the early life period on IBD risk, omics analysis of early life biological samples are critical to unravel downstream effects of these exposures. For example, in analyses of offspring of mothers with IBD with and without IBD, the former was reported to have intestinal dysbiosis [G], observed as altered microbial composition, which was found to trigger changes in adaptive immune cell subsets in germ free mice inoculated with stool from these individuals, and elevated faecal calprotectin [G] levels, a marker of intestinal inflammation, compared to the latter30,31. Based on these data, we hypothesize that early life exposures can modulate gut microbiome [G], mucosal immunological maturation, and thereby prime the immune system towards future health and disease already during the first years of life.
Early life exposures (조기 생애 노출)
조기 생애 기간(early life period)은
일반적으로 태아기부터 5세까지로 정의되며,
면역 성숙(immune maturation)에 매우 중요한 시기입니다.
이 기간 동안의 노출은
이후 생애의 질환 위험을 조절할 수 있습니다²⁰.
조기 생애 노출의 영향은
IBD를 포함한 다른 IMID에도 미칩니다¹³,²¹,²².
Agrawal et al.이 114개 연구를 체계적 검토·메타분석한 결과,
생애 첫 5년 동안의 노출(감염, 항생제, 저발생 지역에서 고발생 지역으로의 이주, 간접흡연, 모유수유 등)이
IBD 위험을 조절한다는 것이 보고되었습니다¹³.
이는
초기 생애의 ‘중요한 시간 창(critical window of time)’이
숙주의 면역 톤(immunological tone)을 결정하며,
이 기간 내 변화가 이후 염증성 질환 취약성을 증가시킨다는 동물 연구와 유사합니다²³.
모유수유는
IBD에 대해 보호 효과가 있는 것으로 보이지만¹³,
다른 노출들은 해로울 수 있습니다.
후속 역학 분석에서 Agrawal 등은
임신 중 항생제 3회 이상 투여와
조기 생애 메벤다졸(mebendazole, 광범위 구충제) 노출이 궤양성 대장염 위험을 증가시킨다고 보고했습니다²⁴,²⁵.
또한 녹지(greenspace)와 대기오염물질이 IBD 위험에 미치는 영향에 대한 연구도 있으며,
녹지 노출은 위험을 감소시키고 대기오염은 위험을 증가시킨다는 결과가 나왔습니다²⁶,²⁷.
출생 당시 부모가 크론병 진단을 받은 경우(출생 후 진단은 제외),
자녀의 크론병 위험이 증가한다는 보고도 있습니다²⁸.
마지막으로,
IBD 환자 12명과 비환자 16명을 대상으로 한 deciduous teeth(유치) 파일럿 분석에서
중금속 농도가 IBD 진단과 양의 상관관계가 있음이 보고되었습니다²⁹.
이러한 데이터는
조기 생애 기간이 IBD 위험에 미치는 영향을 중요한 통찰을 제공하지만,
조기 생애 생물학적 샘플의 오믹스(omics) 분석이 이러한 노출의 downstream 효과를 밝히는 데 필수적입니다.
예를 들어,
IBD 산모의 자녀(IBD 유무에 따라 분류) 분석에서
IBD 산모의 자녀는 장내 미생물 불균형(dysbiosis)을 보였으며,
이는 무균 마우스에 이들의 대변을 이식했을 때
적응면역 세포亚형 변화와 장내 염증 지표인 fecal calprotectin 상승을 유발했습니다³⁰,³¹.
이러한 데이터를 바탕으로 우리는
조기 생애 노출이 장내 미생물총,
점막 면역 성숙을 조절하여 생애 초기부터 미래 건강과 질환을 priming한다고 가정합니다.
Exposures later in life
Whereas physiological changes and environmental exposures in the early life period have been suggested to function as priming events making the immune system vulnerable to disease associated pathological changes, exposures encountered later in life might act as triggering events in the disease development or might function to further shape the immunological landscape. To date, several exposures have been suggested to increase risk of IBD, including urban living32, ultra-processed foods33–35, infections36, smoking37–39 and other factors 14. The usage of antibiotics has also been shown to increase risk of IBD. A study utilizing Danish register data identified exposure to antibiotics to be a risk factor for IBD within IBD families (two or more affected FDRs)40. Substantiating these findings, a population-based study published in 2023 linked antibiotics use to IBD risk across ages (10 to ≥60 years) 41. Interestingly, the risk increased with subsequent antibiotic courses and the highest risk of disease was observed 1–2 years after antibiotic exposures, indicating that antibiotics could be a potential trigger in the development of IBD, possibly acting through effects on the intestinal microbiome. Furthermore, nonsteroidal anti-inflammatory drugs (NSAIDs) usage has also been associated with increased risk of IBD. A study utilizing the nurses health cohort (n = 76,795), with 123 incident cases of Crohn’s disease and 117 cases of ulcerative colitis) showed that usage of NSAIDs at least 15 days per month was associated with increased risk of Crohn’s disease42.
An experimental study showed that propyzamide, a commonly utilized herbicide, promotes intestinal inflammation in IBD animal models43. Similarly, a study investigating two common emulsifiers showed induction of low-grade inflammation in wild-type mice and robust colitis in engineered mouse strains (Il10−/− and Tlr5−/− mice)44. Studies like these might help elucidate the mechanisms by which certain exposures increases IBD risk. Increased focus has been placed on perfluoroalkyl substances (PFAS). These compounds have so far been associated with ulcerative colitis in two studies, of respectively, 3,713 individuals45 and 32,254 individuals46. . However, evidence is still conflicting, underlined in a nested case–control study finding PFAS exposure to have no association with ulcerative colitis risk and an indication of an inverse association with Crohn’s disease risk47. Further research into these exposures in the pre-clinical phase and the mechanism by which they affect disease risk might aid in elucidating possible disease triggering events for IBD. Importantly, similar to the inter-individual differences in the contribution of environment versus genetics, it is likely that the influence of the various exposures could vary at each individual at risk, depending on timing, dose, synergistic effect or individual gene–environment interactions. Thus, it is plausible that a specific exposure might increase future risk of disease or act as a trigger initiating disease associate pathological changes in the individual patient.
Exposures later in life (후기 생애 노출)
조기 생애 기간의 생리적 변화와 환경 노출이
면역계를 질환 관련 병리학적 변화에 취약하게 만드는
priming event(준비 사건)로 작용할 수 있는 반면,
후기 생애에 접하는 노출은
질환 발달의 triggering event(유발 사건)로 작용하거나
면역 환경을 더욱 형성하는 역할을 할 수 있습니다.
현재까지
도시 생활³², 초가공식품(ultra-processed foods)³³⁻³⁵, 감염³⁶, 흡연³⁷⁻³⁹ 등
여러 노출이 IBD 위험을 증가시킨다는 보고가 있습니다.
항생제 사용 역시
IBD 위험을 높이는 것으로 밝혀졌습니다.
덴마크 등록 자료를 이용한 연구에서 항생제 노출은
IBD 가족(2명 이상의 1촌 친척이 환자) 내에서 IBD 위험 요인으로 확인되었습니다⁴⁰.
이를 뒷받침하듯 2023년에 발표된 인구 기반 연구는
10세부터 60세 이상까지 모든 연령대에서
항생제 사용이 IBD 위험과 연관되어 있음을 보여주었습니다⁴¹.
흥미롭게도 위험은
항생제 투여 횟수가 증가할수록 높아졌으며,
항생제 노출 후 1~2년에 질환 위험이 가장 높았습니다.
이는 항생제가 장내 미생물총에 미치는 영향을 통해
IBD 발달의 잠재적 유발 요인(trigger)이 될 수 있음을 시사합니다.
또한
비스테로이드성 항염증제(NSAIDs) 사용도 IBD 위험 증가와 연관이 있습니다.
Nurses’ Health Cohort(76,795명, 크론병 신규 환자 123명, 궤양성 대장염 117명)를 이용한 연구에서
한 달에 15일 이상 NSAIDs를 사용한 경우
크론병 위험이 증가한다는 결과가 나왔습니다⁴².
실험 연구에서는
흔히 사용되는 제초제 propyzamide가
IBD 동물 모델에서 장내 염증을 촉진한다는 것이 밝혀졌습니다⁴³.
마찬가지로 두 가지 흔한 유화제(emulsifiers)를 조사한 연구에서는
야생형 마우스에서 저등급 염증을,
engineered 마우스(Il10⁻/⁻, Tlr5⁻/⁻)에서는 강한 대장염을 유발하는 것으로 나타났습니다⁴⁴.
이러한 연구들은
특정 노출이 IBD 위험을 증가시키는 기전을 밝히는 데 도움이 될 수 있습니다.
최근
퍼플루오로알킬 물질(PFAS)에 대한 관심이 높아졌습니다.
이 물질은 지금까지 두 연구(각각 3,713명⁴⁵, 32,254명⁴⁶)에서 궤양성 대장염과 연관이 있는 것으로 보고되었습니다. 그러나 증거는 여전히 상충되며, nested case-control 연구에서는 PFAS 노출이 궤양성 대장염 위험과 무관하고, 오히려 크론병 위험과 역상관관계(inverse association)를 보인다는 결과가 나왔습니다⁴⁷.
이러한 노출들이 preclinical phase에서 미치는 영향과 질환 위험에 작용하는 기전에 대한 추가 연구가 IBD의 유발 사건(triggering events)을 밝히는 데 도움이 될 것입니다.
중요한 점은 환경 대 유전의 기여도에 개인차가 있는 것처럼, 다양한 노출의 영향력도 개인마다 시기, 용량, 시너지 효과, 유전자-환경 상호작용에 따라 다를 가능성이 높다는 것입니다. 따라서 특정 노출이 특정 개인에게 미래 질환 위험을 증가시키거나, 질환 관련 병리학적 변화를 시작시키는 trigger로 작용할 수 있습니다.
Preclinical phase: disease initiation
Studies utilizing samples from individuals who later develop IBD have increased rapidly in number in the past few years, with more studies on the horizon. The two main strategies utilized in these studies are retrospective studies utilizing serum and/or plasma repositories, exemplified by the Proteomic Evaluation and Discovery in an IBD Cohort of Tri-service Subjects (PREDICTs) study from the USA, which utilizes a retrospective military cohort with longitudinal samples collected during active military service of the included individuals48, and prospective studies following patients over time, exemplified by the Crohn’s and Colitis Canada Genetic Environmental Microbial (CCC GEM) project. This development has given rise to a wealth of new evidence aiding in the characterization of the pre-clinical phase of IBD and has shown that changes associated with disease development can be observed as far back as 10 years before clinical onset of disease.
(Preclinical phase: 질환 개시 단계)
최근 몇 년 동안 IBD로 진행되는 사람들의 샘플을 이용한 연구가 급증했으며, 앞으로 더 많은 연구가 진행될 예정입니다. 이러한 연구에서 사용되는 두 가지 주요 전략은 다음과 같습니다:
- 후향적 연구: 혈청·혈장 저장소(repository)를 이용한 연구. 미국의 PREDICTs 연구가 대표적이며, 군 복무 중 종단 샘플을 수집한 군인 코호트를 활용합니다⁴⁸.
- 전향적 연구: 환자를 장기 추적하는 연구. Crohn’s and Colitis Canada Genetic Environmental Microbial (CCC GEM) project가 대표적입니다.
이러한 발전으로 pre-clinical phase를 특징짓는 새로운 증거가 풍부해졌으며, 임상 발현 10년 전부터 질환 발달과 관련된 변화가 관찰될 수 있다는 것이 밝혀졌습니다.
Intestinal permeability
IBD is characterized by a chronic inflammatory state in the intestine of the affected individual and a hallmark of the disease is observed changes in the intestinal environment, including dysbiosis49–51, changes in epithelial barrier properties52–55, and a dysregulated intestinal mucosal immune response56–58. The CCC GEM project have specifically set out to investigate if changes in intestinal environment and function that are described post-disease diagnosis might also be detectable in the pre-clinical phase of the disease 59,60. The GEM cohort is composed of samples from close to 5,000 healthy FDRs from patients with Crohn’s disease who were followed over 10 years, of when around 100 so far have developed IBD. The first study published from this cohort measured fraction excretion ratio of lactulose to mannitol (LMR) in urine as a surrogate for intestinal barrier permeability in pre-clinical patients with Crohn’s disease59. Higher LMR was found to be significantly associated with development of Crohn’s disease (HR, 3.03; 95% CI, 1.64-5-63; P = 3.97 × 10−4) 3 years prior to diagnosis. Importantly, this association remained statistically significant when only including individuals with measurements from >3 years before diagnosis59. Presently, the etiology behind the increased permeability is not precisely defined. One view is that it is thought to represent a dysfunctional host–microbial interface. However, several environmental exposures, including smoking61, NSAID usage62 and alcohol consumption63, have been shown to affect intestinal permeability in humans. A previous study from the same group found that the genetic background in FDRs of patients with Crohn’s disease only had a limited effect on intestinal permeability64, which might suggest that the largest contribution to the increased permeability is due to other factors such as changes in the local intestinal environment. Thus, it is not clear from the present data if the observed increase in intestinal permeability is caused by changes in the microbiome or if it is a consequence of separate factors, such as environmental exposures. Furthermore, a GEM study published in 2021 found that matrix metalloproteinase 12 (MMP12), a matrix metalloproteinase previously associated with barrier dysfunction in a IBD mouse model65, and the chemokine Chemokine (C-X-C motif) ligand 9 (CXCL9) was simultaneously associated with Crohn’s disease development and increased intestinal permeability66, thereby linking proteolytic and inflammatory changes with increased permeability.
Intestinal permeability (장 투과성)
IBD는
환자의 장에 만성 염증 상태를 특징으로 하며,
질환의 특징적인 변화로는
**미생물 불균형(dysbiosis)**⁴⁹⁻⁵¹, 상피 장벽 특성 변화⁵²⁻⁵⁵, 조절 이상된 장 점막 면역 반응⁵⁶⁻⁵⁸이 있습니다.
CCC GEM project는 진단 후 관찰되는 장 환경 및 기능 변화가
pre-clinical phase에서도 검출될 수 있는지를 조사하는 것을 목표로 합니다⁵⁹,⁶⁰.
GEM 코호트는
크론병 환자의 가까운 1촌 친척 약 5,000명의 샘플로 구성되어 있으며,
10년간 추적 관찰 중 약 100명이 IBD로 진행했습니다.
이 코호트에서 처음 발표된 연구는
pre-clinical 크론병 환자에서
락툴로오스-만니톨 분획 배설 비율(LMR)을 소변에서 측정하여
장벽 투과성의 대리 지표로 사용했습니다⁵⁹.
LMR이 높은 경우
진단 3년 전에 크론병 발병과 유의한 연관성이 있었습니다(HR 3.03; 95% CI 1.64–5.63; P = 3.97 × 10⁻⁴).
특히
진단 3년 이상 이전 측정값만 포함했을 때에도
이 연관성은 통계적으로 유의했습니다.
현재 장 투과성 증가의 정확한 원인은 명확하지 않습니다.
한 가지 견해는
이것이 숙주-미생물 상호작용의 기능 장애를 반영한다는 것입니다.
그러나
흡연⁶¹, NSAIDs 사용⁶², 알코올 섭취⁶³ 등
여러 환경 노출이 인간의 장 투과성을 변화시킨다는 것이 알려져 있습니다.
같은 그룹의 이전 연구에서는
크론병 환자 1촌 친척의 유전적 배경이 장 투과성에 미치는 영향이 제한적이라는 결과가 나왔습니다⁶⁴.
이는
장 투과성 증가의 대부분이 장 내 국소 환경 변화 같은 다른 요인에 기인할 수 있음을 시사합니다.
따라서
현재 데이터로는 관찰된 장 투과성 증가가 미생물총 변화에 의한 것인지,
아니면 환경 노출 같은 별개의 요인에 의한 것인지 명확하지 않습니다.
또한
2021년에 발표된 GEM 연구에서는
matrix metalloproteinase 12 (MMP12) (IBD 마우스 모델에서 장벽 기능 장애와 연관된 물질)과
CXCL9 chemokine이 크론병 발병 및 장 투과성 증가와 동시에 연관되어 있음을 밝혔습니다⁶⁶.
이는
단백분해 및 염증 변화와 장 투과성 증가를 연결짓는 결과입니다.
Dysbiosis
In line with the findings described in the previous section, another study from CCC GEM utilized fecal samples from 7 patients with ulcerative colitis, 13 patients with pre-ulcerative colitis, and 48 healthy individuals and found an increase in the fecal proteolytic activity in the pre-ulcerative colitis group compared with healthy controls, which was associated with microbiota changes, including increases in Bacteriodes vulgatus and decreases in Akkemansia and Adlercreutzia in these patients60. Furthermore, colonization of germ-free mice with the pre-ulcerative colitis microbiome gave rise to similar microbiota changes and increased the colonic cell counts of polymorphonuclear leukocytes, suggesting that the microbial changes and increased proteolytic activity possibly result in intestinal inflammation. Changes in the intestinal proteolytic environment have previously been reported for patients with IBD with active disease67–69, and from the findings described earlier it seems that compositional and functional changes in the microbiota, which might augment intestinal inflammation, are present prior to clinical onset of ulcerative colitis in some patients. Several studies have previously shown that healthy siblings to patients with IBD have altered gut microbiota with lower microbial diversity than healthy individuals70–72. In 2023, utilizing data from the GEM cohort, the first study showing that gut microbiome changes associated with later Crohn’s disease onset was published. In this study, the authors utilized a machine learning approach to produce a microbiome risk score (MRS) and showed that this MRS was associated with Crohn’s disease onset (HR, 2.24, 95% CI, 1.03–4.84, P = 0.04) and could to some degree predict disease onset in up to 5 years before disease onset (AUC = 0.67)73. Interestingly, in the GEM cohort, healthy siblings shared aspects of the dysbiosis observed in patients with Crohn’s disease, including lower concentrations of Faecalibacterium prausnitzii, Clostridia cluster IV and Roseburia spp., additionally some of these changes in the siblings correlated with intestinal permeability. This finding might indicate a link between the observed changes in intestinal permeability in patients with pre-Crohn’s disease and dysbiosis70. Besides the indicated link between dysbiosis and intestinal permeability, changes in the composition of the microbiome are likely also associated with changes in the metabolome [G]. One study showed that P. gingivalis induced dysbiosis in a mouse model directly correlated with metabolic changes, including metabolites involved in lipid metabolism and amino acids metabolism, 74.In another study, microbiome alterations in newborn mice induced behavioral impairment in the mice, which was mediated by changes in circulating metabolites, including 4-methylphenol 75. Changes in metabolic processes have been found in patients with IBD and many of these changes are suggested to be associated with host–microbiota interactions76. A study utilizing two different pre-clinical cohorts showed for the first time that perturbances in metabolic profiles were present years before diagnosis of disease in both patients with Crohn’s disease and ulcerative colitis77. Changes that could be hypothesized to be linked to compositional changes in the microbiome.
Dysbiosis (미생물 불균형)
이전 섹션에서 설명한 결과와 일관되게, CCC GEM project의 또 다른 연구에서는 궤양성 대장염 환자 7명, pre-ulcerative colitis 환자 13명, 건강인 48명의 대변 샘플을 분석한 결과, pre-ulcerative colitis 그룹에서 건강 대조군에 비해 대변 단백분해 활성(proteolytic activity)이 증가했으며, 이는 Bacteroides vulgatus 증가, Akkermansia와 Adlercreutzia 감소 등의 미생물총 변화와 연관되어 있었습니다⁶⁰.
더 나아가, pre-ulcerative colitis 미생물총으로 무균 마우스를 colonization한 결과 비슷한 미생물 변화와 대장 내 다형핵 백혈구(polymorphonuclear leukocytes) 수 증가가 관찰되었습니다. 이는 미생물 변화와 단백분해 활성 증가가 장내 염증을 유발할 가능성을 시사합니다.
장내 단백분해 환경 변화는 이미 활동성 IBD 환자에서 보고된 바 있으며⁶⁷⁻⁶⁹, 앞서 언급한 결과들을 종합하면 미생물총의 조성 및 기능 변화가 일부 환자에서 궤양성 대장염의 임상 발현 이전에 이미 존재하며, 이는 장내 염증을 증폭시킬 수 있습니다.
이전에 여러 연구에서 IBD 환자의 건강한 형제자매(siblings)도 건강인에 비해 미생물 다양성 감소를 포함한 장내 미생물총 변화가 있다는 것이 보고되었습니다⁷⁰⁻⁷².
2023년 GEM 코호트 데이터를 이용한 연구에서는 크론병 발병과 연관된 장내 미생물총 변화를 처음으로 보여주었습니다. 이 연구에서 연구자들은 기계학습(machine learning) 기법을 이용해 미생물 위험 점수(Microbiome Risk Score, MRS)를 개발하였으며, 이 MRS가 크론병 발병과 연관되어 있음(HR 2.24, 95% CI 1.03–4.84, P=0.04)을 확인했습니다. 또한 이 점수는 발병 최대 5년 전까지 질환을 어느 정도 예측할 수 있었습니다(AUC=0.67)⁷³.
흥미롭게도 GEM 코호트에서 건강한 형제자매들은 크론병 환자에서 관찰되는 dysbiosis의 일부 측면(Faecalibacterium prausnitzii, Clostridia cluster IV, Roseburia spp. 농도 감소)을 공유하고 있었으며, 일부 변화는 장 투과성과도 상관관계가 있었습니다. 이는 pre-Crohn’s disease 환자에서 관찰된 장 투과성 증가와 dysbiosis 사이의 연관성을 시사합니다⁷⁰.
dysbiosis와 장 투과성의 연관성 외에도, 미생물총 조성 변화는 대사체(metabolome) 변화와도 관련이 있을 가능성이 높습니다. 한 연구에서는 P. gingivalis가 마우스 모델에서 dysbiosis를 유발하였으며, 이는 지질 대사와 아미노산 대사에 관여하는 대사체 변화와 직접 상관관계가 있음을 보여주었습니다⁷⁴. 또 다른 연구에서는 신생 마우스의 미생물총 변화가 순환 대사체(특히 4-methylphenol) 변화를 매개로 행동 장애를 유발한다고 보고했습니다⁷⁵.
IBD 환자에서도 대사 과정 변화가 관찰되었으며, 이 중 많은 변화가 숙주-미생물 상호작용과 관련이 있는 것으로 제안되고 있습니다⁷⁶. 두 개의 서로 다른 pre-clinical 코호트를 이용한 연구에서는 크론병과 궤양성 대장염 모두에서 진단 수년 전부터 대사 프로필의 섭동(perturbation)이 존재한다는 것이 처음으로 밝혀졌습니다⁷⁷. 이는 미생물총 조성 변화와 연관되어 있을 가능성이 높습니다
Autoimmune and antimicrobial humoral responses
Substantiating the observed changes in the intestinal environment, elevated levels of different antimicrobial antibodies, as well as some autoantibodies [G], have also been associated with disease development, some as far back as 10 years before diagnosis78–80. Hence, dysregulated humoral responses seem to be activated years before diagnosis.
Hitherto, most studies have focused on antimicrobial antibodies. Israeli et al. were the first to cross-link records of patients with IBD with available serum from the Israeli Army’s serum repository, thereby identifying 38 pre-diagnosis serum samples from 32 patients with Crohn’s disease and 10 pre-diagnosis serum samples from 8 patients with ulcerative colitis, which were tested for ASCA [G] (anti-Saccharomyces cerevisiae antibody) IgA, ASCA IgG and ANCA (antineutrophil cytoplasmic antibodies). Overall, 31% of patients with Crohn’s disease and 0% of healthy individuals as controls tested positive for ASCA. The mean titters of ASCA increased towards diagnosis, as did the proportion of patients with ASCA positivity. After ASCA detection, the mean interval to Crohn’s disease diagnosis was 3.2 years (range 1.7–6.4 years). In ulcerative colitis, 25% of patients versus 0% of the matched controls tested positive for ANCA9. These results were later expanded using serum samples from the European Prospective Investigation into Cancer and Nutrition study that reported on 77 incident cases of Crohn’s disease (mean time before diagnosis 4.5 years, SD 3.2) and 167 incident cases of ulcerative colitis (mean time before diagnosis 4.4 years, SD 3.1), matched to two healthy controls. Pre-diagnosis samples were tested for ASCA IgG, ASCA IgA, perinuclear ANCA (pANCA), anti-OmpC and anti-CBir181. The predictive accuracy of combining markers was higher than the accuracy of each marker alone. Subsequently, the PREDICTs study showed that antimicrobial antibodies are present at least 5 years before diagnosis82,83. In 200 individuals who developed Crohn’s disease compared with healthy individuals, the most predictive anti-microbial markers were ASCA-IgA, anti-FlaX and ASCA-IgG. Their predictive performance based on univariate models was 0.69 (95 % CI,0.61–0.76), 0.61 (95 % CI, 0.53–0.69), and 0.69 (95 % CI, 0.62–0.77), respectively, 5 years before diagnosis82. In this large study, pANCA was not predictive of ulcerative colitis development82. From the same study, investigators showed that antimicrobial antibodies, such as ASCA-IgA, were associated with an increased risk of developing Crohn’s disease stricturing [G] and/or penetrating [G] complications at diagnosis (HR: 1.33; 95% CI 1.13–1.55 at 2–4 years before diagnosis; HR: 1.30; 95% CI 1.10–1.51 at 6 years before diagnosis)84. In the CCC GEM cohort, a baseline positivity for at least 2 antimicrobial antibodies (which was observed in 43% of FDRs developing Crohn’s disease versus 11% of healthy FDRs as controls) was associated with an adjusted odds ratio of Crohn’s disease of 6.5 (95% CI, 3.4–12.7; P <0.001), an observation that was independent of intestinal permeability, fecal calprotectin level, C-reactive protein level, and CD-polygenic risk score78. These data provocatively suggest that immune dysregulation might be an independent risk factor in the subsequent development of IBD.
Using the PREDICTs study samples, a separate study looked into Granulocyte Macrophage-Colony Stimulating Factor (GM-CSF) autoantibodies (aGMAb), reporting that both IgG and IgA aGMAb were found 6 years prior to Crohn’s disease diagnosis in 21% and 7% of samples, respectively, but not in ulcerative colitis or healthy individuals, with additional patients seroconverting and mean titer increasing from 1/190 to 1/320 towards the time of diagnosis.79 By the time of diagnosis, the seroprevalence for IgA and IgG aGMAb in individuals that developed Crohn’s disease was 12% and 25%, respectively, suggesting that increasing titers of the pro-inflammatory IgG antibodies57 correlated with clinical disease. Additionally, these autoantibodies were associated with ileal and/or ileocolonic involvement and a 2.8 risk (HR) of developing penetrating and/or stricturing disease or undergoing surgery following Crohn’s disease diagnosis79. IgA aGMAb was a predictor of Crohn’s disease development with >97% specificity and with sensitivity increasing from 15% to 21% as time to diagnosis decreased (AUC 0.6)79. In a 2023 study, the presence of anti-integrin αvβ6 IgG autoantibodies (anti-αvβ6) were tested in the preclinical stages of ulcerative colitis. For this analysis, serum from 82 individuals who later developed ulcerative colitis who were matched to 82 individuals that remained healthy (healthy controls) was studied in the PREDICTs study, and validated in the GEM cohort. The authors found that anti-αvβ6 levels were significantly higher in sera from patients who developed ulcerative colitis than the controls at all timepoints tested (earliest sample obtained at 10 years before diagnosis). Seropositivity increased from 20.7% at the earliest timepoint to 52.4% at diagnosis, and the predictive performance of anti-αvβ6 increased from 0.79 at 10 years to 0.89 at two years before diagnosis80.
Altogether, these findings suggest that evidence of dysregulated immune responses precede clinical disease and imply possibly breaking of immune tolerance similar to what is seen in other IMIDs such as RA and SLE85,86. The observation of such changes up to 10 years prior to diagnosis supports the notion of a long initiation phase in IBD.
Autoimmune and antimicrobial humoral responses (자가면역 및 항균 체액성 반응)
장 환경 변화에 대한 증거를 뒷받침하듯, 다양한 항균 항체와 일부 자가항체(autoantibodies)의 상승도 질환 발달과 연관되어 있으며, 일부는 진단 10년 전부터 관찰됩니다⁷⁸⁻⁸⁰. 따라서 조절 이상된 체액성 면역(humoral responses)이 진단 수년 전부터 활성화되는 것으로 보입니다.
지금까지 대부분의 연구는 항균 항체에 초점을 맞추었습니다. Israeli et al.이 처음으로 IBD 환자의 기록과 이스라엘 군 혈청 저장소의 혈청을 연계하여 분석한 결과, 크론병 환자 32명의 진단 전 혈청 38개와 궤양성 대장염 환자 8명의 진단 전 혈청 10개를 ASCA IgA, ASCA IgG, ANCA(항호중구세포질항체)로 검사했습니다. 전체적으로 크론병 환자의 31%가 ASCA 양성(건강 대조군 0%)이었으며, ASCA 역가와 양성 비율은 진단에 가까워질수록 증가했습니다. ASCA 검출 후 크론병 진단까지의 평균 기간은 3.2년(범위 1.7–6.4년)이었습니다. 궤양성 대장염에서는 환자의 25%가 ANCA 양성(대조군 0%)이었습니다⁹.
이 결과는 이후 European Prospective Investigation into Cancer and Nutrition 연구의 혈청 샘플을 이용해 확대되었습니다. 크론병 신규 환자 77명(진단 전 평균 4.5년), 궤양성 대장염 신규 환자 167명(진단 전 평균 4.4년)을 대상으로 ASCA IgG, ASCA IgA, pANCA, anti-OmpC, anti-CBir1을 검사한 결과, 여러 마커를 조합했을 때 개별 마커보다 예측 정확도가 높았습니다⁸¹.
이후 PREDICTs 연구에서는 항균 항체가 진단 최소 5년 전부터 존재한다는 것이 확인되었습니다⁸²,⁸³. 크론병으로 진행된 200명을 건강인과 비교한 결과, 가장 예측력이 높은 항균 마커는 ASCA-IgA, anti-FlaX, ASCA-IgG였으며, 5년 전 단변량 모델에서의 예측 성능은 각각 0.69, 0.61, 0.69였습니다⁸². 이 대규모 연구에서 pANCA는 궤양성 대장염 발병을 예측하지 못했습니다.
같은 연구에서 ASCA-IgA 등 항균 항체는 크론병 진단 시 협착(stricture) 및 관통(penetrating) 합병증 위험 증가와 연관되어 있었습니다(진단 2~4년 전 HR 1.33; 6년 전 HR 1.30)⁸⁴.
CCC GEM 코호트에서는 기저 시점에 최소 2개 이상의 항균 항체 양성(크론병으로 진행된 FDR 43% vs 건강 FDR 11%)이 크론병 발병의 조정 odds ratio 6.5(95% CI 3.4–12.7, P<0.001)와 연관되어 있었으며, 이는 장 투과성, fecal calprotectin, CRP, CD-polygenic risk score와 무관한 독립적 위험 요인이었습니다⁷⁸. 이는 면역 조절 이상(immune dysregulation)이 IBD 발달의 독립적 위험 요인일 수 있음을 시사하는 도발적인 결과입니다.
PREDICTs 연구 샘플을 이용한 별도의 연구에서는 Granulocyte Macrophage-Colony Stimulating Factor (GM-CSF) 자가항체(aGMAb)를 분석한 결과, IgG와 IgA aGMAb가 크론병 진단 6년 전부터 각각 21%와 7%에서 검출되었으며(궤양성 대장염과 건강인에서는 검출되지 않음), 진단에 가까워질수록 추가 환자에서 seroconversion(항체 양전화)이 일어나고 평균 역가가 1/190에서 1/320으로 증가했습니다⁷⁹. 진단 시점에는 IgA와 IgG aGMAb의 seroprevalence가 각각 12%와 25%였으며, 이는 염증 촉진성 IgG 항체 역가 증가가 임상 질환과 상관관계가 있음을 시사합니다. 또한 이 자가항체는 회장 및 회맹부 침범과 크론병 진단 후 관통 및 협착 질환 또는 수술 위험 증가(HR 2.8)와 연관되어 있었습니다⁷⁹. IgA aGMAb는 97% 이상의 특이도로 크론병 발병을 예측하였으며, 진단까지의 기간이 짧아질수록 민감도는 15%에서 21%로 증가했습니다(AUC 0.6)⁷⁹.
2023년 연구에서는 anti-integrin αvβ6 IgG 자가항체(anti-αvβ6)를 궤양성 대장염의 preclinical 단계에서 검사했습니다. PREDICTs 연구에서 이후 궤양성 대장염으로 진행된 82명과 건강하게 남은 82명을 매칭하여 분석하고, GEM 코호트에서 검증한 결과, anti-αvβ6 수준은 진단 10년 전부터 모든 시점에서 궤양성 대장염으로 진행된 환자에서 대조군보다 유의하게 높았습니다. Seropositivity는 가장 이른 시점 20.7%에서 진단 시 52.4%로 증가했으며, 예측 성능은 10년 전 0.79에서 2년 전 0.89로 향상되었습니다⁸⁰.
이러한 결과들은 조절 이상된 면역 반응이 임상 질환에 앞서 나타난다는 것을 시사하며, RA나 SLE와 유사하게 면역 관용(immune tolerance)의 붕괴가 일어나고 있음을 암시합니다⁸⁵,⁸⁶. 진단 10년 전까지 이러한 변화가 관찰된다는 것은 IBD에 긴 initiation phase(개시 단계)가 존재한다는 개념을 뒷받침합니다.
Changes in protein markers
An earlier study from Swedish nationwide registries reported that elevated erythrocyte sedimentation rate (≥15 mm) among male individuals in late adolescence was associated with a diagnosis of Crohn’s disease later in life (HR 5.95, 95% CI 4.47–7.92)87. Thereafter, the Nurses’ Health Study investigated markers of inflammation in 83 cases of incident Crohn’s disease and 90 cases of ulcerative colitis (one serum sample available per individual, median time interval between blood collection and diagnosis of Crohn’s disease or ulcerative colitis of 6.6 and 6.8 years, respectively). Serum levels of IL-6 and C-reactive protein (CRP) of the pre-IBD groups were significantly higher than healthy individuals controls, with a positive correlation between levels of these systemic markers and risk of IBD88. The large PREDICTs study assessed the predictive value of a panel of 1,129 proteins (SomaLogic®, Colorado, USA)82. Overall, 51 proteins were predictive of Crohn’s disease with a 76% accuracy up to 5 years prior to diagnosis, and 87% accuracy at 1-year pre-diagnosis. Proteomic markers preceding disease diagnosis were markers of inflammation (levels of CRP, serum amyloid P, trypsin 2), markers involved in cytokine signaling, innate immunity and response to bacteria (complement factors, TNF-receptor subunits, lipopolysaccharide binding protein, proteinase-3 and several interleukins)82. Several dysregulated pathways in preclinical Crohn’s disease were identified, such as the lysosome pathway, pathways involved in glycosaminoglycan metabolism and the complement pathway82. The GEM cohort proteomics in serum were studied using the Olink® (Olink Holding, Uppsala, Sweden) Proximity Extension Assay platform (446 circulating proteins) and their association with levels of anti-microbial antibodies and fecal calprotectin, as well as measurement of intestinal permeability, was assessed. Overall, 71 healthy FDRs who developed Crohn’s disease were matched to 284 FDRs that remained healthy. The authors reported that 25 proteins associated with risk of developing Crohn’s disease (bearing biological plausibility) the most consistent being Chemokine (C-X-C motif) ligand 9 that presented the highest OR with future risk of Crohn’s disease (OR=2.07 per SD, 95% CI 1.58–2.73, q=7.9e-5)66. Importantly, CXCL9 was also significantly associated with all other Crohn’s disease-risk biomarkers with consistent direction of effect. Notably, in the GEM cohort, the timeframe before diagnosis is quite narrow in some patients (interquartile range (IQR) 1.0–3.5 years before diagnosis). Even if different panels were used to study proteomics it is interesting to note that no statistically significant overlap was identified with the set of proteins described in the PREDICTs study66. Finally, using the plasma samples biobanked from individuals who developed ulcerative colitis later in life (n = 72) and matched healthy controls (n = 140), Swedish investigators measured the abundance of 92 protein (Olink® panel). The median period from when a prediagnostic sample was obtained to the diagnosis of ulcerative colitis was 4.8 years (IQR 2.2–7.2 years). They described a set of six proteins (MMP10, CXCL9, CCL11, SLAMF1, CXCL11 and CCL2) to be upregulated in the serum of those with preclinical ulcerative colitis as compared with controls. However, the predictive accuracy of each marker alone was under 65%, and of the 6 markers combined was 0.71 (0.63–0.78)89. Thus, there are signs that disease-associated systemic inflammation is present years prior to diagnosis in IBD patients, indicating a long disease initiation phase.
Changes in the glycome
The human glycome, defined as the multitude of complex carbohydrates produced by our cells, covering surfaces of both cells and proteins, are increasingly recognized as having an important role in both homeostatic and pathological responses90. Dysregulation of the glycome has been shown in IBD91 and have been linked to autoimmune diseases through changes in antibody glycosylation patterns92,93 and reaction to host-derived glycans94. Presently, no studies have been conducted specifically to investigate glycome changes in pre-clinical IBD. However, in addition to the discovery of the aGMAb antibody in the previously mentioned PREDICTs study, it was also found that these antibodies targeted a changed glycosylation of the GM-CSF protein. These antibodies were further associated with altered glycosyltransferase expression in ILC3 (type 3 innate lymphoid cells) and T cells79. Furthermore, in another PREDICTs study, pathway analysis on serum protein markers identified glycosaminoglycan metabolism as a dysregulated pathway in pre-clinical Crohn’s disease82. Thus, it is likely that changes in the glycome precede onset of IBD and might play and important part in disease development.
Pre-clinical phase : disease expansion
From the initiation phase data, we can infer increased intestinal permeability and dysbiosis leads to dysregulated innate and adaptive immune responses, and thereby the observed increases in inflammatory and serological markers. The latest evidence, especially within epidemiology, indicates the presence of an escalation of pathophysiological processes a few years prior to diagnosis, characterized by subclinical inflammation [G] and increased use of healthcare services.
Subclinical inflammation
Studies reporting on fecal calprotectin levels, a biomarker of intestinal inflammation, in asymptomatic individuals are key towards characterizing both the initiation and expansion phase. Several studies focusing on healthy relatives of patients with IBD have found that a subset of those relatives display elevated faecal calprotectin levels78,95–97. In a study from the GEM cohort including 1,420 FDRs of whom 50 developed Crohn’s disease during follow-up (median follow-up time 2.95 years) faecal calprotectin level >100 μg/g was associated with an increased risk of developing Crohn’s disease (HR, 7.76; 95% CI 3.99–15.11). Furthermore, faecal calprotectin level was weakly correlated with intestinal permeability at recruitment (R=0.069, P=0.012, Spearman correlation)59. A study that recruited 480 healthy FDRs (siblings, offspring or parents), calculated a risk score for disease development based on polygenic risk scores (PRS) and smoking history. Those individuals falling into the highest or lowest risk score quartiles were asked to undergo a video capsule endoscopy98,99. From these groups, 35% had elevated faecal calprotectin level ≥50 μg/g, and 21%, mostly from the high quartile risk score (n=22), presented a Lewis score ≥135 (abnormal inflammation); notably, in 11 participants, again from the high-risk group, Lewis score was ≥790 (moderate-to-severe small bowel inflammation), and one individual was diagnosed with Crohn’s disease during the 3 year follow-up98,99. These data suggest that subclinical intestinal inflammation is likely to be present a few years prior to symptomatic disease onset. Notably, the pre-clinical samples utilized in the previously described GEM study investigating association between proteomic markers and serological markers, permeability and intestinal subclinical inflammation, corresponded to ~2 years prior to diagnosis and the disease-associated changes observed could therefore be hypothesized to be linked to subclinical inflammation during a phase of disease expansion66. This idea is underlined by their finding that several of the disease-associated proteomic markers were also associated with increased faecal calprotectin levels.
Epidemiological data
Use of medical records from population-based registers to investigate healthcare and laboratory parameters prior to IBD onset has helped understand better the pre-clinical phase, whilst also highlighting that the transition point from the initiation phase to the expansion phase seems to be fluid. Published in 2022, Cohen et al. reviewed medical records from an Israeli health register (n = 5,643) to investigate changes in laboratory parameters, healthcare services and medication use 5 years before diagnosis of IBD100. The authors reported a significant increase in the use of health care services, such as visits to general practitioner and ER visits, prior to diagnosis for both Crohn’s disease and ulcerative colitis, with a marked increase 2 years prior to diagnosis (P <0.001). A finding in line with a Danish population-based cohort study including 9,019 patients with Crohn’s disease and 20,913 patients with ulcerative colitis showing increased pre-clinical social costs compared with controls representing the general population (10 years before diagnosis: 1.4 times higher for Crohn’s disease and 1.5 times higher for ulcerative colitis)101. A difference between ulcerative colitis and Crohn’s disease was observed in that several parameters changed for Crohn’s disease, but not ulcerative colitis, within the 5 years prior to diagnosis. These parameters included inflammatory biomarkers such as CRP levels, white blood cell count and platelet count, as well as a greater number of Helicobacter pylori tests taken and elevated use of medications, including antibiotics, proton pump inhibitors and NSAIDs, especially in the 2 years prior to IBD diagnosis. A limitation of the Israeli study is the lack of a matched healthy control population, hindering the comparability to the general population. Rodríguez-Lago et al. reported that of 31,005 individuals who underwent screening colonoscopy, an incidental diagnosis of IBD was made in 0.35% of the cohort. Of these individuals, some showed endoscopic signs indicative of subclinical inflammation and 36% of individuals developed symptoms after a follow-up period of 25 months (IQR = 10.5–42)102,103. Lastly, in a retrospective study that investigated healthcare and medication use preceding diagnosis in the same cohort, a higher use of primary and specialized care, as well as increased steroid use, was observed in the 3–5 years prior to diagnosis104. Another population-based case–control study published in 2021 investigated gastrointestinal symptoms before diagnosis of IBD in 19,554 cases and 78,114 healthy individuals as controls observed increases in reported gastrointestinal symptoms during a 10-year period prior to diagnosis (9.6% and 10.4% of Crohn’s disease and ulcerative colitis cases, respectively, compared with 5.8% for controls)105. In line with these findings, a Danish population-based study investigating medication use of patients with IBD in the pre-clinical phase between years 2005 and 2018, found that medication use across all organ systems was increased in the 10 years prior to IBD diagnosis, compared with matched controls (1.1 to 1.8-fold higher), with marked increase in the 2 years prior to diagnosis106. The described findings suggest that not only do symptoms, apparently unrelated to disease, arise many years before diagnosis, but the general increased use of medication across all organ systems indicate that the disease might have a more far-reaching effect than previously expected.
The data discussed here suggest increased healthcare utilization up to at least 10 years prior to IBD diagnosis, especially in last 2–3 years preceding diagnosis, hence suggesting a transition from initiation phase to the expansion phase at this stage. Notably, there might also be differences between preclinical Crohn’s disease and ulcerative colitis. The described epidemiological findings could indicate a less pronounced pre-clinical phase in ulcerative colitis than in Crohn’s disease or that clinically active disease happens more acutely in ulcerative colitis. However, the observations might be influenced by other factors as well, such as ulcerative colitis generally being a more mucosal disease3, which could influence the measured laboratory markers.
Proposed integrated model
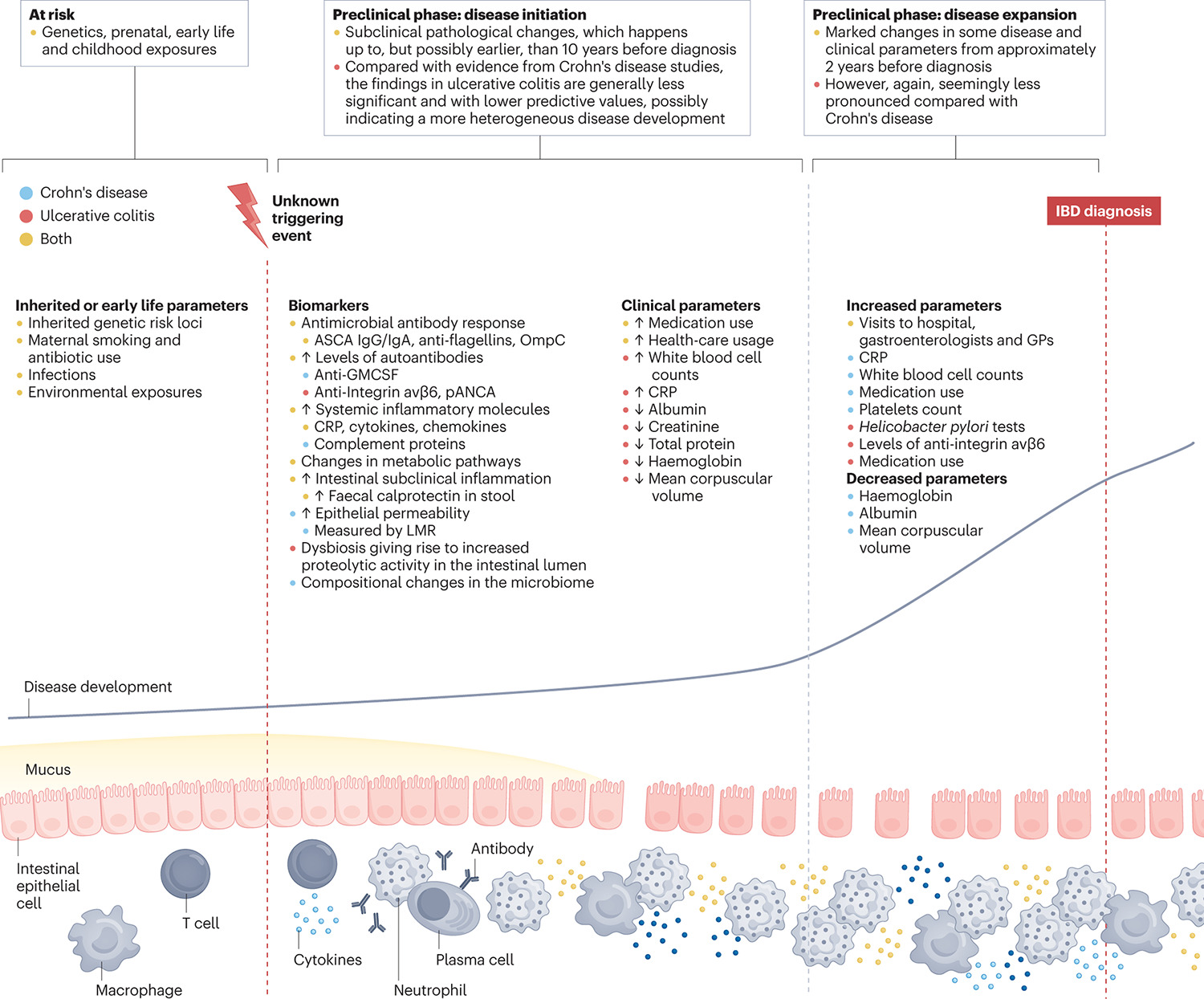
A critical step towards prediction and preventative strategies in IBD is to delineate the integrated pathways that lead to disease onset. With expansion of research in pre-clinical IBD, we now have insights into multilevel perturbations that lead to disease onset. Integrating these factors, we applied the putative model of preclinical IBD suggested by the European Crohn’s and Colitis Organization (ECCO)10 with grouping of the pre-clinical period into phases evolving from at-risk individuals through pre-clinical disease initiation, over a pre-clinical disease expansion phase of approximately 2 years, to actual diagnosis of disease (Figure 1). However, the sequence of events in the pre-clinical phase of IBD is ambiguous due to lack of longitudinal data and biological samples, and limited clarity on the timing of triggering events and disease initiation. Current data, including those from epidemiological studies, suggest increased healthcare utilization and subclinical inflammation years prior to diagnosis of clinical disease. From the described evidence, the pre-clinical phase in Crohn’s disease seems to be characterized by a heightened inflammatory state that involves perturbations within host–microbial interactions, loss of epithelial integrity and dysregulation of mucosal immune pathways, some of which can also be detected within the systemic circulation. By contrast, although less is evident in the pre-clinical phase of ulcerative colitis, emerging data suggests that disruptions of the immune system lead to targeting of endogenous antigens. With ongoing research, more preclinical abnormalities are likely to emerge in both Crohn’s disease and ulcerative colitis. The described findings seem to substantiate the previously hypothesized escalation of pathophysiological processes that culminate in overt clinical disease, therefore not only pointing to opportunities to presage the clinical diagnosis, but also to development of preventative or disease-modifying therapeutic interventions.
Figure 1 |. Proposed model of disease development in IBD based on the current evidence.
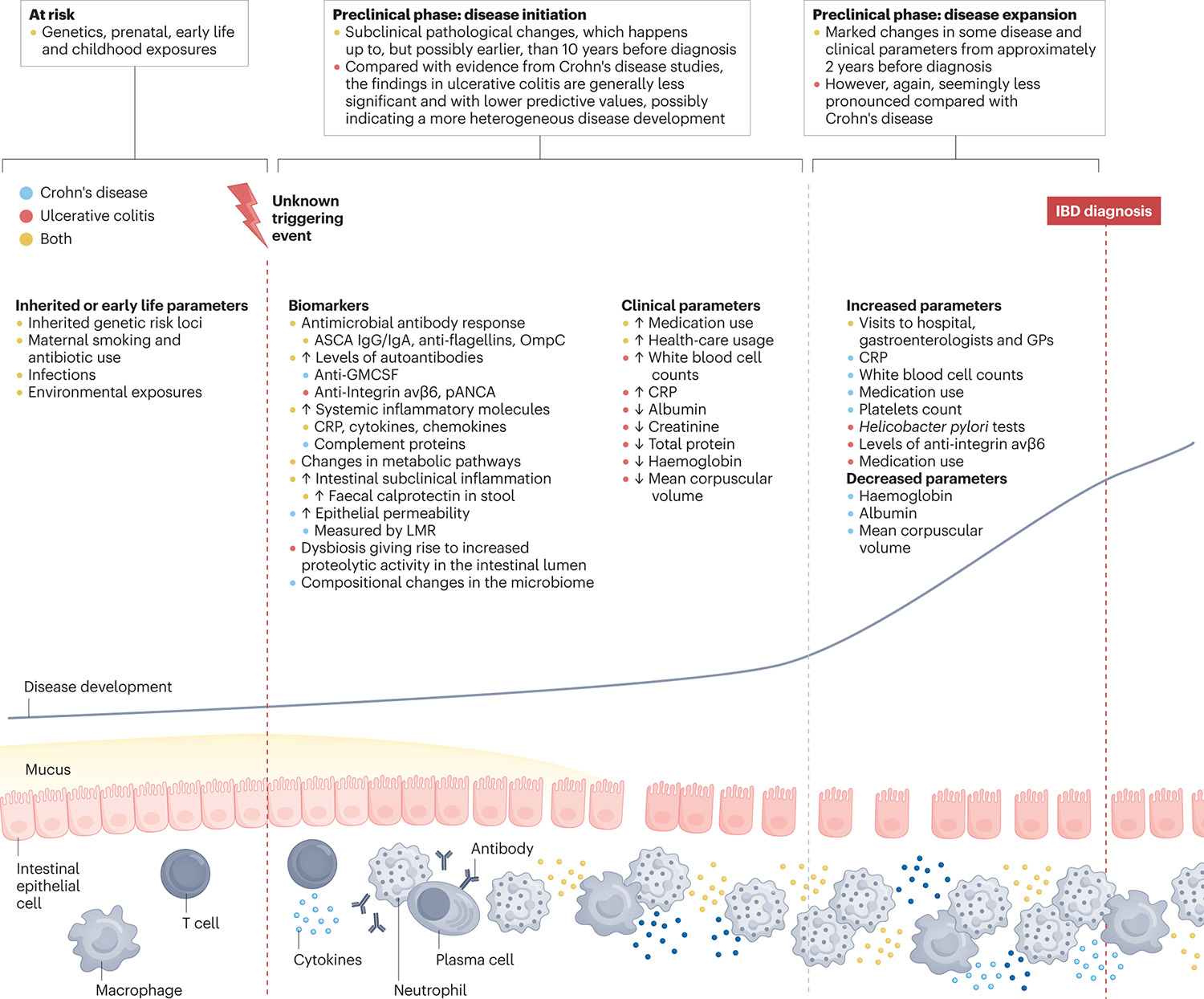
It is hypothesized that development of inflammatory bowel disease (IBD) is structured into several subphases, as initially suggested by the European Crohn’s and Colitis Organization (ECCO)10, evolving from at-risk individuals through pre-clinical disease initiation, over a disease expansion phase of approximately 2 years, to actual diagnosis of disease. The at-risk period is characterized by genetic and environmental risk factors, which could prime the intestinal immune system towards dysregulation and future disease. One or more unknown triggering events are suggested to push susceptible individuals towards disease initiation. This disease initiation phase is characterized by several pathological changes, including breaking of immune tolerance, as implied by autoantibody and antimicrobial antibody production, increased intestinal permeability, dysbiosis and changes in some clinical parameters, with so far elusive temporal order. It is proposed that from approximately 2 years prior to diagnosis escalation of pathophysiological processes that culminate in overt clinical disease takes place, characterized by marked changes in some parameter’s indicative of possible subclinical inflammation and acceleration of not yet disease attributed symptoms. Evidence pertaining to the different disease subtypes has been indicated as follows (see key): blue dot, evidence pertaining pre-clinical Crohn’s disease; pink dot, evidence pertaining to pre-clinical ulcerative colitis; yellow dot, evidence pertaining to both subtypes. ASCA; anti-Saccharomyces cerevisiae antibodies; CRP, C-reactive protein; GP, General practitioner; LMR, lactulose-to-mannitol ratio; OmpC, Outer-membrane porin C; pANCA, perinuclear anti-neutrophil cytoplasmic antibodies. Original illustration by Jill K. Gregory, adapted with permission of © Mount Sinai Health System
Future directions
Current evidence suggests a marked overlap across IMIDs, which could inform future directions in IBD research (Box 1). The preclinical phases of other IMIDs, such as RA and SLE, are relatively well-characterized; such frameworks are applicable towards IBD 6–8,85,86. The disease with the longest studied pre-clinical phase is RA with studies looking at association between pre-clinical Rheumatoid Factor (RF) and disease development going as far back as 1988, in which patients diagnosed between 1967 and 1986 were investigated. This longitudinal population study found that higher titers of RF associated with increased incidence of RA (48.3 cases per 1,000 for RF titer >1:256, P <0.001)107. A later study utilizing serial measurements of IgM RF and anti-cyclic citrullinated peptide (anti-CCP) antibodies from 79 pre-clinical RA blood donor samples, showed seropositivity of either antibody in 49% of the patients before symptomatic onset of disease108. Additionally, a study published in 2012 profiling autoantibodies in pre-clinical RA and their association with disease development showed that anti-CCP2 seropositive patients had increasing mean numbers of anti-citrullinated protein antibodies (ACPAs) and increased mean total number of elevated cytokines towards diagnosis109, thereby linking production of autoantibodies with increases in inflammatory makers in pre-clinical RA. Similarly, a study using longitudinal serum samples from the Department of Defense Serum Repository (DoDSR) (84 SLE cases with ~3 samples per case) found that antinuclear autoantibodies and several soluble inflammatory markers, including IL-5, IL-6 and IFN-γ, were elevated more than 3 years prior to diagnosis in SLE. Furthermore, they observed elevation of several inflammatory mediators, including IFNγ and IL-4, IL-5 and IL-6, prior to development of seropositivity (HR range between 1.54 – 7.13)110, indicating that an elevated inflammatory state might start prior to autoantibody production in SLE. These findings underline the strength of individual patient longitudinal samples in combination with measurement of several disease-associated parameters in attempting to elucidating temporal order of events within the pre-clinical phase.
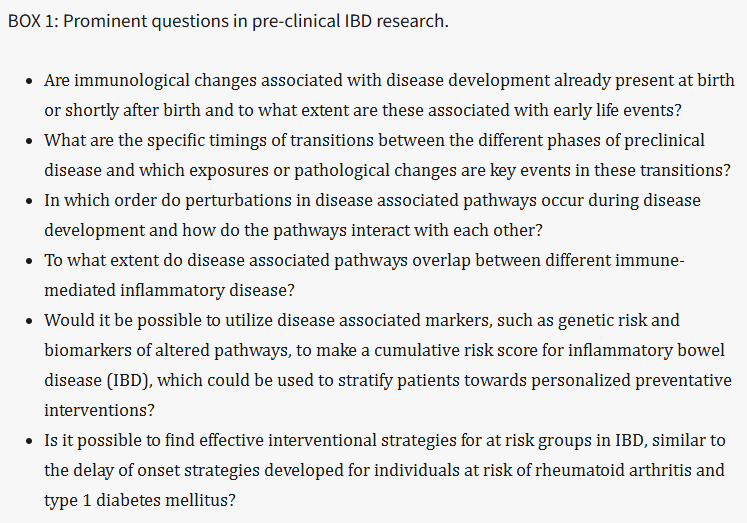
BOX 1: Prominent questions in pre-clinical IBD research.
From these described studies, common features across IMIDs seems to be the detection of autoantibodies in some individuals, as well as elevated levels of systemic inflammatory markers, many years prior to diagnosis of disease, implying breaking of immune tolerance and a heightened inflammatory state. Interestingly, a study investigated disease characteristic autoantibodies across IMIDs (RA, SLE and type 1 diabetes mellitus (T1DM)), utilizing 1,321 samples collected from patients with active disease and unaffected autoantibody positive and negative FDRs. They observed that alternative autoimmunity, defined as presence of at least one autoantibody associated with another IMID, occurred in all investigated groups (patients with SLE, 56%; SLE FDRs 57.4%; patients with RA, 32.6 %; RA FDRs, 34.8; patients with T1DM, 43%), therefore showing that autoantibody signatures can be shared across these IMIDs111. To our knowledge no such study design has been performed investigating pre-clinical parameters between IBD and other IMIDs. Such studies might be of interest as to elucidate possible common pathways between diseases. Notably, it is observed across IMIDs that only a subset of patients who develop disease are seropositive for a given autoantibody, indicating that the presence of these autoantibodies in themselves are not enough to cause disease. This observation might suggest that the development through the pre-clinical phase is driven by either one major pathway or an interplay between several personalized pathways, which has previously been suggested for RA86. As dysregulation of glycosylation patterns have been implicated in both active IBD and other diseases, and have shown to affect simultaneously dysbiosis, the mucosal immune system and epithelial barrier integrity, it is tempting to hypothesize that a pathological change in the glycome might be a common central pathway in IBD90–92. Interestingly, several studies have shown association between aberrant glycosylation of antibodies and disease development in RA93,112. One study utilizing longitudinal samples from 126 FDRs found extensive V-domain glycosylation in FDRs who later developed RA, and this glycosylation was strongly associated with future disease onset (HR = 6.07)93. Another study utilizing samples from several cohorts found that increased galactosylation of IgG autoantibodies was present prior to disease and correlated with disease activity in RA (Spearmans’s P = 0.37, P <0.0001)112. Thus, investigations of such aberrant antibody glycosylation could be a relevant topic for future research in pre-clinical IBD, as well as in cross-IMID studies. Lastly, it has been suggested that changes in intestinal permeability and dysbiosis contributes to the pathogenesis in several IMIDs113, therefore it can be hypothesized that such changes are a key event not only in IBD development but across IMIDs. Hence, investigations of pre-clinical changes in the microbiome and intestinal barrier properties across IMIDs could be of interest to test this hypothesis. Although many advances have been made over the past few years in finding biomarkers and highlighting pathogenic mechanisms in the pre-clinical stages of IBD, research in this area is still behind compared to what has been done in other IMIDs such as RA or T1DM, where disease-prevention trials have been started many years ago. A clue to what might be possible can be found in T1DM, in which a randomized controlled trial from 2019 with 76 high-risk patients showed that a 2-week course treatment with teplizumab, an anti-CD3 monoclonal antibody, could delay diagnosis of clinical T1DM in high-risk patients by a median of 2 years114. A finding that later in November 2022 resulted in a landmark approval of the drug to delay T1DM onset115. Similar observations of delay of disease onset by treatment of at-risk groups have also been noted for RA116. Thus, going forward it is crucial to work towards better stratification of risk-groups, and to elucidate underlying pathways that could serve as therapeutic targets for disease modulation and/or interception. This effort might in the future make it possible to propose different interventional strategies dependent on the specific pathways involved (personalized treatment), the level of disease risk and the specific stage of disease development (Figure 2).
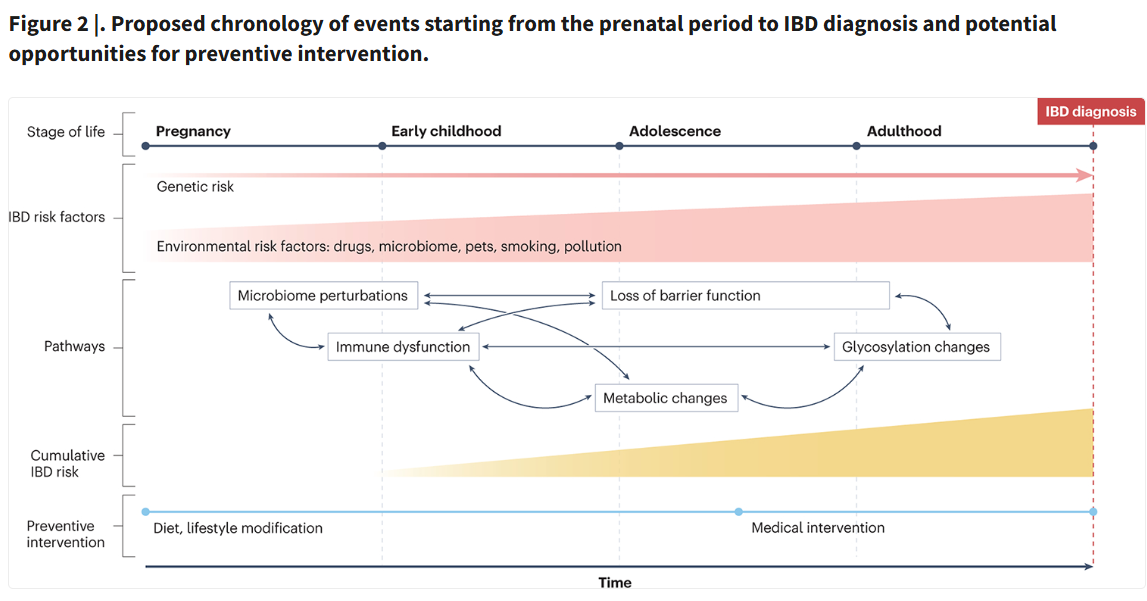
Figure 2 |. Proposed chronology of events starting from the prenatal period to IBD diagnosis and potential opportunities for preventive intervention.
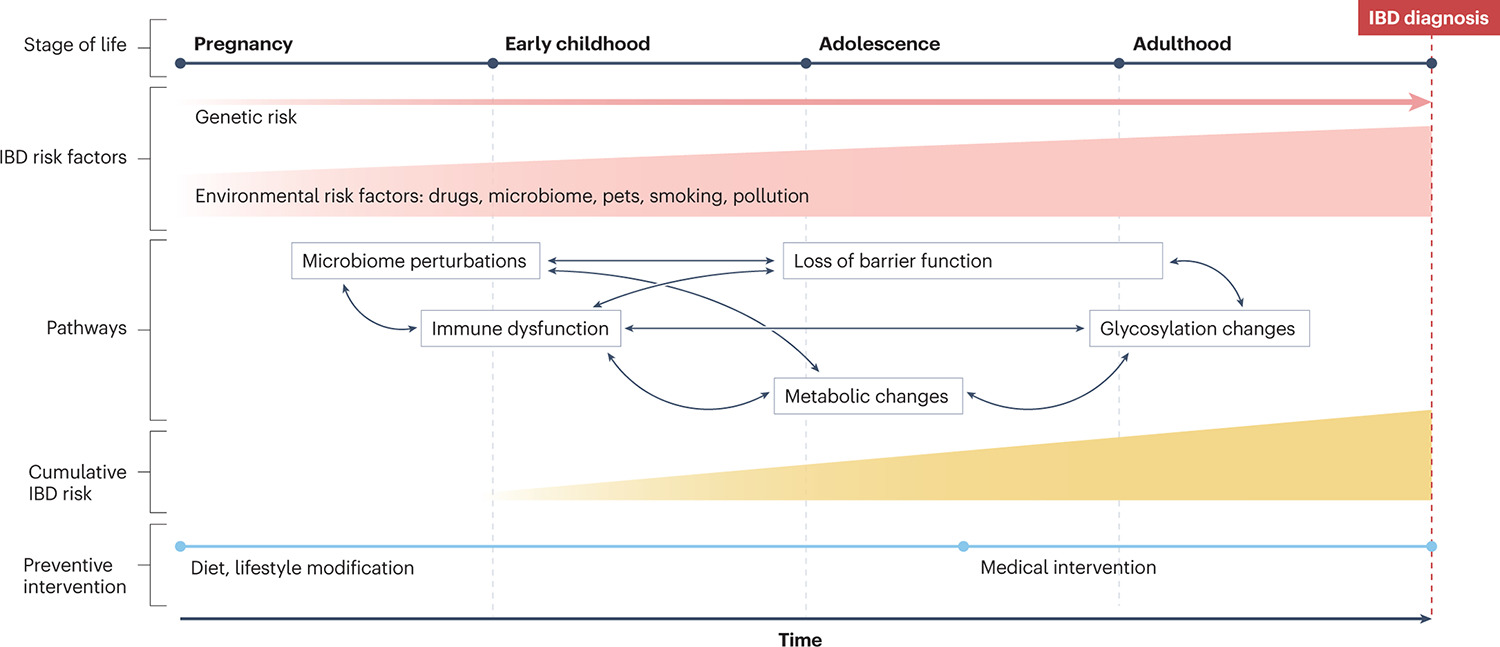
In this figure, we hypothesize that the window of susceptibility starts during the prenatal period and continues until inflammatory bowel disease (IBD) diagnosis. In a background of genetic risk, progressive and cumulative exposure to relevant environmental risk factors (for example, infections, antibiotics, pets, smoking, pollution) might contribute to IBD risk over the course of an individual’s life. These exposures lead to downstream events, including gut microbiome perturbations with loss of microbial diversity and alterations in specific taxa, altered innate and humoral immune function, loss of intestinal epithelial integrity, metabolic changes, and altered glycosylation of potentially pathogenic antibodies. The order in which these perturbations occur is not yet established, but crosstalk across pathways is likely. We propose that a cumulative risk score representing genetic risk and biomarkers of altered pathways can help estimate preclinical IBD risk and it can be stratified towards personalized preventive interventions. For example, diet and lifestyle modification might be a reasonable intervention for low-risk persons, whereas medical intervention might be appropriate for high-risk individuals. Notably, this timeline represents a broad overview of IBD. Considering substantial heterogeneity across IBD risk, phenotypes and outcomes, these events and timeline are likely to vary across different subsets of IBD. Original illustration by Jill K. Gregory, adapted with permission of © Mount Sinai Health System
From the described evidence, there is clearly substantial overlap in pre-clinical disease development across IMIDs. These commonalities and the evidence already present from other IMIDs can prove to be a valuable inspiration for future research in the field of pre-clinical IBD. To facilitate understanding of the complexities governing IBD development, the utilization of cohorts containing longitudinal pre-clinical samples within the same individual is likely crucial. Such studies will aid in the elucidation of temporal changes in disease relevant parameters before disease onset. Furthermore, combining several different data sources (such as proteomics, glycomics, metabolomics and serology), via state-of-the-art network analysis, seem essential for elucidating relationships between pathological events and discovering novel pathways. It is also crucial to investigate the mechanistic effects of identified exposures in the pre-clinical phase and to understand whether the influence of early life events is measurable at the molecular level already at birth, which could also enhance our understanding of priming of the intestinal immune system. Lastly, the overlap of pre-clinical features across IMIDs makes cross-IMID studies of great interest to identify common pathways and facilitate shared preventative strategies.
Conclusions
In summary, the vast expansion of studies investigating the pre-clinical phase of IBD within the last years have made it evident that events associated with disease development happens many years prior to its clinical onset, as observed for several other IMIDs6,85,86. Overlaps across preclinical disease across IMIDs suggest commonalities across underlying pathways pertaining to immune dysregulation. Recent data suggest that preclinical IBD occurs at least two years prior to IBD diagnosis and is characterized by systemic and intestinal subclinical inflammation, as well as increases in non-specific symptoms and healthcare utilization. However, the precise sequential order of pathological events within the pre-clinical phase is still elusive with the current evidence, as is the exact timing of transition from disease initiation phase to disease expansion phase. To uncover the phases of disease development and discover how demonstrated pathological changes are associated with specific pathways, it will be crucial to utilize cohorts containing longitudinal pre-clinical samples within the same individual in combination with state-of-the-art bioinformatics methodologies, such as network analysis. Furthermore, studies investigating disease relevant parameters across IMIDs could prove crucial in understanding commonalities in development of immune mediated inflammatory disease.
Table 1 |.
Selected studies investigating the preclinical phase of IBD
ReferenceDisease subtypes investigatedTimepoint(s) before diagnosisaCohort detailsMain findings
| Singular timepoint in the pre-clinical phase | ||||
| Van Schaik et al. (2013)81 | Crohn’s disease and ulcerative colitis | ~4.5 years | 77 pre-Crohn’s disease cases (mean age at diagnosis, 52.6 years) and 154 healthy individuals as controls (mean age at recruitment, 52.5 years); 167 pre-ulcerative colitis cases (mean age at diagnosis, 58 years) and 334 healthy individuals as controls (mean age at recruitment, 53.6 years) | A combination of serological markers (pANCA, ASCA, CBir1 and OmpC) could to some degree predict disease development (Crohn’s disease: AUC = 0.679; ulcerative colitis: AUC = 0.657). |
| Choung, R. S. et al. (2016)83 | Crohn’s disease | ~6 years | 100 pre-Crohn’s disease cases (median age at diagnosis, 30 years) | Showed that increased seropositivity towards antimicrobial serological markers is associated with complications at or shortly after diagnosis. |
| Lochhead, P. et al. (2017)88 | Crohn’s disease and ulcerative colitis | ~6–7 years | 83 pre-Crohn’s disease cases (median age, 52.7 years), 90 pre-ulcerative colitis cases (median age, 50.4 years), 344 healthy individuals (median age, 51.7 years) | Elevated plasma levels of CRP and IL-6 was associated with disease development in both Crohn’s disease and ulcerative colitis. |
| Turpin, W. et al. (2020)59 | Crohn’s disease | ~3 years | 50 pre-Crohn’s disease FDRs (median age at recruitment, 16 years) and 1,370 healthy FDRs (median age at recruitment, 19 years) | Observed increased intestinal permeability (through LMR measurements) in FDRs that later develop Crohn’s disease. |
| Lee, S. H. et al. (2021)78 | Crohn’s disease | ~3 years | 77 pre-Crohn’s disease FDRs (median age at recruitment, 16 years) and 307 healthy FDRs (median age at recruitment, 16.1 years) | High seropositivity of a panel of antimicrobial antibodies was significantly associated with Crohn’s disease development (OR 6.5). Association was independent of abnormal barrier function, subclinical inflammation and Crohn’s disease-related genetic risks. |
| Bergemalm, D. et al. (2021)89 | Ulcerative colitis | ~5 years | Pre-clinical cohort: 72 pre-ulcerative colitis cases (median age at diagnosis, 54 years) and 140 healthy individuals as controls (median age at sampling, 50 years). Inception cohort: 101 treatment-naïve ulcerative colitis cases (median age at diagnosis, 37 years) and 50 healthy individuals as controls (median age at sampling, 26 years). Healthy twin cohort: 37 healthy twins (median age at sampling, 59 years) and 41 healthy individuals as controls (median age at sampling, 60 years) | Six inflammatory proteins were found to be elevated in pre-clinical ulcerative colitis cases compared with healthy individuals. These proteins could discriminate Treatment-naïve patients with ulcerative colitis from healthy individuals with an AUC of 0.92. |
| Galipeau, H. J. et al. (2021)60 | Ulcerative colitis | ~4.5 years | 13 pre-ulcerative colitis FDRs (mean age at recruitment, 19.7 years) and 48 healthy individuals as controls (mean age at recruitment, 20.3 years) | Increased proteolytic activity was observed for patients with pre-ulcerative colitis and this changed activity was associated with functional changes in the gut microbiome. |
| Hua, X. and Ungaro R. C. et al. (2022)77 | Crohn’s disease and ulcerative colitis | Nurse cohort: ~10 years for ulcerative colitis and ~8 years for Crohn’s disease. PREDICTs cohort: ~12 years for ulcerative colitis and ~6.5 years for Crohn’s disease | Nurse cohort: 55 pre-ulcerative colitis cases (mean age at diagnosis, 55.8 years), 49 pre-Crohn’s disease cases (mean age at diagnosis, 55.7 years) and 208 healthy individuals as controls (mean age at blood sampling, 55.8 years). PREDICTs cohort: 25 pre-ulcerative colitis cases (mean age at diagnosis, 34.1 years), 25 pre-Crohn’s disease cases (mean age at diagnosis, 33.3 years) and 25 healthy individuals as controls. | Several metabolic pathways were significantly associated with disease development for both ulcerative colitis and Crohn’s disease. First study to show that there are changes in metabolic pathways in the pre-clinical phase of IBD. |
| Leibovitzh, H. et al. (2023)66 | Crohn’s disease | ~2 years | 71 pre-Crohn’s disease FDRs (median age at recruitment, 15 years) and 284 healthy FDRs (median age at recruitment, 16 years) | 25 serum proteins were found to be significantly associated with Crohn’s disease development. Several of these proteins were also associated with markers of subclinical inflammation, antimicrobial antibody responses and gut barrier function. |
| Garay, R. et al. (2023)73 | Crohn’s disease | ~3 years | 73 pre-Crohn’s disease FDRs and 3,483 healthy FDRs Median age at recruitment was 17 years (range, 6–35 years) | Utilizing a machine learning approach on 16S ribosomal RNA sequencing data and the construction a microbiome risk score (MRS) the authors showed for the first time an association between changed microbial composition and later Crohn’s disease onset (HR: 2.24). Furthermore, this MRS could to some degree predict patients with pre-Crohn’s disease up to 5 years before onset (AUC: 0.67) |
| Longitudinal timepoints in the pre-clinical phase | ||||
| Israeli, E. et al. (2005)9 | Crohn’s disease and ulcerative colitis | >60 months, 37–60 months, 1–37 months | 32 pre-Crohn’s disease cases (mean age at diagnosis, 24.8 years) and 95 healthy individuals as control, 8 pre-ulcerative colitis cases (mean age at diagnosis, 23.5 years) and 36 healthy individuals as controls | 31.3% of the patients with Crohn’s disease in the cohort were ASCA positive prior to diagnosis and ACSA positivity was seen in 15.4% of the samples taken 60 months prior to diagnosis. |
| Torres, J. et al. (2020)82 | Crohn’s disease and ulcerative colitis | ~5 years, ~4 years, ~2 years and at diagnosis (± 1 year) | Four longitudinal samples from 200 pre-Crohn’s disease cases (mean age at diagnosis, 31.4 years), 199 pre-ulcerative colitis cases (mean age at diagnosis, 28.9 years) and 200 healthy individuals as controls (mean age at latest sample, 28 years) | A panel of serum antibodies and proteins found to be associated with disease development every year from 5 years before disease development was shown to predict Crohn’s disease development with high accuracy (AUC range: 0.76 at −5 years and 0.85 at −1 year). |
| Mortha, A. et al. (2022)79 | Crohn’s disease and ulcerative diagnosis | ~ 6 years, ~3.5 years and at diagnosis | Three to four longitudinal samples from 220 pre-Crohn’s disease cases (mean age ~31 years), 200 pre-ulcerative colitis cases (mean age, ~ 31 years) and 200 healthy individuals as controls (mean age, ~32 years) | Anti-GM-CSF autoantibodies were found up to 6 years prior to disease development in patients with pre-Crohn’s disease and these antibodies were associated with complications within 100 days of diagnosis (HR: 2.8). Titers of autoantibody increased towards diagnosis. The autoantibodies were found to be specific for an altered post-translational glycosylation on GM-CSF. |
| Livanos, A. E. et al. (2023)80 | Ulcerative colitis | ~10 years, ~4 years, ~2 years and at diagnosis | Main cohort: four longitudinal samples from 82 pre-ulcerative colitis cases (mean age at diagnosis, 32 years) and 82 healthy individuals as controls (mean age at recruitment, 32.6. years) Validation cohort: 12 pre-ulcerative colitis (mean age at recruitment, 17.7 years) and 49 healthy individuals as controls (mean age at recruitment, 17.3 years) | Anti-integrin-αvβ6 autoantibodies was significantly increased in patients with pre-ulcerative colitis up to 10 years prior to diagnosis and predicted ulcerative colitis development (AUC range: 0.79 at -10 years and 0.89 at -2 years). The autoantibodies were significantly associated with adverse disease outcomes (HR: 1.39). |
| Choung, R. S. et al. (2023)84 | Crohn’s disease | ~6 years, ~4 to ~2 years (aggregated) and at diagnosis | Three to four longitudinal samples from 201 pre-Crohn’s disease cases (mean age at diagnosis, ~31 years) and 201 healthy individuals as controls (mean age, 28.5 years) | Levels of antimicrobial antibodies and protein markers (reflecting inflammatory, fibrosis and tissue protection markers) were associated with development of complicated Crohn’s disease onset up to 6 years prior to diagnosis. |
| Register data to investigate the pre-clinical phase | ||||
| Vadstrup, K et al. (2020)101 | Crohn’s disease and ulcerative colitis | 10 years before diagnosis to diagnosis | 9,019 pre-Crohn’s disease cases (mean age at diagnosis, 42.2 years) and 20,913 pre-ulcerative colitis cases (mean age at diagnosis, 47.5 years). Controls matched 1:1. | Societal costs and number of additional diagnosis were found to be substantially higher for patients with IBD than the general population in the 10 years prior to diagnosis with a spike from 2 years prior to diagnosis. |
| Blackwell, J. et al. (2021)105 | Crohn’s disease and ulcerative colitis | 10 years before diagnosis to diagnosis | 5,874 pre-CD cases, 13,681 pre-ulcerative colitis cases and 54,616 healthy individuals Age at diagnosis of cohort mostly >39 years. | One in four cases of IBD was found to have reported gastrointestinal symptoms > 6 months prior to diagnosis with 9.6% and 10.4% reported symptoms 5 years before Crohn’s disease and ulcerative colitis diagnosis, respectively. Previous diagnosis of IBS and depression was associated with delays in specialist review. |
| Cohen, N. A. et al. (2022)100 | Crohn’s disease and ulcerative colitis | 5 to 1 year before diagnosis | 3,039 pre-Crohn’s disease cases (mean age, 37.48 years), 2,322 pre-ulcerative colitis cases (Mean age, 41.2 years) and 282 pre-indeterminate colitis (Mean age, 44.21 years) | Showed changes in laboratory parameters, healthcare service and medication use occur in the 5 years preceding IBD diagnosis. A spike in the 2 years prior to diagnosis was noted in CD patients for some parameters, including levels of CRP, White blood cells counts, platelets and usage of medications, such as NSAIDs and antibiotics. Both disease subtypes showed similar spikes in health care utilization. |
| Rodríguez-Lago, I. et al. (2023) 104 | IBD | 5 and 3 years prior to diagnosis | 124 pre-IBD cases, 305 symptomatic-onset IBD and 372 healthy individuals as controls Median age of 56 years (Interquartile range [IQR], 53–62) | Increased visits to primary care and use of steroids in the periods of 3 and 5 years prior to diagnosis for patients with IBD. |
| Bonfils, L et al. (2023) 106 | IBD | 10 years before diagnosis to diagnosis | 29,219 pre-IBD cases and 292,190 non-IBD cases | Increased use of a broad range of medications was observed for patients with IBD up to 10 years prior to diagnosis with a steep increase in the 2 years prior to diagnosis. |
A table showing information about publications on the preclinical phase of IBD divided into publications looking at a single pre-clinical timepoint, several pre-clinical timepoints (longitudinal studies) and publications utilizing data from registries. ASCA; anti-Saccharomyces cerevisiae antibodies, AUC; Area under the ROC Curve; CRP, C-reactive protein; FDR, First degree relative; HR, Hazard ratio; LMR, lactulose-to-mannitol ratio; OmpC, Outer-membrane porin C; OR, Odds ratio; pANCA, perinuclear anti-neutrophil cytoplasmic antibodies; PREDICTs, PRoteomic Evaluation and Discovery in an IBD Cohort of Tri-service Subjects.
a
The noted timepoint(s) for the non-register-based studies are reflecting mean or median time from sample acquisition to diagnosis in the cohort for the given studies.
Key points.
Acknowledgements
The authors thank Jill Gregory, Certified Medical Illustrator, Icahn School of Medicine at Mount Sinai, for the original versions of the illustrations. M.A. is supported by the National Institute of Diabetes and Digestive and Kidney Diseases (K23DK129762-02). T.J. is funded by a center of excellence grant from the Danish National Research Foundation (DNRF148); the foundation had no role in the review.
GlossaryIMIDs
Immune-mediated inflammatory diseases comprise a diverse spectrum of diseases, which share commonalities in the inflammatory nature of the diseases and similar genetic, environmental and immunological factors
Dysbiosis
An imbalance in the composition of the microbial community that is associated with adverse health outcomes
Faecal calprotectin
An intracellular neutrophilic protein commonly measured in fecal samples as a way to measure degree of intestinal inflammation
Microbiome
The collection of genetic material from all the microorganisms present in which are part of a specific environment
Preclinical disease
The part of disease development prior to clinical onset of disease
Commensals
Microorganisms that derives benefits from the host without aiding or causing harm to said host
Self-antigen
An antigen produced by your own cells that elicits an immune response by your own immune cells leading to production of self-reactive antibodies known as autoantibodies, often as consequence of breaking of immune tolerance
Immune tolerance
The state of unresponsiveness of the immune system towards molecules produced by the host, as to prevent damage to healthy tissues
Autoantibodies
Antibodies targeting molecules produced by the hosts own cells, also known as self-antigens
Metabolome
The complete spectrum and number of metabolites present within an organism, tissue, or cell
ASCA
Antibodies targeting mannan molecules on the fungus Saccharomyces cerevisiae
Stricturing complications
The narrowing of a part of the intestine as a consequences of scar tissue in the intestinal wall, often as a result of chronic inflammation
Penetrating complications
Formation of fistulas or abscess in the intestinal wall as a result of chronic uncontrolled inflammation
Subclinical inflammation
An inflammatory condition that does not yet give rise to clinically apparent symptoms in the individual
Footnotes
Competing interests
S.M. has received research grants from Genentech and Takeda; payment for lectures from Genentech, Morphic and Taleda; and consulting fees from Arena Pharmaceuticals, Ferring, Morphic and Takeda. J.-F.C. reports has received research grants from AbbVie, Janssen Pharmaceuticals and Takeda; payment for lectures from AbbVie, Amgen, Allergan. Ferring Pharmaceuticals, Shire and Takeda; has received consulting fees from AbbVie, Amgen, Arena Pharmaceuticals, Boehringer Ingelheim, BMS, Celgene Corporation, Eli Lilly, Ferring Pharmaceuticals, Galmed Research, Genentech, Glaxo Smith Kline, Janssen Pharmaceuticals, Kaleido Biosciences, Imedex, Immunic, Iterative Scopes, Merck, Microbia, Novartis, PBM Capital, Pfizer, Protagonist Therapeutics, Sanofi, Takeda, TiGenix, Vifor; and holds stock options in Intestinal Biotech Development. J.T. has received research grants from AbbVie and Janssen Pharmaceuticals; has received ad board fees from AbbVie, Janssen Pharmaceuticals, Pfizer and BMS; has received speaker fees from AbbVie, Janssen Pharmaceuticals and Pfizer. J.J.R., M.A. and T.J. declare no competing interests.
Peer review information
Nature Reviews Gastroenterology & Hepatology thanks Luc Biedermann, Iago Rodriguez-Lago and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
References
- 1.Xavier RJ & Podolsky DK Unravelling the pathogenesis of inflammatory bowel disease. Nature 448, 427–434 (2007). [DOI] [PubMed] [Google Scholar]